
Abstract
Background:
Non-obstructive dysphagia is a commonly encountered clinical problem.
Methods:
We retrospectively analyzed a single tertiary hospital system electronic database from January 2021 to October 2021 for patients undergoing EGD with dilation using ICD-10 codes 43248 and 42450.
Results:
Of the 411 patients meeting inclusion criteria, 75% of these patients had improvement with empiric dilation. The presence of a superficial mucosal tear post dilation was statistically significant.
Conclusion:
Empiric dilation is a useful tool for patients with non-obstructive dysphagia.
Introduction
Dysphagia is the term used to describe difficulty swallowing and is a common clinical concern. In a recent survey involving 30,000 individuals, nearly 16% experienced dysphagia, but only half sought treatment. 1 Dysphagia can be categorized as oropharyngeal or esophageal, with subcategorization of the latter into obstructive versus non-obstructive. Obstructive dysphagia is defined as the inability of food to pass in the esophagus due to the presence of a mechanical obstruction. In non-obstructive dysphagia (NOD), there is no visible obstruction detectable on endoscopy or radiographic studies.2,3 Approximately 50% of NOD patients have a motility disorder.2,4-7 When standard diagnostic testing is unrevealing, the Rome IV criteria classifies patients as having functional dysphagia. 4 Minimal therapeutic guidance exists for NOD dysphagia. In 1999, the American Gastroenterological Association reported empiric bougie dilation could be a reasonable treatment for patients with NOD to solids. 8 In 2014, the American Society for Gastrointestinal Endoscopy recommended against the use of empiric dilation in patients with NOD. 9 The recommendation against empiric dilation in NOD was due to potential risk of perforation with large-bore dilators, particularly in patients with undiagnosed eosinophilic esophagitis. One study examining empiric dilation in 7,256 patients reported only 2 perforations and 3 patients with postprocedural bleeding. 6 The risk of perforation from EGD alone is 0.03%. 10 Given the conflicting recommendations, our study retrospectively examined a cohort of patients with NOD to solids and liquids who underwent EGD and were treated with empiric esophageal dilation. We aim to investigate whether empiric dilation leads to subjective improvement of dysphagia.
Materials/Methods
Patient Cohort
A single tertiary hospital system (Prisma Health-Upstate) electronic database (EPIC, Verona, WI) was queried between January 2021 and October 2021 for patients undergoing EGD with dilation using ICD-10 codes 43248 (Esophagogastroduodenoscopy, flexible, transoral; insertion of guide wire followed by passage of dilator(s) through esophagus over guide) and 43450 (Dilation of esophagus, by unguided sound or bougie, single or multiple passes). Adult patients 18 to 80 years old were included. Demographics, dilation occurrence (recorded as “yes” or “no” responses), dilator size, tissue disruption, stricture, visual assessment for normal appearing esophagus, proton pump inhibitor use before and after the procedure, and work up after dilation were manually extracted from the medical charts. If procedural documentation lacked commentary on esophagitis, abnormal Z-line, and suspected Barrett’s, the esophagus was considered “visually normal.” Patient exclusions included history of foregut surgery, opioid use, marijuana use, endoscopic visualization of a stricture, Barrett’s esophagus, and pathology findings of eosinophilic esophagitis. The patient’s response to dilation was recorded as “yes” or “no” and patients without documentation were contacted via telephone and asked about symptomatic changes after the procedure. Patients unable to be reached, or those lacking follow up documentation, were classified as treatment failures.
Statistical Analysis
Data were analyzed as both continuous and categorical variables. All continuous variables are expressed as Mean ± (SD) and categorical as numbers or percentages. Categorical variables were analyzed using Chi-square or Fisher exact tests, when appropriate. An independent t-test was used for normally distributed continuous variables. In all analyses, the P-value < 0.05 was significant. Statistical analysis was performed using SPSS (SPSS Inc. Chicago, IL, version 25.0 for windows).
Results
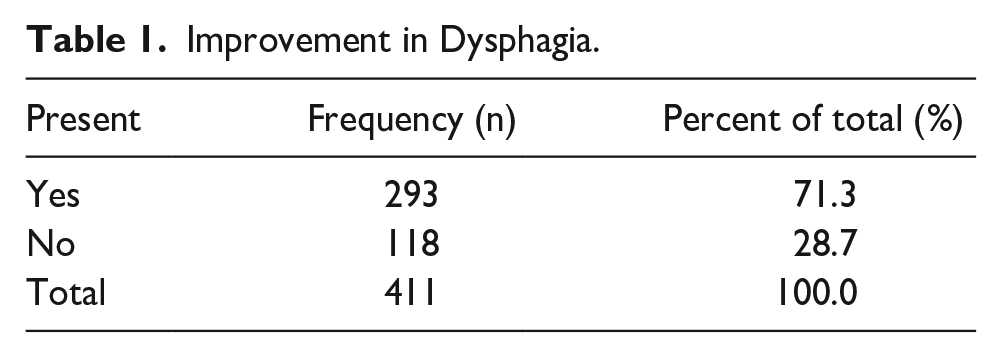
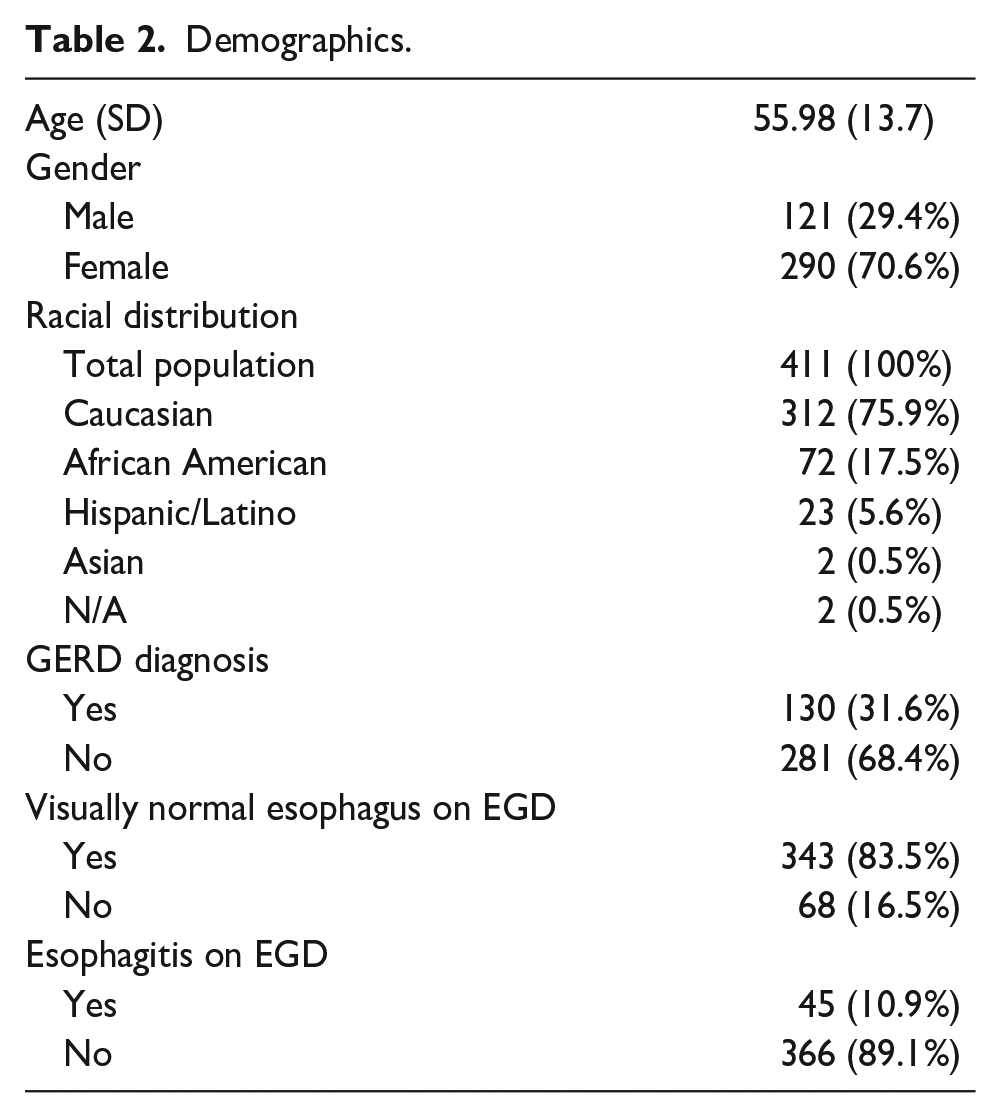
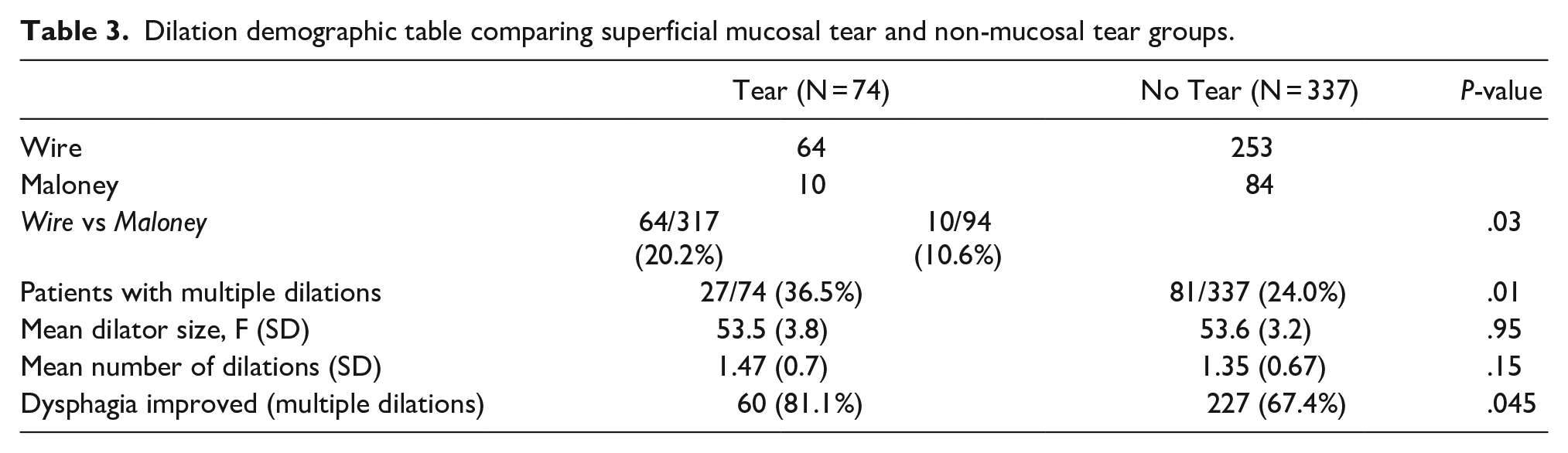
After exclusion criteria, 411 cases underwent empiric dilation. The mean age of our cohort was 56 years ±13.7 (range: 21-80). The majority were Caucasian 76%, African American 17%, Hispanic/Latino 5.7%, and Asian 0.3%. A visually normal esophagus was reported in 83.5% of procedures; Esophagitis was noted in 11% of patients. GERD was listed as a medical problem in ~32% of patients at the time of procedure. Of the 411 patients who underwent empiric esophageal dilation, 380 (92.5%) had an assessment of symptoms documented post-procedurally. Improvement in non-obstructive dysphagia was reported in 293 subjects (71.3%) (Table 1). The mean age reporting improvement was 56 years (SD 13.9) and similar to those without improvement 55 years (SD 13.5) (Table 2). Our proceduralists used Maloney bougie (N = 94) and Savary-Gilliard wire-guided (N = 317) dilators (Table 3). Dilator sizes ranged from 36 to 60 F, with 54 F being the most frequently used caliber overall. Of the total sample, 108 were serially dilated with escalating sizes during the same procedure. Average maximal dilation caliber was similar between groups (“mucosal tear” = 53.51 F, “no mucosal tear”= 53.46 F). There was no significant difference in maximal dilator size used in correlation to superficial mucosal tears or improvement in dysphagia. The frequency of superficial mucosal tears was more frequently seen with Savary wire dilation (P = .03) and serial dilations trended toward but failed to prove a significant correlation (P = .05).
Improvement in Dysphagia.
Demographics.
Dilation demographic table comparing superficial mucosal tear and non-mucosal tear groups.
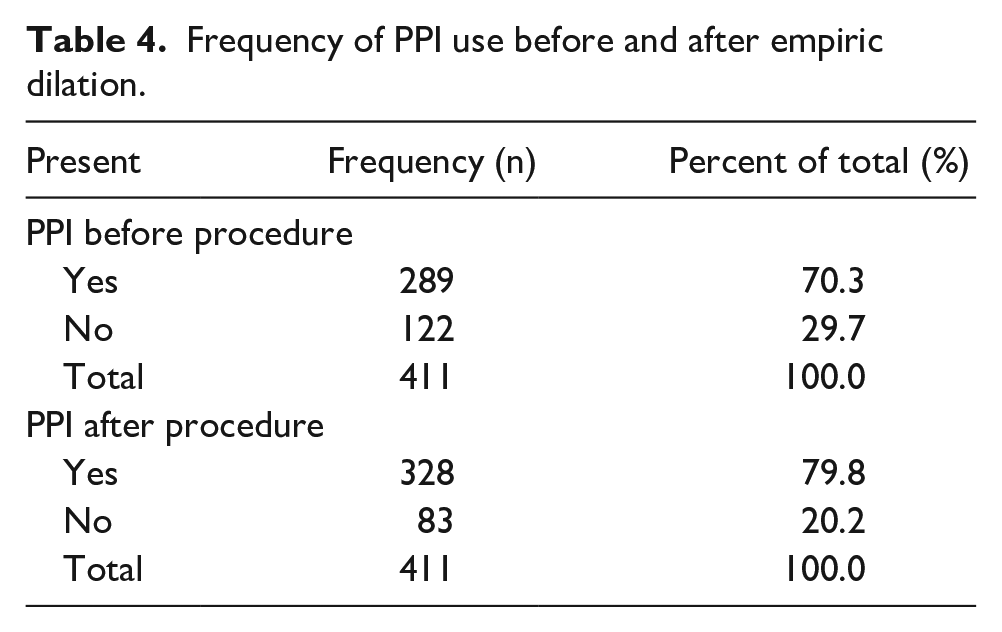
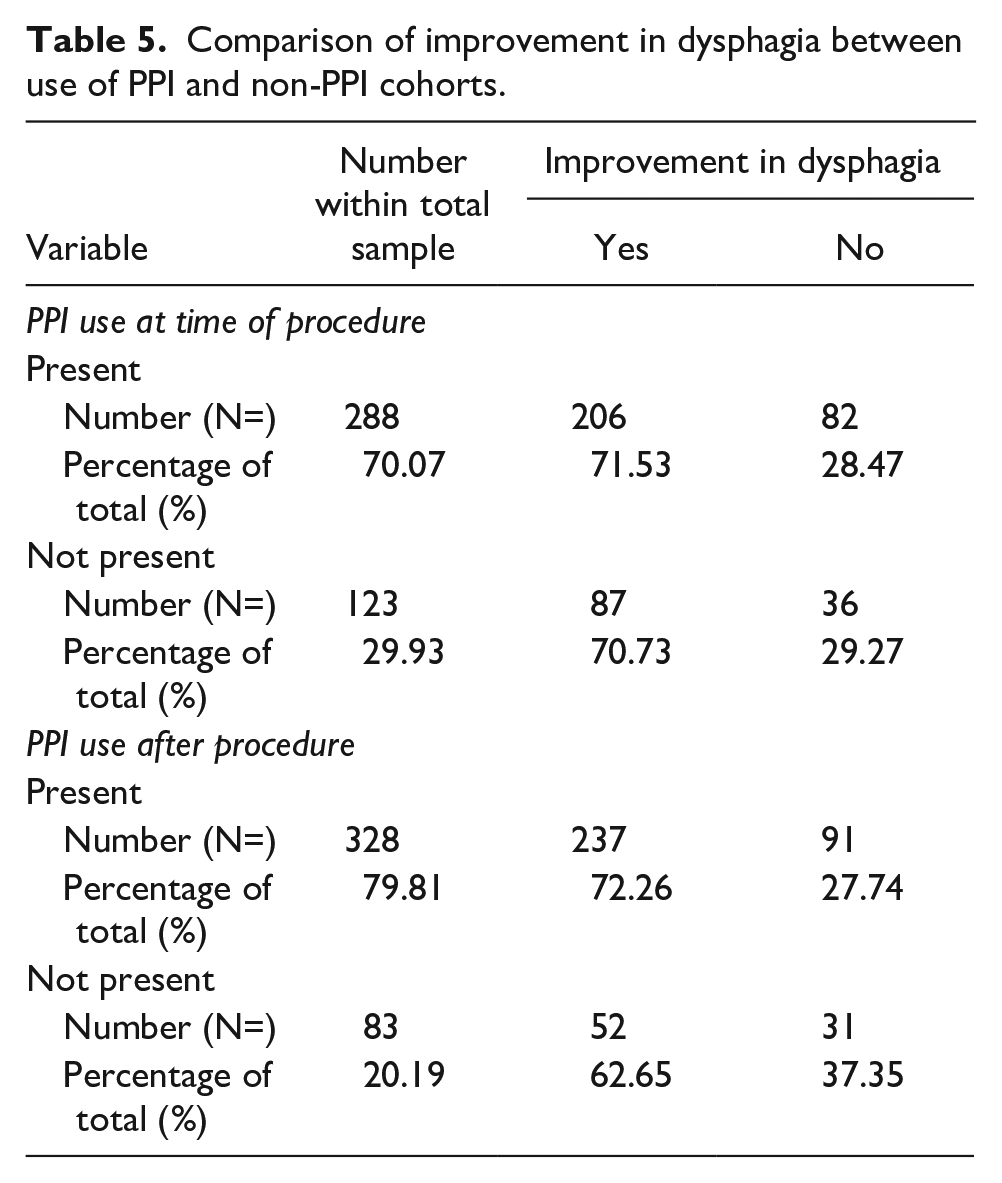
Prior to empiric dilation, PPI use was found in 70.3% of patients (Table 4), and 29.7% were not on PPI. After dilation, PPI use increased to 79.8% (Table 4). Of the patients already on PPI therapy, 71.5% reported improvement in dysphagia after the dilation (Table 5). Regarding patients not on PPI, 70.7% reported improvement. Of the patients who improved on PPI therapy, 72.3% were discharged with PPI therapy (Table 5).
Frequency of PPI use before and after empiric dilation.
Comparison of improvement in dysphagia between use of PPI and non-PPI cohorts.
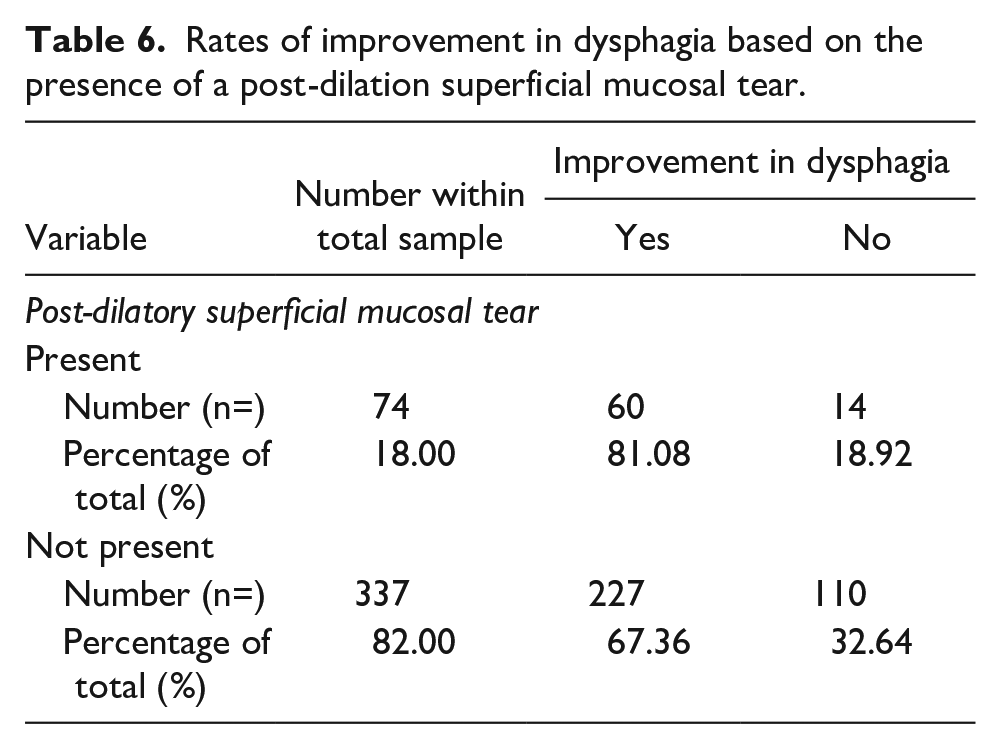
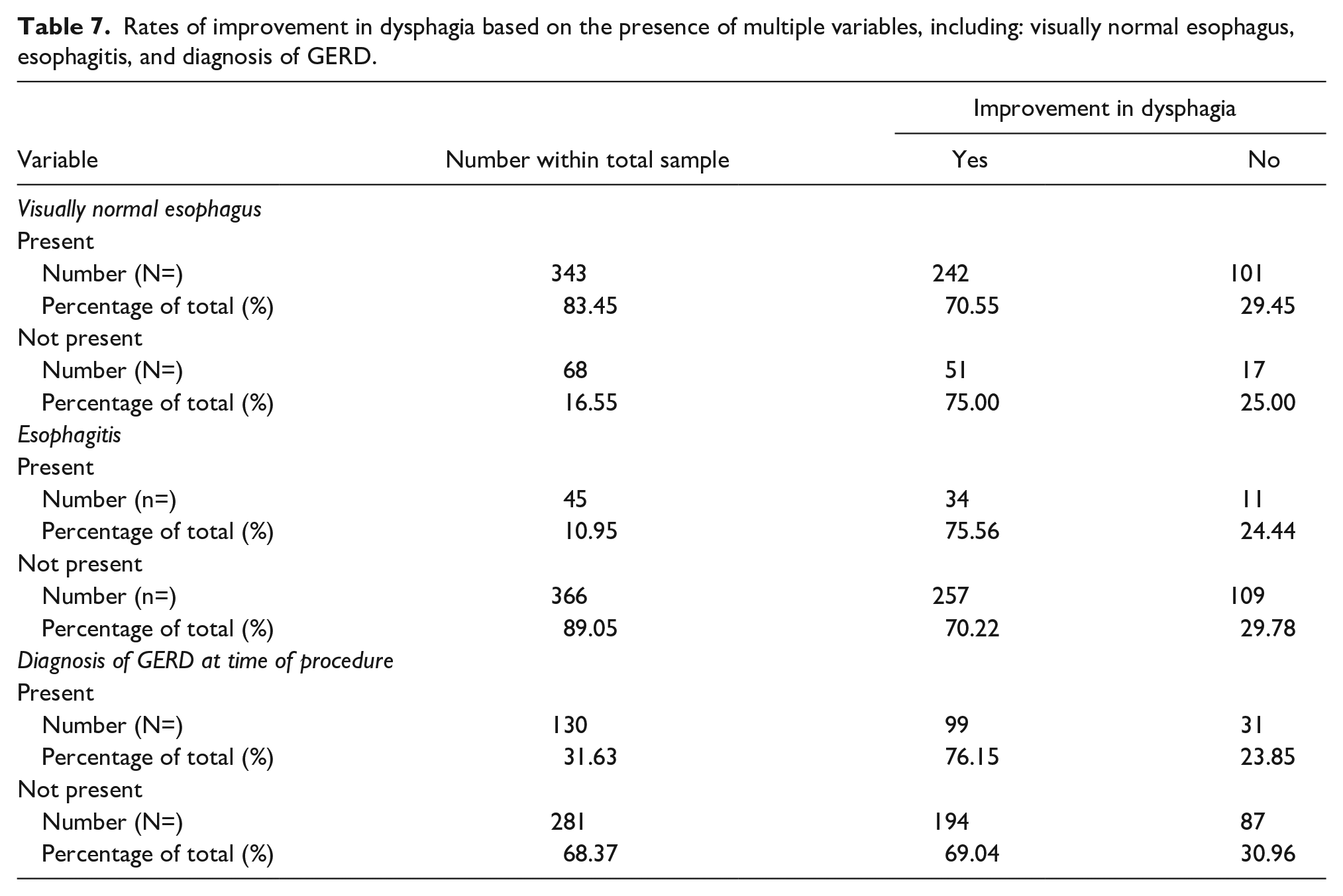
Further analysis leads us to comparison of the changes to dysphagia symptoms in relation to endoscopic findings during the procedure. Of the 74 cases of mucosal disruption (esophageal superficial-mucosal tear) after dilation, 81.1% (n = 60) reported improved dysphagia compared to 67.4% improvement in subjects without a tear (P = .02) (Table 6). Of the patients with a visually normal esophagus, esophagitis, or GERD, improvement was reported in 70.6%, 75.6%, and 76.1%, respectively (Table 7). Table 8 contains a graphical comparison of percentage improvement in dysphagia after dilation across all variables.
Rates of improvement in dysphagia based on the presence of a post-dilation superficial mucosal tear.
Rates of improvement in dysphagia based on the presence of multiple variables, including: visually normal esophagus, esophagitis, and diagnosis of GERD.
Percentage of Improvement in Dysphagia by Variable.
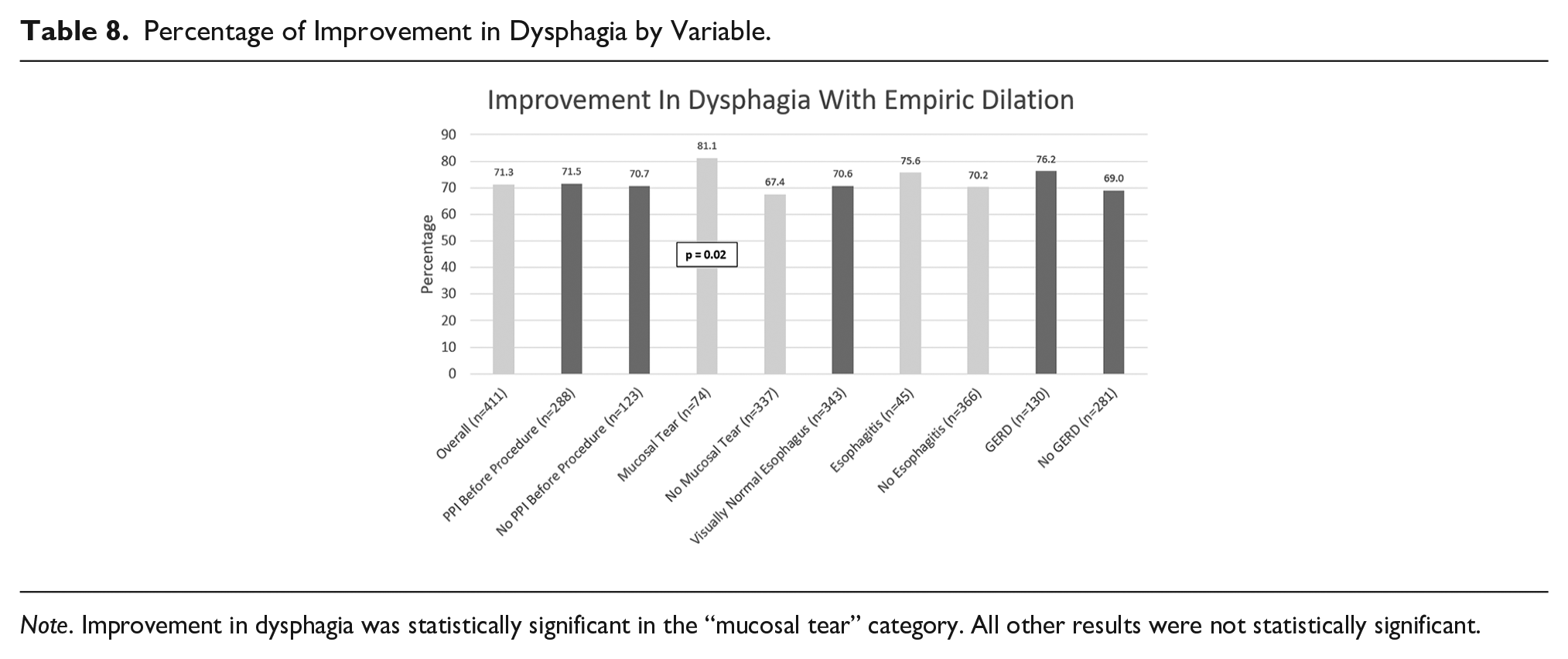
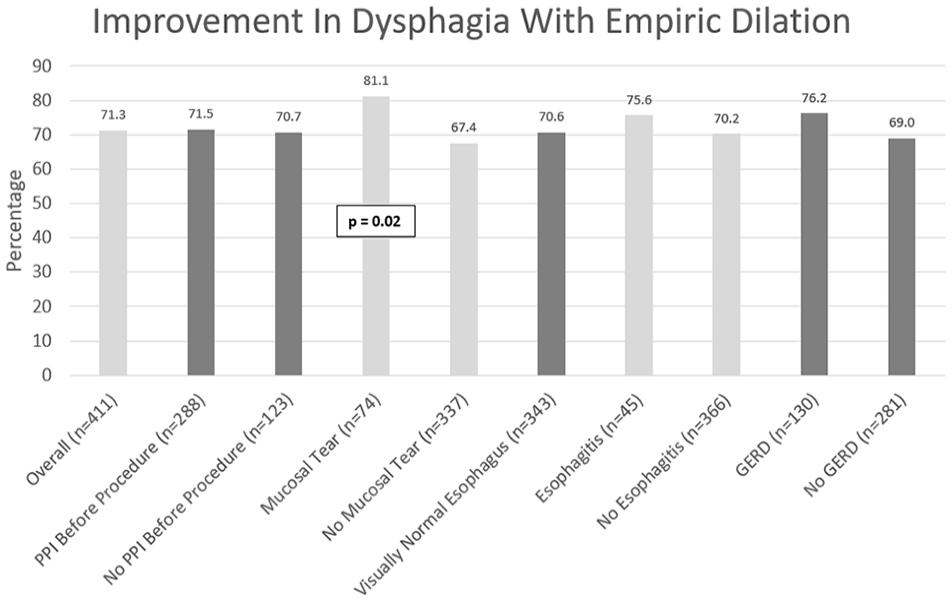
Note. Improvement in dysphagia was statistically significant in the “mucosal tear” category. All other results were not statistically significant.
Discussion
Limited literature exists on the treatment of NOD despite empiric dilation being a common practice. A review of endoscopic data repository by Olson et al. found 7,256 empiric dilations were performed for NOD. 6 Retrospective, prospective, and randomized studies have attempted to shed light on empiric dilation for NOS, although these studies have small sample size and conflicting results. The first study to assess the value of empiric dilation was in 1996, when Marshall and Chowdhury prospectively examined 20 patients with NOD who underwent empiric dilation with 42-Fr then 54-Fr bougies. 11 They found 95% of patients with solid dysphagia had complete resolution of dysphagia symptoms. In 2000, Colon et al. randomized 23 patients to empiric dilation with 26-Fr (“sham”) and 50-Fr bougie dilators. 5 Both groups reported improved dysphagia symptoms, although the results were not statistically significant. Between the 2 groups, the dilation with the 50 -French dilator achieved a sustained response at 2 years. 5 Although the control group underwent dilation with a smaller caliber bougie, it is possible that the dilation influenced the symptoms of dysphagia. In 2001, Scolapio et al. randomized 83 patients with NOD to 54-Fr balloon empiric dilation versus sham. Improvement in dysphagia at 6 months with dilation was 84% versus 73% with sham. They concluded empiric dilation could not be recommended. 12 Their study differed in several ways from ours. They used a patient questionnaire to track symptoms before and after the procedure. It is possible that the description of the patient’s dysphagia was not completely described in their survey. They featured a much smaller sample size than our study and their dilations were carried out solely via balloon. The dilator type could theoretically correspond to a different symptomatic response. In 2004, Lavu et al. randomized 30 patients with NOD to empiric dilation with 56-Fr Maloney dilator versus sham (40-Fr Maloney). Both groups improved, but the degree of improvement was not statistically significant. 13 Perhaps this is because the sham dilator was of significant caliber and may have conferred therapeutic effect. The improvement in both groups alludes to the need for a true “sham” procedure without dilation to definitely document the symptomatic variation between dilation and sham. Naini et al. retrospectively analyzed patients with dysphagia, 107 of whom had NOD. 3 Sixty patients were treated with empiric dilation and proton pump inhibitor while the rest received proton pump inhibitor alone. They found no statistically significant difference in symptom resolution between the 2 groups, but suggested patients with nonobstructive esophageal rings are more likely to benefit from esophageal dilation. In 2011, Pasumarthy et al. prospectively assessed 102 patients with NOD who underwent empiric dilation. 14 At 6 month follow up, 83% of patients had statistically significant improvement in dysphagia symptoms. In 2017 and 2020, two retrospective abstracts, by Zakaria et al. 15 and Velez et al., 16 found improvement in dysphagia after empiric dilation for NOD. Most recently, in 2021, Kamal et al. 17 performed a systematic review and meta-analysis which examined 4 studies. This included 3 RCTs and 1 observational study, discussed above, which found no statistical difference in clinical success or post procedure dysphagia score. In the mentioned studies, no complications were observed or reported. Between all the studies noted, there is a lack of standardization of dilation procedure, with variety in use of bougie dilation and balloon dilation. The sample sizes were also significantly smaller than our study.
In our study, we examined 411 patients with NOD and found 71.3% improvement in symptoms in all-patient reports. Interestingly, there was improvement regardless of a concurrent GERD diagnosis, PPI therapy, or the finding of esophagitis. This enforces the idea that none of these factors, in combination with empiric dilation, leads to improved outcomes in dysphagia. Regarding post-dilatory mucosal changes, we did observe a statistically significant (P = .02) response rate in subjects with a superficial mucosal tear.
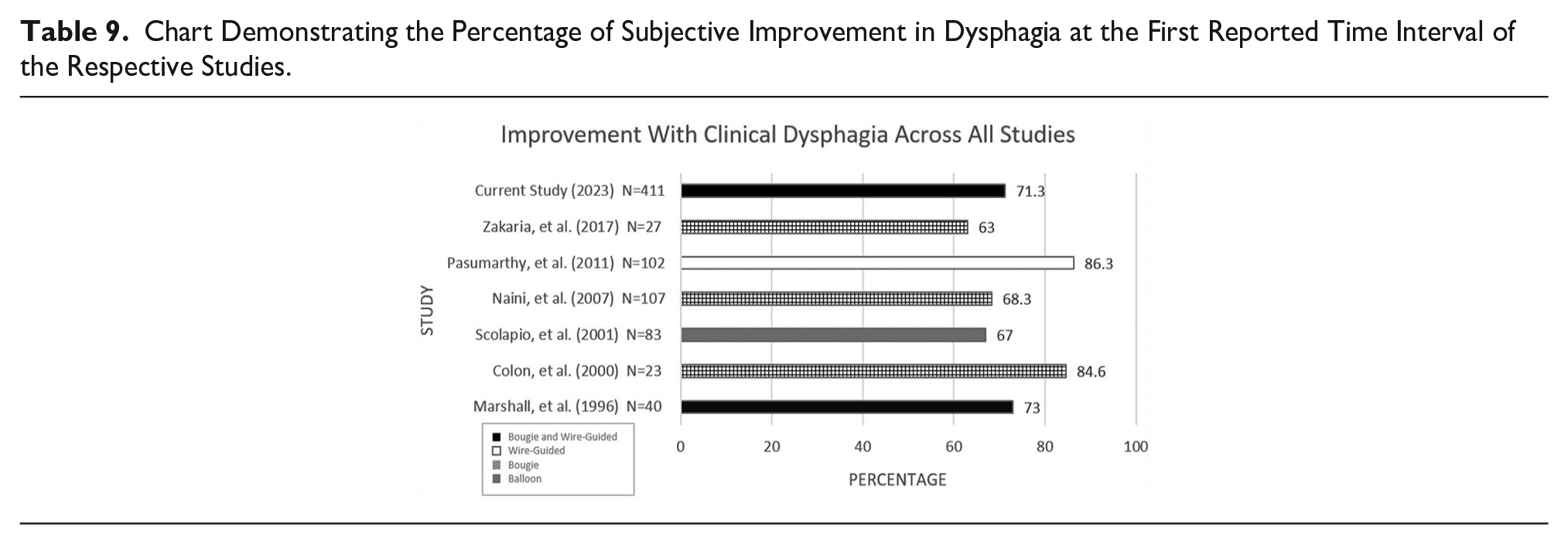
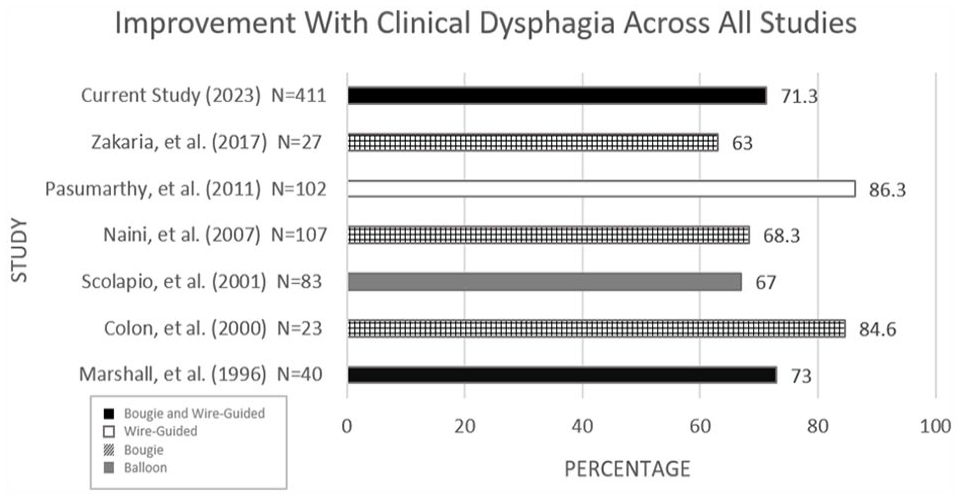
A comparison of studies denoting the number of patients who symptomatically improved after empiric dilation demonstrates encouraging percentages of improvement post-procedurally (Table 9). Although our study is the largest retrospective assessment for empiric dilation in subjects with NOD, several limitations are notable. The timing between dilation and follow up was not documented; the outcome was categorical and not on a nominal scale which could have provided deeper information, and the duration of improvement post dilation was not assessed. Patients with absent documentation who were contacted regarding symptomatic change may have had a recency bias affecting their reporting. We did not differentiate the effect of empiric dilation on dysphagia to solids, liquids, or both. Our study also featured a demographic distribution of mostly caucasian individuals, limiting population generalizability. While the majority of follow up results were obtained, there was a sizable sample of 31 individuals in which subsequent documentation was absent. These individuals were tallied as treatment failures to minimize bias toward the recommending of esophageal dilation, like an “intention to treat” analysis in randomized-controlled trials. It is reasonable to assume that some patients had an undiagnosed upper-esophageal abnormality such as a web or subtle stricture. It is also possible some patients experienced a placebo effect due to treatment. While symptomatic improvement was seen in many of our patients, we are not able to guarantee the absence of a primary esophageal motility disorder in, at least, a proportion of our cohort. For patients in which this may be true, the pursuit of additional investigative studies (such as esophageal manometry and EndoFLIP) may further guide management. Lastly, we did not collect data on procedural complications, but none were reported on our follow-up phone calls. Previous studies using Savary-wire or Maloney dilator for empiric dilation have demonstrated vary rare rates of complications.6,12,14,16 Regarding future studies, a large multicenter randomized-controlled trial that utilizes validated patient reported outcomes is warranted.
Chart Demonstrating the Percentage of Subjective Improvement in Dysphagia at the First Reported Time Interval of the Respective Studies.
In conclusion, our results suggest empiric esophageal dilation for NOD is a beneficial practice that provides both patients and providers an additional therapeutic option in the management of esophageal dysphagia.
Footnotes
Correction (May 2024):
Article updated to add Ethical approval statement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board and individual patient consent was waived.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.