
Abstract
Background:
Perforated peptic ulcer (PPU) remains a surgical emergency with considerable morbidity and mortality. While both simple closure and omental patch are widely adopted repair techniques, their relative effectiveness continues to be debated. This meta-analysis aimed to compare surgical outcomes between these 2 approaches.
Methods:
A systematic search of Europe PMC, Medline, Scopus, and the Cochrane Library was performed to identify studies directly comparing simple closure and omental patch repair in patients with PPU. Data were synthesized using Review Manager 5.4. Dichotomous outcomes were expressed as odds ratios (OR) and continuous outcomes as mean differences (MD), both with 95% confidence intervals (CI). Random-effects models were applied.
Results:
Eight studies met eligibility criteria. The rates of overall complications (P = .70), postoperative leak (P = .48), ileus (P = .61), surgical site infection (P = .95), intra-abdominal collection (P = .86), reoperation (P = .24), and mortality (P = .58) showed no significant differences between groups. Similarly, length of hospital stay (MD −0.21 days, 95% CI −1.06 to 0.63) and time to resume oral intake (MD −0.08 days, 95% CI −0.89 to 0.73) were comparable. However, operative time was significantly shorter in the simple closure group (MD −21.73 minutes, 95% CI −30.15 to −13.32).
Conclusions:
Both techniques appear to have comparable safety and effectiveness across most clinical outcomes. However, simple closure is associated with a shorter operative duration, which may make it a reasonable option to consider, particularly in resource-limited or emergency settings.
Introduction
Perforated peptic ulcer (PPU) remains a frequent surgical emergency worldwide, carrying significant risks of morbidity and death if not treated promptly. 1 Although advances in resuscitation and antimicrobial therapy have improved early management, the choice of definitive operative repair continues to influence short-term outcomes such as leak, infection, and need for reoperation, as well as longer-term measures like recurrence and functional recovery. 1 Surgeons most commonly use either simple primary closure of the perforation or a closure reinforced with an omental patch; both techniques aim to seal the defect and limit peritoneal contamination, yet they differ in complexity, tissue handling, and theoretical durability.2,3
Despite decades of clinical experience, consensus is lacking on whether the addition of an omental patch offers measurable advantages over simple closure across diverse patient groups and clinical settings.2,3 Some practitioners argue that the omental patch provides a biologic buttress that reduces the risk of re-perforation and promotes healing, while others contend that the extra manipulation may prolong operative time and increase local inflammation without clear benefit—particularly in small perforations or when omentum quality is poor.3,4 Existing single-center series and observational cohorts frequently report conflicting results, are variably adjusted for confounders (age, comorbidity, peritonitis severity), and use heterogeneous outcome definitions, which complicates direct comparison and guideline development.5,6 For example, Mahmoud et al 5 reported that patients with PPU treated using simple closure technique experienced a reduced likelihood of leakage and were able to restart oral feeding earlier compared with those managed with an omental patch. In contrast, Abd Ellatif et al 6 found no meaningful difference between the 2 techniques regarding leakage rates or the interval to resumption of oral intake.
A rigorously conducted meta-analysis can synthesize the available evidence to address these inconsistencies. This study therefore aims to move beyond fragmented single-study conclusions by (1) quantifying the comparative effectiveness and safety of simple closure versus omental patch repair for PPU and (2) identifying patient- and procedure-level modifiers of effect. The results will provide clinicians and guideline committees with consolidated, empirically grounded guidance to select the most appropriate operative strategy for patients with PPU.
Materials and Methods
Eligibility Criteria
The review process complied with PRISMA recommendations. 7 Its protocol was prospectively entered into the PROSPERO database (CRD420251137725), and the selection criteria were structured based on the PICOS model.
Population: adult patients diagnosed with PPU (gastric or duodenal) who underwent surgical repair.
Intervention: managed surgically using the simple closure technique (primary closure without additional tissue reinforcement).
Control: treated with the omental patch (eg, Graham’s patch or other variants).
Outcome: reporting at least 1 clinically relevant outcome: • Primary Outcome: total complications rate. • Secondary Outcomes: postoperative leak, ileus, surgical site infection, intra-abdominal collection, reoperation, mortality, operating time, length of hospital stay, and time to resume oral diet.
Study Design: randomized controlled trials (RCTs), non-randomized controlled studies, prospective and retrospective cohort studies, and case-control studies.
Meanwhile, studies were excluded if they met any of the following predefined criteria: (1) Studies restricted to pediatric populations, experimental models, or cases of traumatic/non-peptic perforation; (2) Reports where simple closure is combined with adjunctive procedures (eg, gastric resection, vagotomy, or reinforcement other than omental patch); (3) Studies comparing omental patch with surgical methods other than simple closure; (4) Studies that fail to provide extractable or comparable outcome data; (5) Case reports, case series without a comparison group, review articles, editorials, conference abstracts without full data, or studies with overlapping patient cohorts.
Literature Search and Study Selection
We systematically queried 4 electronic databases—MEDLINE (via PubMed), Scopus, Europe PMC, and the Cochrane Library—from database inception through August 31, 2025. No restrictions were applied on publication year or language at the search stage. Reference lists of all eligible studies and relevant reviews were also hand-checked to identify additional reports. The strategy combined controlled vocabulary and free-text terms related to PPU and the 2 surgical techniques of interest. Search strings were adapted to the indexing of each database. An example of PubMed syntax was: (“peptic ulcer” [MeSH] OR “duodenal ulcer” OR “gastric ulcer” OR “perforated peptic ulcer” OR “PPU”) AND (“simple closure” OR “primary closure” OR “direct closure”) AND (“omental patch” OR “Graham patch” OR “omentopexy”). Equivalent Boolean logic (title/abstract keywords plus subject headings such as Emtree in Scopus and MeSH in Cochrane/Europe PMC where applicable) was used across sources. Full database-specific strategies are provided in the Supplementary Table 1.
All records were exported to a reference manager and de-duplicated algorithmically, followed by manual verification. Two reviewers independently screened titles and abstracts against prespecified PICOS criteria. Potentially eligible reports were retrieved in full text and assessed independently by the same reviewers. Disagreements at any stage were resolved through discussion; a third reviewer adjudicated when consensus was not reached.
Data Extraction
Two reviewers independently extracted data using a predesigned extraction form; discrepancies were resolved by discussion and, if needed, by a third reviewer. Data were captured directly from text, tables, and figures; when necessary, we contacted study authors for missing or unclear information. All extracted numeric data were entered as raw counts or continuous summary statistics (means and standard deviations). If studies reported medians with ranges or interquartile ranges, we converted these to means ± SD using published estimation methods and documented the method used for each conversion. Extracted items included study characteristics, patient demographics, details of ulcers/perforations, and reported outcomes.
The primary outcome was the total complications rate, defined as any postoperative adverse event reported within the study’s stated observation window (or within 30 days if the study did not specify).
Secondary outcomes comprised:
• Postoperative leak, defined as clinically evident or radiologically confirmed leakage from the repair site (gastric or duodenal), as reported by the study (eg, presence of enteric content from drains, contrast extravasation on imaging, or reoperation for suspected leak).
• Ileus, defined as failure to achieve expected return of bowel function (absent flatus or stool) or inability to tolerate oral intake requiring nasogastric decompression or delaying discharge, as defined by the authors.
• Surgical site infection, defined as local wound infection occurring at the incision site, diagnosed clinically and/or microbiologically and reported by the study.
• Intra-abdominal collections, defined as any postoperative fluid collection within the peritoneal cavity identified by imaging or at reoperation and attributed to infectious or inflammatory etiology (including abscess).
• Reoperation, described as any return to the operating theatre for a complication related to the index procedure (eg, control of leak, drainage of collection, wound debridement).
• Mortality, defined as death occurring in the postoperative period as reported by the study.
• Operating time, defined as duration of the index operation measured from skin incision to skin closure (or equivalent intraoperative time reported by the study).
• Length of hospital stay, reported as number of days from index surgery to discharge from hospital.
• Time to resume oral diet, reported as interval (in days) from surgery to the first tolerated oral intake (sips, liquids, or normal diet—we recorded the specific definition used by each study).
Because several postoperative outcomes—such as ileus and time to oral intake—were defined inconsistently across the included studies, we standardized outcome extraction using the most commonly reported or clinically conventional definitions as described above. When studies used broader or narrower criteria, we abstracted the definition verbatim and classified the outcome into the prespecified category that most closely matched our operational definition. If definitions were irreconcilably different, the study was excluded from the pooled analysis for that specific endpoint. To assess the potential impact of definitional variability, we performed sensitivity analyses by repeating the meta-analysis after removing studies with atypical or explicitly discordant definitions. Results were compared with the primary estimates to evaluate the robustness of pooled effects.
Risk of Bias Assessment
The methodological quality of the included observational studies was appraised using the Newcastle-Ottawa Scale (NOS), which evaluates 3 domains: selection of participants, comparability of study groups, and adequacy of outcome assessment. 8 Each study was scored across these domains, with a maximum possible score of 9. 8 In this review, studies achieving a score of 7 or higher were categorized as having good methodological quality, while those below this threshold were considered at higher risk of bias. 8 Two reviewers performed the assessment independently, and disagreements were settled through discussion to reach consensus.
Statistical Analysis
All statistical procedures were carried out using Review Manager (RevMan) version 5.4. For dichotomous outcomes, treatment effects were expressed as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). For continuous outcomes, pooled estimates were reported as mean differences (MDs) with 95% CIs. A random-effects model was applied as the default analytical approach to account for anticipated clinical and methodological variability across studies. Statistical heterogeneity was evaluated using the I2 statistic, with values above 50% indicating substantial inconsistency. 9 Potential sources of heterogeneity were further explored through subgroup and sensitivity analyses when adequate data were available. Prespecified subgroup analyses were undertaken for the primary outcome (total complications) and outcomes that showed significant heterogeneity to examine potential effect modifiers. Analyses were stratified by: geographic origin of the study (Taiwan vs outside Taiwan), study design (prospective cohort vs retrospective cohort), type of surgery (all laparoscopy vs mixed open and laparoscopy), ulcer location (predominantly duodenal vs predominantly gastric vs not specified), and perforation size (mostly ≤5 mm vs mostly >5 mm). Publication bias was examined visually using funnel plots if at least 10 studies were included in a given comparison. A 2-sided P < .05 was considered statistically significant.
Results
Study Selection and Characteristics
An initial retrieval from the 4 designated databases yielded 421 records. Following the removal of duplicates and the screening of titles and abstracts, 383 studies were excluded, and 38 full-text articles were evaluated in detail. Among these, 30 were eliminated for not meeting the inclusion requirements: 18 lacked an appropriate control group, 5 did not provide distinct outcome data, 4 were review articles, and 3 involved pediatric cohorts. Ultimately, 8 studies5,6,10-15 satisfied all criteria and were incorporated into the final analysis (Figure 1). Of the studies included, 7 employed a retrospective cohort design, whereas one followed a prospective cohort approach. Geographically, 4 studies originated from Taiwan, 2 from Egypt, and one each from China and the United States. In terms of surgical techniques, 6 investigations utilized exclusively laparoscopic procedures for PPU repair, while the other 2 incorporated both laparoscopic and open methods. Regarding ulcer sites, 3 studies reported duodenal involvement, 1 primarily examined gastric ulcers, and 4 did not specify the anatomical location of the perforations. In most cases, perforation size was reported as ≤5 mm. Study populations varied considerably, with sample sizes ranging from 26 to 182 patients in the simple closure groups and 20 to 108 in the omental patch groups. A summary of baseline study characteristics is displayed in Table 1.
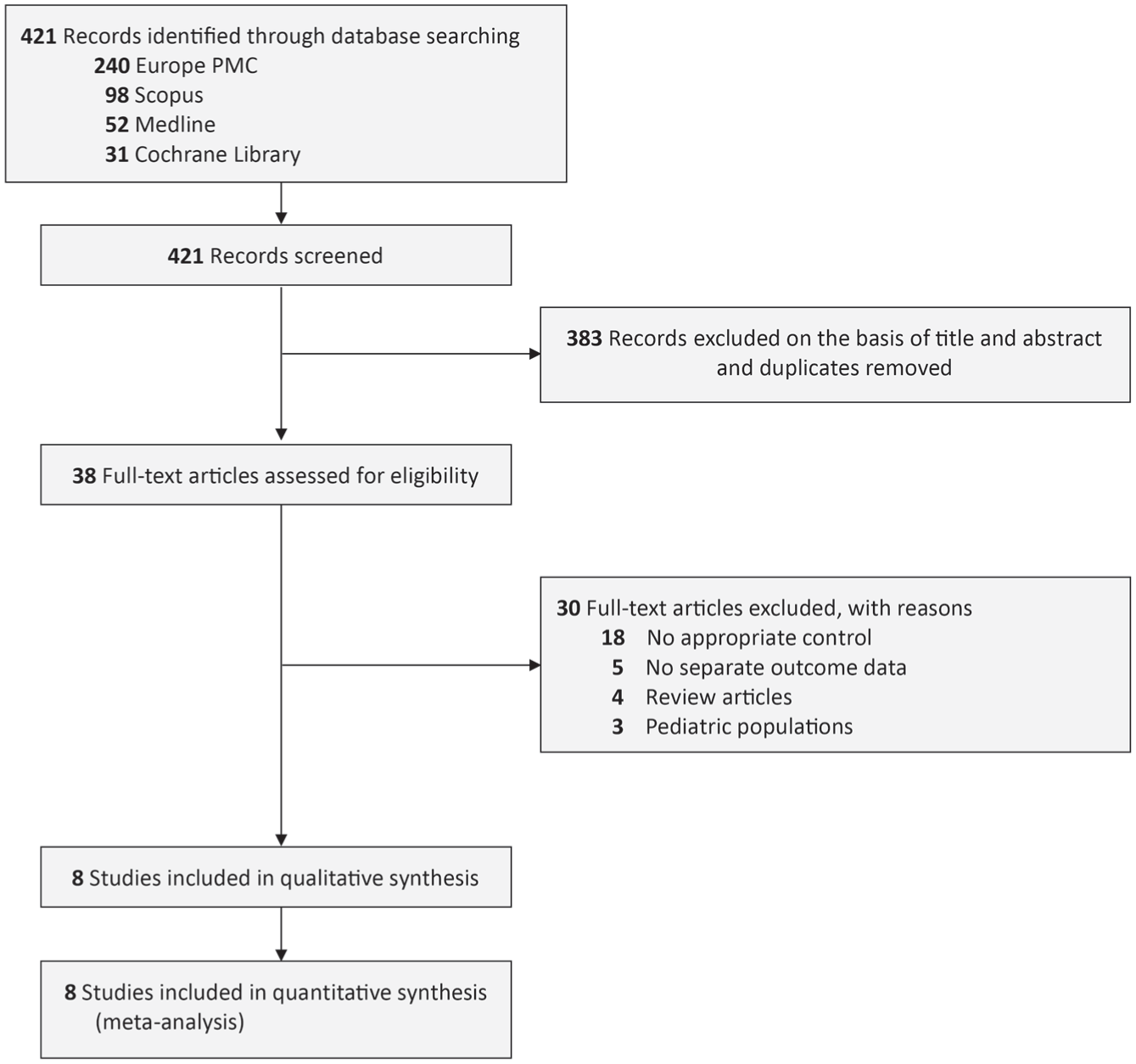
PRISMA diagram of the detailed process of selection of studies for inclusion in the systematic review and meta-analysis.
Baseline Characteristics of the Included Studies.
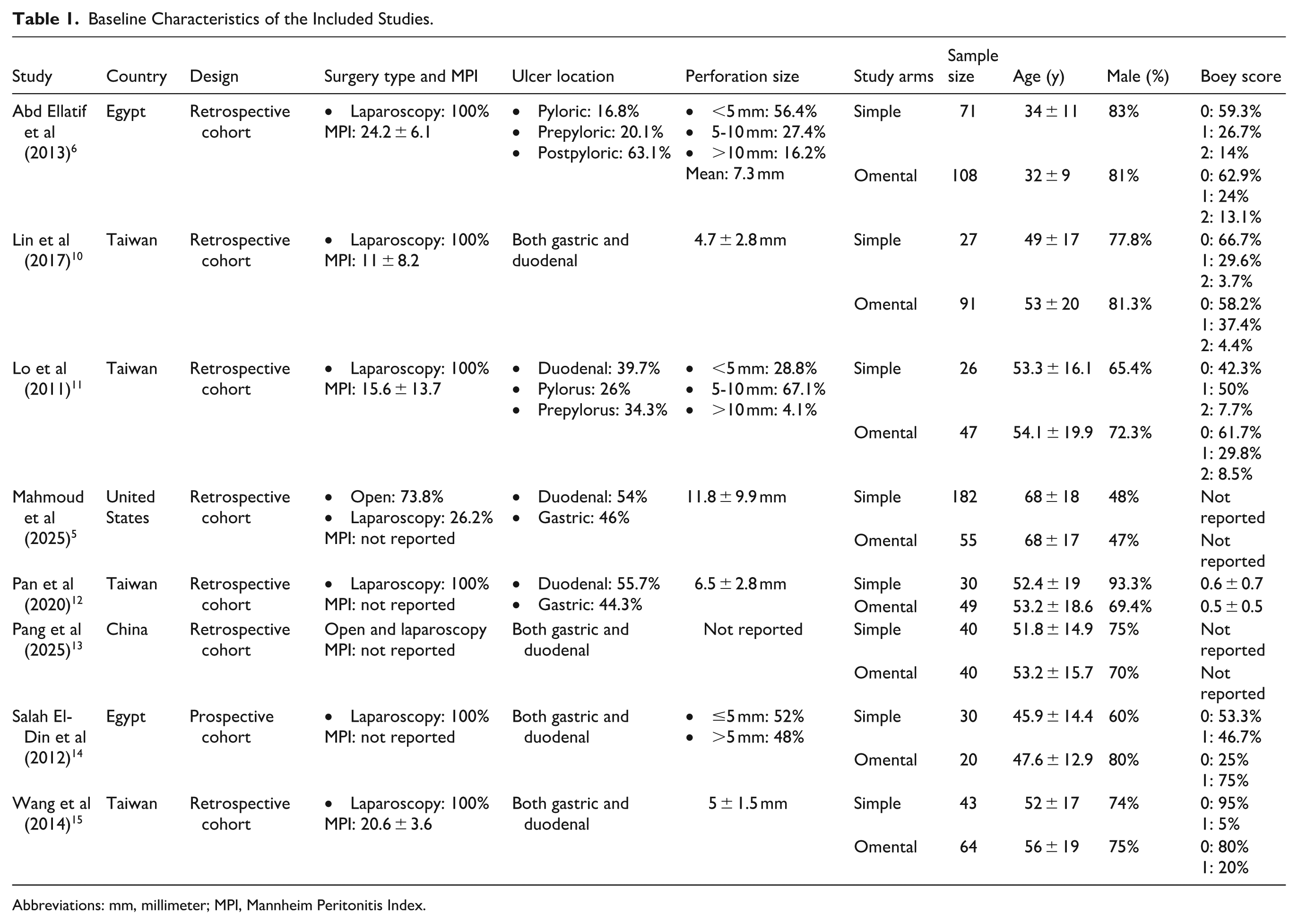
Abbreviations: mm, millimeter; MPI, Mannheim Peritonitis Index.
Quality of Study Assessment
Based on the risk of bias appraisal performed with the NOS tool, all observational studies achieved scores between 7 and 8, reflecting good methodological quality (Table 2).
Newcastle-Ottawa Quality Assessment of Observational Studies.
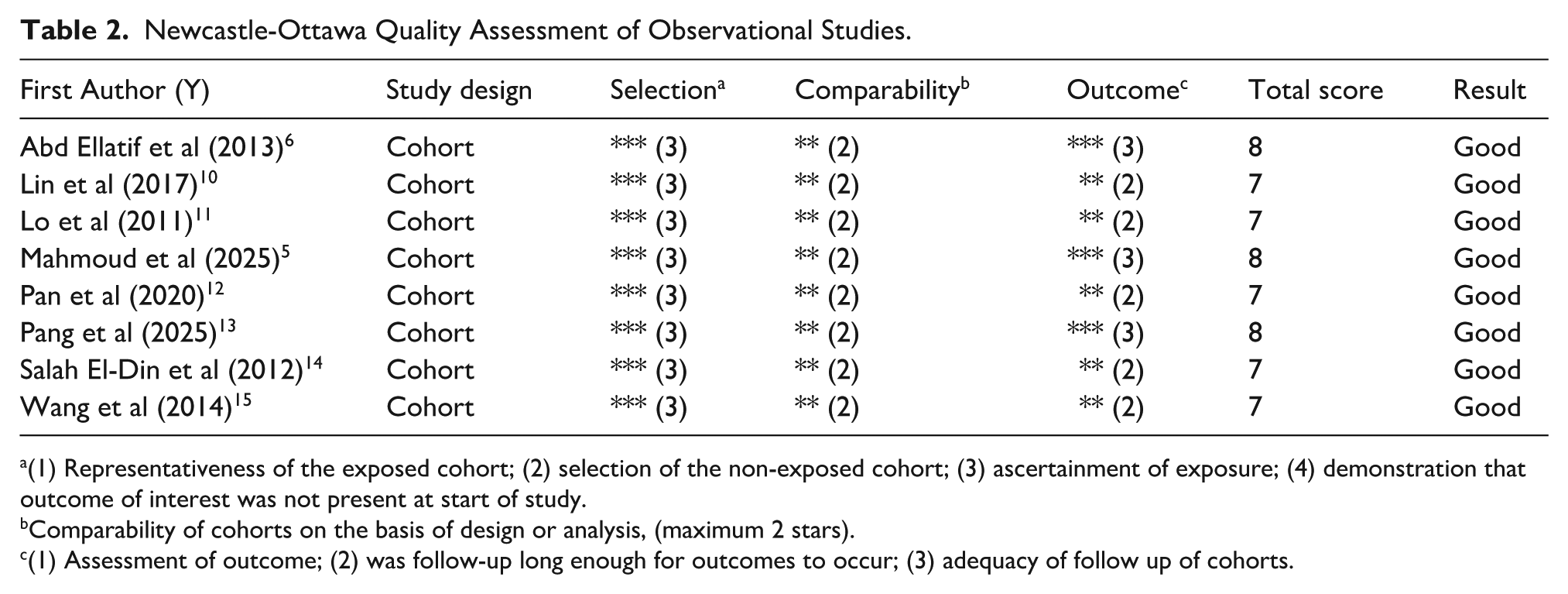
(1) Representativeness of the exposed cohort; (2) selection of the non-exposed cohort; (3) ascertainment of exposure; (4) demonstration that outcome of interest was not present at start of study.
Comparability of cohorts on the basis of design or analysis, (maximum 2 stars).
(1) Assessment of outcome; (2) was follow-up long enough for outcomes to occur; (3) adequacy of follow up of cohorts.
Primary Outcome (Total Complications)
A pooled analysis of 8 studies encompassing 923 patients indicated that the total complication rates did not differ significantly between the simple closure approach and the omental patch method for PPU repair (OR 0.93 [95% CI 0.65-1.33], P = .70, I2 = 0%, random-effect models; Figure 2 and Table 3).
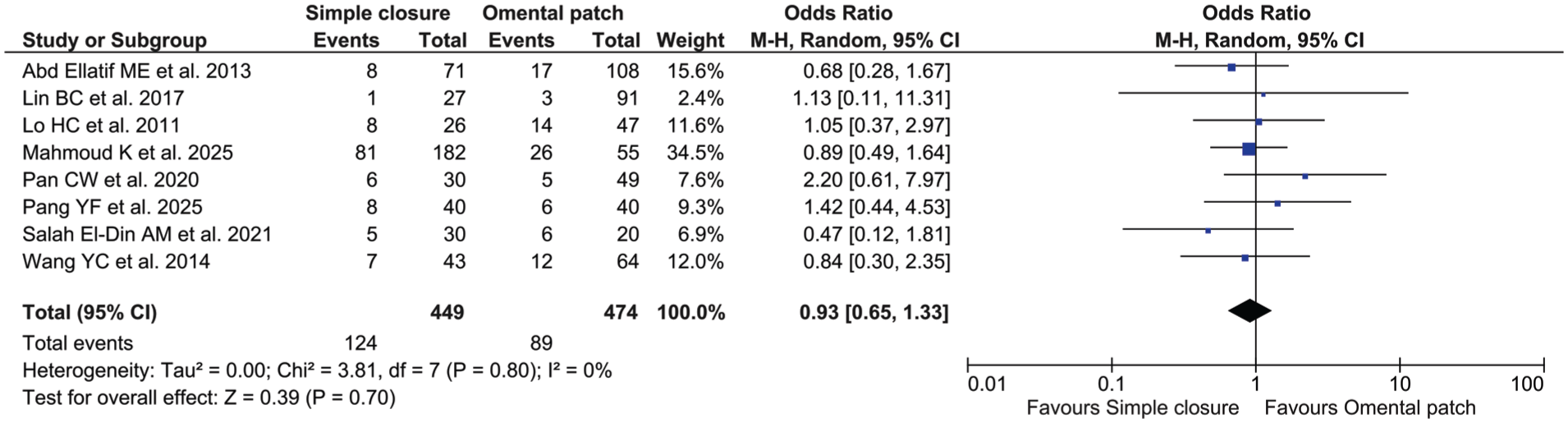
Forest plot depicting the incidence of total complications in PPU repairs utilizing simple closure versus omental patch techniques.
Summary of Meta-Analysis Results for Comparison Between Simple Closure and Omental Patch for the Management of Perforated Peptic Ulcer.
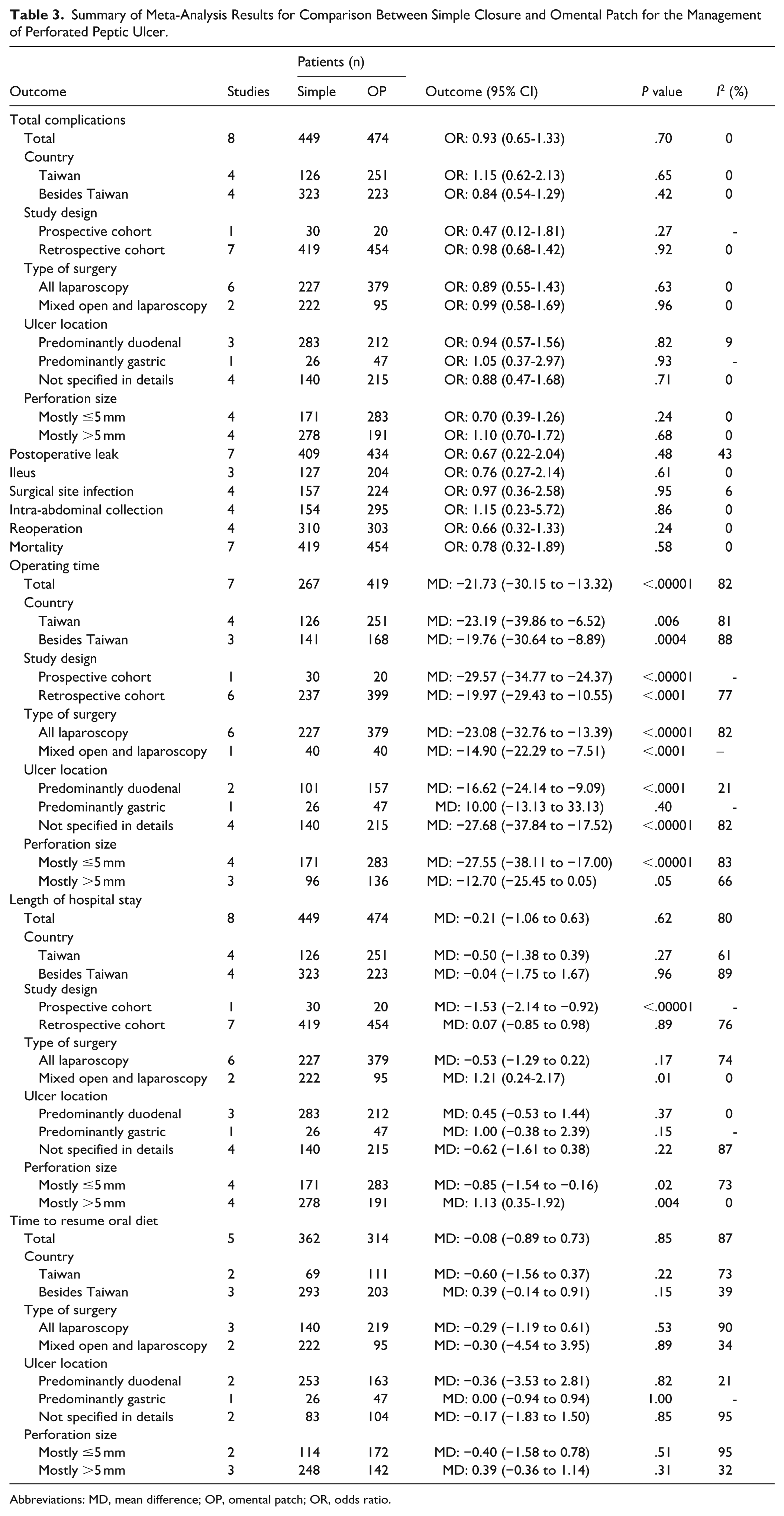
Abbreviations: MD, mean difference; OP, omental patch; OR, odds ratio.
Subgroup analysis by country indicated that studies conducted outside Taiwan (OR 0.84 [95% CI 0.54-1.29], P = .42, I2 = 0%, random-effect models) showed a trend toward lower OR compared to those originating from Taiwan (OR 1.15 [95% CI 0.62-2.13], P = .65, I2 = 0%, random-effect models), although both findings did not reach statistical significance (Table 3).
When stratified by study design, prospective cohorts (OR 0.47 [95% CI 0.12-1.81], P = .27, random-effect models) demonstrated lower OR compared with retrospective cohorts (OR 0.98 [95% CI 0.68-1.42], P = .92, I2 = 0%, random-effect models); however, neither subgroup analysis yielded statistically significant findings (Table 3).
Analysis based on surgical approach revealed that studies limited to laparoscopic repair (OR 0.89 [95% CI 0.55-1.43], P = .63, I2 = 0%, random-effect models) produced OR similar to those that included both laparoscopic and open procedures for PPU management (OR 0.99 [95% CI 0.58-1.69], P = .96, I2 = 0%, random-effect models; Table 3).
Subgroup analysis according to ulcer site showed that the OR were similar across studies focusing mainly on duodenal ulcers (OR 0.94 [95% CI 0.57-1.56], P = .82, I2 = 0%, random-effect models), those examining primarily gastric ulcers (OR 1.05 [95% CI 0.37-2.97], P = .93, random-effect models), and those in which the ulcer location was not clearly specified (OR 0.88 [95% CI 0.47-1.68], P = .71, I2 = 0%, random-effect models; Table 3).
Finally, analysis stratified by perforation size indicated that studies with predominantly ≤5 mm defects (OR 0.70 [95% CI 0.39-1.26], P = .24, I2 = 0%, random-effect models) showed lower OR compared with those involving mainly perforations larger than 5 mm (OR 1.10 [95% CI 0.70-1.72], P = .68, I2 = 0%, random-effect models); however, neither subgroup yielded statistically significant outcomes (Table 3).
Secondary Outcomes
Postoperative Leak
The combined findings from 7 studies (n = 843) indicated that postoperative leak incidence did not differ significantly between PPU repair using simple closure technique and those using omental patch technique (OR 0.67 [95% CI 0.22-2.04], P = .48, I2 = 43%, random-effect models; Table 3).
Ileus
The pooled results from 3 studies comprising 331 participants demonstrated that the occurrence of ileus was not significantly different between patients undergoing simple closure and those treated with the omental patch for PPU repair (OR 0.76 [95% CI 0.27-2.14], P = .61, I2 = 0%, random-effect models; Table 3).
Excluding the study by Abd Ellatif et al 6 that has different definition of ileus in a sensitivity analysis did not meaningfully alter the pooled effect; however, the level of heterogeneity rose from 0% to 24% repair (OR 1.06 [95% CI 0.18-6.05], P = .95, I2 = 24%, random-effect models).
Surgical Site Infection
A meta-analysis of 4 studies involving 381 patients found no significant difference in surgical site infection rates between simple closure and omental patch techniques for PPU repair (OR 0.97 [95% CI 0.36-2.58], P = .95, I2 = 6%, random-effect models; Table 3).
Intra-Abdominal Collection
A pooled analysis of 4 studies (n = 449) demonstrated that the occurrence of intra-abdominal collection did not differ significantly between PPU repairs utilizing simple closure technique and those using omental patch technique (OR 1.15 [95% CI 0.23-5.72], P = .86, I2 = 0%, random-effect models; Table 3).
Reoperation
Based on 4 studies including 613 individuals, the pooled analysis indicated that reoperation rates were similar between PPU repairs performed with simple closure and those utilizing an omental patch (OR 0.66 [95% CI 0.32-1.33], P = .24, I2 = 0%, random-effect models; Table 3).
Mortality
Synthesis of data from 7 studies involving 873 patients showed no meaningful difference in mortality between PPU repairs performed with simple closure and those managed using an omental patch (OR 0.78 [95% CI 0.32-1.89], P = .58, I2 = 0%, random-effect models; Table 3).
Operating Time
Combined data from 7 studies involving 686 patients indicated that operating time was shorter in PPU repairs performed with simple closure compared with those using an omental patch (MD −21.73 minutes [95% CI −30.15 to −13.32], P < .00001, I2 = 82%, random-effect models; Figure 3A and Table 3).
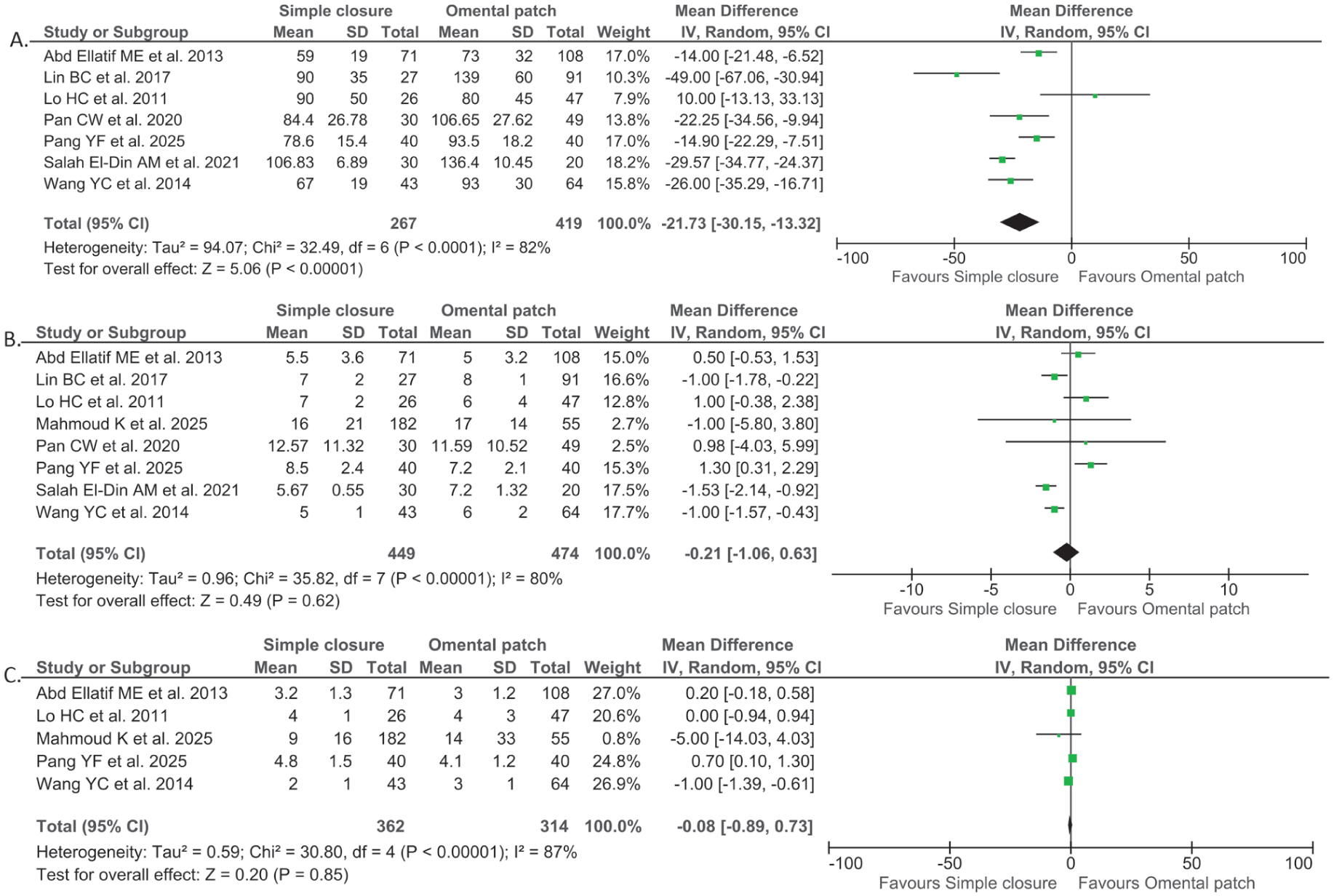
Forest plot depicting the operating time (A), length of hospital stay (B), and time to resume oral diet (C) in PPU repairs utilizing simple closure versus omental patch techniques.
Country-based subgroup analysis suggested that investigations from Taiwan (MD −23.19 minutes [95% CI −39.86 to −6.52], P = .006, I2 = 81%, random-effect models) tended to report higher mean differences than those carried out in other regions (MD −19.76 minutes [95% CI −30.64 to −8.89], P = .0004, I2 = 88%, random-effect models; Table 3).
When stratified by study design, prospective cohorts (MD −29.57 minutes [95% CI −34.77 to −24.37], P < .00001, random-effect models) demonstrated greater mean differences compared with retrospective cohorts (MD −19.97 minutes [95% CI −29.43 to −10.55], P < .0001, I2 = 77%, random-effect models; Table 3).
Analysis based on surgical approach revealed that studies limited to laparoscopic repair (MD −23.08 minutes [95% CI −32.76 to −13.39], P < .00001, I2 = 82%, random-effect models) produced higher mean differences than those that included both laparoscopic and open procedures for PPU management (MD −14.90 minutes [95% CI −22.29 to −7.51], P < .0001, random-effect models; Table 3).
Subgroup analysis according to ulcer site showed that the mean differences were highest among studies that did not specify the ulcer location in details (MD −27.68 minutes [95% CI −37.84 to −17.52], P < .00001, I2 = 82%, random-effect models), followed by those examining primarily duodenal ulcers (MD −16.62 minutes [95% CI −24.14 to −9.09], P < .0001, I2 = 21%, random-effect models), and finally those investigating primarily gastric ulcer, although the results for this specific subgroup did not reach statistical significance and only derived from 1 study (MD 10.00 minutes [95% CI −13.13 to 33.13], P = .40, random-effect models; Table 3).
Finally, in the subgroup analysis based on perforation size, statistical significance was observed only in studies where most perforations measured ≤5 mm (MD −27.55 minutes [95% CI −38.11 to −17.00], P < .00001, I2 = 83%, random-effect models), whereas studies with predominantly larger perforations (>5 mm) did not show significant results (MD −12.70 minutes [95% CI −25.45 to 0.05], P = .05, I2 = 66%, random-effect models; Table 3).
Sensitivity analysis using the leave-one-out approach showed that excluding individual studies sequentially did not substantially alter the pooled estimates, suggesting the results were stable and not disproportionately driven by a single study (Supplementary Figure 1).
Length of Hospital Stay
Combined data from 8 studies (n = 923) indicated no notable difference in the length of hospital stay between PPU repairs using simple closure technique and those employing omental patch technique (MD −0.21 days [95% CI −1.06 to 0.63], P = .62, I2 = 80%, random-effect models; Table 3).
Subgroup analysis by study location showed that research conducted in Taiwan (MD −0.50 days [95% CI −1.38 to 0.39], P = .27, I2 = 61%, random-effect models) reported a greater mean difference compared with studies from other regions (MD −0.04 days [95% CI −1.75 to 1.67], P = .96, I2 = 89%, random-effect models); however, neither subgroup demonstrated statistical significance (Table 3).
When analyzed by study design, statistical significance was observed in prospective cohort study (MD −1.53 days [95% CI −2.14 to −0.92], P < .00001, random-effect models), whereas retrospective cohorts did not demonstrate significant findings (MD 0.07 days [95% CI −0.85 to 0.98], P = .89, I2 = 76%, random-effect models; Table 3).
Subgroup assessment by surgical method indicated that studies incorporating both open and laparoscopic procedures showed a trend favoring the omental patch over simple closure (MD 1.21 days [95% CI 0.24-2.17], P = .01, I2 = 0%, random-effect models), while analyses restricted to laparoscopic repair alone demonstrated no significant difference between the 2 techniques (MD −0.53 days [95% CI −1.29 to 0.22], P = .17, I2 = 74%, random-effect models; Table 3).
Subgroup analysis according to ulcer site showed that the greatest reduction in the form of mean differences were highest among studies that did not specify the ulcer location in details (MD −0.62 days [95% CI −1.61 to 0.38], P = .22, I2 = 87%, random-effect models), followed by those examining primarily duodenal ulcers (MD 0.45 days [95% CI −0.53 to 1.44], P = .37, I2 = 0%, random-effect models), and finally those investigating primarily gastric ulcer, although the results for this specific subgroup only derived from 1 study (MD 1.00 days [95% CI −0.38 to 2.39], P = .15, random-effect models; Table 3).
Finally, in the subgroup analysis stratified by perforation size, studies predominantly involving perforations ≤5 mm demonstrated a significant reduction in hospital stay with simple closure technique compared to omental patch technique (MD −0.85 days [95% CI −1.54 to −0.16], P = .02, I2 = 73%, random-effect models). Conversely, in studies where most perforations exceeded 5 mm, the findings shifted to favor omental patch over simple closure (MD 1.13 days [95% CI 0.35-1.92], P = .004, I2 = 0%, random-effect models; Table 3).
Leave-one-out sensitivity analysis demonstrated that sequential exclusion of individual studies produced no notable changes in the overall effect estimates, indicating that the findings were consistent and not unduly affected by any single study (Supplementary Figure 2).
Time to Resume Oral Diet
Pooled evidence from 5 studies encompassing 676 patients showed that the time required to restart oral feeding was comparable between PPU repairs performed with simple closure and those utilizing an omental patch (MD −0.08 days [95% CI −0.89 to 0.73], P = .85, I2 = 87%, random-effect models; Table 3).
Subgroup analysis by study location showed that research conducted in Taiwan (MD −0.60 days [95% CI −1.56 to 0.37], P = .22, I2 = 73%, random-effect models) reported a greater reduction in the form of mean difference compared with studies from other regions (MD 0.39 days [95% CI −0.14 to 0.91], P = .15, I2 = 39%, random-effect models); however, neither subgroup demonstrated statistical significance (Table 3).
Subgroup analysis based on surgical approach showed that the mean differences were nearly equivalent between studies limited to laparoscopic repair (MD −0.29 days [95% CI −1.19 to 0.61], P = .53, I2 = 90%, random-effect models) and those that included both open and laparoscopic techniques (MD −0.30 days [95% CI −4.54 to 3.95], P = .89, I2 = 34%, random-effect models; Table 3).
When stratified by ulcer location, the largest mean difference was observed in studies focusing mainly on duodenal ulcers (MD −0.36 days [95% CI −3.53 to 2.81], P = .82, I2 = 21%, random-effect models), followed by those without clear specification of ulcer site (MD −0.17 days [95% CI −1.83 to 1.50], P = .85, I2 = 95%, random-effect models), while the smallest effect was seen in studies centered on gastric ulcers (MD 0.00 days [95% CI −0.94 to 0.94], P = 1.00, random-effect models; Table 3).
Finally, in the subgroup analysis stratified by perforation size, studies in which the majority of defects measured ≤5 mm (MD −0.40 days [95% CI −1.58 to 0.78], P = .51, I2 = 95%, random-effect models) demonstrated greater mean differences than those primarily involving perforations exceeding 5 mm (MD 0.39 days [95% CI −0.36 to 1.14], P = .31, I2 = 32%, random-effect models; Table 3).
Sensitivity analysis by removing a study by Wang et al that has slightly different definition of outcome reduced the observed heterogeneity from 87% to 19% without changing the overall significance of the findings (MD 0.31 days [95% CI −0.07 to 0.70], P = .11, I2 = 19%, random-effect models), thereby affirming the consistency and robustness of the overall findings (Supplementary Figure 3).
Publication Bias
Evaluation of publication bias could not be undertaken, as the number of available studies was fewer than 10, a threshold below which such analyses are considered unreliable.16,17
Discussion
This meta-analysis compared the surgical outcomes of simple closure and omental patch techniques for PPU. The pooled evidence demonstrated that simple closure was associated with significantly shorter operative time compared with omental patch, with the greatest benefit observed in laparoscopic procedures, in duodenal (post-pyloric) ulcers, and in perforations measuring ≤5 mm. No significant differences were identified between the 2 approaches in overall complication rates, including postoperative leakage, ileus, surgical site infection, intra-abdominal collection, reoperation, or mortality. Similarly, no meaningful differences were detected in hospital stay or time to resume oral diet, although subgroup analysis indicated that simple closure was linked with shorter hospitalization for perforations ≤5 mm.
The reduced operative time with simple closure likely reflects the technical simplicity of the procedure. Omental patch repair requires mobilization of the omentum and its fixation over the ulcer defect, steps that prolong the surgery. 4 This effect becomes more apparent in laparoscopic settings, where intracorporeal suturing is inherently more demanding, and additional maneuvers such as handling and anchoring the omentum further increase operative duration. 4 By contrast, direct closure without reinforcement eliminates these steps, thereby streamlining the repair. Although simple closure was associated with a statistically shorter operative time compared with omental patch repair, the clinical relevance of an ~20-minute difference warrants careful consideration. In hemodynamically stable patients, this magnitude of time saving is unlikely to independently influence major postoperative outcomes such as morbidity or mortality, particularly when weighed against other determinants of recovery including perforation size, degree of contamination, and timeliness of source control. In high-resource settings with ample operating room availability and standardized perioperative pathways, a modest reduction in operative duration may have limited impact on workflow efficiency or patient throughput.
Conversely, in resource-limited environments or high-volume emergency surgical units, even relatively small reductions in operative time may carry greater practical significance. Shorter procedures may translate into improved operating room turnover, reduced anesthesia exposure, and the ability to accommodate additional emergency cases, particularly where staffing, equipment, or theater availability is constrained. In critically ill or physiologically unstable patients, minimizing operative duration may also be advantageous as part of a damage-control approach. However, these potential benefits must be balanced against the overall safety and durability of the repair, which remain paramount. Therefore, operative time alone should not be considered a decisive factor in selecting between simple closure and omental patch, and its importance is likely context-dependent rather than universally clinically meaningful.
The enhanced benefit of simple closure for duodenal and smaller perforations can be explained by the tissue and anatomical context. Duodenal perforations are often characterized by firmer tissue margins than gastric ulcer that allow direct suturing with minimal tension, making reinforcement unnecessary.18,19 Small perforations (≤5 mm) provide an even more favorable setting, as the defect size falls within the limits where tissue approximation can be achieved without excessive tension.18,19 In larger defects or in gastric ulcers with more friable tissue, reinforcement with an omental patch may provide mechanical stability, explaining why the time-saving and hospitalization benefits of simple closure were most evident in carefully selected cases.18,19
Despite differences in operative duration, no disparities were noted in complication rates between the 2 techniques. The lack of significant differences in complication rates suggests that the biological healing of the perforation is not substantially affected by the use of omental reinforcement, provided that closure is technically adequate. Leak, infection, and mortality appear more closely linked to host factors—such as comorbidities, delay in presentation, and sepsis at the time of surgery—than to the choice of closure technique. 20 Likewise, resumption of diet and hospital stay were broadly similar, reflecting that the overall recovery trajectory in PPU surgery is influenced by systemic illness and perioperative care rather than subtle variations in surgical repair. 20 The observed shorter hospitalization with simple closure in small perforations may be a downstream effect of reduced operative time and less tissue manipulation, potentially facilitating earlier recovery.
These findings hold important implications for surgical decision-making. Simple closure may be considered a safe and efficient option in selected patients, particularly when laparoscopic repair is employed, when the ulcer is duodenal, and when perforation size is small. In these scenarios, avoiding omental patch not only reduces operative time but also appears to achieve comparable postoperative outcomes. Nevertheless, omental reinforcement remains valuable in larger perforations or when tissue integrity is questionable, as it may enhance mechanical security in higher-risk cases. Thus, surgical choice should be individualized based on ulcer characteristics, intraoperative findings, and surgeon expertise.
The findings of the present meta-analysis are broadly consistent with those reported by Demetriou and Chapman, 21 who likewise observed no statistically significant differences in major clinical outcomes between simple closure and omental patch repair for perforated peptic ulcer. Notwithstanding this overall agreement, several methodological distinctions between the 2 analyses merit consideration. The meta-analysis by Demetriou and Chapman 21 included 6 studies; however, only 1 directly compared simple closure with omental patch, whereas the remaining studies primarily evaluated variations of Graham patch techniques. As such, the scope of comparisons differed from that of the present analysis, which exclusively included studies providing direct comparisons between simple closure and omental patch repair. In addition, the earlier review assessed a limited set of outcome measures, whereas the current meta-analysis examined a broader range of perioperative and postoperative endpoints, including length of hospital stay, postoperative ileus, intra-abdominal collections, and reoperation rates, thereby offering a more comprehensive assessment of short-term outcomes. Furthermore, subgroup and sensitivity analyses were performed in the present study to explore potential sources of heterogeneity and to evaluate the robustness of pooled estimates, which were not extensively addressed in the prior review. These methodological differences may partly explain variations in analytical depth and highlight the complementary nature of the 2 studies in informing the existing evidence base.
Several limitations warrant consideration. First, the number of eligible studies was modest, and subgroup analyses in particular were based on relatively small sample sizes, which may limit statistical power. Second, all included studies were observational—predominantly retrospective cohort designs—and therefore inherently susceptible to selection bias, residual confounding, and inconsistencies in data recording. Surgeons’ decisions to perform simple closure or omental patch repair were not randomized and were likely influenced by clinical factors such as patient stability, ulcer size and location, degree of contamination, comorbid burden, and institutional resources. Because these factors were variably reported across studies, the ability to assess baseline comparability and adjust for confounders was limited. Third, substantial statistical heterogeneity was observed across several pooled outcomes, including time to oral intake, length of hospital stay, and operative duration, with I2 values frequently exceeding 70%. This inconsistency likely reflects variations in surgical technique (open vs laparoscopic approach, method of patch construction), ulcer characteristics, perioperative protocols, postoperative feeding pathways, and differences in institutional settings. Definitions of key outcomes also varied, further contributing to between-study variability. Although random-effects models were used to account for this heterogeneity, the wide prediction intervals indicate that the pooled estimates represent average associations across diverse contexts rather than effects consistently reproducible in any single clinical environment. Given these limitations, the results should be interpreted with caution. The observational and heterogeneous nature of the evidence reduces confidence in the effect estimates and precludes firm conclusions regarding comparative superiority of either technique. Well-designed prospective studies with standardized reporting and adequate adjustment for confounding are needed to validate and refine these findings. Fourth, although multiple subgroup analyses were performed, many were based on a limited number of studies and small sample sizes, resulting in low statistical power. As a result, these subgroup findings should be considered exploratory and interpreted with caution, as the analyses may be insufficient to reliably detect true differences between groups. Finally, publication bias could not be formally assessed due to the limited number of studies included in each outcome.
Future studies should focus on prospective, adequately powered trials to confirm the relative effectiveness of simple closure versus omental patch in different clinical contexts. RCTs stratified by ulcer size, location, and surgical approach (laparoscopic vs open) would provide more definitive evidence to guide practice. Standardized reporting of outcomes, particularly postoperative complications and recovery parameters, would enhance comparability across studies. Additionally, cost-effectiveness analyses may be valuable, as reduced operative time with simple closure could translate into meaningful resource savings in healthcare systems.
Conclusion
In summary, this meta-analysis indicates that simple closure is associated with a shorter operative time compared with omental patch repair for perforated peptic ulcer, with this difference more consistently observed in laparoscopic procedures, smaller perforations, and duodenal ulcers. Rates of postoperative complications, recovery-related outcomes, and mortality were broadly comparable between the 2 techniques. Given the observational nature of the available evidence and the potential for residual confounding, these findings should be interpreted as exploratory and hypothesis-generating rather than as strongly supported or definitive comparative conclusions. As such, they may serve as preliminary guidance to inform clinical decision-making in selected contexts, while underscoring the importance of individualized surgical judgment and the need for further well-designed prospective studies to clarify the relative roles of simple closure and omental patch repair across different clinical scenarios.
Supplemental Material
sj-docx-1-gut-10.1177_26345161261420287 – Supplemental material for Simple Closure Versus Omental Patch in the Surgical Management of Perforated Peptic Ulcer: A Meta-Analysis of Comparative Studies
Supplemental material, sj-docx-1-gut-10.1177_26345161261420287 for Simple Closure Versus Omental Patch in the Surgical Management of Perforated Peptic Ulcer: A Meta-Analysis of Comparative Studies by Andrea Hasudungan, Mona Galatia and Efrison Marudut in Foregut
Footnotes
Ethical Considerations
This is a systematic review and meta-analysis study. The Faculty of Medicine, HKBP Nommensen University Research Ethics Committee has confirmed that no ethical approval is required.
Author Contributions
Conceptualization: Andrea Hasudungan, Mona Galatia, Efrison Marudut. Methodology: Andrea Hasudungan, Mona Galatia, Efrison Marudut. Formal analysis and investigation: Andrea Hasudungan, Mona Galatia, Efrison Marudut. Writing—original draft preparation: Andrea Hasudungan, Mona Galatia, Efrison Marudut. Writing—review and editing: Andrea Hasudungan, Mona Galatia, Efrison Marudut. Resources: Andrea Hasudungan, Mona Galatia, Efrison Marudut. Supervision: Andrea Hasudungan, Mona Galatia, Efrison Marudut.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.