
Abstract
Background:
Esophageal dysmotility is common after esophageal atresia (EA) repair. Esophageal manometry (HRM) is the gold standard to investigate motility. We aim to characterize esophageal dysmotility and bolus transit for liquid and solids in children with repaired EA.
Method:
Retrospective analysis of HRM from children with repaired EA. Five liquid and 5 solid swallows per child were assessed for the standard manometric measurement and peristalsis pattern. Impedance tracings were used to assess bolus transit.
Results:
Ninety measurements were assessed from 9 patients, 44% Females. Mean age was 10.5 (±4.6) years. All children had dysphagia and anastomotic strictures were excluded. None of the children had intact peristalsis, 44.4% of the liquid swallows were failed, 33.3% fragmented and 22.2% ineffective. 44.4% of the solid swallows were failed, 44.4% fragmented and 11.1% ineffective. 33.3% had incomplete bolus transit in the whole esophagus, 44.4% in the upper and 11% in the lower esophagus. Mean peristalsis break for liquid was 7 cm (±2.1) and for solid was 5.9 cm (±3.2) P .025.
Conclusion:
Impaired esophageal motility is universal post EA repair. Failed and ineffective peristalsis predominate with incomplete bolus transit and large peristalsis breaks after liquid and solid swallows. HRM can provide clinical guidance, diagnostic and prognostic information post EA repair.
Key Learning Points
Abnormal esophageal motility is common post EA repair
Contractility of liquid and solid bolus swallows were similarly affected, and Incomplete bolus clearance involved the proximal esophagus in the majority of cases
HRM can provide essential guidance for the clinical care of post EA repair
Introduction
Esophageal atresia (EA) is a common congenital malformation of the esophagus with a stable worldwide prevalence. 1 Due to the advances in surgical techniques combined with improved pre and post-operative care, the outcome of repaired EA is improving and most children are expected to reach advanced adulthood, albeit with associated gastrointestinal and respiratory morbidity burdens. 2 Gastroesophageal reflux, feeding difficulties, dysphagia and recurrent aspiration are common and can adversely affect the quality of life for children and their families. 3
Other types of esophageal motor disorders have also been described in children post EA repair by using standard esophageal manometry and multi-channel intraluminal impedance. The use of high resolution esophageal manometry (HRM) has allowed improved characterization and classification of different types of esophageal dysmotility. Peristalsis integrity and a range of distal contractile patterns have been accurately described and documented since the development and the wider use of HRM. 4 Normal values and result interpretation in adults are based on plethora of evidence 5 but normative values in pediatric HRM are often based on small cohort studies.6-8 In one pediatric study, all children with repaired EA were reported to have had an abnormal HRM findings. 9
Impaired motility can lead to abnormal transit in the esophageal body and/or incomplete bolus clearance (IBC). Although the exact role of IBC in the pathogenesis of esophageal disorders is poorly understood, IBC is often described in patients with gastroesophageal reflux disease, directly impacting quality of life and delayed bolus clearance is commonly associated with erosive esophagitis and Barret’s esophagus. 10 However, the difference between liquid and solid bolus transit across the esophageal body and the presence of IBC in children with EA has not been previously reported.
The topographic visualization of HRM can permit accurate assessment of contraction patterns and measurement of breaks in the isobaric contour. Small breaks are often seen in asymptomatic healthy individuals but large breaks are common in patients with dysphagia, prolonged acid exposure and other esophageal symptoms.11,12 Recently, breaks in contraction integrity have been described as a predictor of incomplete bolus transit in healthy volunteers. 11
In this study, we aim to characterize the patterns of esophageal motility and bolus transit for liquids and solids in children with repaired EA. Understanding these patterns can provide valuable insights into the management and treatment of EA-related complications, ultimately improving the quality of life for affected children and their families.
The study was registered with our institution’s clinical governance team and a full ethic review was not required.
Methods
A retrospective review of all children with repaired EA who had undergone a HRM at Evelina London Children’s Hospital between June 2017 and June 2021.
Data was collected using a combined solid state manometry and impedance catheter, with either 36 or 25 (based on the child’s size) unidirectional pressure sensors spaced at 1 cm intervals and 12 impedance sensors spaced at 2 cm intervals (Laborie©, formerly MMS, Enschede, The Netherlands). Patients were fasted for 4 hours prior to the procedure and medications affecting gastrointestinal motility were stopped between 24 hours and 7 days prior to the procedure, to ensure the data collected was a true representation of the physiological state. The catheter was passed trans-nasally, positioned with at least 2 sensors in the stomach and the pharyngeal contraction visualized. Patients were placed in a semi-recumbent position and given a period of time to acclimatize to the catheter. Patients were then asked to swallow 5 mL of oral rehydration solution up to 10 times and then eat a solid food of their choice (often a sandwich) with a minimum of 5 bites. All data collected was manually analyzed post-procedure using MMS Database (v9.5; MMS). For pediatrics normal values, we have used a previously published data.6-8
Bolus transit was assessed using the impedance contour traces to visualize where the bolus remained in the esophageal body either post-peristalsis where present, or post-lower esophageal sphincter (LES) closure where peristalsis failed. IBC was defined as bolus (liquid or solid) entry without bolus clearance at any of the impedance recording sites and is divided into upper, lower and whole failure, dependent on area of incomplete clearance within the esophageal body. 13 Patients were regarded as having IBC if >30% of the swallows had incomplete clearance. An example of incomplete bolus transit with peristalsis present is included in Figure 1. Five representative wet swallows and 5 representative solid swallows were identified for each patient following identification of bolus transit.

Examples of bolus transit across the esophageal body: (A) incomplete bolus transit in the whole esophagus, (B) incomplete bolus transit in the upper esophagus, and (C) incomplete bolus transit in the lower esophagus.
The Integrated Relaxation Pressure (IRP), Distal Latency (DL), Distal contractile integral (DCI) were recorded, analyzing the quality of the peristaltic contractions. Location of the IBC within the esophageal body was also recorded. Peristalsis breaks were reported by measuring the vertical length of the isobaric contraction contours. Peristaltic contractions were defined (when at least 50% of the contractions were affected) as “Failed” when the DCI was <100 mmHg, as “Ineffective” with DCI between 100 and 450 mmHg and “Fragmented” when the DCI measured at least 450 mmHg, 5 but a large transition zone defect of the isobaric contour of 20 mmHg was identified.
Statistical analyses were performed using SPSS software (v27; IBM© SPSS, Chicago, IL, USA).
Results
Ninety swallows were collected from 9 patients (45 liquid and 45 solid swallows). Four children were female and mean age was 10.5 (±4.6) years, background information, peristalsis and bolus transit were detailed in Table 1. One child had type B, another type D EA and 3 children had VACTERAL (vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities) association. We were unable to define the exact type of EA in other children as their surgical care was at different institutions. All children had pneumatic dilatations to treat anastomotic strictures after the initial repair. All children presented with dysphagia and had undergone an upper endoscopy and contrast study to exclude anastomosis stricture prior to HRM. 44.4% of the liquid swallows were failed, 33.3% were fragmented and 22.2% were ineffective while 44.4% of the solid swallows were failed, 44.4% were fragmented and 11.1% were ineffective. Summary of IRP, DCI, DL and break size in liquid and solid swallows were detailed in Table 2.
Demographic, Peristalsis and Bolus Transit Description.
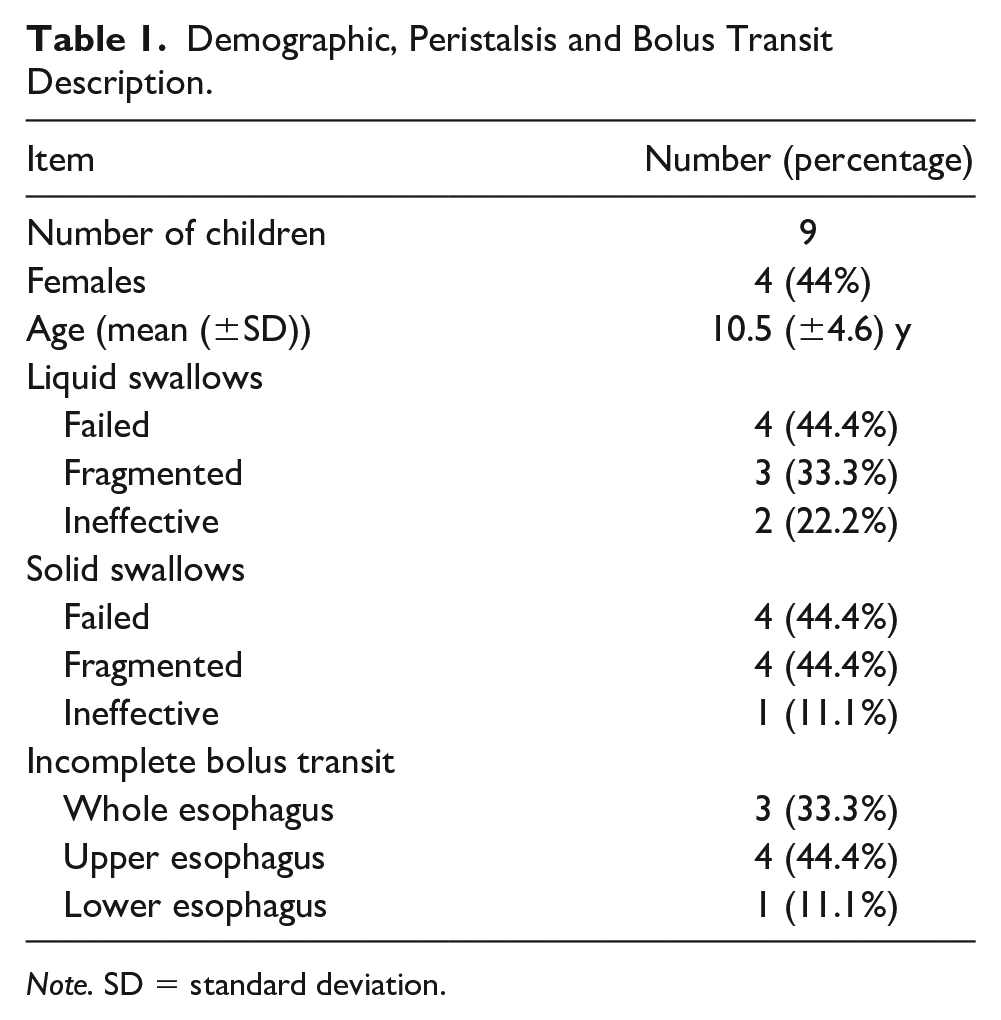
Note. SD = standard deviation.
Summary of Esophageal Manometry Findings.
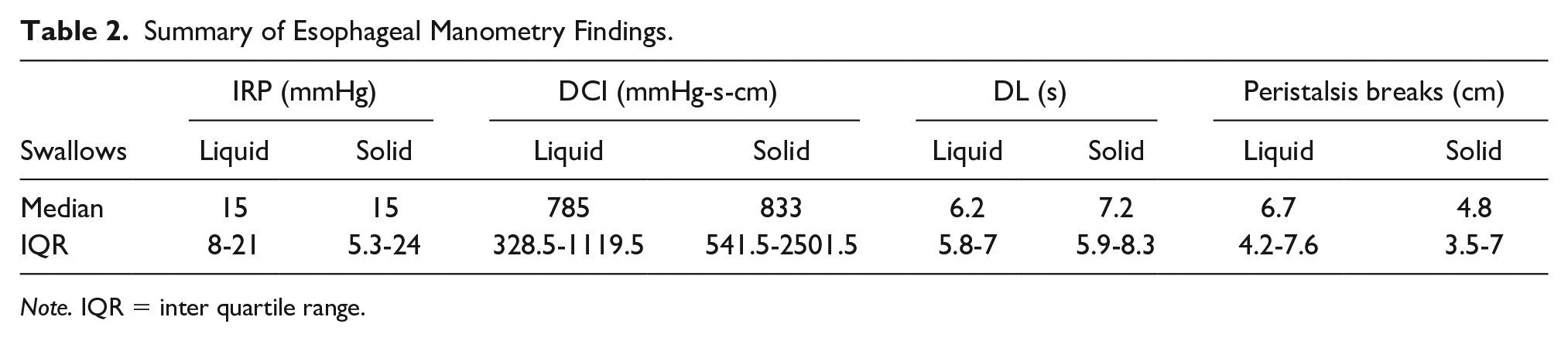
Note. IQR = inter quartile range.
IRP values based on type of contraction are displayed in Figure 2 and show higher IRP values in fragmented contractions and lowest values in the failed contractions.
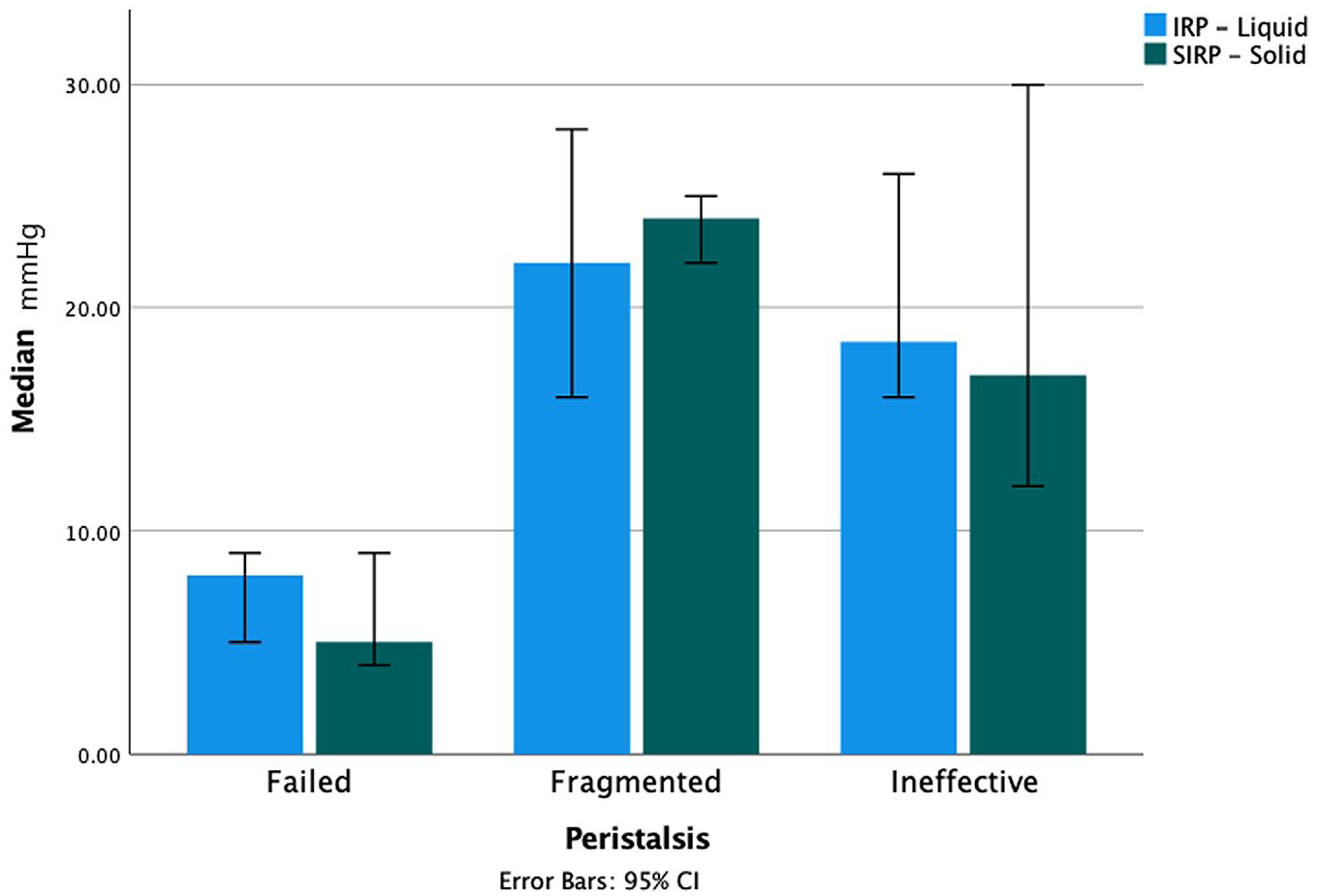
IRP values based on peristalsis type.
In this cohort, 33.3% had incomplete bolus transit in the whole esophagus, 44.4% in the upper and 11% in the lower esophagus. Figure 3 shows IRP values based on bolus clearance. IBC from the upper esophagus group appeared to have the highest IRP values, while IBC from the lower esophagus group had the lowest IRP values. There was no significant correlation demonstrated between break size and IRP during liquid swallows, but the size of the break was negatively correlated to IRP value during solid swallows (Pearson correlation = 0.61 P = .001).
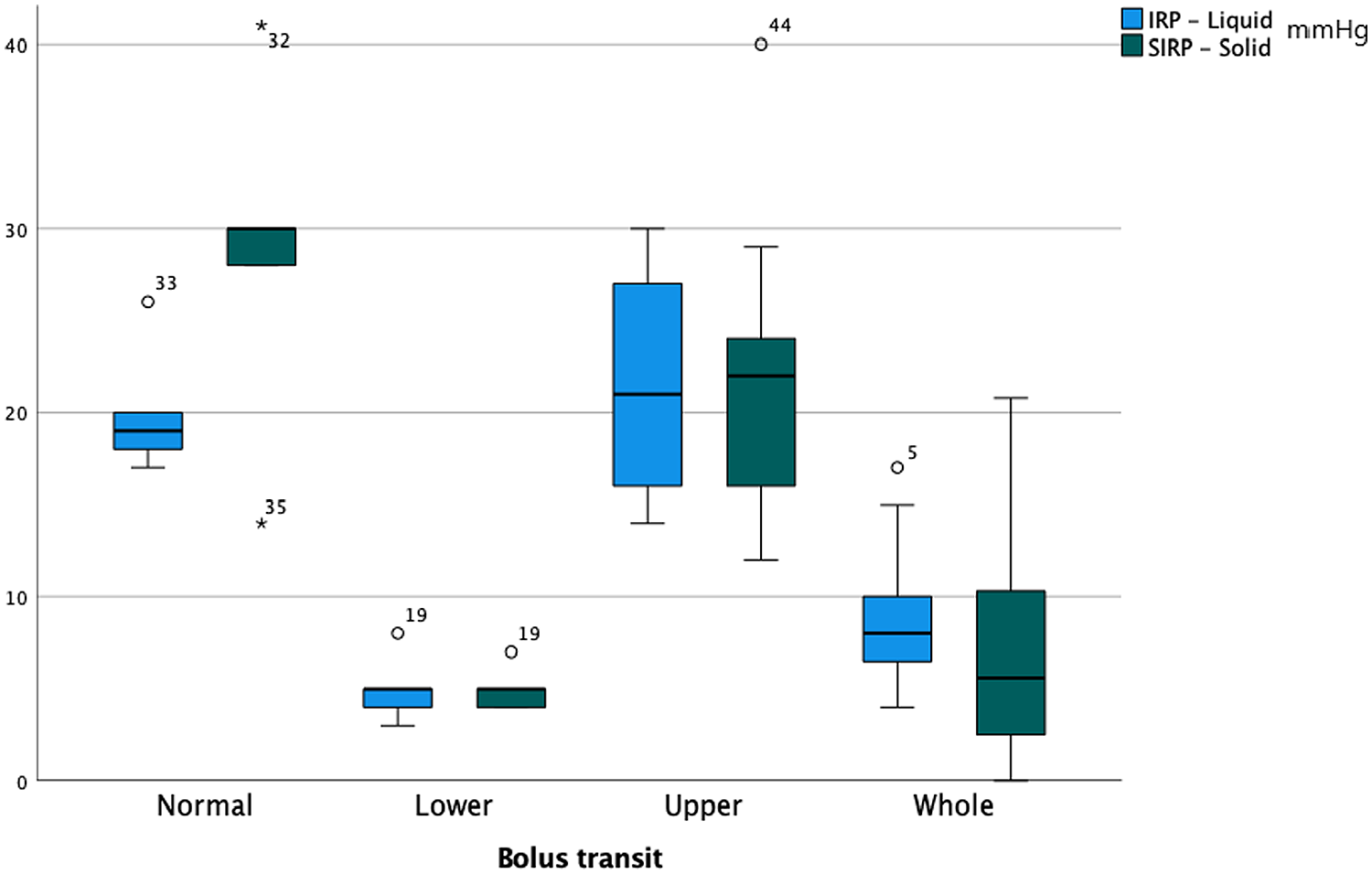
Shows IRP values based on bolus clearance.
There was a difference in the mean length of the breaks during liquid and solid swallows in the whole cohort, the mean break for liquid was 7 cm (±2.1) and for solid was 5.9 cm (±3.2) (Figure 4).
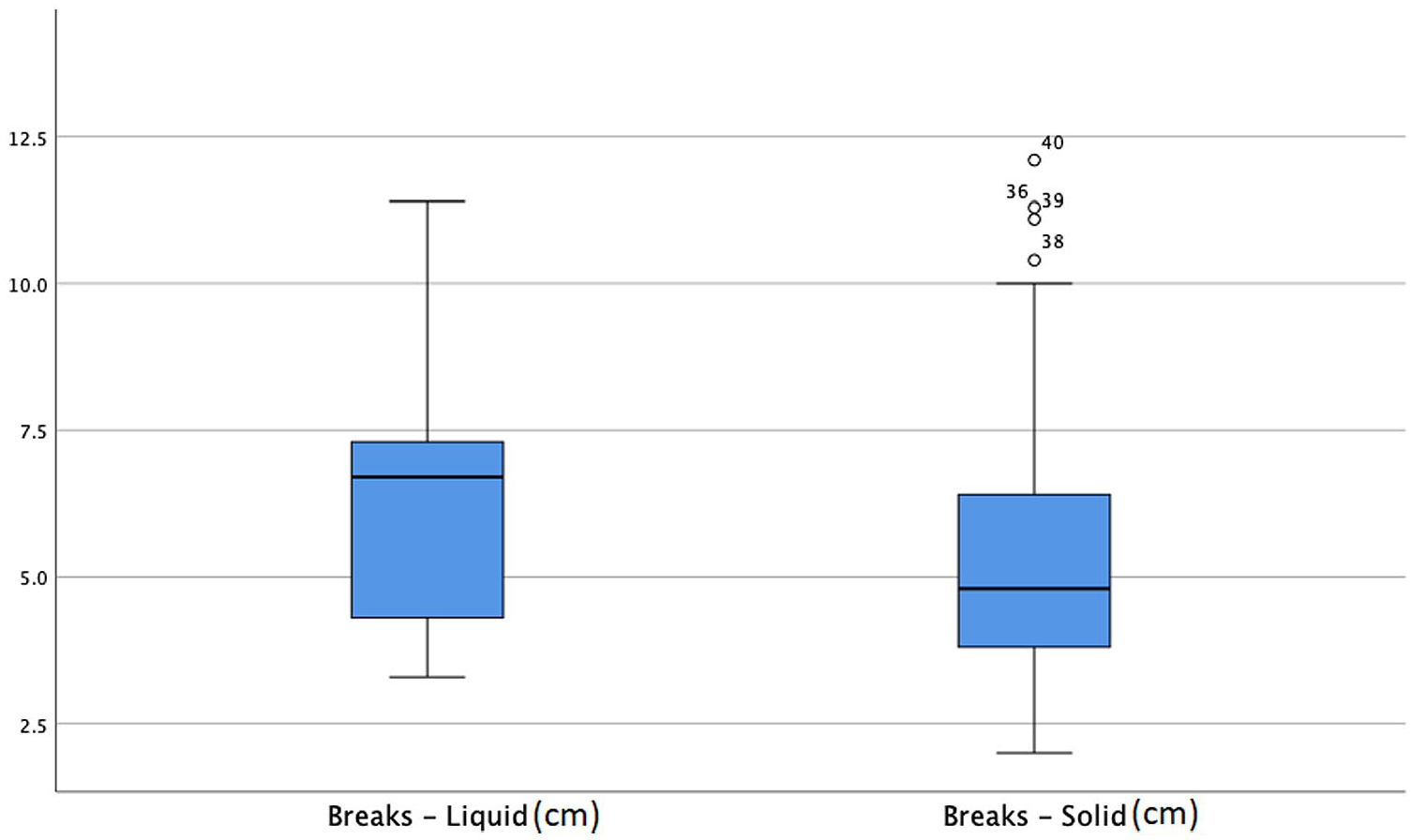
The mean length of the breaks during liquid and solid swallows in whole cohort.
Children with IBC in the lower esophagus had the lowest measured IRP. Children with IBC at the upper esophagus had above average readings with the median IRP for liquid 21 mmHg (IQR 16-27) and solid swallows 22 mmHg (IQR 16-24).
Discussion
Abnormal esophageal motility following EA repair is common and can be attributed to many factors, as arrested neuromuscular development and abnormal innervation of the esophagus may occur alongside the esophageal malformation and can lead to a variety of neurogenic and/or myogenic motor abnormalities. 14 The surgical repair of the atresia can also lead to direct damage and scar formation with the resultant esophageal dysmotility. 15
In this study, we looked at esophageal motility for liquid and solid swallows using HRM following a standard procedural protocol. All children with repaired EA who presented with dysphagia had abnormal esophageal motility patterns. Over half of the children had ineffective esophageal motility and the remaining patients had failed peristalsis with liquid swallows. Interestingly, one patient, despite having ineffective contractions, had complete bolus transit for liquid. The same child retained ineffective esophageal contractions with solids, however, we observed incomplete bolus clearance in the upper esophagus.
Dysphagia is a persistent symptom in both children and adults with repaired EA, there are many causative factors that can lead to dysphagia, including anastomotic stricture, dysmotility and inflammatory conditions such eosinophilic esophagitis. 16 Barium studies and endoscopies are regularly performed in children post EA repair, however the uptake of gastrointestinal motility investigations is sparse. In 2016, the European/North American Society of Pediatric Gastroenterology, Hepatology and Nutrition stated that pH impedance studies are useful in evaluation and correlation of symptoms to gastro esophageal reflux disease (GERD) post EA repair. 17 HRM was also thought to be useful but its impact on clinical practice was not clear at the time. Since the publication of that guidance, many studies have highlighted the value of capturing and identifying manometric abnormalities, for improved clinical care and indeed subsequent patient outcomes. However, the overall use of HRM post EA repair remains limited.
In this cohort, children with IBC in the lower esophagus had the lowest measured IRP. This suggests impaired propagation of contractions, rather than higher LES pressure, which leads to leakage of both liquid and solid at the lower esophagus. In contrast, children with IBC in the upper esophagus have had above average readings with the median IRP for liquid 21 mmHg (IQR 16-27) and solid swallows 22 mmHg (IQR 16-24). Particularly considering the large peristalsis break in both groups (liquid and solid swallows), the median break during liquid swallow being 7 cm (IQR 5.3-8.3) and for solid 4.9 cm (IQR 3.8-9.1), it is likely that the relative high pressure at the LES creates a back pressure leading to incomplete clearance in the upper esophagus. The size of the break appeared to negatively correlate with IRP in solid swallows, (Pearson correlation = 0.61 P = .001), but no direct correlation to liquid swallows was identified.
The integrity of esophageal contraction in our studied group was different when the children consumed liquid compared to solids, the length of the breaks for liquid swallows was 7 cm (±2.1) compared to 5.9 cm (±3.2) for solids (P = .025). Where the contractions failed, both groups had a low IRP, the median for liquid was 8 mmHg (IRQ 4.3-9.8) and 5 mmHg (IRQ 3.2-10) in the solid group- reflecting a major disruption to the esophageal neuromuscular function. Gravity and the minimum outlet resistance were the main factors for esophageal bolus transit in this group. Large peristalsis breaks can be associated with prolonged bolus retention, exacerbating any pre-existing esophageal symptoms,18-20 however we were unable to report difference in symptoms severity in this group, likely due to small sample size.
Failed peristalsis, the most common disorder of contractility observed in this group, is often associated with bolus retention and clinical symptoms of dysphagia and/or chest pain. The rest of the cohort had ineffective contractility. Although the recent Chicago Classification has removed fragmented peristalsis as a disorder of peristalsis due to lack of distinct clinical characteristics 5 we chose to retain this term in this cohort due to lack of evidence on the use of the standard Chicago Classification in its entirety for this small subset of children with repaired EA. The fragmentation of the contraction can reflect a degree of motor function in the lower segment of the esophagus and can present as a separate group to the generalized impaired contractility seen in the “ineffective” esophageal motility group. The contractility was also different between liquid and solid consumption, providing a potential indicator to influence ongoing clinical management.
This report has a number of limitations, the retrospective data collection and the small sample size are notable but EA is an uncommon disorder in children and HRM is not widely available in pedpediatric practice, restricting wider recruitment.
In conclusion, we described a range of esophageal motor disorders in children with repaired EA by using HRM following liquid and solid consumption. About half of the children had failed peristalsis and the rest ineffective and fragmented peristalsis. IBC is almost universal in post EA repair patients and can affect the upper, lower or entire esophagus and is also correlated with the size of peristalsis break. Relatively high IRP appears to cause a degree of outlet obstruction leading to IBC in the upper esophagus. HRM can provide valuable information to be utilized alongside more established motility investigations, to guide clinical management and prognosis in children with repaired EA, ultimately improving patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.