
Abstract
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated esophageal disease increasingly encountered by surgeons across foregut practice, presenting as dysphagia, food bolus impaction, and fibro stenotic strictures. Although medical and dietary therapies are first-line, surgeons play a critical role in perioperative recognition, obtaining diagnostic biopsies at the index endoscopy, and endoscopic management. This clinically focused review highlights clinical cues for EoE, best practices for endoscopy and biopsies, pathophysiology, and operative planning considerations, and evolving treatment paradigms. Durable outcomes require multidisciplinary coordination to optimize inflammation, prevent recurrent fibro stenosis, and avoid inappropriate operations or reoperations.
Introduction: Why EoE Matters to Surgeons
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory disease of the esophagus that has emerged over the past 3 decades as one of the most common causes of dysphagia and food impaction in adults. However, EoE occurs across the age spectrum, from early childhood through older adulthood, presenting with various symptoms evolving with age and disease chronicity. With a prevalence approaching 1 in 1000 in Western populations and a rising incidence, 1 EoE is no longer a diagnosis confined to gastroenterology or allergy clinics, and is now a condition that surgeons across multiple disciplines encounter regularly—often without recognizing it.
The relevance of EoE to surgeons is broad. It is a leading cause of dysphagia and food impaction that can trigger surgical referral, it can masquerade as (or coexist with) gastroesophageal reflux disease (GERD), and its fibro stenotic sequelae mimic peptic stricture. When EoE goes unrecognized perioperatively, the risk is operating on the wrong problem. When the diagnosis is missed postoperatively, recurrent symptoms may be incorrectly attributed to a “tight wrap” and potentially lead to an avoidable reoperation. Surgeons may face EoE in the evaluation of esophageal strictures and in the management of complications such as perforation and food impaction. In many cases, as endoscopists, surgeons may be the first clinician to make a diagnosis of EoE, but only if a clinical suspicion is high to prompt sufficient and appropriate biopsies. Because EoE is a chronic condition with a characteristically long diagnostic delay — one associated with progressive fibro stenotic remodeling and stricture formation — earlier recognition represents an opportunity to initiate treatment, improve symptom control and quality of life, and potentially prevent long-term complications and disease progression. 2
This review emphasizes what surgeons and endoscopists need at the point of care: when to suspect EoE, how to confirm the diagnosis, practical management of beyond dilation of strictures, and guidance for managing co-occurring conditions.
The Surgeon’s Role in EoE: Perioperative Recognition and Procedural Planning
Before turning to diagnostic criteria and treatment considerations, it is useful to define the surgeon’s role in EoE. Although EoE is established by clinicopathologic criteria, surgeons and endoscopists often determine whether the diagnosis is even considered by recognizing clinical cues, obtaining appropriate esophageal biopsies at the index endoscopy, and documenting the degree of fibro stenotic remodeling (eg, rings, strictures, narrow caliber esophagus) in a way that informs procedural risk and technique. For patients being evaluated for foregut operations, EoE should be considered in symptom attribution, operative planning, and expectations for postoperative dysphagia. Awareness of EoE-related tissue stiffness and fragility may support staged dilation, deferment of elective intervention until inflammation is better controlled, or a more conservative approach when dilation is needed. In these ways, the surgeon’s role may not primarily in long-term disease management, but perioperative recognition, procedural planning, and coordination with gastroenterology colleagues to ensure that procedures are paired with maintenance therapy and disease control. Surgeons also remain important in recognizing complications such as perforation, although detailed management of EoE-related complications is addressed in Dr. Dellon’s companion article, “Assessment, treatment, and prevention of complications in EoE.”
Natural History of EoE
EoE affects children and adults worldwide, with the highest reported prevalence in North America and Europe. 3 It is more common in males and in patients with atopic disease (asthma, allergic rhinitis, eczema, food allergy). Symptom onset often precedes diagnosis by years; that delay is clinically consequential because ongoing inflammation drives fibro stenotic sequelae such as rings, strictures, and narrow-caliber esophagus. EoE is increasingly understood as a progressive disease — one that begins with esophageal inflammation but evolves toward fibro stenosis and stricture formation through remodeling over time. 4 This understanding of its natural history is supported by the clinical observation that younger patients tend to present with a predominantly inflammatory phenotype, while adults with longstanding disease show a markedly higher prevalence of esophageal strictures and scarring. This remodeling has direct procedural implications as chronic inflammation can reduce esophageal compliance and distensibility, resulting in a stiff, ringed, or diffusely narrowed lumen. This may translate to persistent dysphagia despite therapy, technical difficulty with passing bougie dilators, and increased risk of mucosal disruption and post-procedural pain after endoscopy. These features should inform preprocedural planning: strictures, narrow caliber, and mucosal fragility may warrant control of inflammation before an elective surgery, smaller-caliber or staged dilation techniques, and heightened caution to reduce mucosal injury or perforation risk.
Clinical Presentation and When to Suspect EoE
The classic clinical presentation of EoE is in young-to-middle-aged males with atopic conditions. However, it is important to remember that EoE can affect any age, race, gender or ethnicity so should be suspected in all patients with symptoms of dysphagia. The dominant symptom of EoE in adults is dysphagia to solid foods—characteristically for meats, breads, and dense textures— often long-standing, intermittent, and minimized by the patient through adaptive or modified eating behaviors. Many patients modify their eating habits for years before presenting - cutting food into very small pieces, chewing excessively, eating slowly, drinking copiously with meals, or simply avoiding problematic foods or pills altogether.5,6 Because these adaptations become habitual, patients frequently do not volunteer dysphagia as a complaint, may not recognize it as abnormal, and describe their symptoms in various ways including choking, chest pain, episodes, or flares. Symptoms are commonly dismissed — by patients and providers alike — as the result of eating too quickly, not chewing enough, stress or anxiety. Because patients can commonly unconsciously minimize their symptoms (“I’ve always eaten this way”), a careful history from the patient (or often time friends and family members) and keen index of suspicion is key to making a diagnosis. A personal history of atopic conditions (asthma, eczema, allergic rhinitis, food allergy) can raise our pretest probability. Non-cardiac chest pain and symptoms that resemble heartburn are also common, and refractory esophageal strictures labeled as “peptic” without a convincing reflux history should raise immediate suspicion for fibro stenotic EoE (Table 1).
When to Suspect EoE.
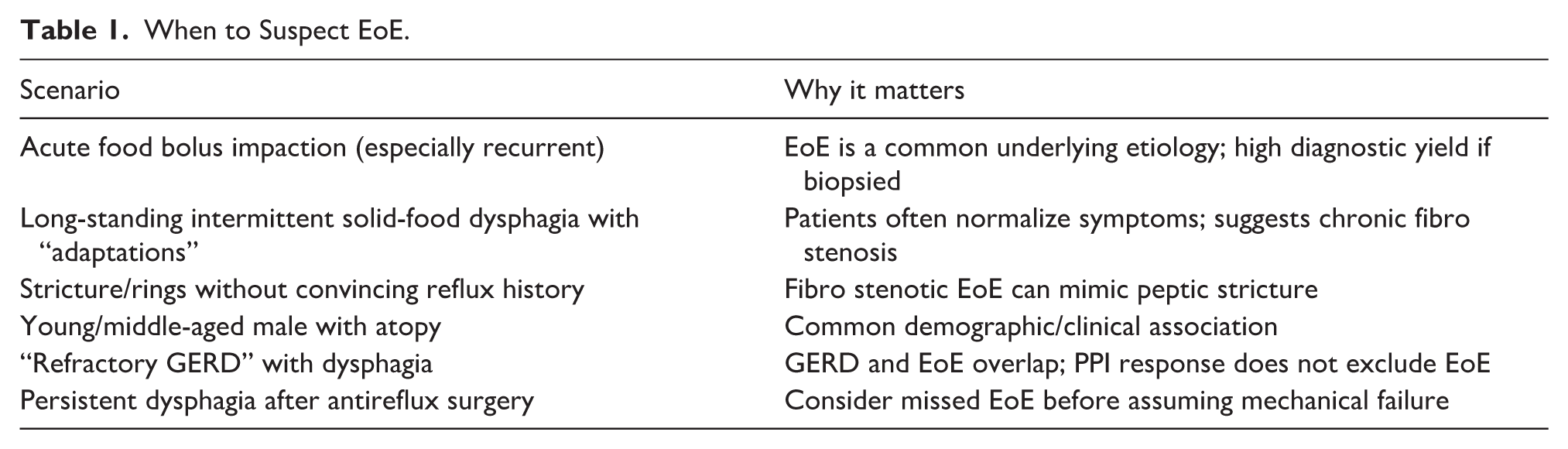
Acute esophageal food bolus impaction is a common initial presentation of EoE in adolescents and adults, often the precipitating event that brings an EoE patient to surgical attention and often the first time a diagnosis is considered. 7 The management of food bolus impaction and strategies to prevent complications during impaction are reviewed in the companion article, “Assessment, treatment, and prevention of complications in EoE.”
In children and adolescents, the symptom profile of EoE is more variable. 5 Infants and young children may present with feeding difficulties, food refusal, failure to thrive, or vomiting — symptoms that are easily attributed to other common childhood conditions and that rarely prompt consideration of an esophageal diagnosis. School-aged children can present with vomiting, regurgitation, and abdominal or chest pain, while dysphagia may not be a prominent complaint. Across all pediatric age groups, symptoms are frequently nonspecific, and a history of atopic disease (eg, asthma, allergic rhinitis, eczema, food allergy) may provide an important clue. As in adults, adaptive eating behaviors are common in older children and adolescents and can be easily overlooked.
Diagnosing EoE
Clinical Symptoms
A diagnosis of EoE is made based on a combination of symptoms of esophageal dysfunction, upper endoscopy with esophageal biopsies showing mucosal eosinophilia (≥15 eosinophils per high-power field in the esophageal epithelium), and exclusion of other causes of esophageal eosinophilia. 8
Endoscopic Evaluation
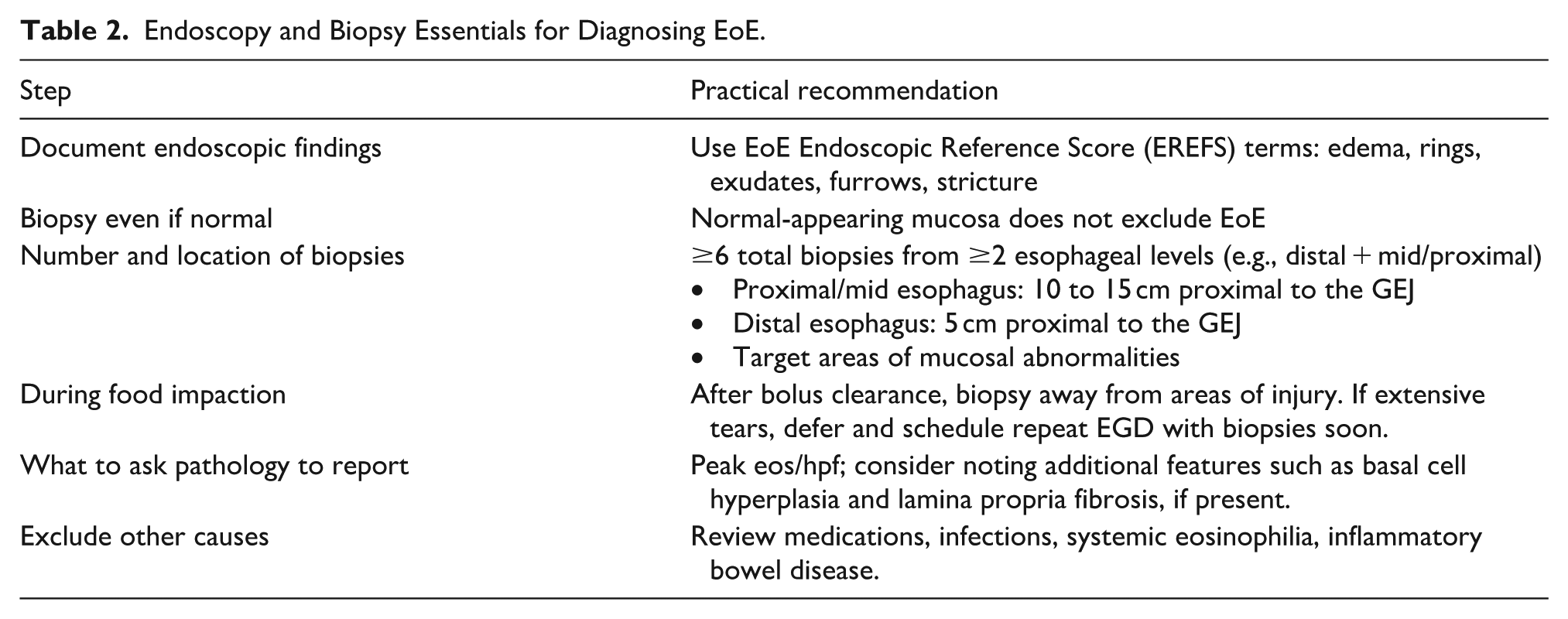
Classic mucosal findings of EoE seen on upper endoscopy include fixed concentric rings (“trachealization”), longitudinal furrows, white exudates, mucosal edema with loss of vascular pattern, and focal or diffuse structuring. However, in a proportion of patients, the esophageal mucosa can appear grossly normal or these findings may be subtle and missed on a quick review. For example, inflammatory exudates may appear as fine white specks on initial endoscope insertion of the endoscope and can be washed away, and therefore missed, after irrigation. Therefore, a normal-appearing esophagus does not exclude EoE, and biopsies must be obtained regardless of endoscopic impression whenever EoE is on the differential. To describe these typical mucosal findings of EoE with a standardized framework, the EoE Endoscopic Reference Score (EREFS) spells out the common features — Edema, Rings, Exudates, Furrows, Strictures – and improvement in the endoscopic appearance ought to be a treatment endpoint (Figure 1). 9 As esophageal biopsies are a diagnostic cornerstone, they must be obtained correctly. Because EoE can be a patchy disease, ensuring that adequate biopsies are taken from multiple levels (eg, distal + mid/proximal) is essential. Sampling only the distal esophagus or the gastroesophageal junction will miss a proportion of cases. 10 Clinical guidelines recommend at least 6 biopsies from 2 or more esophageal levels (eg, distal and mid-to-proximal) be obtained, targeting abnormal-appearing areas should be targeted (eg, furrows, exudates) to increase diagnostic yield (Table 2). 11
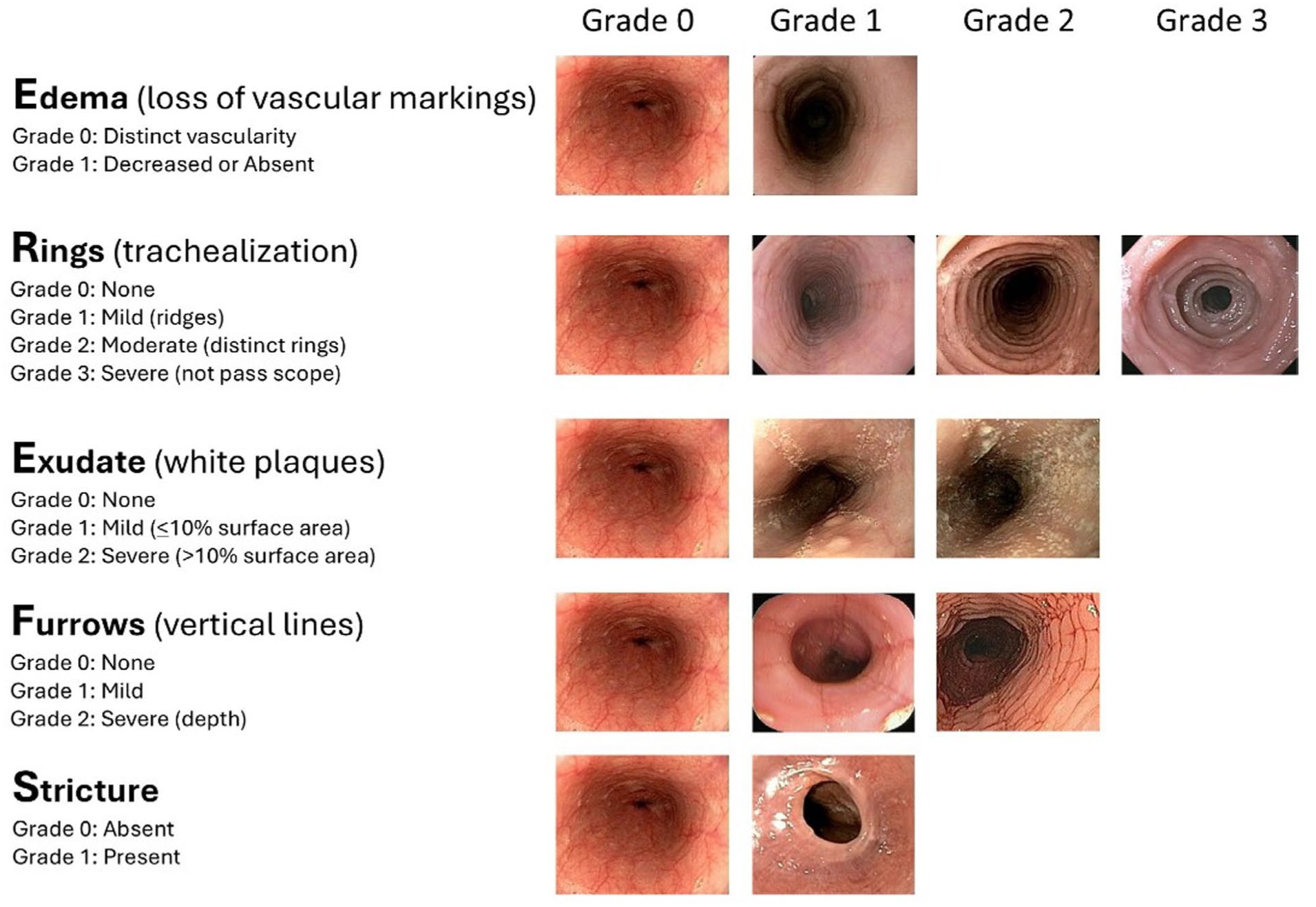
Eosinophilic esophagitis endoscopic reference score (EREFS).
Endoscopy and Biopsy Essentials for Diagnosing EoE.
Histopathology
The esophagus is unique among the gastrointestinal tract in that eosinophils are absent from the healthy mucosa, so eosinophils in the esophageal epithelium indicate an underlying pathologic process. A diagnosis of EoE requires ≥15 eosinophils per high-power field from multiple levels of the esophagus, but additional histologic features can provide additional context on disease chronicity and remodeling.12,13 Basal cell hyperplasia and dilated intercellular spaces reflect epithelial injury from ongoing inflammation. Eosinophilic microabscesses or clusters of degranulating eosinophils and surface layering suggest active, high-burden disease. Lamina propria fibrosis reflects remodeling and disease chronicity, and potentially predicts reduced esophageal compliance.
Differential Diagnosis: Other Causes of Esophageal Eosinophilia
In a patient with compatible symptoms and esophageal eosinophilia on biopsy, the diagnosis of EoE is confirmed after other causes are reasonably excluded. Alternative causes of esophageal eosinophilia are important when the clinical picture is atypical or treatment fails. GERD is the most common consideration, as it can produce low-level esophageal eosinophilia. Additionally, GERD can also coexist with EoE, so eosinophilia in a reflux patient should not automatically be attributed to excessive acid exposure. Other causes include pill esophagitis, fungal or viral infections, Crohn’s disease with esophageal involvement, eosinophilic gastrointestinal disease, hyper eosinophilic syndrome, drug hypersensitivity reactions, and connective tissue or autoimmune disorders. Achalasia and other motility disorders can coexist with EoE and can precipitate secondary esophageal eosinophilia, complicating the interpretation of both manometry and histology. When the clinical picture is atypical—prominent weight loss, liquid dysphagia, regurgitation-predominant symptoms, or a poor response to anti-inflammatory therapy—additional workup including manometry and ambulatory pH-impedance testing should be pursued in collaboration with gastroenterology before committing to any therapeutic intervention.
Surgical Planning When EoE Overlaps With Foregut Disease: Preventing the Wrong Operation (or Reoperation)
EoE can complicate surgical decision-making because its symptoms and sequelae overlap with common foregut surgical indications. Symptoms of dysphagia, regurgitation, chest pain or pressure, food intolerance, and heartburn may reflect active eosinophilic inflammation, the presence of a fixed stricture, GERD, dysmotility, postsurgical anatomy, or some combination of these. For this reason, the surgeon’s task is not simply to determine whether EoE is present, but to decide whether it is contributing to the patient’s symptoms and whether this should change the management plan, such as optimizing medical therapy or dilation before elective surgery or counseling about persistent postoperative dysphagia (Figure 2).
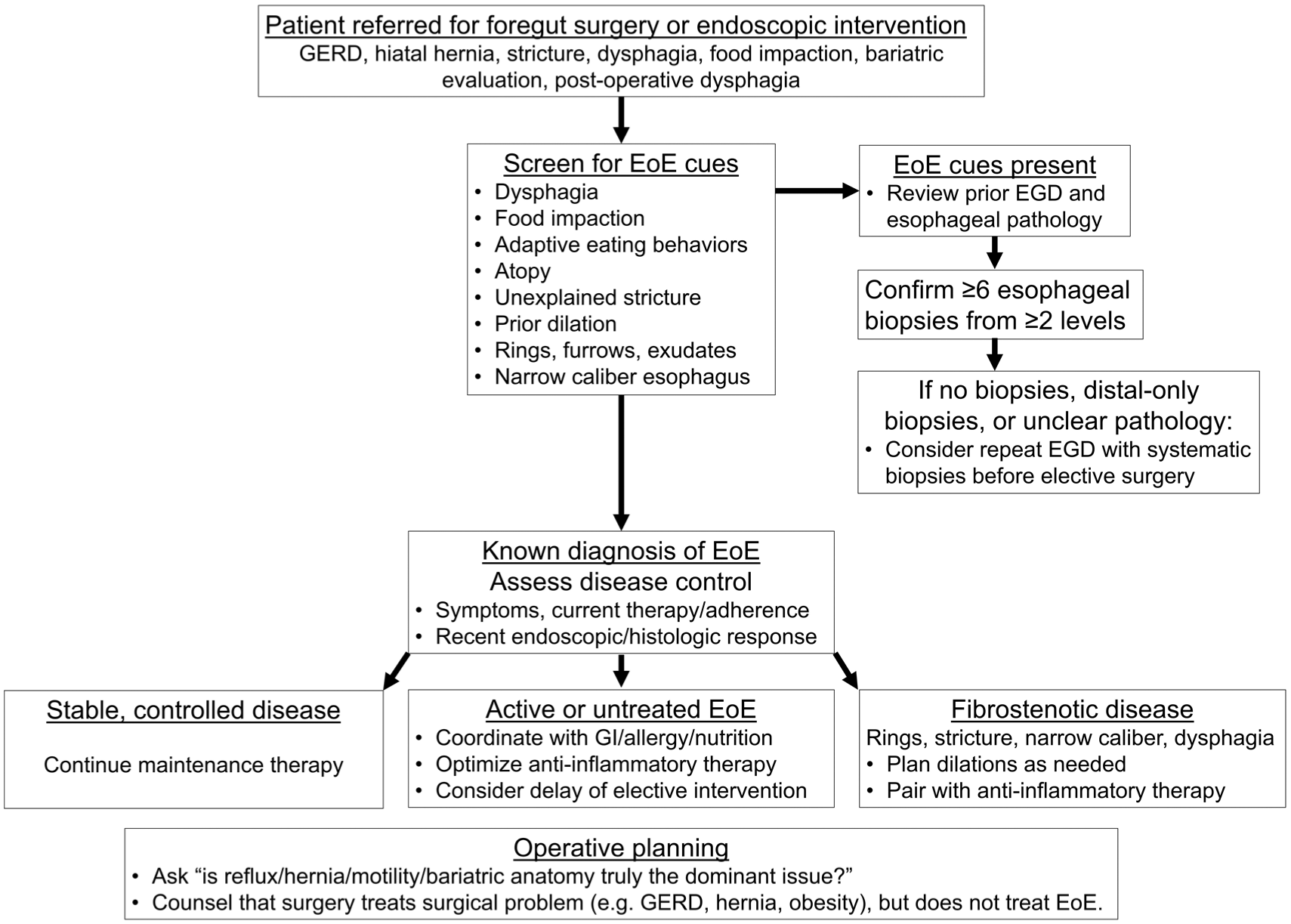
Preoperative EoE screening and planning algorithm for surgeons.
Antireflux Surgery in EoE
Symptoms of GERD and EoE frequently overlap and the 2 conditions can coexist. Heartburn, regurgitation, chest discomfort and pressure, and dysphagia may occur in either condition. Further blurring the lines, reflux can be associated with esophageal eosinophilia, and symptom response to PPI therapy does not exclude EoE. Although GERD can cause low-level eosinophilia in the distal esophagus, it rarely causes significant eosinophilia (≥15 eos/hpf); therefore, esophageal eosinophilia above this threshold and especially present at multiple esophageal levels should prompt evaluation for EoE.
When considering a surgical referral for GERD or hiatal hernia, surgeons should ensure that uncontrolled EoE is not driving symptoms by taking a careful, symptom-directed history that asks about dysphagia to various food textures, adaptive eating behaviors, and food impaction, not just heartburn and regurgitation. When EGD is performed preoperatively, any history of dysphagia, impaction, unexplained stricture, or endoscopic features such as rings, furrows, exudates, mucosal fragility, or narrow caliber should trigger taking esophageal biopsies from multiple levels (eg, ≥6 biopsies from ≥2 levels) and documentation of EREFS features. In addition, current GI society guidelines recommend that evaluation of dysphagia include endoscopy with systematic esophageal biopsies to assess for EoE, even when the mucosa appears endoscopically normal.11,14
For surgical planning, antireflux surgery is best supported by objective evidence of excessive and pathologic reflux – abnormal ambulatory pH or pH-impedance monitoring, or endoscopic findings of erosive esophagitis or Barrett’ esophagus, or symptomatic hernia physiology. 15 Confirmation of excessive acid exposure is even more important when dysphagia is part of the presenting symptom, as symptom report alone may reflect an alternative or coexisting diagnosis of EoE. In cases where there is diagnostic uncertainty (eg, GERD-like symptoms, borderline acid exposure, endoscopic findings consistent with EoE), a second EGD with careful biopsies and initiation of anti-inflammatory therapy may be appropriate before committing to surgery.
When both EoE and GERD are confirmed and surgery is indicated for the reflux component, it is not necessarily required to achieve complete EoE remission before proceeding. The conditions can be managed concurrently—antireflux surgery addresses the mechanical reflux pathology while anti-inflammatory EoE therapy addresses the eosinophilic inflammation. If EoE is active and the operation is elective, optimizing anti-inflammatory therapy and treating strictures with adjunctive dilation may reduce postoperative confusion and persistent dysphagia. Because active EoE can itself cause dysphagia, reduced esophageal compliance, and manometric abnormalities, these findings should be interpreted cautiously, and ideally reassessed after treatment, before they are used to guide wrap selection or counseling. Patients should be counseled that reflux symptoms may improve after surgery, however because fundoplication or hernia repair does not treat EoE-driven inflammation or fibro stenosis, dysphagia and other EoE-related symptoms may persist and EoE maintenance therapy will still be required. These decisions can be made collaboratively with gastroenterology to optimize outcomes for this patient population. Perioperatively, patients on EoE treatments should continue their regimen; there is no established need to hold or delay initiation of EoE therapy in the immediate postoperative period, though specific decisions should be made in partnership with the managing gastroenterologist.
Persistent or recurrent dysphagia after antireflux surgery should not be reflexively labeled a “tight wrap,” particularly when dysphagia predated surgery or there is a history of atopy, food impaction, or adaptive eating behaviors. The differential should include mechanical obstruction, motility disorder, recurrent hernia, and unrecognized or undertreated EoE. Endoscopic evaluation should assess the wrap and luminal diameter, but also include esophageal biopsies when EoE has not been excluded or disease control is uncertain. If EoE is identified as the cause of postoperative dysphagia, GI referral for evaluation and initiation of anti-inflammatory therapy is the appropriate next step, with consideration of dilation if fibro stenotic disease is present. The decision to pursue revision surgery or fundoplication takedown should not be made in the setting of undertreated EoE. Instead, reoperation may be considered when there is objective evidence of a mechanical surgical cause, and EoE inflammation and fibro stenosis have been adequately treated.
Achalasia and Esophageal Motility Testing in the Setting of EoE
EoE can be associated with esophageal dysmotility and a wide range of motility abnormalities — including esophagogastric junction outflow obstruction (EGJOO) or patterns resembling achalasia — not necessarily as a result of primary motility dysfunction, but as a result of esophageal wall stiffness and altered compliance.16,17 The reverse is also true: true achalasia can be associated with secondary esophageal eosinophilia, further complicating interpretation. 18 For surgeons, the practical implication is that equivocal motility findings in a patient with suspected or active EoE should be interpreted cautiously. When manometric findings are uncertain in the setting of possible EoE, the preferred approach is to treat the underlying inflammation first and reassess, rather than proceeding directly to myotomy or pneumatic dilation. If achalasia is clearly established, standard therapies directed at the lower esophageal sphincter (LES) may still be appropriate, but coexisting EoE should be recognized as a potential cause of persistent dysphagia even after the LES is successfully treated.
Bariatric Surgery Considerations
EoE does not, by itself, preclude bariatric surgery or mandate a particular bariatric procedure. Rather, a diagnosis should be considered in the context of other foregut conditions, such as GERD and hiatal hernia, when planning surgery and counseling patients. EoE is not an absolute contraindication to bariatric surgery, but unrecognized disease can complicate both procedure selection and interpretation of post-operative symptoms. As is the case for antireflux surgeries, preoperative evaluation should include a detailed history directed at dysphagia, compensatory or adaptive eating behaviors, food bolus impactions, and if present, EGD with esophageal biopsies should be considered first. This is particularly important as postoperative symptoms of dysphagia, regurgitation, nausea, vomiting, or food intolerance could be attributed to the postsurgical anatomy, dietary noncompliance, esophagitis, or stricture.
Treatments
EoE therapy has 2 overarching goals: (1) to relieve symptoms and prevent impactions, and (2) prevent or slow fibro stenotic remodeling by controlling inflammation. Treatment success is assessed across 3 domains – symptoms, endoscopic appearance (eg, improvement tin EREFS features), and histology with improvement of esophageal eosinophilia <15 eosinophils per high power field. It is important to note that symptoms do not correlate with underlying disease activity and mucosal inflammation. Treatment response in EoE is not reliably assessed by symptoms alone, thus clinical guidelines support repeating endoscopy with esophageal biopsies to confirm endoscopic, histologic, and symptomatic response, generally 6-8 weeks after starting dietary or pharmacologic therapy and 5-6 months after initiating dupilumab.
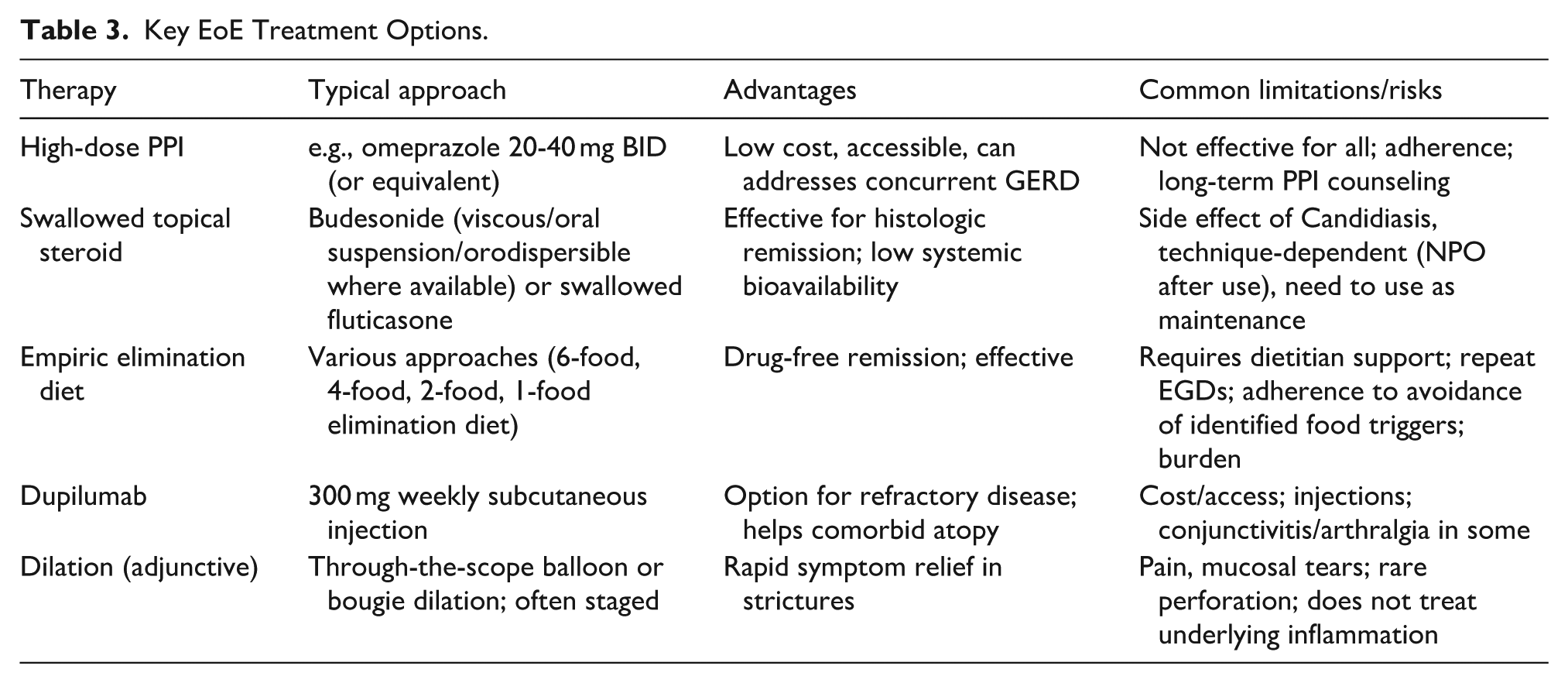
The current foundation of EoE therapy is often summarized as the “3 D’s”: drugs (medications), diet (diet elimination), and dilation. Table 3 provides a concise reference.
Key EoE Treatment Options.
Medical Therapies
Three pharmacologic treatment strategies are used in EoE, each targeting the underlying Th2-mediated inflammation – proton pump inhibitors (PPI), topical corticosteroids, and biologics. PPIs (eg, omeprazole 20-40 mg twice daily or equivalent) are often used early given their ease of use and benefit for coexisting GERD. However, only 30% to 50% of patients achieve histologic remission on PPI therapy alone and are deemed “PPI responsive”. 19 Swallowed topical corticosteroids such as swallowed budesonide or fluticasone are highly effective at inducing and maintaining histologic disease remission in up to 70%.20,21 However, a practical tradeoff is the need to avoid eating or drinking for 30 to 60 minutes after medication use to maximize esophageal dwell time. Although approved options exist (eg, budesonide oral suspension in the United States, budesonide orodispersible tablet in Europe), insurance coverage and cost often necessitate off-label use of repurposed asthma preparations such as swallowed fluticasone from a metered dose inhaler or diskus, mixing budesonide respules into viscous slurry, or compounded formulations of either. 22 With these various options, response rates to PPIs and topical steroids may be dose and regimen-dependent. For example, twice daily PPI dosing has been associated with higher histologic remission compared to once daily dosing, and the efficacy of topical steroids may vary with dose, formulation, and esophageal dwell time. 23 For patients with refractory or severe disease, dupilumab (an IL-4/IL-13 receptor antagonist) is FDA-approved, used as a once-weekly subcutaneous injection, and can be particularly useful in those with concurrent atopic comorbidities for which dupilumab is also approved (eg, moderate to severe atopic dermatitis, asthma, chronic rhinosinusitis with nasal polyposis).24,25
Dietary Therapies
Dietary elimination therapy is a non-pharmacologic, anti-inflammatory treatment option for EoE that can be highly effective in appropriately selected and supported patients. The rationale is that for many patients, food antigens drive Th2-mediated esophageal inflammation, so identifying and removing specific food triggers can lead to symptomatic, endoscopic, and histologic remission, often times without using a medication. 26 The favored dietary approach is an empiric elimination diet, in which the most common trigger foods – dairy/animal milk, wheat, soy, eggs – are removed for a set time, followed by endoscopy to demonstrate disease remission. 27 This is then followed by stepwise food reintroduction with subsequent endoscopies to identify individual triggers. Empiric elimination diets can also be highly effective, inducing histologic remission in up to 60%, with response rates generally increasing as more food groups are eliminated (eg, ~50% with 1-food elimination and ~60% with 6-food elimination in many adult series). 28 For many patients, dietary therapy is appealing because it offers the possibility of medication-free remission and can identify specific food triggers that drive disease activity. The tradeoff is the burden of elimination and reintroduction, and once a trigger is identified, ongoing avoidance is generally required to maintain remission—analogous to continued adherence to an effective medication.
For surgeons, the practical considerations are that diet therapy can be resource- and time-intensive. Partnering with a dietitian or nutrition specialist is crucial to the successful implementation of the diet, long-term adherence, and patient quality of life. Using symptoms alone are unreliable to determine food triggers, so repeat EGD with biopsies to confirm initial response to elimination and during food reintroduction phases is key. Allergy-test–directed diets have variable performance and are not a substitute for structured empiric elimination. 8 At some centers, less-invasive monitoring approaches, such as esophageal sponge, esophageal string test, and unsedated trans nasal endoscopy, are being used to assess EoE disease activity, including during dietary therapy, although the availability, protocols, and validation of these vary.29-31
Endoscopic Dilation
Dilation is a safe and effective way to manage symptomatic fibrostenotic EoE: focal or ring strictures, a narrow-caliber esophagus, or persistent dysphagia despite improvement in mucosal inflammation on therapy. 32 Symptoms do not always correlate with underlying disease activity and at times, histologic remission (histology of <15 eos/hpf) does not always translate to symptomatic relief when there is fibrosis present. In such patients, endoscopic dilation can be offered as an adjunct to anti-inflammatory medications or diet therapy to disrupt the fibrotic sequelae. Because subtle strictures may be missed on visual inspection, dilation is a reasonable next step in patients with persistent dysphagia despite endoscopic and histologic improvement, and the presence of a mucosal disruption or dilation effect may reveal an underlying narrowing that was not appreciated. Conversely, dilation should not be used as a substitute for anti-inflammatory treatment because although it addresses the fibrotic consequence of EoE, it does not treat the underlying inflammatory process that drives remodeling. Instead, histologic response to an effective pharmacologic or dietary therapy is associated with substantially fewer dilations, supporting the need for inflammation control with dilation, rather than dilation alone. 33 Although not required in the management of EoE, barium esophagram can be a useful adjunct when the anatomy is unclear, estimating the length and luminal diameter of the esophagus to help plan the dilation approach. Approaches to dilation in EoE are reviewed in “Assessment, treatment, and prevention of complications in EoE” and summarized in Table 4.
Dilation Pearls in EoE Strictures.
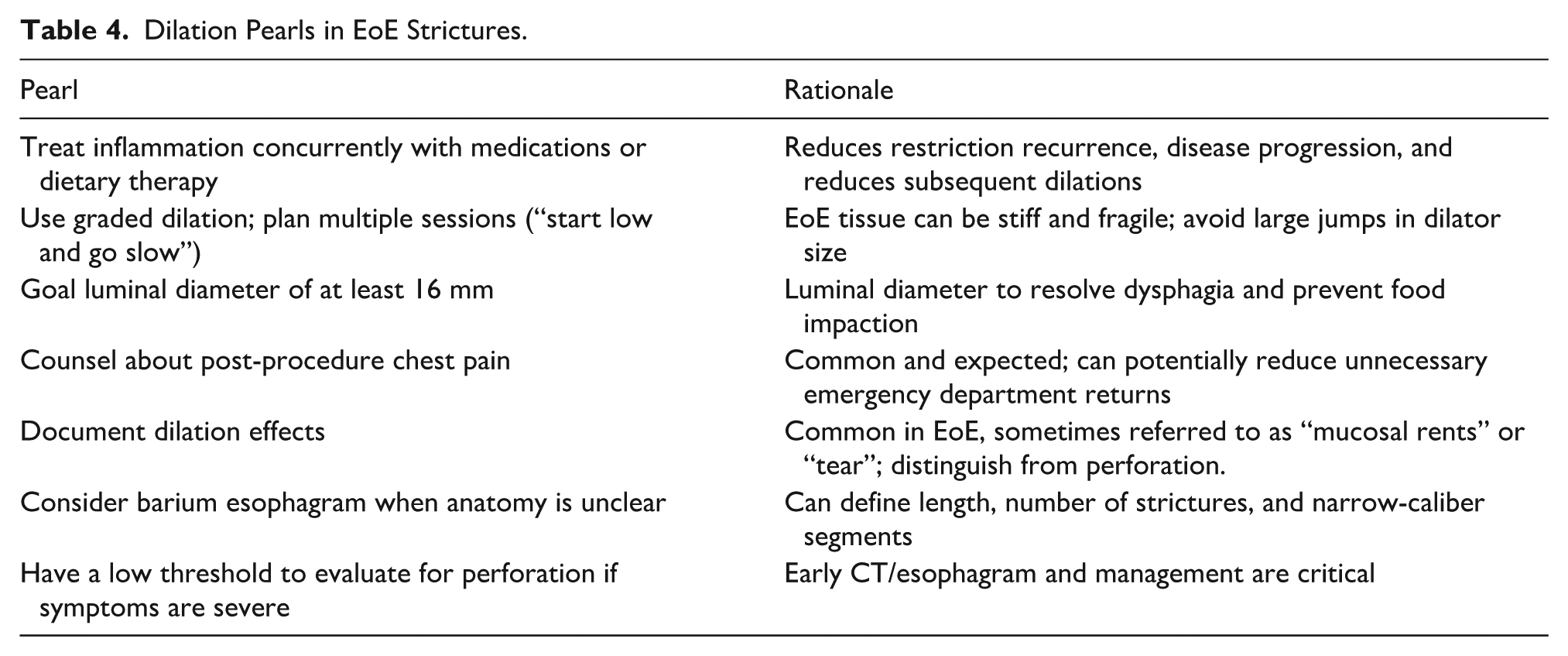
Post-dilation chest pain and odynophagia can be common in patients with EoE. Pre-procedure counseling can reduce anxiety and improve post-procedure decision-making, while still reinforcing the need to seek urgent evaluation for concerning features (eg, escalating pain, fever, dyspnea, persistent tachycardia, or inability to tolerate liquids) that may suggest a complication. One technical point worth emphasizing is that dilation in highly active EoE can be associated with more post-procedure pain than when dilation is performed after inflammation is at least partially controlled. When feasible, consider deferring dilation until some treatment response is achieved. However, in the situation that dilation cannot wait (eg, severe stricture or nutritional compromise), proceed conservatively with graded dilation and plans to repeat once inflammation is better controlled.
A more nuanced issue is the finding of pneumomediastinum on CT after dilation. Small amounts of mediastinal air can be common after esophageal dilation in EoE—particularly given the expected and desired dilation effects—and in a clinically stable patient without fever, escalating pain, or hemodynamic compromise, a contained finding does not necessarily mandate operative intervention. Management should be guided by the clinical picture: a patient who is comfortable, tolerating liquids, and afebrile can often be managed conservatively with close observation, even if CT shows a small amount of extraluminal air. Conversely, any concern for free perforation, mediastinitis, or clinical deterioration should prompt standard perforation pathways (broad-spectrum antibiotics, NPO, cross-sectional imaging with oral contrast, and surgical consultation).
In summary, EoE is a chronic, progressive inflammatory disease that is quickly moving beyond gastroenterology and allergy practices. Surgeons are increasingly on the front lines of its recognition and management, and several practical take-home points are worth noting. First, EoE should be considered in any patient presenting with dysphagia or food impaction, particularly young and middle-aged patients, those with a history of atopic disease, or those whose history reveals long-standing adaptive eating behaviors. Second, a normal-appearing esophagus does not exclude the diagnosis — biopsies should be obtained routinely, targeting at least 6 samples from 2 or more esophageal levels. Third, dilation is an effective tool to manage fibrosis in EoE and improves symptoms, but does not treat the underlying inflammatory disease; dilation is best paired with anti-inflammatory therapy. Fourth, antireflux surgery addresses reflux — not EoE. The 2 conditions must be distinguished preoperatively when dysphagia is present, and EoE should remain on the differential in any patient with dysphagia that persists or recurs following fundoplication. Finally, as EoE is a chronic disease, durable outcomes in EoE require long-term maintenance therapy for sustained disease control and the prevention of fibro stenotic progression.
Footnotes
Abbreviations
EoE, eosinophilic esophagitis; GERD, gastroesophageal reflux disease; EGD, esophagogastroduodenoscopy; LES, lower esophageal sphincter; PPI, proton pump inhibitor.
Ethical Considerations
Ethical approval is not required for this manuscript.
Author Contributions
JWC was responsible for the conception and design of the review, literature review and interpretation, manuscript drafting, critical revision, and final approval of the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JWC is supported by funding in part by NIH award K23DK129784.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Chang reports consulting fees from Sanofi-Regeneron, Takeda, Bristol Myers Squibb, Amgen AstraZeneca.
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.