
Abstract
Ehlers-Danlos syndrome (EDS) is a heritable collagen disorder characterized by joint hypermobility and tissue fragility, with hypermobile Ehlers-Danlos syndrome (hEDS) as the most common subtype. Rates of gastroesophageal reflux disease (GERD) symptoms are reportedly higher in the hEDS population than the general population. This could be caused by increased esophageal hypersensitivity and/or connective tissue laxity leading to hiatal hernias or increased relaxations of the lower esophageal sphincter. Despite this, Barrett’s esophagus rates in hEDS do not appear to be higher than in the general population. This review examines the epidemiology, pathophysiology, and unique considerations for management of GERD in hEDS.
Keywords
Key Learning Points
Gastroesophageal reflux disease (GERD) has been reported more frequently in hypermobile Ehlers-Danlos syndrome (hEDS) than in the general population.
Proposed mechanisms for increased prevalence of GERD in hEDS include connective tissue laxity weakening the antireflux barrier, visceral hypersensitivity, and autonomic nervous system dysfunction.
There does not appear to be an increased risk for Barrett’s esophagus in patients with hEDS.
Introduction
Ehlers-Danlos syndrome (EDS) is a heritable connective tissue disorder with 13 different subtypes, of which the most common is hypermobile Ehlers-Danlos syndrome (hEDS). 1 EDS is characterized by hypermobile joints, hyperextensible skin, and fragile tissue due to defects in collagen from genetic mutations. While studies to identify the causative genetic mutations in hEDS are ongoing and promising, a common underlying mutation has not been identified, resulting in more specific clinical criteria for hEDS in 2017.1,2 Patients with non-inflammatory joint hypermobility who do not meet criteria for hEDS or other hereditary connective tissue disorders are categorized as having hypermobility spectrum disorder (HSD). 3 Gastrointestinal (GI) manifestations are increasingly recognized in all these connective tissue disorders, with symptoms of gastroesophageal reflux disease (GERD) described at rates exceeding those in the general population. Chronic GERD is a risk factor for Barrett’s esophagus, a premalignant condition and precursor to esophageal adenocarcinoma. 4 This review examines the epidemiology, pathophysiology, and management of GERD in patients with hEDS/HSD, highlighting the unique considerations required for these populations and identifying areas requiring further investigation.
Epidemiology of hEDS/HSD and GERD
EDS has been reported in 1:5000 people, with hEDS representing about 80% to 90% of cases. 5 In 2016 in Wales, EDS and joint hypermobility syndrome (JHS) were identified in 1:500 people, predominantly in females (70%). 6 Gastrointestinal symptoms and pathologies have been reported at higher rates in patients with EDS. From the 2016 United States National Inpatient Sample, EDS patients had significantly more GI conditions compared to controls (44% vs 18%, OR = 3.57, 95% CI: 3.17, 4.02), of which irritable bowel syndrome, gastroparesis and celiac disease were strongly associated. 7 EDS patients were also more likely to have longer hospitalizations and rates of autonomic dysfunction such as postural orthostatic hypotension syndrome (POTS). 7 In a United Kingdom survey of over 600 individuals with hEDS/HDS, 98% patients met diagnostic criteria for disorders of gut brain interaction (DGBI) compared to 47% in the control group (P < .001). 8
While DGBI in hEDS/HSD have been increasingly well outlined, including in 2025 American Gastroenterological Association Clinical Practice Guidelines, there is limited data on objective GERD as defined by the Lyon 2.0 Consensus Criteria in these patients.8,9 GERD affected about 10% of patients worldwide in 2021, 10 whereas rates of GERD symptoms and diagnoses as high as 30% to 70% have been described in studies where the 2017 hEDS diagnostic criteria has been used (Table 1). Typical GERD symptoms include heartburn, regurgitation and chest pain. 11 For this review, keywords “GERD”, “heartburn”, “hypermobile Ehlers-Danlos syndrome” and “joint hypermobility” were used to search PubMed and Google Scholar (2017 – May 2026). OpenEvidence was used to identify any additional relevant studies which used the 2017 hEDS diagnostic criteria to some degree to identify patients. After retrieving all full texts, five articles were highlighted in Table 1 of this review.
Studies Reporting GERD Diagnoses and Symptoms and Barrett’s Esophagus in hEDS/HSD Using the 2017 hEDS Diagnostic Criteria.
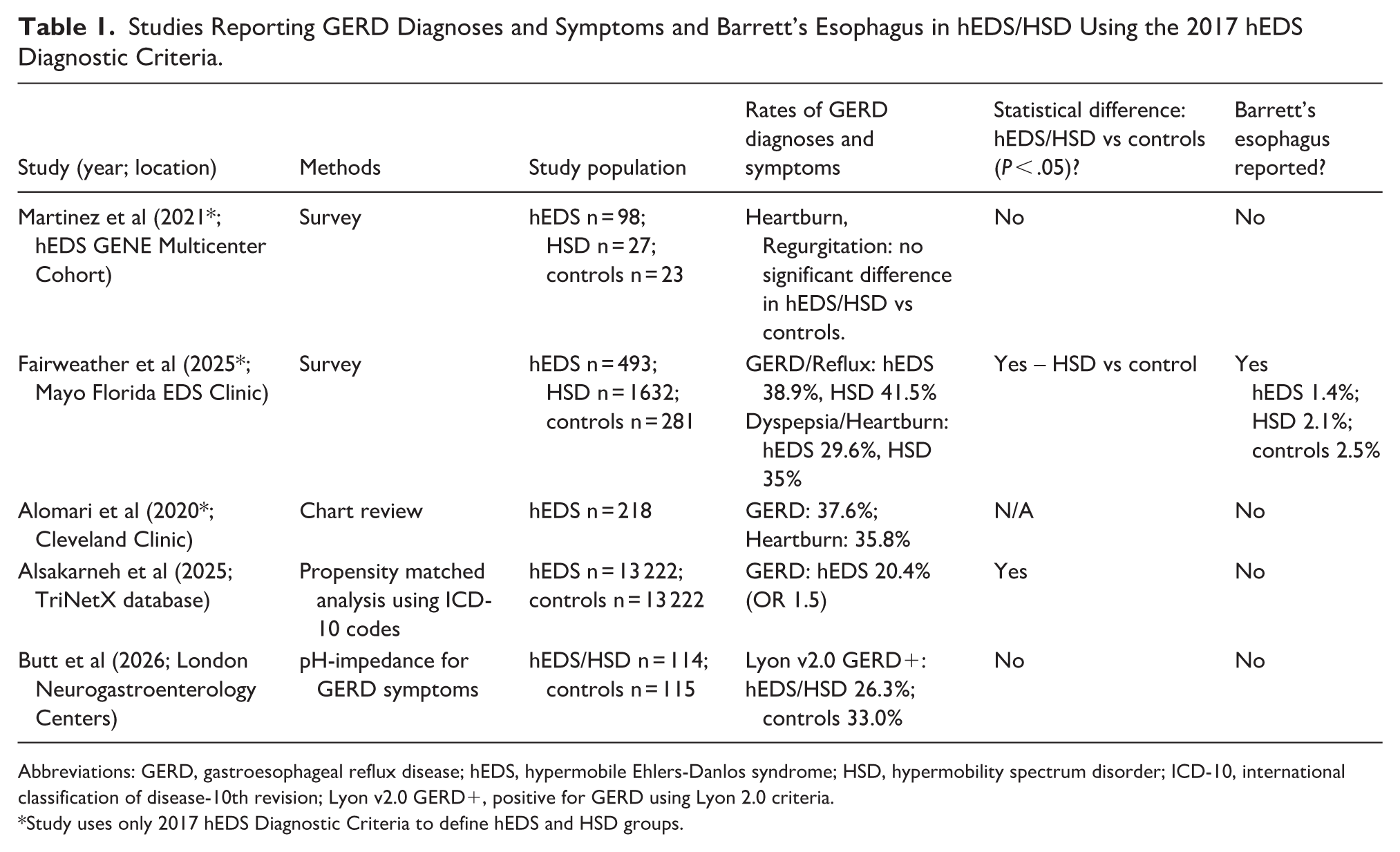
Abbreviations: GERD, gastroesophageal reflux disease; hEDS, hypermobile Ehlers-Danlos syndrome; HSD, hypermobility spectrum disorder; ICD-10, international classification of disease-10th revision; Lyon v2.0 GERD+, positive for GERD using Lyon 2.0 criteria.
Study uses only 2017 hEDS Diagnostic Criteria to define hEDS and HSD groups.
Two studies exclusively used the 2017 hEDS diagnostic criteria and evaluated for GERD via symptom questionnaires. The hEDS GENE study was a multicenter, cohort study in which patients completed a Gastro-Questionnaire symptom survey including typical and atypical GERD symptoms. The reported rates of heartburn and regurgitation were no different when comparing the hEDS/HSD group to the control group. However, there was a significantly greater number of patients with hEDS and HSD who reported difficulty swallowing (P = .002) and chest pain (P < .0001). 12 In addition, a study from the Mayo Clinic Florida EDS Clinic included 2695 patients who completed an intake questionnaire. They identified 1632 patients with HSD (60%) HSD and 493 patients with hEDS (18.3%). Patients self-reported reflux and heartburn symptoms, as well as a history of Barrett’s esophagus. Reflux was reported in 38.9% patients and heartburn reported in 29.6% patients with hEDS, neither of which were significantly different from controls. Patients with HSD had significantly more symptoms of reflux (41%) and heartburn (35%) than controls (P < .05). Notably, Fairweather et al 13 published the only manuscript to date that assessed Barrett’s esophagus among patients with hEDS (n = 7, 1.4%) and HSD (n = 34, 2.1%), demonstrating no significant difference compared with controls (n = 7, 2.5%; P = .69).
In a study reviewing patients evaluated at the Cleveland Clinic Center for Personalized Genetic Healthcare from 2007 to 2017, 218 patients with hEDS were identified who had been evaluated previously by a geneticist and rheumatologist. The 2017 hEDS diagnostic criteria were applied for inclusion in the study and chart review was performed for symptoms, medical history, and prior motility testing. Of these patients, 82 patients (37.6%) had a history of gastroesophageal reflux disease. Of the symptoms reported, the most common was abdominal pain (49.8%), followed by heartburn (35.8%), irritable bowel syndrome (21.6%), belching/bloating (27.1%), and dysphagia (14.2%). 14 GI motility testing in these patients revealed that 11.9% had esophageal dysmotility, 42.8% had gastroparesis and 9.5% had global dysmotility. After multivariable analysis, only POTS (OR: 5.74, 95% CI: 2.25-16.7, P = .0005) was significantly associated with an increased likelihood of gut dysmotility. 14
The largest published study to date evaluating GI conditions in hEDS performed propensity-matched analysis of 13 222 patients with hEDS from 2005 to 2023 in the TriNetX database using International Classification of Disease (ICD), 9th and 10th Revision codes. Of note, this study did include patients diagnosed with hEDS using both the pre-2017 and post-2017 diagnostic criteria. GERD was one of the most common gastrointestinal disorders in hEDS patients, affecting 20.4% of patients and significantly more patients compared to matched controls (OR 1.52; 95% CI: 1.43-1.62, P < .001). 15 Furthermore, hiatal hernia (OR 2.09; 95% CI: 1.74-2.51, P < .001) and gastroparesis (OR: 8.40; 95% CI: 6.78-10.42, P < .001) were identified more frequently in hEDS compared to matched controls. Additionally, psychiatric conditions including depression (OR 1.29; 95% CI: 1.21-1.37, P < .001) and anxiety (OR 2.03; 95% CI: 1.92-2.15, P < .001) as well as eating disorders (OR 1.98; 95% CI: 1.62-2.42, P < .001) and chronic pain syndrome (OR 9.3; 95% CI: 8.02-10.8, P < .001) were diagnosed more frequently in hEDS. 15
There is limited data analyzing the prevalence of GERD in hEDS using objective criteria for GERD rather than self-reported symptoms or diagnosis codes. While empiric treatment of typical GERD symptoms with proton pump inhibitors (PPI) is part of the GERD management guidelines, a 10% to 15% placebo effect can confound the diagnosis. 16 As such, the Lyon 2.0 consensus notes that ‘response to an empiric PPI trial alone is insufficient for a conclusive GERD diagnosis’. 11 Objective criteria for GERD based on the Lyon 2.0 criteria include endoscopic evidence of Los Angeles Grade B, C or D esophagitis, peptic stricture, biopsy-proven Barrett’s esophagus, or positive ambulatory pH testing. 11
One study has evaluated pH studies and high resolution manometry studies in patients with reflux symptoms or dysphagia who were seen at two London neurogastroenterology clinics. Of note, patients were included in the hEDS/HSD group if they had a joint hypermobility diagnosis using both pre- and post-2017 criteria (hEDS, HSD, JHS, EDS Type III, or EDS-Hypermobility Type). They found that the proportion of patients diagnosed with Lyon 2.0 GERD was not significantly different between persons with hEDS/HSD (26.3%) versus patient controls (33.0%) (P = .3). 17 Neither the total acid exposure time nor the total number of reflux events differed significantly between groups. Despite this, there no difference in the rates of functional heartburn (62% vs 52%) and reflux sensitivity (32% vs 28%) diagnosed in hEDS/HSD versus controls. 17 Furthermore, the high resolution manometry results revealed higher rates of normal esophageal motility seen in hEDS/HSD group compared to controls (61% vs 46%, P = .005). 17
Additional studies published using exclusively the pre-2017 nomenclature of EDS-hypermobile type and joint hypermobility syndrome also reported pH impedance data or endoscopic findings. Fikree et al 18 published a study of 30 patients with JHS and regurgitation, reflux or dysphagia; 53% of symptomatic patients had pathological acid reflux on pH-impedance monitoring. Otherwise, 21% of patients had reflux hypersensitivity, and 25% had functional heartburn. Acid exposure was more commonly increased in the recumbent than upright position (64% vs 43%) and a hiatal hernia was noted in 33% of patients. Of the 18 patients with JHS and POTS, those with POTS had worse reflux scores (24.5 vs 16.5, P = .05) though no significant difference in pathologic reflux (64% vs 36%, P = .1). 18 Motility testing was also performed in the JHS patients. In patients with dysphagia, 60% had normal esophageal motility, 32% had ineffective esophageal motility and 8% had fragmented contractions. 18 Impaired esophageal motility can worsen esophageal clearance and prolong the mucosal exposure to refluxed acidic contents. 19
Furthermore, a 20-year retrospective cohort study of 471 patients with EDS-hypermobile subtype from Mayo Clinic (1993-2013) demonstrated that 57% patients reported GI symptoms, including abdominal pain (56%), nausea (44%), constipation (42%), and heartburn (38%). 20 Among the 143 patients who underwent an esophagogastroduodenoscopy (EGD), three had Barrett’s esophagus, two had a distal esophageal stricture, and 12 had reflux esophagitis, predominantly LA Grade A. Hiatal hernia was seen during EGD in 11 patients and frequently seen during barium contrast upper GI series. 20
Pathophysiology of GERD Symptoms in hEDS/HSD
The pathophysiology of GERD in hEDS and HSD is likely multifactorial, involving structural, neurologic, and systemic mechanisms that distinguish it from GERD in the general population (Figure 1). Underlying genetic causes of hEDS are also under investigation, which could also connect the multisystemic nature of hEDS and its associated pathologies. 2
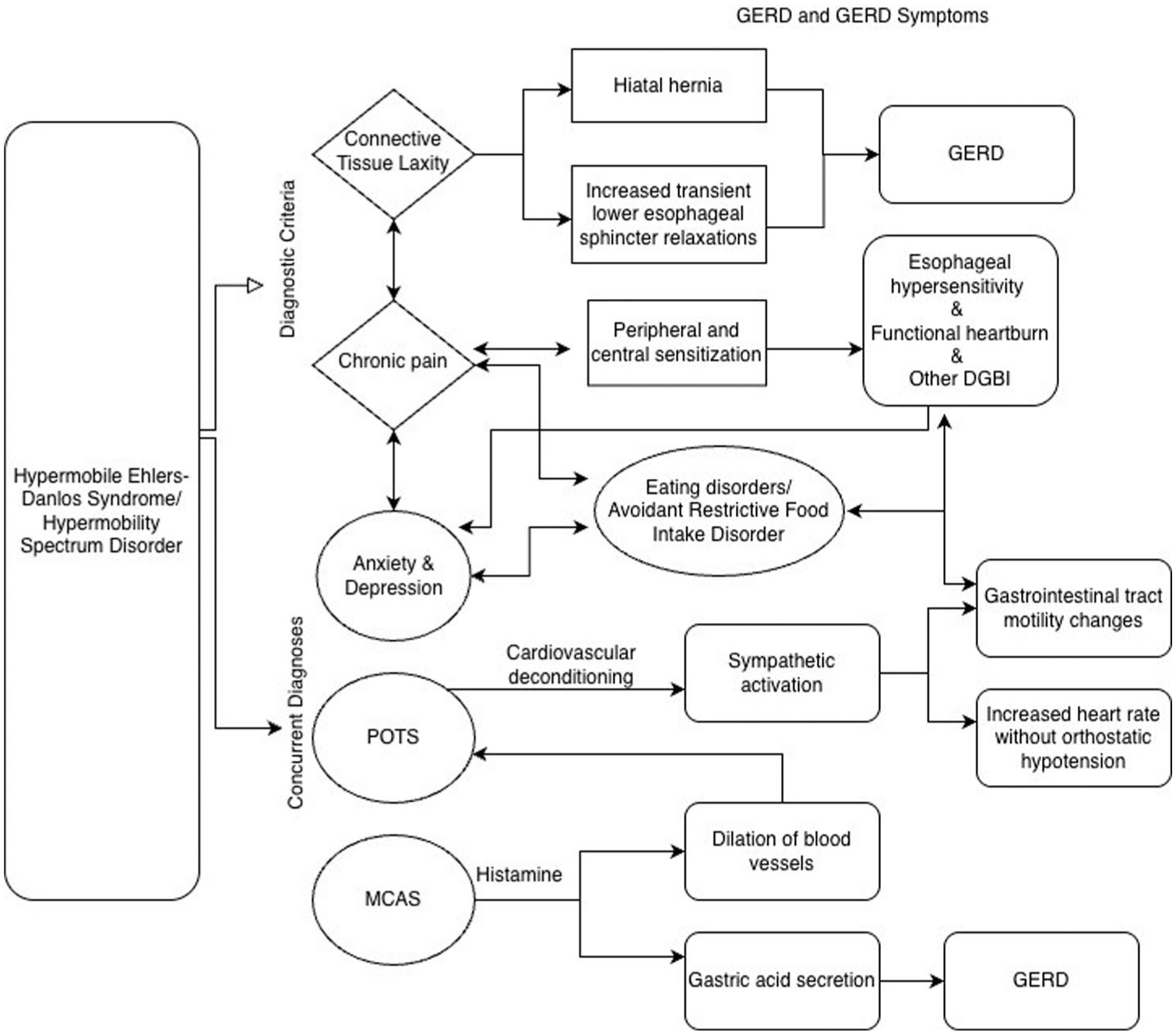
Proposed mechanism of gastroesophageal reflux disease and gastrointestinal symptoms in hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorder.
Structural: Connective Tissue Abnormalities
The fundamental issue in EDS is defective collagen production resulting in altered connective tissue structure and function. The gastroesophageal junction anti-reflux barrier depends on the lower esophageal sphincter (LES), diaphragmatic crura, and angle of His. 21 In hypermobility, connective tissue laxity could reduce the integrity of the phrenoesophageal ligament and lower esophageal sphincter, potentially leading to development of hiatal hernia or increased transient lower esophageal sphincter relaxations. 22 Hiatal hernias were present in hEDS patients twice as frequently as in matched controls (2.7% vs 1.3%, P < .001) from the Alsakarneh et al 15 TriNetX database study.
Neurologic: Functional and Motility
Reflux hypersensitivity and functional heartburn are common diagnoses in the hEDS/HSD population when pH impedance testing is performed.17,18 Visceral hypersensitivity, and therefore esophageal hypersensitivity, can be promoted by the presence of chronic widespread pain due to central sensitization. 23 Chronic pain is a key feature of hEDS/HSD, with 92% to 98% of patients reporting the presence of chronic pain in a global survey. 24 Chronic pain for longer than 3 months that is widespread, musculoskeletal, or limited to the joints is also part of the 2017 diagnostic criteria for hEDS. 1 Chronic pain, DGBI, mood disorders such as depression and anxiety, and eating disorders can be interrelated and more frequently identified in hEDS compared to controls.15,25,26 Eating disorders can exacerbate GI symptoms as gastrointestinal motility slows and the gastrocolic reflex is not stimulated. 27 Collaboration with psychiatry and nutrition for specialized treatment of these conditions is extremely important in this patient population.
A common GI motility pathology seen more frequently in patients with hEDS, especially in those with concurrent POTS, is gastroparesis.12,15 Gastric distension can also trigger a vasovagal reflex resulting in TLESR and thereby contribute to GERD. 28 While proximal stomach distension and retention of food in the fundus could cause increased transient lower esophageal sphincter relaxations, studies have not shown that gastroparesis is connected to increased acid exposure time. 29 In a study of 30 patients with typical GERD symptoms, a 24-hour pH impedance study to test for GERD and a 13C–octanoic acid breath test to understand gastric emptying were both performed. Among 13 patients with delayed gastric emptying, there were higher rates of weakly acidic/non-acid reflux, greater proximal extent of reflux events, and increased bolus clearance time compared to patients with normal gastric emptying. 29 This suggests that gastroparesis has an impact on volume regurgitation although retained gastric contents may be neutralizing the acid measurements on pH impedance testing.
Lastly, ineffective or absent esophageal motility can worsen esophageal clearance and prolong the mucosal exposure to refluxed acidic contents. 19 Butt et al 17 and Fikree et al 18 published results showing predominantly normal esophageal motility in patients with joint hypermobility, though approximately 40% of patients had minor disorders of esophageal motility in both studies. Inquiry about dysphagia symptoms and consideration of esophageal motility testing should be part of the algorithm for GERD workup in patients with hEDS, especially in patients who are not responding as expected to GERD treatments, to understand if there is an additional contributor to esophageal symptoms.
Systemic Contributors: Autonomic Dysfunction and Mast Cells
Dysautonomia and hEDS/HSD have been identified concurrently in a sizable percentage of patients. Studies report that 60% to 80% of patients with hEDS/HSD have a disorder of orthostatic intolerance. 30 Postural orthostatic tachycardia syndrome is characterized by an excessive increase in heart rate of more than 30 beats per minute without associated hypotension, within 10 minutes of standing. 30 In a cohort of POTS patients, 31% (28/91) met clinical criteria for the 2017 criteria of hEDS. 31 Fikree et al 18 showed that patients with concurrent hEDS and POTS had significantly higher rates of reflux symptoms and double the amount of pathologic reflux on pH testing, though it was not statistically significant. The vagus nerve and myenteric plexus help relax the lower esophageal sphincter via the parasympathetic nervous system, and the splanchnic nerves and celiac ganglion predominantly contract the lower esophageal sphincter via the sympathetic nervous system. 28 In concert with the enteric nervous system, they play key roles in regulating lower esophageal sphincter tone, transient lower esophageal sphincter relaxations (TLESR), esophageal peristalsis and gastric emptying. 32 The Journal of American College of Cardiology published a focus seminar on POTS with a proposed pathophysiologic cycle termed the “downward spiral,” whereby an inciting event leads to orthostatic and exercise intolerance, increased bedrest and cardiovascular deconditioning, and ultimately results in more constant sympathetic activation when the patient is upright. 33 Gut motility issues, typically slowing of the GI tract, can result from more frequent sympathetic nervous stimulation. 33
Overall, impaired functioning of the autonomic nervous system could reasonably contribute to higher rates of GERD, though the exact mechanisms in hEDS and POTS have yet to be discovered.
Mast cell activation syndrome (MCAS) represents another important comorbidity in the hEDS population. MCAS is characterized by mast cell degranulation and release of histamine, heparin and other cytokines causing multisystemic symptoms commonly involving the GI tract, skin, respiratory tract, and cardiovascular system. 9 In particular, histamine stimulates gastric acid secretion and vasodilation. In a study of 30 patients with MCAS, diagnosed by symptoms as well as elevated serum tryptase or urinary prostaglandin D2 and N-methylhistamine, 13 patients (43%) had hEDS/HSDD and six patients (20%) had the triad of MCAS, POTS, and hEDS or HSD. 34 When treated with MCAS therapies, 60% reported GI symptom improvement (nausea, vomiting, cramps, loose stools or diarrhea). 34 Mast cells may induce inflammation, barrier dysfunction, and visceral hypersensitivity contributing to DGBI. 9 Mast cells can influence GERD via histamine causing esophageal shortening, as shown in possum models. In an acid-exposed possum esophagus, pre-treatment with mast-cell stabilizers (doxantrazole or disodium cromoglycate) prevented esophageal shortening. 35 These theoretical mechanistic links between hEDS, POTS, and MCAS require further investigation to elucidate the underlying pathophysiology. It is important to note, that medications frequently used to treat POTS and MCAS, such as fludrocortisone, midodrine or antihistamines, can cause nausea, diarrhea, and constipation as common side effects. 36 Careful consideration of the medical treatment side effect profile and multidisciplinary care is key in managing these patients with various systemic symptoms.
Identifying a Genetic Cause
There have been research efforts to identify underlying genetic causes of hypermobile EDS. The Norris lab identified the kallikrein-15 (KLK15) gene as a common gene variant in two families after performing whole genome sequencing in 200 patients with hEDS. 2 In KLK15 knock-in mouse models, the mice had features of hEDS such as increased Achilles tendon elasticity, increased rates of mitral valve prolapse, and dysregulated cytokine profiles. The kallikrein gene is known to regulate proteolytic cascades controlling extracellular matrix remodeling, inflammation, connective tissue integrity, inflammation, vascular tone and autonomic regulation. While multiple genes rather than one is likely to explain most cases of hEDS, the KLK gene provides an additional possible pathophysiologic mechanism behind some of the multisystemic issues seen with hEDS, POTS and MCAS and could reframe hEDS as a condition beyond just a structural collagenopathy. 2
Barrett’s Esophagus
Barrett’s esophagus (BE) develops when metaplastic columnar mucosa replaces squamous epithelium in the distal esophagus due to chronic inflammation from GERD. BE is a premalignant condition with the potential to evolve into esophageal adenocarcinoma. BE prevalence is reported at 0.5% to 2% in the general population and 5% to 15% of patients with chronic GERD. 4 It has frequently been described in older, male patients with a history of smoking and obesity. This differs from the typical EDS phenotype. Fairweather et al 13 reported that Barrett’s esophagus rates were similar among patients with hEDS (n = 7, 1.4%) and HSD (n = 34, 2.1%) when compared to controls (n = 7, 2.5%; P = .69). Furthermore, the authors of this review presented preliminary data in an abstract reporting rates of GERD and Barrett’s esophagus in hEDS patients. 37 Using the TriNetX database and ICD-10 codes from 2005 to 2025, 25 716 patients with hEDS (mean age 35±13 years, 90% female) were identified. GERD was present in 35% of hEDS patients, which significantly increased when patients had a concurrent diagnosis of MCAS and/or POTS. Barrett’s was present in 0.8% of hEDS patients, with no significant difference when patients had a concurrent diagnosis of MCAS and/or POTS. 37 Most hEDS cohorts are young and predominantly female, which may reduce the baseline BE risk compared to a classic high-risk population. While limited, the existing data suggests there is no increased incidence of BE in hEDS/HSD, though additional studies are needed to confirm these findings.
Procedural and Surgical Considerations
Diagnosis and management of GERD rely upon the ability to perform procedures such as EGD, pH testing, esophageal manometry and if required and/or desired by the patient, surgical procedures such as fundoplication. While rates of endoscopy-related perforation were increased in patients with vascular EDS (9%), patients with classical and hypermobility-type EDS had perforation rates (0.6%) comparable to standard rates in endoscopy. 38 No studies to date have been published on surgical outcomes of fundoplication in patients with hEDS/HSD. However, given the high rates of DGBI in this population, a comprehensive work-up, including barium esophagram, endoscopy, esophageal manometry, and pH monitoring, should be mandatory prior to consideration of a surgical fundoplication. 39 When extrapolating conclusions from studies in other connective tissue diseases, laparoscopic fundoplication is safe with regards to mortality. 39 To decrease the risk of post-operative dysphagia, the degree of the wrap should be tailored based on the robustness of esophageal motility on high resolution manometry. 39 While no data on fundoplication failure rates has been published to date in the hEDS/HSD population, there is concern that increased tissue laxity could theoretically be at greater risk of operative failure or decreased longevity of a fundoplication in this population.40,41
Conclusions
Multiple observational studies and cohort series report high rates of reflux symptoms in hEDS/HSD. However, the proportion attributable to objectively proven gastroesophageal reflux disease (GERD) versus motility abnormalities, reflux hypersensitivity or functional heartburn remains uncertain. In these patients, ongoing symptoms despite PPI therapy are not necessarily evidence of uncontrolled acid reflux and may require neuromodulators, behavioral therapy, or other DGBI-directed interventions rather than more acid suppression or surgery. As such, evaluation for objective GERD as per the Lyon 2.0 consensus criteria is important in this population. Because of the interconnectedness of the GI tract and upstream effects of impaired GI motility, gastroenterologists caring for patients with hEDS should inquire about symptoms such as dysphagia, chest pain, nausea, early satiety, constipation and incomplete evacuation. Based on the related symptoms reported by the patient and overall high rates of GI dysmotility in hEDS patients, GI motility testing including esophageal motility testing, gastric emptying studies, colonic transit studies, and anorectal manometry should be considered in the algorithm for GERD, who are not responding as expected to antireflux medications. Distinguishing between functional and objective GI pathologies in hEDS/HSD is important given the high rates of DGBI, and is important to understand the true risk of GERD and Barrett’s esophagus in this population.
There are several possible mechanisms for GERD and GERD symptoms in patients with hEDS and HSD, and the pathophysiology is likely multifactorial. In hEDS, defects in collagen could lead to connective tissue laxity resulting in weakening of the gastroesophageal junction anti-reflux barrier. Chronic pain leading to visceral hypersensitivity could also contribute to increased rates of heartburn, chest pain, and regurgitation in the hEDS/HSD population. Chronic pain, disorders of gut brain interaction, mood disorders such as depression and anxiety, and eating disorders can be interrelated and more frequently identified in hEDS compared to controls. Eating disorders can exacerbate GI symptoms as gastrointestinal motility slows and the gastrocolic reflex is not stimulated. Collaboration with psychiatry and nutrition for treatment of these conditions is extremely important in this patient population. Furthermore, because concomitant diagnoses of POTS and MCAS have demonstrated even higher rates of GI symptoms than in hEDS alone, the autonomic and mast-cell inflammatory effects of these conditions on the esophagus and anti-reflux barrier should also be further investigated. Efforts to identify genetic etiologies, such as the KLK15 gene, can help us better understand underlying pathophysiologic mechanisms as well. Importantly, medications commonly used to treat POTS, MCAS, and DGBI frequently have anticholinergic side effects as well as other GI side effects. 36 Management of this patient population involves careful consideration of pharmacologic side effects as well as multidisciplinary care to manage the various systemic symptoms.
From a GERD management standpoint, endoscopy is safe in patients with hEDS though caution should be exercised when performing endoscopic procedures in vascular EDS. Fundoplication has been shown to have low mortality when performed in other connective tissue diseases. While there is concern that surgical fundoplication could have shorter longevity in hEDS/HSD patients, it has not been explicitly studied and should be investigated further.
hEDS/HSD patients represent a more complex GERD phenotype and their workup should include objective assessment for GERD, as well as inquiry into symptoms and workup of esophageal dysmotility and gastroparesis. Carefully consider all of these overlapping influences when managing this group of patients and setting expectations for outcomes of medical therapy or surgery.
Footnotes
Abbreviations
EDS: Ehlers-Danlos Syndrome
hEDS: hypermobile Ehlers-Danlos syndrome
HSD: hypermobility spectrum disorder
GI: gastrointestinal
GERD: gastroesophageal reflux disease
JHS: joint hypermobility syndrome
POTS: postural orthostatic tachycardia syndrome
DGBI: disorders of gut brain interaction
PPI: proton pump inhibitor
EGD: esophagogastroduodenoscopy
HRM: high resolution manometry
EHR: electronic health record
LES: lower esophageal sphincter
TLESR: transient lower esophageal sphincter relaxations
ICD-10: international classification of disease-10th revision
MCAS: Mast cell activation syndrome
BE: Barrett’s esophagus
Ethical Considerations
Ethical approval is not required for this manuscript.
Author Contributions
Michelle E. Lee – article concept, literature review, manuscript writing, manuscript editing. Lucinda Harris – article concept, manuscript editing. Philip O. Katz – article concept, manuscript editing. All authors (ML, PK and LH) contributed equally to the conception and design of the study. ML drafted the manuscript. All authors provided critical revision of the article and gave final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of Artificial Intelligence
Artificial intelligence (ChatGPT and OpenEvidence) were used for assistance with literature review and table formatting. All AI material was reviewed for accuracy.