Abstract
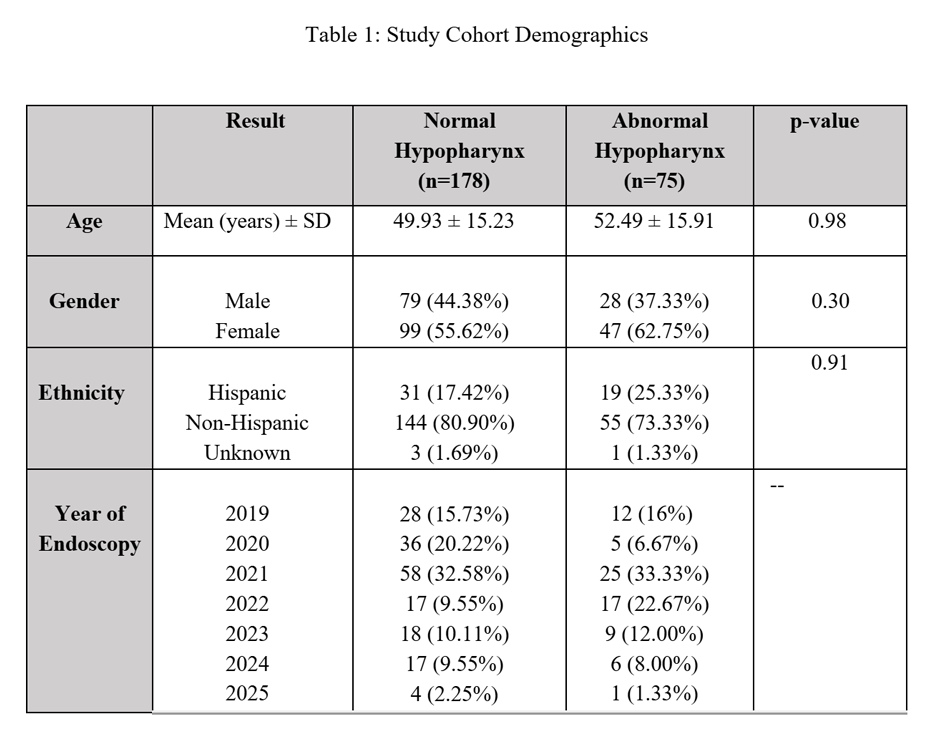
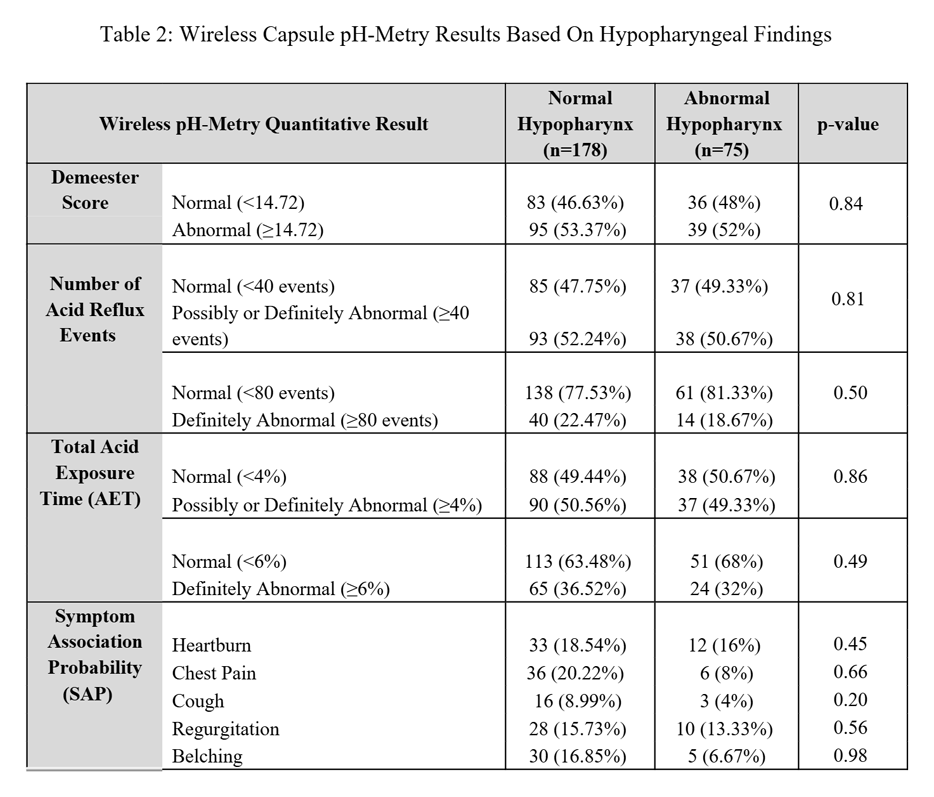
Otolaryngologists often refer patients for assessment of gastroesophageal reflux (GER) with suspected laryngopharyngeal reflux (LPR) after seeing hypopharyngeal erythema and/or edema. Research has demonstrated an inconsistent link between atypical GER/LPR-like symptoms and excess GER on quantitative testing compared to more typical GER symptoms of heartburn and regurgitation. This study’s aim was to determine whether visualized hypopharyngeal abnormalities accurately predict excess GER on wireless capsule pH-Metry. All patients undergoing wireless pH-Metry testing off acid reduction therapy by a single high-volume esophagologist from 2019-2025 were reviewed. Patients were included if explicit documentation of hypopharyngeal findings (normal/abnormal), complete pH-Metry results and demographics were available. Wireless pH-Metry findings were assessed based on Lyon 2.0 criteria, with <40 acid reflux events/day definitely normal and ≥80 abnormal, along with total acid exposure time (AET) <4% normal and ≥6% abnormal. DeMeester scores >14.72 were considered abnormal, and symptom association probability (SAP) >95% was considered significant. Chi Square and Wilcox rank sumstatistical analyses were used to compare variables of interest. Of 253 eligible patients (58% female, mean age 49.3 years), 178 (70.4%) had an endoscopically normal hypopharynx (Table 1). There was no significant difference in endoscopic hypopharyngeal findings when evaluating the continuous variables of DeMeester score (p=0.25), total number of acid reflux events (p=0.16), total AET (p=0.29) or longest reflux interval (p=0.25). Likewise, there was no difference in the percentage of patients with excess GER based on Lyon 2.0 AET and reflux events cutoffs, or for any symptom association probability (Table 2). The presence of visible hypopharyngeal abnormalities does not significantly change the likelihood of identifying quantitatively abnormal GER during wireless pH-Metry testing, nor does it predict stronger symptom correlation. These results should serve as a reminder for providers to avoid treating reflux solely based on hypopharyngeal findings, as this can lead to misdiagnosis and inappropriate treatment.