
Abstract
Background:
The need for surgical management of severe obesity in the context of inflammatory bowel disease (IBD) is becoming an increasingly common clinical scenario, yet has been met with significant reservation due to the paucity of current data from which to inform evidence-based clinical decision making. The aim of our study was to perform a systematic review to characterize and evaluate the safety and efficacy of bariatric surgery in IBD patients.
Methods:
A medical librarian developed and executed comprehensive searches on November 2, 2021. The population of interest was adult subjects (>18 years) diagnosed with inflammatory bowel disease (IBD) undergoing any type of bariatric surgery. Meta-analysis was used to evaluate outcomes using RevMan 5.4.1.
Results:
A total of 330 687 patients were identified within the 11 studies included. Within all included studies there were 1595 patients with IBD. Patients had a mean weighted age of 46.0, with a female predominance (n = 1287, 80.7%). The mean duration of follow up was 39.7 months. Metabolic and anthropometric outcomes were only reported in noncomparative studies evaluating only patients with IBD, limiting the ability to complete meta-analysis. Meta-analysis revealed that IBD was associated with increased rates of postoperative complications (RR 2.14; 95% CI 1.87-2.44; P < .00001) in comparison to controls without IBD.
Conclusion:
While bariatric surgery presents an effective weight loss option for patients with IBD, these patients are associated with higher rates of postoperative complications. This work highlights the need to better delineate the effect of bariatric procedures for patients with IBD with respect to both metabolic and IBD-related outcomes.
Introduction
The global rise of obesity has increased exponentially over the last several decades, in part due to sedentary lifestyles and convenient access to highly processed foods.1,2 These factors are contributing to obesity not only in the general population but also within other disease states like inflammatory bowel diseases (IBD) where patients have traditionally suffered from malnutrition and difficulties with maintaining adequate body weight. 3 Indeed, the need for surgical management of severe obesity in the context of IBD is becoming an increasingly common clinical scenario, yet has been met with significant reservation due to the risks of adverse postoperative outcomes like leaks, wound infections, and malnutrition. There currently exists a paucity of data on outcomes of bariatric surgery in patients with IBD.
Another area of growing interest has been the role of bariatric surgery in modifying IBD disease course. Similar to IBD, obesity itself presents a state of chronic systemic and gastrointestinal inflammation. 4 Obesity may thus potentiate the pro-inflammatory milieu of IBD, potentially leading to adverse propagation of both disease states.5,6 For example, studies have shown that both zonulin, a biomarker of intestinal permeability as well as other systemic markers of inflammation including tumor necrosis factor (TNF)−α6 and C-reactive protein, are elevated in obesity, potentially perpetuating intestinal permeability and inflammation present in IBD.7-9 It stands to reason, that since bariatric surgery has been demonstrated to reduce chronic systemic inflammation and improve gut barrier integrity, it may also positively influence the disease course of IBD. 10 This concept, however, has not yet been investigated.
The aim of our study was to perform a systematic review and meta-analysis to characterize and evaluate the safety and efficacy of bariatric surgery in patients with IBD. Secondary outcomes were to evaluate the role of bariatric surgery on modifying IBD disease course. Understanding the comparative safety profile and outcomes of bariatric surgery in patients with IBD will inform future obesity interventions in this patient population.
Materials and Methods
Study Design and Formulation of Research Question
This systematic review and meta-analysis was performed in keeping with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines (Supplemental Tables 1 and 2).11,12 To design the study question we used the PICOS (population, intervention, comparison, outcome, and study design) framework. The population of interest was adult subjects (≥18 years) diagnosed with inflammatory bowel disease (IBD) undergoing any type of bariatric surgery. Comparison was made to patients without IBD undergoing bariatric surgery.
Our primary outcome aimed to assess procedural safety, while secondary outcomes evaluated procedural efficacy regarding anthropometric outcomes, IBD disease course, and nutritional outcomes. All observational and comparative studies enrolling >5 adult patients were eligible, while case reports, abstracts, letters, narrative, or systematic reviews were excluded. Due to scarcity of literature covering this topic, we planned to evaluate both observational and comparative studies with independent analysis according to study type. Ethics board review was not required for this study.
Search Strategy
The medical librarian (JK) developed and executed comprehensive searches in Ovid MEDLINE, Ovid Embase, Scopus, Web of Science Core Collection, and Cochrane Library (via Wiley) on November 2, 2021. To capture all relevant literature on the effectiveness and challenges of bariatric surgery in patients with inflammatory bowel disease, relevant keywords and controlled vocabulary were carefully selected. No language or date limits were applied. Refer to the appendices for full-text search strategies.
A total of 2703 results were retrieved and after deduplication, 1495 unique results remained for the initial title and abstract screening using Covidence (www.covidence.org), a web-based tool. In addition to subscription databases, the research team evaluated the first 200 results in Google Scholar for inclusion, which has been demonstrated to be a reasonable number of results to screen since there is high overlap between Web of Science and Google Scholar. 13 Bibliographies from included studies were also reviewed.
Study Inclusion Criteria and Definition of Outcomes
Inclusion criteria was defined as studies evaluating >5 patients who are ≥18 years old, diagnosed with IBD, and undergoing bariatric surgery. Animal studies, duplicate studies, studies published solely as abstracts, and studies that did not evaluate our primary outcomes were excluded. Non-English studies were excluded due to limited translation services access and animal studies were excluded due to unclear clinical relevance. Titles and abstracts were screened by 1 author (HW), and 2 authors (HW and VM) subsequently screened full text articles. Discrepancies were resolved by consensus. Outcomes were determined following inclusion of studies in order to ensure that all reported and relevant outcomes were assessed. Pertinent data was collected from selected trials using an excel spreadsheet by one reviewer (HW) and verified by independent extraction by a second reviewer (VM).
Our primary outcome was postoperative complications, defined by the Clavien-Dindo Classification as Grade III or higher where an adequate description was available to assess the severity of the complications. 14 Where Clavien-Dindo outcomes were not explicitly provided within included studies, the authors extrapolated this data by consensus. Length of hospital stay, rates of readmission and reoperation, and mortality were also reported.
Secondary outcomes included changes in anthropometrics, IBD disease control and IBD therapy. Anthropometric data included percentage of excess weight loss (EWL) and change in body mass index (BMI). IBD disease control was described using the following categories: presence of acute flare or IBD related complication in the postoperative period and changes in IBD related symptoms. Changes in IBD therapy included escalation, de-escalation and maintenance of preoperative medications.
Statistical Analysis
As discussed above, due to inclusion of both observation and comparative studies, we report data independently for observational studies, comparative studies, and all studies combined. Descriptive categorical data were expressed as percentages and continuous data were expressed as weighted means where appropriate. Medians were converted to means using the formula by Hozo et al. 15 Meta-analysis was used to evaluate the risk of postoperative complications between cohorts. Estimated effects were calculated using RevMan 5.4.1 software with a Mantel-Haenszel random-effects model. Heterogeneity was quantified by the I2 statistic: (1) low = 25%; (2) moderate = 50%; and (3) high = 75%. 16 Tests for statistical significance were 2-tailed with significant p-values defined as <0.05 a priori.
Risk of Bias Assessment
Assessment of study bias was performed by 2 authors (HW and KV), with disagreements resolved by third-party (VM). Non-randomized studies were assessed for quality using the Methodological Index for Non-Randomized Studies (MINORS). 17 This validated index is used for non-randomized comparative studies and consists of 12 items that are each scored as 0 when not reported, 1 for reported but inadequate, and 2 for reported and adequate. 16 Using MINORS, non-comparative scores can be assessed as: 0 to 4 = very low quality; 5 to 8 = low quality; 9 to 12 = moderate quality; and 13 to 16 = high quality. Comparative study scores can be assessed as: 0 to 6 = very low quality; 7 to 12 = low quality; 13 to 18 = moderate quality; and 19 to 24 = high quality (25). 15
Results
Study Selection
Initial literature search yielded 2703 articles. After initial screening of titles and abstracts, 17 studies underwent full-text assessment for eligibility. There were 11 manuscripts18-28 that met all inclusion criteria (Figure 1). The included manuscripts consisted of 6 retrospective cohort studies, 4 retrospective observational studies, and one prospective descriptive study summarized in Table 1. Of those, 3 were included in the meta-analysis.20,22,28
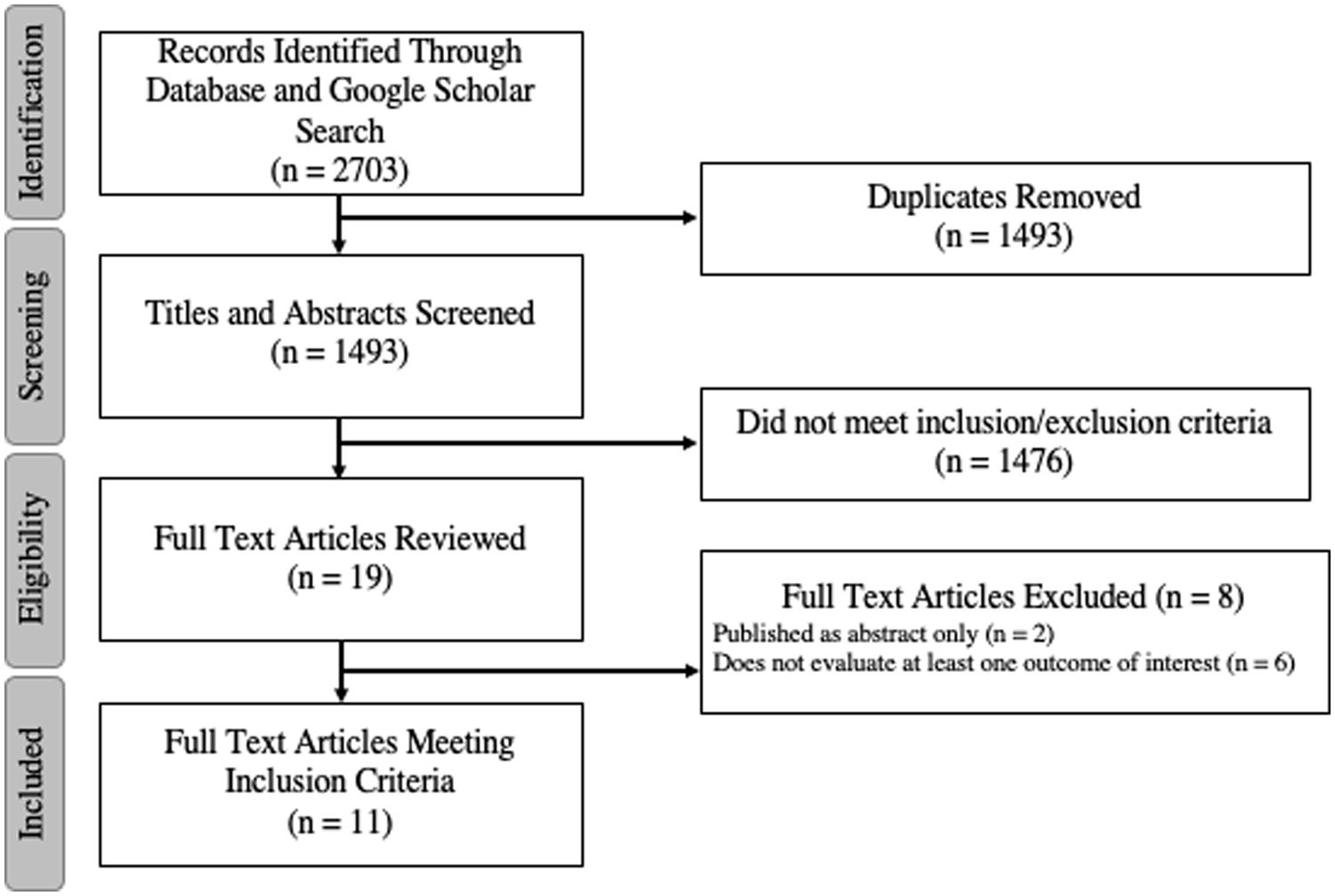
PRISMA diagram of included studies.
Summary of Included Studies.
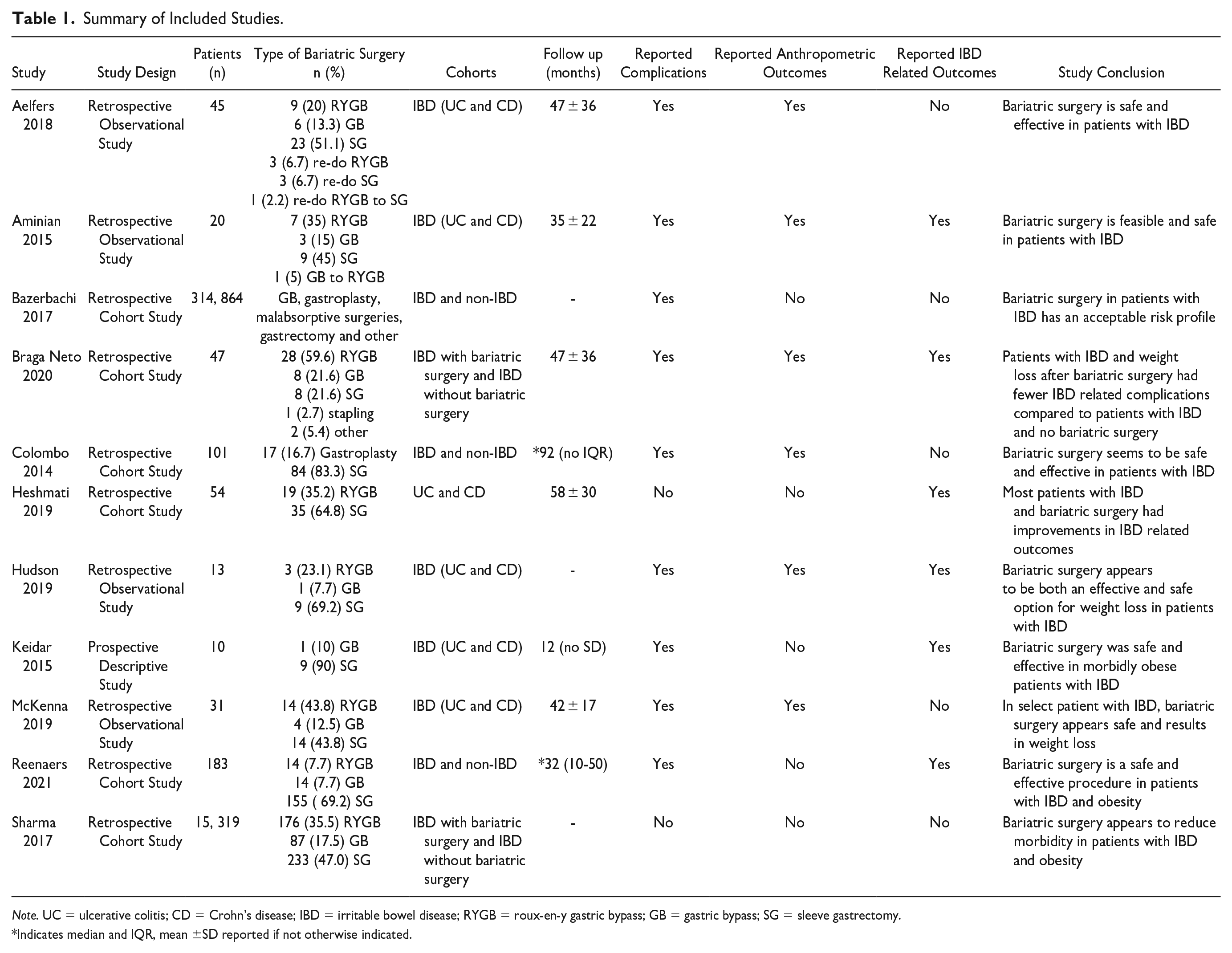
Note. UC = ulcerative colitis; CD = Crohn’s disease; IBD = irritable bowel disease; RYGB = roux-en-y gastric bypass; GB = gastric bypass; SG = sleeve gastrectomy.
Indicates median and IQR, mean ±SD reported if not otherwise indicated.
Baseline Demographics of Study Population
A total of 330 687 patients were identified within the 11 studies included (Table 2). Within all included studies (comparative and observational) there were 1595 patients with IBD. Patients had a mean weighted age of 46.0, with a female predominance (n = 1287, 80.7%). The mean duration of follow up was 39.7 months.
Demographics of Included Patients.
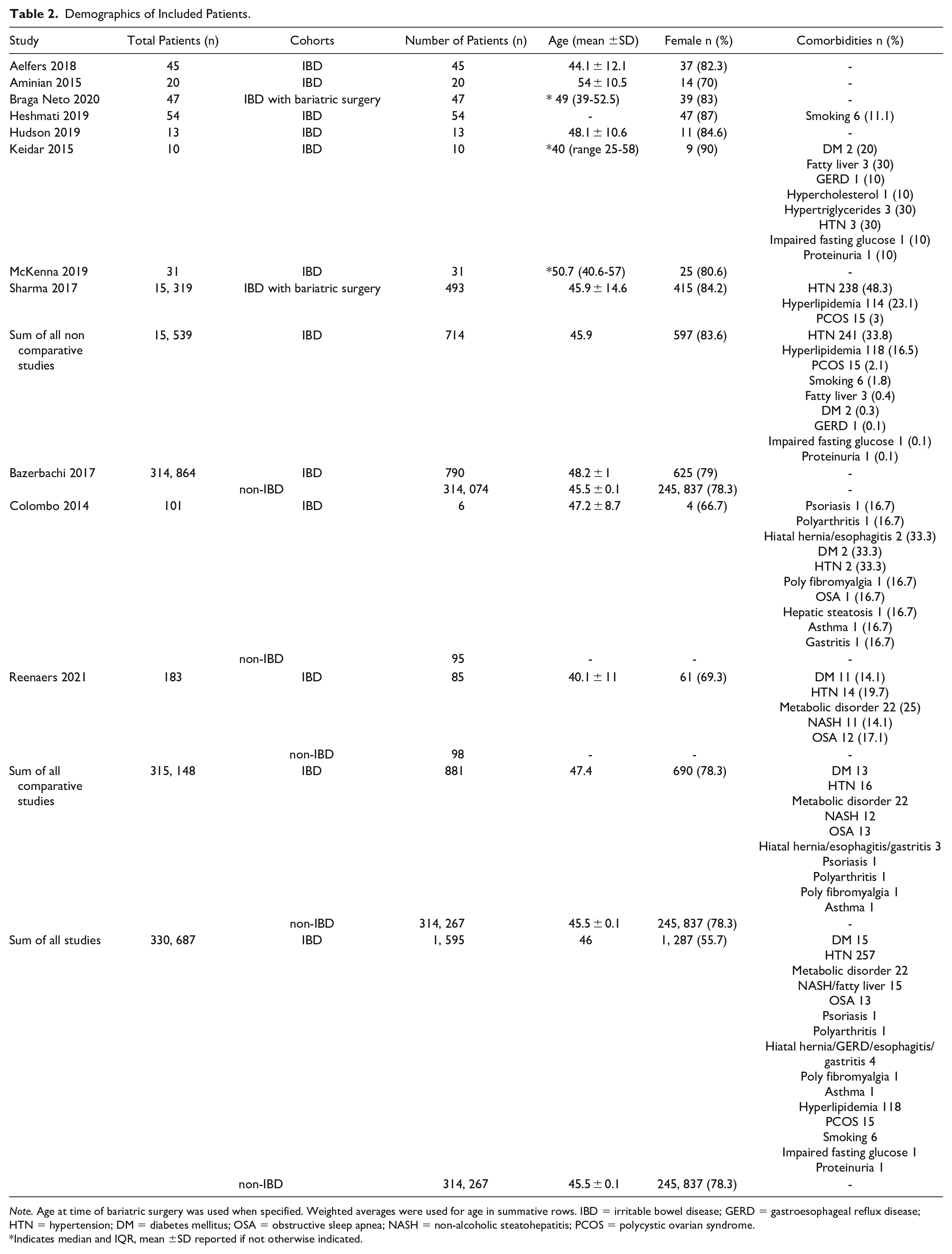
Note. Age at time of bariatric surgery was used when specified. Weighted averages were used for age in summative rows. IBD = irritable bowel disease; GERD = gastroesophageal reflux disease; HTN = hypertension; DM = diabetes mellitus; OSA = obstructive sleep apnea; NASH = non-alcoholic steatohepatitis; PCOS = polycystic ovarian syndrome.
Indicates median and IQR, mean ±SD reported if not otherwise indicated.
Within the studies directly comparing IBD and non-IBD patients (n = 3 studies) there were 881 patients with IBD and 314 267 without.20,22,28 Demographics of included patients were similar for both age (47.4 years in the IBD cohort vs 45.5 years in the non-IBD cohort) and female predominance (78.3% in both cohorts). The 3 most common types of bariatric surgery performed in the IBD cohort was sleeve gastrectomy (n = 579, 57.8%), Roux-en-Y gastric bypass (n = 270, 27%), other bypass (n = 124, 12.4%) (Table 1). The types of bariatric surgery performed in the non-IBD cohort were not provided by the included articles.
Evaluation of demographics for patients with IBD within both observational and comparative studies reported similar patient ages (45.9 years for observational studies and 47.4 years for comparative studies). Female predominance was also similar between both types of studies (n = 597, 83.6% observational vs n = 690, 78.3% comparative). Patients with Ulcerative Colitis (UC) comprised 44.1% of patients, patients with Crohn’s Disease (CD) accounted for 55.4% of patients and the remaining 0.5% of patients had indeterminate IBD (n = 704, 883 and 8, respectively). From the 5 studies that reported patient comorbidities, the most common comorbidities in participants with IBD included hypertension (n = 257), metabolic disorder (n = 22) diabetes mellitus (n = 15) non-alcoholic steatohepatitis/fatty liver (n = 15) and hyperlipidemia (n = 15).
Meta-Analysis and Pooled Postoperative Complications and Safety Outcomes for Patients With and Without IBD
Meta-analysis revealed that IBD was associated with increased rates of postoperative complications (RR 2.14; 95% CI 1.87-2.44; P < .00001; 3 studies20,22,28,I2 = 0%) in comparison to controls without IBD (Figure 2).
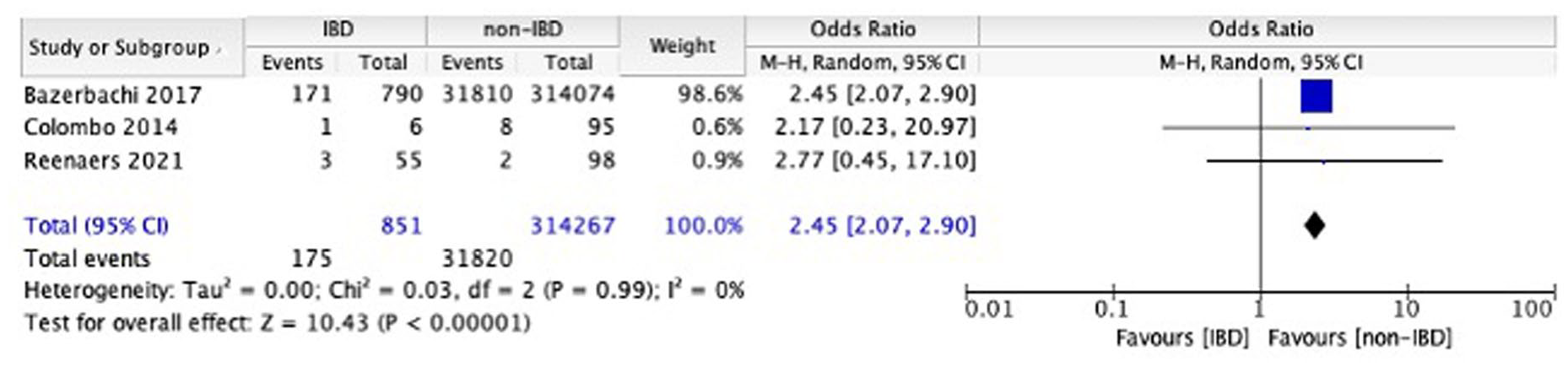
Meta-analysis of complications in IBD versus Non-IBD patients undergoing bariatric surgery.
The rate of pooled postoperative complications was also nearly twice as high in participants with IBD compared to controls (20.2% in patients with IBD vs 10.1% in patients without IBD). Substantial contributors to the difference in complications between cohorts included that patients with IBD were more likely to require reoperation and readmission (n = 17, 7.9% and n = 14, 6.7% respectively) compared to the non-IBD cohort (n = 5, 2.6% and n = 3, 3.1% respectively).
With regards to other complications, the mortality rate in both cohorts was very low with an IBD cohort mortality of 0.1% versus a mortality of 0.25% in the non-IBD cohort (Table 3). The mean length of hospital stay was the same in both cohorts when all studies were included (2.5 days). Rates of specific complications were not described for the non-IBD cohort. From the studies that reported rates of specific complications in the IBD cohort, 8.3% (n = 8) of participants were reported to experience dehydration, 7.1% (n = 60) had a small bowel obstruction and 5.4% (n = 6) had an incisional hernia. Anastomotic complications and wound infections occurred at a rate of 1.7% (n = 14) and 1.5% (n = 13) of participants with IBD, respectively.
Outcomes of Included Studies.
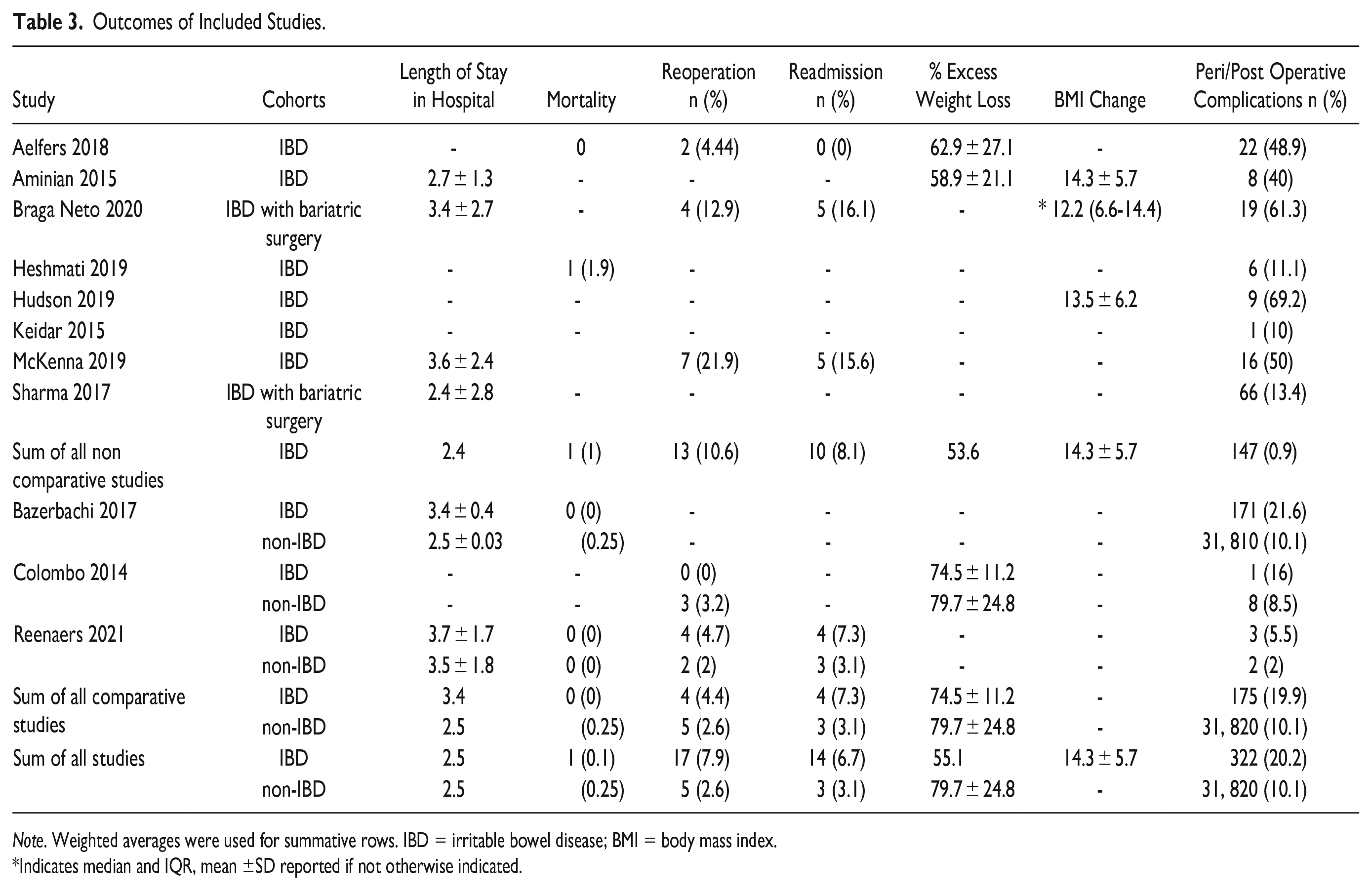
Note. Weighted averages were used for summative rows. IBD = irritable bowel disease; BMI = body mass index.
Indicates median and IQR, mean ±SD reported if not otherwise indicated.
Complications were separated by UC and CD in 7 studies.18,19,21,23-25,27 Of the 27 complications described, there were 16 (59.3%) complications reported in patients with UC and 11 (40.7%) in patients with CD. Complications for patients with UC included 3 reoperations (18.8%), 3 anastomotic leaks (18.8%), 3 small bowel obstructions (18.8%), 2 wound infections (12.5%), 2 incisional hernias (12.5%), one stricture (6.3%), one reversal (6.3%) and one incisional drainage (6.3%). Complications for patients with CD included 5 reoperations (45.5%), 4 incisional hernias (36.4%), one anastomotic leak (9.1%) and one bleed requiring an endoscopic clip (9.1%).
Bariatric Surgery and Nutritional Complications in Patients With and Without IBD 3.4
Reenaers et al. 27 was the only comparative study to report differences in postoperative nutritional deficiencies between patients with and without IBD (Table 4). Patients with IBD had higher rates of anemia (n = 4, 10.5% in patients with IBD vs n = 4, 8% in patients without IBD) and Vitamin B12 deficiency (n = 7, 25.9% in patients with IBD vs n = 2, 5.4% in patients without IBD). Patients without IBD were found to have higher rates of low ferritin levels (n = 4, 9.3%) compared to patients with IBD (n = 0, 0%). There were 2 studies that reported rates of nutritional deficiencies in patients with IBD post bariatric surgery and found that 16 patients (30.8%) developed iron deficiency, 6 had Vitamin B12 deficiency (10%) and 17 developed Vitamin D deficiency (34%).23,25
Impact of Bariatric Surgery on IBD and IBD Therapy.
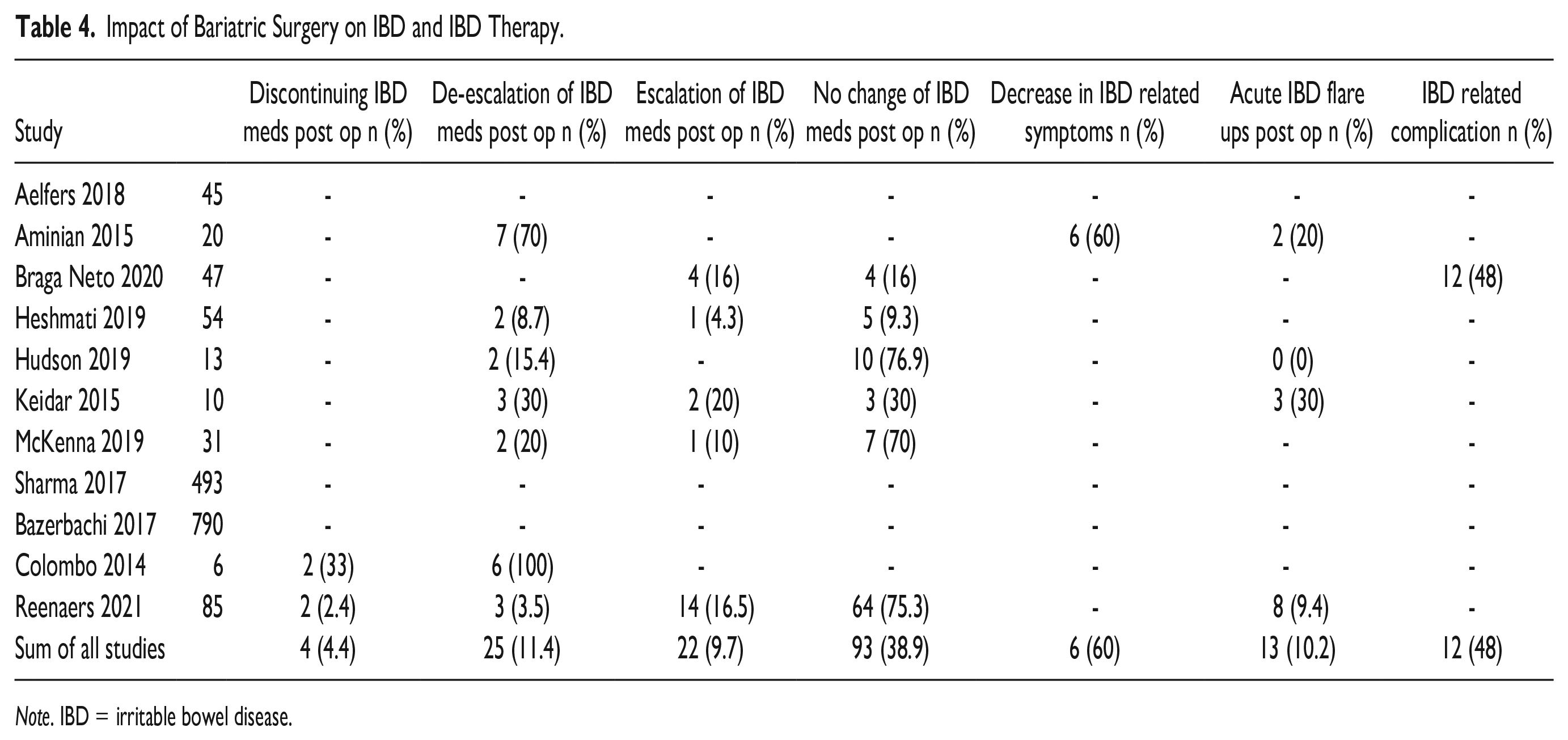
Note. IBD = irritable bowel disease.
Anthropometric Outcomes
Anthropometric outcomes were only reported in non-comparative studies evaluating only patients with IBD, limiting the ability to complete meta-analysis. The percentage of excess weight loss (EWL) was reported by 4 non comparative studies18-20,24, one comparative study 20 (Table 3). The weighted mean percentage of EWL in those 5 studies for the IBD cohort was 55.1%. In the single comparative study reporting this outcome, the IBD cohort lost 74.5 ± 11.2% of EWL, compared to 79.7% ± 24.8% for the non-IBD cohort. Aminian et al. 19 was the only study to report the change in body mass index (BMI) after bariatric surgery in their cohort of IBD patients, which was 14.3 ± 5.7 kg/m2.
Impact of Bariatric Surgery on IBD and IBD Therapy
Of the 11 included studies, 8 reported outcomes related to IBD and IBD therapy.19,21-27 For postoperative IBD medication use, 4.4% (n = 4) of participants discontinued their IBD medications completely, and 11.4% (n = 25) were able to de-escalate their medications. Escalation of IBD medications was reported in 9.7% (n = 22) of participants and 38.9% (n = 93) had no change in their IBD medications. Additionally, 10.2% (n = 13) of participants experienced acute IBD flare postoperatively. Aminian et al 18 was the only study to report a change in IBD related symptoms postoperatively, and found that 60% (n = 6) of participants had a decrease in their IBD related symptoms. Braga Neto et al. 21 was the only study that evaluated IBD related complications after surgery and reported occurrence of this in 48% (n = 12) of their participants.
Risk of Bias for Included Studies
The 11 non-randomized studies were assessed for bias and methodology using the Methodological index for non-randomized studies (MINORS) criteria (Supplemental Table 1). Of the 5 non-comparative studies, 4 were scored as low quality18,19,24,26, one was scored as moderate quality. 27 All 6 of the 6 comparative studies were scored as moderate quality.20-23,27,28 No study met ideal criteria as all studies lacked a prospective calculation of study size and only one study collected data prospectively. 25 Due to the retrospective nature of the majority of studies, 8 of the studies received a score of zero on reporting loss to follow up. Further, 4 of the 6 comparative studies noted small differences in baseline characteristics between cohorts.
Discussion
This study is the first systematic review and meta-analysis to characterize and evaluate safety and efficacy of bariatric surgery in patients with IBD as well as evaluating the potential of bariatric surgery as an IBD disease course modifier. Our meta-analysis findings demonstrate that there is a significantly higher odds of complications related to bariatric surgery in patients with IBD compared to those without. Despite higher postoperative complications, results continue to display beneficial anthropometric outcomes in patients with IBD providing support for efficacy in this cohort as a durable weight-loss procedure. The degree to which bariatric surgery modifies IBD disease course, however, remains unclear and warrants further evaluation.
There are several potential explanations for why we found substantially increased postoperative complications following bariatric surgery in patients with IBD compared to without. Use of steroids, chronic inflammation, previous operations causing subsequent adhesions, and risk of bowel obstructions and strictures may all contribute to the increased rate of complications in the IBD cohort, as these are factors are more common in patients with IBD than the general population.29-32 Chronic immunosuppression from steroids, from example, has been associated with increased postoperative infections, bleeds and anastomotic leaks. 29 The most common cause of small bowel obstructions is adhesions, which are most often formed from a previous surgery. 30 Given that patients with IBD are more likely to have had a previous bowel surgery compared to patients without, these patients are at a higher risk of having pre-existing adhesions. 31 Patients with IBD at baseline are more prone to structural complications including bowel obstructions, and that risk may be further increased following bariatric surgery. 32 The long-term nutritional outcomes were not well described in the included studies, and this is an important consideration for any patient undergoing metabolic surgery as studies demonstrate that poor-pre-operative nutritional status or sarcopenia are associated with adverse serious complications. Overall, due to the underlying diseased state in patients with IBD these findings are not surprising, however, this information will be crucial to inform operative decisions in this patient cohort as an increasing proportion develop obesity and its related complications.
Other studies have demonstrated similar rates of complications in patients with IBD who undergo bariatric surgery. A systematic review by Shoar et al. 33 found that rates of excess weight loss were over 70%, but reported rates of both early and late postoperative complications exceeding 20%. They found that IBD remitted in almost half of patients, which was higher than our results of 11%. Mian and Khan 34 also conducted a systematic review and had similar findings; bariatric surgery is effective for weight loss in patients with IBD but these patients also have a higher rate of complications and increased length of hospital stay compared to patients without IBD. Finally, Aziz et al. 35 conducted a systematic review and meta-analysis on complications for patients with IBD following bariatric surgery using pooled proportions. They found that rates of Clavien-Dindo Classification Grade III or greater was 2%, which was much lower than our finding of 20%. These differences may be due to a variety of factors, including technical reasons, or, more likely, that their method of tracking complications may have been limited due to loss of follow up, and inability to robustly capture all complications such as dehydration, readmission, and wound infections. Additionally, pooled proportion meta-analyses are less robust than relative risk analyses due to their inherent statistical assumptions. These previous reviews remain limited in that they lack a direct comparison group that we have provided in this study, as well as not evaluating the potential for bariatric surgery to be an IBD disease course modifier.
Our findings suggest that although bariatric surgery is effective for weight loss in this cohort, there is no strong evidence for de-escalation of IBD therapy. As excess adipose tissue is thought to secrete proinflammatory adipokines and cytokines, it would be reasonable to suspect that loss of excess body weight in patients with IBD through bariatric surgery would reduce overall inflammation and therefore improve disease control. 36 The general reduction of adipose tissue may lead to improved disease control in a subset of patients with IBD, but this cannot fully explain the large proportion of patients that did not have any change in their IBD therapy after bariatric surgery. However, as we found that 16% of participants with IBD included in this analysis were able to de-escalate their medications or stop them completely after bariatric surgery, this may be an area of research that warrants further investigation. Another area worthy of further research involves identifying the optimal bariatric procedure for this patient population as more complex malabsorptive procedures are inherently associated with an increased peri-operative risk at the cost of producing a potentially more robust and durable anti-inflammatory response.
Although these data offer insights into the outcomes of bariatric surgery in patients with IBD, important limitations should be recognized. First, studies evaluating bariatric surgery in patients with IBD are limited and only 3 studies were available for meta-analysis. As there was inadequate reporting of anthropometric outcomes in the non-IBD cohort to perform a meta-analysis, only the rate of postoperative complications could be included in this portion of the review. Additionally, most studies were evaluated as low quality and only one of the studies included prospective data collection. This highlights the need for improved high quality, prospective studies evaluating these patients. The majority of studies did not describe the baseline comorbidities of their cohorts, making it difficult to effectively generalize findings to the appropriate patient population. Additionally, 4 of the 6 cohort studies identified at least one difference in the baseline characteristics of their cohorts. Further, most studies did not thoroughly describe their postoperative complications, making it challenging to classify them using the Clavien-Dindo Classification, specifically in the non-IBD cohort. Additionally, only a small subset of complications were described as occurring in patients with UC or CD. Therefore, for our main analysis we grouped these patients together, acknowledging that the 2 groups have different treatments and disease courses. As the types of bariatric surgery performed were not described in the non-IBD cohort, we are unable to comment on the influence that specific procedures have on our results. Where bariatric procedures were characterized, no procedure-specific outcomes were provided limiting our ability to conduct procedure-specific meta-analysis. We also couldn’t adjust or control for prior surgeries, which may have influenced the increased postoperative complications found in the IBD group. Furthermore, we were unable to adjust for the varying types of IBD disease modifying pharmacotherapy, which may have also played a role in the response to bariatric surgery. Lastly, given the nature of our study design, we are not able to describe the specific mechanisms responsible for our findings.
As metabolic surgery in patients with IBD is a relatively new and controversial field, it is to be expected that the data is as biased and limited as it is, which highlights the importance of our findings. Our study emphasizes current limitations and provides a framework from which to build future studies, which is valuable as there is a growing population of patients with IBD and concurrent severe obesity pursuing metabolic surgery as a viable weight loss option. Although we are unable to comment on the effects of specific types of bariatric surgery, we would typically expect the non-IBD population to have an even higher proportion of anastomotic procedures which carry a much higher morbidity and mortality, meaning that our finding of an increased odds of serious complications in the IBD cohort is even more important. Lastly, anthropometric measures, while a key aim of metabolic procedures are actually quite limited in their global reporting and reporting standards have only recently been introduced. 37
Despite these limitations, our study is the first comparative systematic review and meta-analysis to explore the relatively novel concept of bariatric surgery outcomes in the context of concurrent IBD. While overall surgical risk does appear higher, the overall rates of complications for bariatric surgery for all comers is low. That together with the potential signal for reduction in overall need for IBD medication suggests that bariatric surgery may have an acceptable risk profile in these patients, but discussing these findings with patients preoperatively is important. Further research investigating surgical outcomes in patients with IBD undergoing bariatric surgery is needed to better delineate the role of bariatric procedures within this growing population.
Conclusion
While bariatric surgery presents an effective weight loss option for patients with IBD, these patients are associated with higher rates of postoperative complications. An overall trend toward reduction in need for IBD medication post bariatric surgery was observed suggesting a correlation between metabolic control and IBD disease course. Together, this work highlights the need to better delineate the effect of bariatric procedures for patients with IBD with respect to both metabolic and IBD-related outcomes.
Supplemental Material
sj-docx-1-gut-10.1177_26345161231185780 – Supplemental material for Safety and Outcomes of Bariatric Surgery in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-gut-10.1177_26345161231185780 for Safety and Outcomes of Bariatric Surgery in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis by Hillary Wilson, Kevin Verhoeff, Jerry Dang, Janice Y. Kung, Noah J. Switzer, Daniel Birch, Karen Madsen, Shahzeer Karmali and Valentin Mocanu in Foregut
Supplemental Material
sj-docx-2-gut-10.1177_26345161231185780 – Supplemental material for Safety and Outcomes of Bariatric Surgery in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-gut-10.1177_26345161231185780 for Safety and Outcomes of Bariatric Surgery in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis by Hillary Wilson, Kevin Verhoeff, Jerry Dang, Janice Y. Kung, Noah J. Switzer, Daniel Birch, Karen Madsen, Shahzeer Karmali and Valentin Mocanu in Foregut
Supplemental Material
sj-pptx-3-gut-10.1177_26345161231185780 – Supplemental material for Safety and Outcomes of Bariatric Surgery in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis
Supplemental material, sj-pptx-3-gut-10.1177_26345161231185780 for Safety and Outcomes of Bariatric Surgery in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis by Hillary Wilson, Kevin Verhoeff, Jerry Dang, Janice Y. Kung, Noah J. Switzer, Daniel Birch, Karen Madsen, Shahzeer Karmali and Valentin Mocanu in Foregut
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent:
For this type of study formal consent is not required. All procedures performed that contributed to the data registry were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.