
Abstract
Resection for refractory peptic strictures at the gastroesophageal junction is often the option of last resort. While resection can be straightforward, the reconstruction options may vary depending on location of the stricture, surgeon experience, and other patient factors. We discuss 4 distinct reconstruction options, including gastric pull up to the upper chest or neck, roux-n-y esophagojejunostomy, colonic interposition, and jejunal interposition graft to the thoracic inlet or higher. Each has different considerations and potential complications. We recommend jejunostomy feeding tubes regardless of reconstruction planned.
Introduction
Resection of the gastroesophageal junction is typically the last resort for a refractory peptic or caustic stricture after all modalities to control the acid exposure, including medical management and fundoplication, and to address the stricture, including repeat dilations and other endoscopic therapy such as steroid injections and stents, have failed. Fortunately, the large majority of benign caustic and peptic strictures (over 90%) respond to these less morbid interventions.1,2 For patients that do not respond, have anatomically or functionally complex disease, or have associated esophageal organ failure, there are several options for surgical resection of the gastroesophageal junction with reconstruction. 3 It should be emphasized, that in the setting of benign disease, the decision whether or not to pursue a more complex surgical approach as well as which operation to perform should be centered around patient function and quality of life.
The objective of this chapter is to present surgical options for reconstruction of the gastroesophageal junction in conjunction with resection of a refractory stricture. We will emphasize surgical decision-making, describe surgical techniques, and discuss outcomes and complications.
Preoperative Evaluation and Decision-Making
While there are many etiologies for strictures at the gastroesophageal junction, we will focus on benign peptic and caustic strictures. Patients are often considered for surgical resection and reconstruction after multiple failed endoscopic interventions or in cases of unique complexity such as tortuosity, multiple esophageal/gastric strictures, or long segments of fibrosis. Preoperative evaluation should include upper endoscopy, barium esophagram, cross-sectional imaging (typically computed tomography) and function assessments such as manometry and pH testing when feasible. It is important to exclude malignancy, and biopsy should be performed for any concerning lesions prior to proceeding. Patient factors such as nutritional status, comorbidities, prior operations, and overall surgical risks should be considered. Key decision-making factors regarding surgical approach include location and length of the stricture and the condition of the stomach and small intestine. For example, a patient with a long segment stricture with fibrosis would not be suitable for a simple resection and esophagogastrostomy with fundoplication, or a patient with diffuse gastric disease is a poor candidate for a gastric pull-through. Pros and cons of the various surgical approaches, as well as general guidelines for patient triaging are described below. Generally, the best reconstruction is one that prioritizes simplicity, function, and durability. We advocate for placement of a jejunostomy feeding tube distal to all anastomoses as part of all reconstruction options.
Surgical Approaches: General Considerations and Operative Techniques
Distal/Partial/Total Esophagectomy (Transhiatal or Transthoracic Partial Esophagectomy) with Gastric Pull-Up or Advancement
Overview and Patient Selection
A distal, partial, or total esophagectomy with gastric pull-through can address more extensive disease while still maintaining some of the benefits of Nissen’s original technique such as the ability to use a local conduit, robust gastric blood supply, and single anastomosis (Figure 1).4,5 In this approach, a longer segment of distal esophagus and possible gastric cardia is removed, and the stomach is partially or fully mobilized into the chest and used as a conduit. This operation is suitable in cases of a shortened esophagus or poor esophageal motility. Cons include risk of complications (as high as >60%) including a 5% to 30% anastomotic leak rate. 6 As the lower esophageal sphincter is not reconstructed, patients may experience postoperative dysphagia or bile-reflux symptoms. Additionally, alterations in digestion can occur, particularly when a significant portion of the stomach is used to create the conduit.
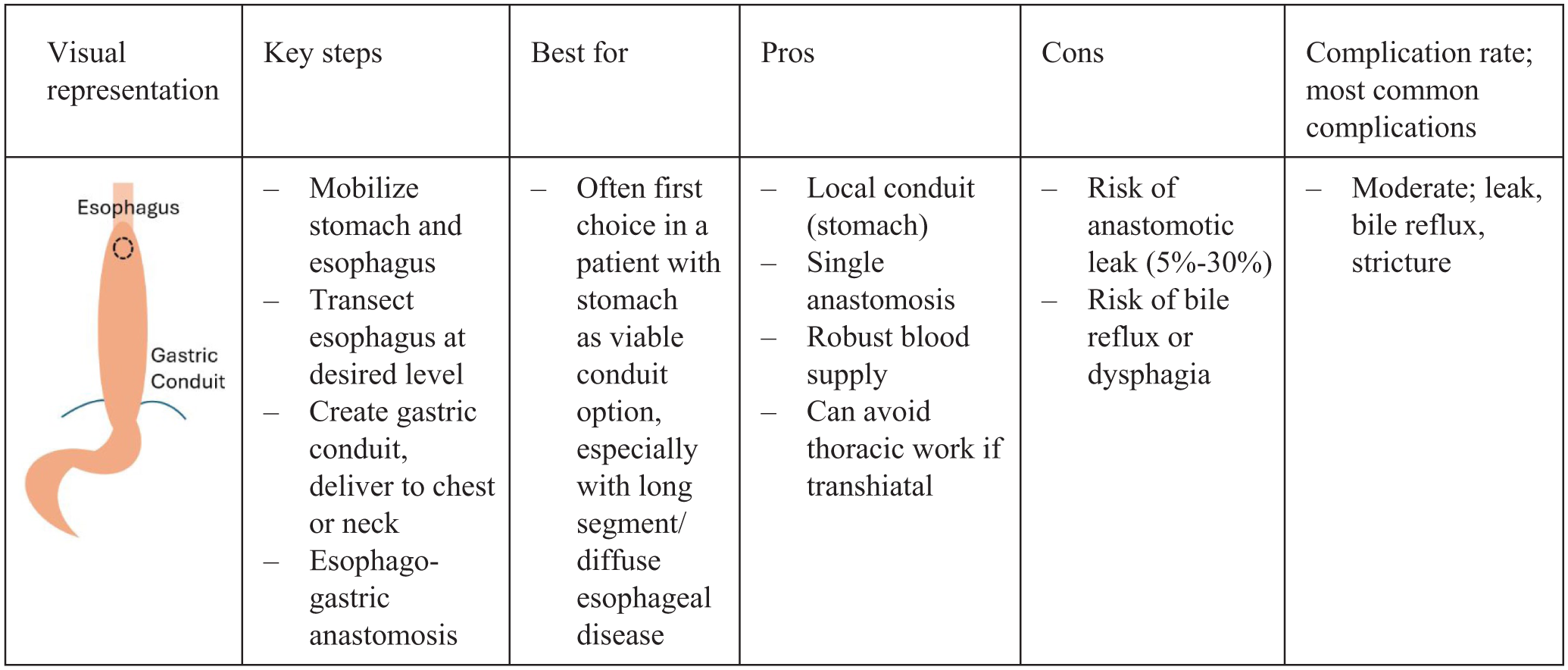
Gastric pull-up.
Operative Technique
There are multiple approaches including transhiatal, transthoracic (Ivor Lewis), and three-hole (McKeown) with a variety of open and minimally invasive approaches possible. While a transthoracic or three-hole esophagectomy provides excellent visualization for dissecting mediastinal lymph nodes, the transhiatal is often preferred in benign disease when feasible, since lymphadenectomy and en bloc resection are no longer applicable as in a cancer operation, to avoid a chest incisions and unnecessary morbidity.
The transhiatal esophagectomy with cervical esophagogastric anastomosis is summarized here.7,8 Abdominal access via upper laparotomy or port placement is achieved. The stomach and esophagus are mobilized up to the level of the carina or higher. A Kocher maneuver is performed when complete mobilization of the stomach into the chest is required. A pyloromyotomy may be performed. A jejunostomy tube is placed. Attention is now turned to the neck where an incision is made along the anterior border of the left sternocleidomastoid muscle. The omohyoid muscle is divided, carotid sheath is retracted laterally, and the trachea and thyroid are rotated medially to expose the esophagus which is bluntly dissected from surrounding structures. The upper thoracic esophagus is bluntly mobilized in the superior mediastinum starting posteriorly. Then working from the diaphragmatic hiatus, blunt dissection of the thoracic esophagus is completed. The upper esophagus is now delivered through the neck incision and divided. The stomach and mid/distal esophagus are delivered out through an abdominal incision, and the blunt dissection field should be inspected for bleeding. The esophagus and proximal stomach (as indicated based on pathology) are now separated from the remaining stomach (future conduit), and the conduit is examined for perfusion. The conduit is then gently passed to the neck, any hiatal defect is closed, and the jejunostomy tube is delivered out of the abdomen. Next, the cervical esophagogastric anastomosis is completed, ensuring adequately perfused tissue. The neck is irrigated, a drain is placed, and the neck is closed in layers.
The transthoracic approach involves a similar abdominal mobilization, followed by a right thoracotomy/thoracoscopy. The gastric conduit may be partially formed, but not completely, so that the conduit can be pulled into the chest. The esophagus and gastric conduit are pulled up into the chest and the middle and proximal esophagus are dissected to the level of the azygous or higher. The azygous is often transected. The esophagus can be stapled across. An esophago-gastric anastomosis is created. Drains or chest tubes are placed next to the anastomosis and the wound sites closed. The conduit is placed as high in the chest as possible minimized bile reflux symptoms postoperatively.
Outcomes
Dr. Orringer reported on the transhiatal esophagectomy with gastric conduit in almost all patients and found good or excellent functional results in ~70% of patients, and though 44% required one or more anastomotic dilations, true anastomotic strictures developed in just 10%. 9 Another study examining esophagectomy (any approach) after at least one prior anti-reflux procedure (with the stomach used as the conduit in 88% of patients) reported leaks in 22%, reoperation rate of 20% and complication rate 63%. 6
Distal Esophagectomy with Esophagojejunostomy via Roux-en-Y Reconstruction
Overview and Patient Selection
A Roux-en-Y esophagojejunostomy is one option that is particularly useful when the stricture is low on the esophagus such that the distal esophagus can be easily accessible after resection through the abdomen, especially when the stomach is not a suitable conduit (Figure 2). Advantages to this approach is the high rate of improvement in reflux, ability to address obesity simultaneously, and typically avoids a thoracotomy or neck incision. Cons include multiple anastomoses, potential for nutritional challenges like vitamin B12 deficiency or dumping syndrome when total or subtotal gastrectomy is performed, often requiring lifelong vitamin supplementation and dietary modifications. Roux-en-Y is typically not suitable if there is more proximal pathology in the esophagus due to constraints of the Roux limb reaching to the chest or neck easily.
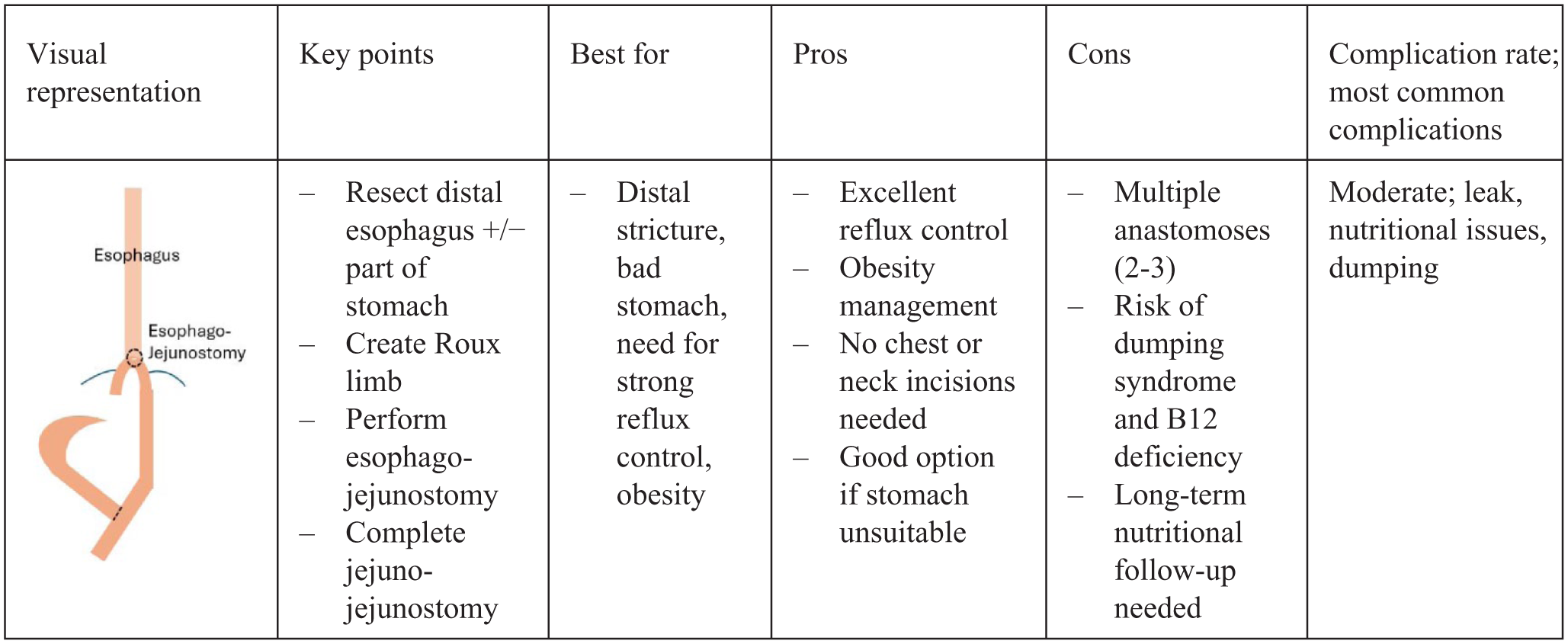
Roux-en-Y esophagojejunostomy.
It should also be noted that a “double-tract” reconstruction is also an option, which is an operation in which an additional anastomosis is made between the jejunal roux limb (about 10-15 cm distal to the esophagojejunostomy) and the proximal stomach. This provides two pathways for food; both through the typical Roux limb, as well as through the remnant stomach. This allows for nutritional benefits of food passing through the stomach which may include decreased weight loss and fewer nutritional deficiencies, but may also increase the risk of reflux and does require an additional anastomosis. 10
Operative Technique
While many limb/anastomosis configuration options and approaches exist, a retrocolic Roux limb with linear stapled anastomoses and near-total gastrectomy with no “double tract” reconstruction will be described here. After entry into the abdomen, the esophagus and proximal stomach are mobilized. If total or subtotal gastrectomy is to be performed, the entire greater curvature is mobilized from the omentum followed by opening the lesser omentum and dividing the left gastric artery. The right gastric and right gastroepiploic arteries are often preserved in cases of proximal subtotal gastrectomy. If performing a subtotal gastrectomy, pyloroplasty or pyloromyotomy should be considered due to possible impairment of gastric emptying. Next, the esophagus is divided just above the stricture and the stomach is divided with a linear stapler usually at the mid-antrum, and the specimen is removed.
The Roux limb is then prepared by transecting the jejunum ~20 to 30 cm from the ligament of Treitz. Then measure ~40 cm (variable depending on patient, but this distance or greater should result in low bile reflux risk) and mark the spot with silk for future jejunojejunostomy. The Roux limb is then brought through a small opening in the transverse mesocolon (if retrocolic) to reach the esophageal hiatus. If there is tension, further mobilization of attachments along the inferior border of the pancreas or spleen may provide further length. Occasionally, division of the middle colic artery may be needed to free the root of the small bowel mesentery if the limb is to reach high into the chest, but this is rarely necessary. Next, the anastomosis between the esophagus stump and Roux limb is created. Perfusion, tension, and orientation should be assessed. Then the side-to-side jejunojejunostomy is created between the cut end of the biliopancreatic limb and the previously marked position on the jejunum (40 cm distal to the esophagojejunostomy in this example). Care should be taken to ensure only a small “blind end” of the Roux limb is present beyond both anastomoses to prevent stagnant loop issues. Mesenteric defects should be closed to prevent the risk of future internal herniation. Leak test of the esophagojejunostomy is often performed, and drains and nasoenteric tube can be placed at the surgeon’s discretion. The abdomen should be inspected for perfusion, lack of anastomotic tension, and correct orientation prior to closure. A jejunostomy tube can be placed distal to the jejuno-jejunostomy also based on clinical circumstances and surgeon preference.
Outcomes
The Roux-en-Y esophagojejunostomy approach provides excellent anti-reflux results. Mortality was 4.6%, complications 22%, and anastomotic leak 6% according to one meta-analysis of five studies. 11 Other studies demonstrate similar results, though typically report a lower mortality.12,13 Notably many studies include patients who technically have a gastrojejunal anastomosis rather than a true esophagojejunal anastomosis. 13 Likely, many patients experience nutritional deficiencies and dumping, and all patients require nutritional considerations postoperatively. Weight loss is common and potentially advantageous.
Distal/Partial/Total Esophagectomy with Colonic Interposition
Overview and Patient Selection
A colonic interposition typically involves the right colon, but the left is used with some frequency as well (both along with the transverse colon; Figure 3). 14 It is often reserved for cases where the stomach is not a suitable conduit and can be the favored 2nd conduit of choice to reach into the neck for a larger esophageal resection. The colon can provide a long and robust conduit with a good blood supply, is relatively resistant to acidic injury, and the right colon can include the ileocecal valve which may decrease reflux. 14 The use of the colon can be challenging in obese patients due to a thickened mesentery and challenges in getting the colon to reach to the upper chest or neck. The presence of diverticulitis or colonic tumors may preclude the use of the colon. Poor arterial blood flow can also be a contraindication, or alternatively may indicate the need to supercharge the proximal conduit. Challenges include three anastomoses, potential for development of native pathology, potential for redundance or future redundance as the conduit may lengthen over time, and a lack of peristalsis. The colon interposition is a technically demanding procedure and has the potential for higher morbidity and therefore should be performed only by experienced surgeons. However, when done successfully, the reconstruction is robust and ideal for many patients with complex pathology, especially when large segments of esophagus and stomach are involved or have previously been operated on.
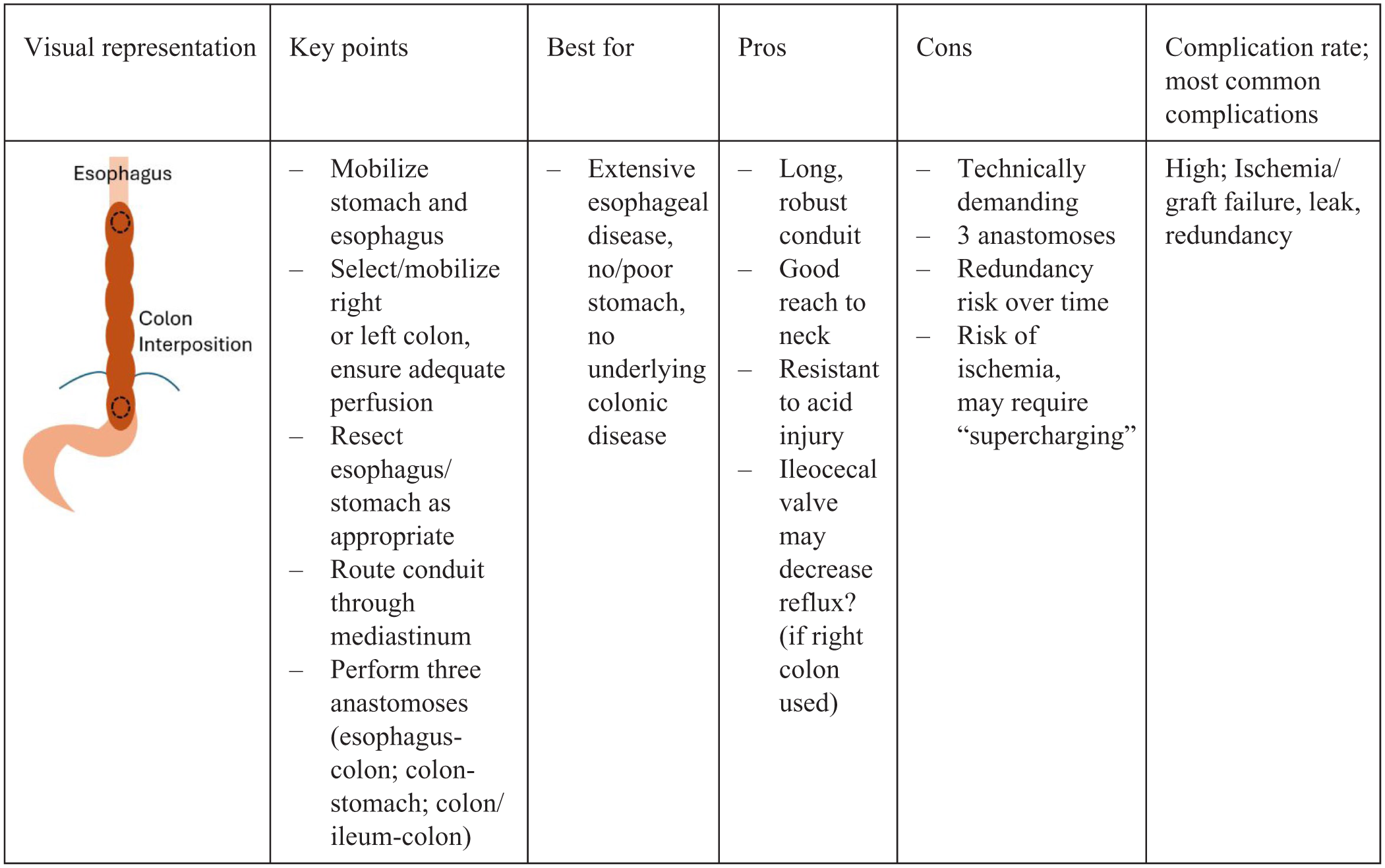
Colon interposition.
Surgical Technique
There is significant variability to approach (right versus left colon, iso- versus antiperistaltic, and use of “supercharging” technique). A transhiatal right colonic isoperistaltic interposition placed in the posterior mediastinum will be described here.
All patients should undergo preoperative colon evaluation with colonoscopy or barium enema. An angiogram can also be performed to identify arterial anatomy. Much of the operation, including esophagectomy and cervical esophagus preparation, mirrors that described above for the transhiatal esophagectomy with gastric pull-up. For right colon graft harvest, the lateral attachments are taken down to the hepatic flexure, then the right colic and middle colic arteries are transilluminated, clamped to test the future conduit, then divided proximally such that the inferior mesenteric artery and left colic artery provide the blood supply to the remaining colon. 14 On table ultrasound can be used to test the marginal artery blood supply after clamping of the colic branches, prior to ligation. Of note, vascular anatomy of the right colon is more variable than the left, and some may alternatively choose to preserve the middle colic artery. The ascending colon is transected just above the cecum and then near the splenic flexure, and the colon is passed through the posterior mediastinum. The esophagocolonic anastomosis is performed the same way as described above using the gastric conduit, with the staple line along a taenia coli. If there are concerns on colonic perfusion at the proximal aspect, super-charging may be performed, where a vascular pedicle can be implanted into the carotid artery and internal jugular vein, typically with the assistance of a surgeon proficient in microvascular anastomoses. This arrangement requires anticipation and detailed planning. The distal transverse colon is then anastomosed to the gastric remnant (or to a Roux-en-Y limb of jejunum when no gastric remnant is available). Finally, the cecum is anastomosed to the transverse/left colon or an ileocolic anastomosis may be preferred. 15 We favor placing a jejunostomy feeding tube to allow for enteral feeding in the case of anastomotic leak.
Outcomes
Colon graft failure is estimated to occur 0% to 14% of the time, and there is evidence this is less common at high volume centers. Mortality is estimated between 0% and 17% and is lower at high volume centers. Anastomotic stricture rate is 0% and 32%. Pulmonary complications (such as aspiration and pneumonia) are the most common postoperative complication and occur in 7% and 50%, likely lower with a transhiatal approach. 75% and 100% of patients are ultimately able to resume an oral diet. 14
Distal/Partial/Total Esophagectomy with Jejunal Interposition (Including Merendino Procedure)
Overview and Patient Selection
The Merendino procedure is one type of jejunal interposition which involves a relatively short segment (~10-15 cm) proximal jejunal pedicled conduit whose proximal end is anastomosed to the esophagus and distal end is anastomosed to the stomach after short-segment gastroesophageal junction resection (Figure 4). Other options for jejunal interposition may involve a longer segment of jejunum (~20+ cm) with blood supply provided by a vascular pedicle or a free flap requiring microsurgical vascular anastomosis. Some favor transecting the vascular pedicle up front in favor or a straight conduit (a true free flap) which likely carries a higher risk of ischemia or venous congestion, while others keep the vascular arcade intact during the supercharge to improve the venous drainage while accepting a slightly tortuous conduit (augmented conduit).
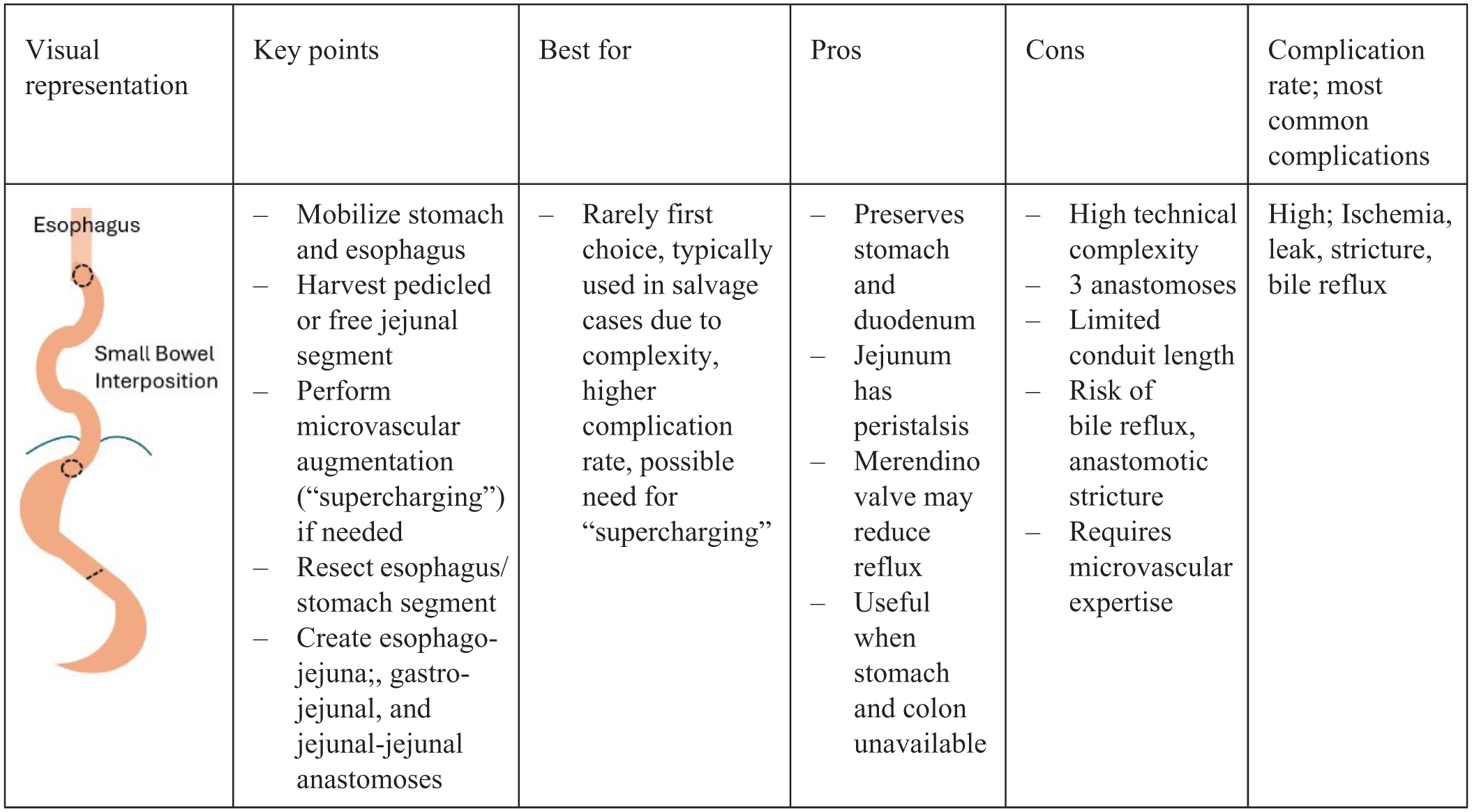
Jejunal interposition.
Pros of jejunal interpositions include largely preserved stomach and duodenum, reducing post-gastrectomy symptoms such as poor nutrition or dumping syndrome. There is also significant redundant jejunum, and it typically lacks intrinsic pathology and also includes peristalsis. 14 The Merendino procedure uses a short jejunal segment and includes a built-in reflux “valve” since a segment of jejunum connects the esophagus to the stomach in a way that creates a flap-valve mechanism to decrease reflux.
Cons include high complexity and evidence for high perioperative complication rate and conversion rate to Roux-en-Y within 1 year of surgery; 67% and 25% respectively in one study of 12 patients who underwent the Merendino procedure. 16 There are also three anastomoses, two of which may be in a heavily scarred field. Functional issues can include difficulty with food passing through the often twisted jejunal conduit, delayed emptying at the interposition, and bile reflux. There is also general lack of high-quality evidence regarding this approach due to relative lack of high-volume surgeon experience, and lack of standardized technique. Additionally, a jejunal free flap may not be suitable for a total/subtotal esophagectomy due to limitations in length, and relative contraindications include past abdominal surgeries, limited cardiovascular and pulmonary function, history of thrombotic events or other atherosclerotic disease of the mesenteric vessels. 15 This approach is often “last resort” and for patients who are not good candidates for colon or stomach conduits and should be performed at an experienced facility.
Surgical Technique
The majority of the operation mirrors that of the colonic interposition. While there are many technique variations, a long segment jejunal interposition with cervical anastomosis which incorporates both distal pedicled blood flow and a proximal microvascular anastomosis is described.14,17 A segment of jejunum is selected approximately 20 cm from the ligament of Treitz such that the first jejunal arterial branch and associated intestine is preserved. Next, the second (for future microvascular anastomosis) and third (simply for length) jejunal branches are typically divide, and the fourth jejunal branch is preserved and will ultimately supply the distal conduit. After broadening the mesentery, the jejunal conduit can be tunneled through the posterior mediastinum, retrosternal, or substernal positions, with possible resection of the left sternoclavicular joint and left hemimanubrium depending partially on the track of the conduit and the location of the future anastomosis. The second jejunal branch is then anastomosed to the internal thoracic artery for inflow (or “supercharged” via cervical vasculature anastomosis), which is typically performed by a microvascular surgeon, followed by venous anastomosis in a similar fashion or using a venous coupler. The esophagojejunal anastomosis is then executed, followed by the gastrojejunal anastomosis and bowel continuity is restored with jejunojejunal anastomosis.
Outcomes
Jejunal conduits are uncommon, so reports on outcomes are more limited. Anastomotic leak rates are between 0% and 36%, the operation carries a relatively high reoperation rate anywhere between 0% and 50%. In hospital mortality is approximately 0% to 5%, with the most common complications being respiratory (pneumonia, aspiration) at 7% to 37%. Resumption oral intake is possible in 80% to 100%. Overall favorable quality of life is reported after surgery.14-16
Final Thoughts and Summary
Critical to all reconstruction options after esophagogastric junction reconstruction are preoperative planning for appropriate choice of approach and conduit, and intraoperative maximization of functional anatomy, anastomotic perfusion, and avoidance of tension. We generally favor the Roux-N-Y esophagojejunostomy through the abdomen or esophagectomy with gastric pull-up for first line therapy. If these aren’t options, then a colon interposition or lastly a small bowel interposition could be considered (Figure 5). It is important to remember that the surgical plan may change intraoperatively based on patient condition and operative findings such as fibrosis, poor conduit suitability (inflammation or ischemia), unresolvable tension, and therefore being prepared with back-up options is essential. It should be emphasized that the reconstructions proposed here are often complex and in scarred reoperative surgical fields. Complications may be higher in low-volume centers, so necessary expertise and support is critical, and choice of approach should partially depend on surgeon experience. 14 It is also worth mentioning that in patients where reconstruction is not feasible or practical, for example in the critically ill patient, the option to delay formal reconstruction with placement of a nasogastric or jejunal feeding tube is reasonable and advisable with referral to a higher volume center in the future.
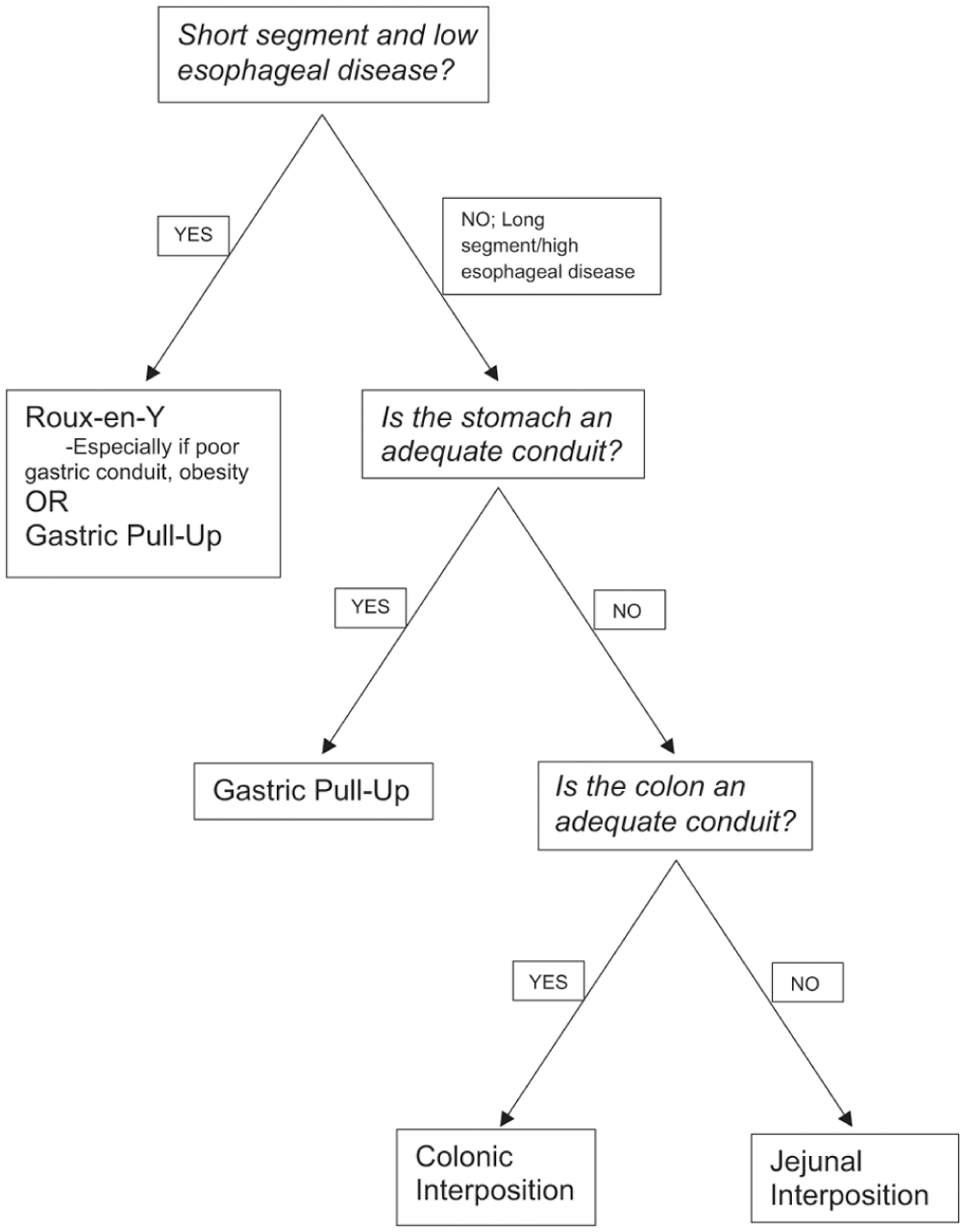
Flow diagram for operative approach to reconstruction.
Footnotes
Ethical Considerations
Ethical approval is not required for this manuscript.
Author Contributions
Ward (literature search, manuscript preparation, editing), Bui (literature search, editing), Reddy (manuscript preparation, editing, supervising).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
Ward/Bui-None, Reddy-Consultant to Intuitive Surgical, Inc, Atricure, and On Target Laboratories (Advisory Board and Grants), Medtronic and Genentech (Advisory Board), BMS (Speaker), Trinity Health (Consultant).
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.