
Abstract
Background
The purpose of this study is to explore the diabetes self-management education (DSME) needs of emerging adults with type 1 diabetes mellitus (T1DM) because addressing these needs may facilitate optimal glycemic management during this challenging transitional period.
Methods
A hybrid qualitative design was utilized. Emerging adults and parents of emerging adults were recruited from endocrinology and primary care clinics and through a Utah-specific T1DM online community. Interviews were conducted to asses needs to achieve target A1C. Data were interpreted thematically.
Results
Emerging adults with T1DM (N = 33) and parents of emerging adults with T1DM (N = 17) were interviewed. Three main themes emerged: (1) mixed desire for personal DSME; (2) I don’t need the education, others do; and (3) health care provider (HCP) attributes that make a difference. Associated subthemes were reported.
Conclusions
Emerging adults reported that further education for themselves was not needed, although newly diagnosed individuals would benefit from increased training in diabetes management. Although many emerging adults had a supportive social network, they endorsed the need for greater public education to avoid diabetes misinformation. Emerging adults felt more connected with HCPs that had diabetes-specific training (ie, endocrinologist) or those who personally live with T1DM.
The challenging period of emerging adulthood is characterized by many significant life transitions, emotional instability, and conflicting priorities. 1 Emerging adults living with type 1 diabetes mellitus (T1DM) experience additional distress during this complicated time as they embark on independent management of their diabetes and the health care system. As they attempt to navigate the many demands of emerging adulthood, other priorities often take precedence over T1DM self-management, leading to suboptimal glycemic outcomes. In fact, over 86% of emerging adults with T1DM do not meet the American Diabetes Association (ADA) self-management goal of A1C <7%. 2 Lapses in diabetes care during this critical period are often linked to both acute and long-term complications and mental health comorbidities. 3
The transition from pediatric to adult care also occurs during emerging adulthood. However, the adult diabetes care environment can be overwhelming for emerging adults who need continued diabetes care and emotional support. Emerging adults with T1DM report noticeable differences in the adult care environment, such as decreased emotional support compared to pediatric diabetes care.4,5 Pediatric diabetes care providers deliver family-centered support to the child and family with T1DM. In contrast, adult diabetes providers focus on the individual’s need for optimal diabetes self-management, do not always integrate a support person, focus on long-term diabetes complications, and have rigid self-management expectations.4,6
Developmentally appropriate care is often lacking on the adult end of the transition. Adult providers feel that they do not have adequate resources or training to address the needs of transitioning emerging adults with T1DM. 7 However, emerging adults with T1DM are in great need of continued, developmentally appropriate diabetes care, education, and support from health care providers (HCPs), family, and friends. Specifically, diabetes self-management education (DSME) is recommended during the transition to independent T1DM self-management, a time in which increased emotional stress, support role changes, and many changes in daily life and self-management occur. 8,9
DSME plays a critical role during emerging adulthood. Therefore, the purpose of this study was to examine education needs of emerging adults with T1DM. By understanding the DSME needs and desires of this demographic, HCPs will be enabled to improve health outcomes of emerging adults with T1DM.
Methods
Research Design
A hybrid qualitative interpretive design was utilized in this study. This paradigm explores the ways people interpret their experiences and make sense of their reality. 10
Recruitment
Emerging adults with T1DM and parents of emerging adults with T1DM were recruited by contacting endocrinology and primary care clinics and through a Utah-specific T1DM private online community. Participants were screened for eligibility and could then provide contact information to schedule the interview. Emerging adults with T1DM participants were included if they were (1) 16 to 25 years old, (2) diagnosed with T1DM, (3) and receiving care for T1DM in Utah and (4) had the ability to read and speak English. Parents were included if they (1) were the parent of child age 16 to 25 years old with T1DM receiving care in Utah and (2) able to read and speak English. Both emerging adults with T1DM and parents of emerging adults with T1DM were excluded if they were unable to read and speak English. Written informed consent was obtained from all participants.
Procedures
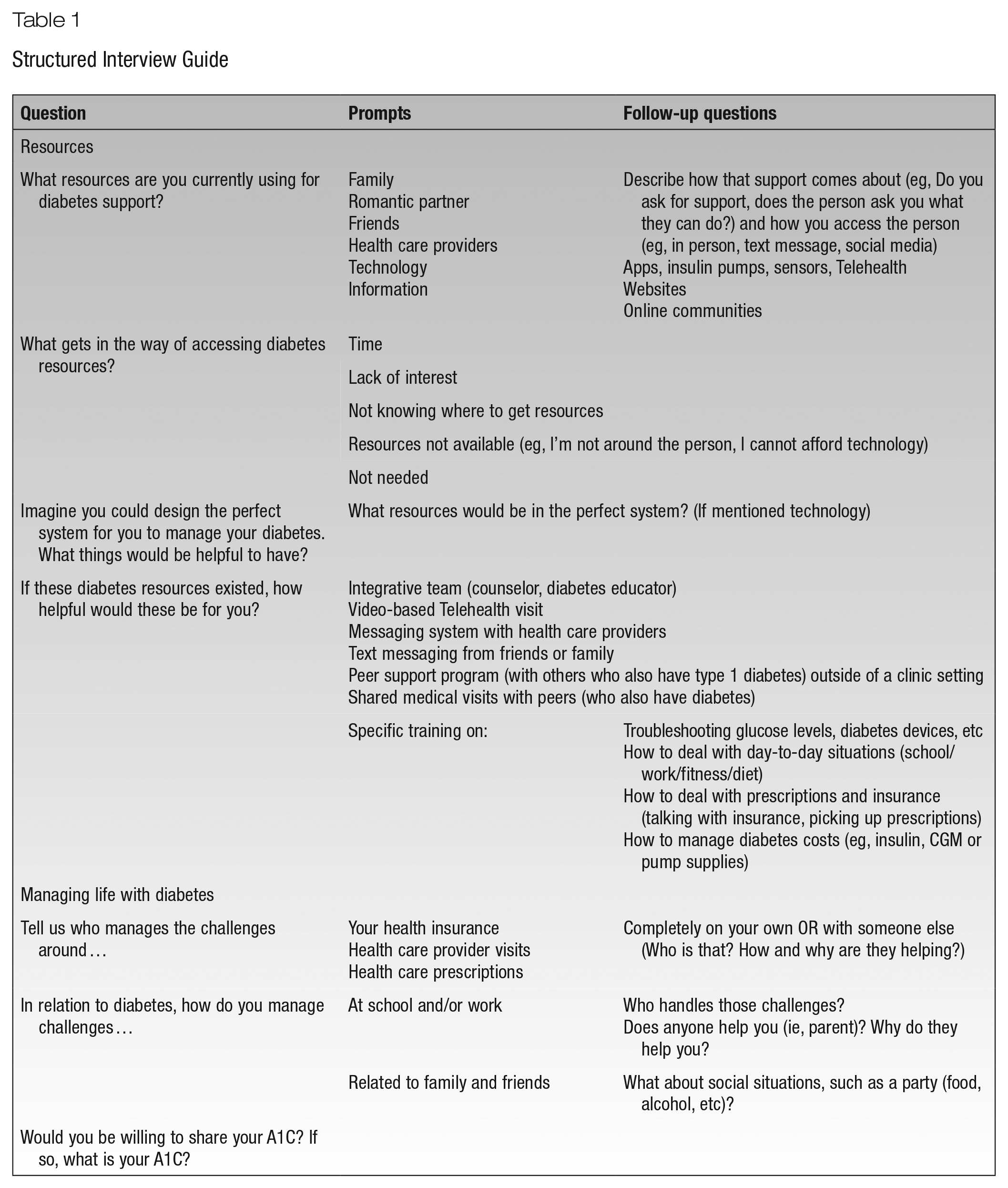
Interviews with emerging adults and parents of emerging adults living in Utah were conducted to assess DSME needs. This study was approved by the University of Utah Ethics Review Board (IRB No. 00126057). There were 33 emerging adults with T1DM and 17 parents of emerging adults with T1DM interviewed by telephone. Each phone call only included the interviewer and the participant. All participants completed the study. Interviews lasted approximately 30 minutes and were conducted by a trained research assistant living with T1DM. Individual interviews focused on what supported and did not support diabetes self-management and what interventions they perceived would be helpful for themselves or others with T1DM their age. A semistructured interview guide developed and pilot tested by the research team (see Table 1) was used. All interviews were audio recorded and transcribed verbatim through CaptionSync software within 1 week following each interview. Researchers verified transcripts for accuracy by reviewing each interview transcript alongside its corresponding recording. Field notes were not made during or after interviews. No repeat interviews were conducted, and data saturation was met.
Structured Interview Guide
Data Analysis
Qualitative interpretive analysis of interview transcripts was conducted11,12; NVIVO Version 11 13 was used to code the data. First, the authors coded 3 of the emerging adult interviews to develop the initial codebook of recurrent themes. Using this codebook, the remaining emerging adult and parent interviews were coded by authors working in pairs or individually. Each interview was reviewed by at least 2 researchers during this process. Using an open coding approach, new codes were added ad hoc. 11 After all interviews were coded, researchers reviewed the codes to determine overarching themes and the frequency of recurrence of each theme. Special note was taken of specific quotes that best represented these themes. Codes were compared, contrasted, and collapsed to develop corresponding themes.10,14
Results
Participant Characteristics
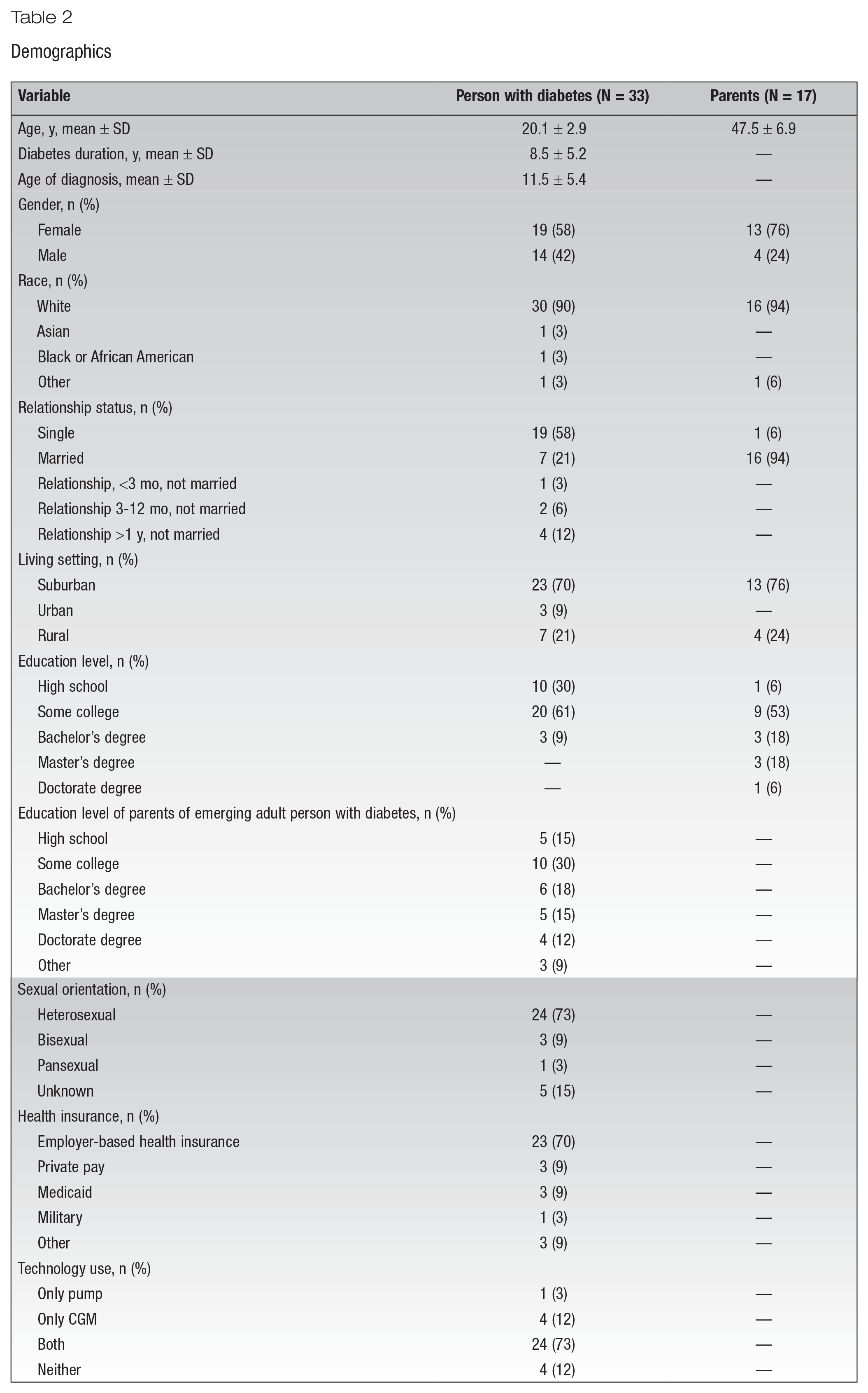
Participants were 33 emerging adults with T1DM and 17 parents of emerging adults with T1DM. The mean age of emerging adults was 20.1 years (±2.9), and mean age of parents was 47.5 years (±6.9). The majority of the emerging adults were CGM and insulin pump users (N = 24, 73%). See Table 2 for additional demographic details.
Demographics
Themes
Three themes emerged from the interviews, and each theme had distinct subthemes. In the following, each theme is described with excerpts from the interviews to illustrate the important subthemes.
Mixed Desire for Personal DSME
People with diabetes (PWD) expressed a desire for increased DSME for newly diagnosed individuals and families and greater awareness of diabetes within their community. However, PWD were not interested in refresher courses.
Enhanced DSME needed for those at T1DM diagnosis only
Many participants discussed a need for DSME for newly diagnosed PWD only. This education should go beyond basic DSME to include T1DM management strategies of navigating daily life, unexpected situations, or emergency scenarios. One PWD stated, “More education would be perfect for newly diagnosed people to understand what happens when you go to a restaurant, or what happens if your insulin vial breaks—just how to deal with different scenarios.”
To assist new PWD in adjusting to their diagnosis, increased DSME for support individuals is necessary as well. When recalling experiences with newly diagnosed individuals, one person with diabetes stated, “[Newly diagnosed] families are just so overwhelmed. They’re like, ‘We don’t know what we’re going to do when we get home.’ More education would be super, super beneficial, at least until they can get the hang of it.” Participants suggested educators go through different scenarios with families, including how they specifically can be helpful in those situations.
Although the desire for enhanced education for newly diagnosed PWD was prevalent, all participants reported that additional education would not be beneficial for them now. One person with diabetes stated, “I don’t know that I’d need more education for me—I’ve had it for 12 years.” Participants described that their lived experiences with diabetes precluded them from needing any additional education from HCPs unless those HCPs lived with T1DM themselves.
Reliance on peer support for learning
Participants were interested in receiving experiential education from peers with T1DM in online and face-to-face settings. Interests were based on day-to-day scenarios (bolusing for certain types of food, how to engage in sports, etc). One parent of a person with diabetes explained, “Every summer 75 kids with T1DM get together and play basketball and learn how to manage their type 1-ness when they’re playing sports. It becomes like a fraternity—it’s an incredible thing.”
Peer support outside of a clinical setting provides access to real-world, daily T1DM management that many were unable to access through HCP visits. One PWD stated, “It has been really cool to talk to others my age and even before I got pregnant, I was able to talk to others [with diabetes] and get advice and talk to them about their own struggles.”
The ability to interact (in person or online) with others living with T1DM provided a helpful resource for learning and support for PWD. One participant reported, “One of my greatest blessings is having friends who are also diabetic. We all support each other and ask things like ‘how are you feeling about your management?’” Another participant stated, “I Snapchat one of my friends about [T1DM] stuff, so I don’t really ever feel like I’m alone [with T1DM].” Asking questions within an online peer support group was preferred over Google to avoid misinformation and to obtain T1DM-specific information.
I Don’t Need the Education, Others Do
Although PWD reported additional personal education as unnecessary, participants did express the desire for increased DSME in family members, friends, and the general public.
Need for increased DSME in family members
Although many participants reported receiving support from family and friends, others felt misunderstood and not supported. Participants reported that although they felt family members were educated on diabetes self-management, they sometimes made comments that were not supportive or empathetic, resulting in frustration. One emerging adult with T1DM stated, “Most of the challenges that have come up are with my dad, because he thinks he knows what’s best for me with diabetes. But he actually doesn’t know hardly anything about diabetes. He’s always like, you need to get your glucose down, you need to do this and that. He just doesn’t understand, it’s not that easy.”
Others reported feeling frustrated about lack of family and friend knowledge regarding T1DM. One participant stated, “I’ll try to explain things to them, but they’re not really involved much. They think they know everything just from being there for one doctor visit? They definitely need to learn more.” Another PWD reported, A lot of my family doesn’t quite understand it. So, they’ll say something, and I know it’s wrong. I’ll try and teach them, and if they’re too stubborn, I just kind of nod my head. I know what’s right, and I know how to take care of myself. But sometimes they do the wrong thing. For example, one time my grandma said, “I have sugar free candy for you.” But then I read the back and there were 64 carbs in it.
Participants felt isolated and unsupported because family members were never provided with comprehensive DSME. One participant stated, “I feel like there’s not that many resources out there for family and friends to go and learn these things.” Another person with diabetes explained, There’s not that many people out there who’s willing to say, hey, bring your family, we’ll talk with them about this. Even when I was first diagnosed, the doctor is just like, oh, yeah, like your dad’s right here, he can just watch you do this, but never really discussed things with him. So they don’t really know much. I mean, they know the basics from what I’ve told them, but other than that, I’m kind of on my own.
However, emerging adults who were in relationships did not describe the need to train spouses or new partners on T1DM.
Desire for T1DM public awareness
PWD expressed concern and frustration with the lack of general public awareness about T1DM. Participants explicitly wanted the public to be aware of the differences between T1DM and T2DM, that their diet is not limited as long as they take insulin, and that they did not do anything to cause their diabetes. Lack of public awareness increased a perceived sense of stigma among emerging adults with T1DM because they felt others equated them to people with T2DM. One participant stated, “People tell me ‘If you just lose some weight and exercise, you won’t have diabetes anymore.’ I’m like sure, that’s not how it works for me.”
Combating misinformation is a regular issue for many emerging adults living with T1DM, and the task of educating others about T1DM can be burdensome. One participant stated, “A lot of people say ‘just take essential oils and pills, this will cure your diabetes.’ They don’t understand this disease . . . so I try to stay around people who I know and trust.” The widespread misconceptions affect emerging adults in academic institutions as well. A person with diabetes stated, “Type 1 diabetes is not taught very well to the public and people have a misunderstanding what it actually is. When I present my diabetes accommodation letters to college professors, having to explain T1DM to them is my biggest fear.” Fears related to faculty invalidating the need for accommodations was a major concern. Misperceptions around diabetes are reinforced due to media (television, movies) and society (health campaigns), which can result in public perceptions of stigma.
HCP Attributes That Make a Difference
Emerging adults living with T1DM indicated that their HCPs were resources in diabetes management if they were highly accessible and personally understood T1DM. However, not all HCP encounters were like this.
Lack of T1DM specialty training
PWD appreciated HCPs who had advanced training in T1DM, such as endocrinologists and diabetes care and education specialists (DCES). PWD described disappointing experiences with HCPs not trained in an endocrinology specialty (ie, primary care, emergency room, or hospitalist) due to the HCPs’ lack of T1DM knowledge. One participant described her recent T1DM diagnosis in the emergency room: “They had no idea. As a brand-new diabetic that has no idea what’s going on, that is so disappointing and so scary. You trust these health care workers and they have no idea how to help you.” A person with diabetes from a rural area had higher expectations for HCPs in the city; one stated, “I was really surprised that a [urban city] hospital doctor had no idea what to do with a type 1 diabetic.”
Emerging adults living with T1DM also described a marked difference between what HCPs learn in school versus real-life management of T1DM. One participant stated, “There is disconnect with a lot of health care providers that don’t have diabetes. So, it’s just like what they read in the textbook is like the only reference that they ever had with it.”
HCPs who personally understand T1DM
PWD especially appreciated those who personally “got it” because they lived with or parented a child with T1DM. One emerging adult stated, “[My HCP] has been the biggest support. Not only is he diabetic, but he has 2 twin sons who are diabetic as well. And he just knows everything.” Another participant stated, “my endocrinologist is super awesome. I recommend him to all of my Type I Diabetic friends. He’s also a Type I diabetic himself and he’s been dealing with it for several years. He’s very encouraging, very positive, makes sure that nobody ever feels like they’re being punished or being labeled by their diabetes.”
Emerging adults reported that seeing an HCP who also lives with diabetes helps promote collaborative conversations about diabetes management. One participant recounted, “My current doctor will say, hey, I get how it is. He’s diabetic as well. He can say, ‘I’ve been through that, here’s what I’ve done, here are other ideas’ and so on. It just feels more personal and it makes having the disease more normal, if that makes sense.” In some instances, health counseling from HCPs personally affected by T1DM are more highly regarded. One parent added, “[My son] takes [physician with T1DM] advice and recommendations a lot more seriously, even though the other doctors I’m sure are good and everything but it’s just like, ‘OK, that guy gets me. That guy knows what it’s about.’” Having an HCP who personally understands T1DM can facilitate the development of a positive relationship between the emerging adult living with T1DM and the HCP.
HCPs who address mental wellness and coping
Whether the HCPs personally had T1DM or not, HCPs who were encouraging and supportive and addressed psychosocial health in addition to biophysical health were viewed by PWD as more resourceful. Participants wanted HCPs to recognize the effort it takes to manage their diabetes and celebrate the smalls wins. One person with diabetes stated, From one appointment to the next, I dropped my A1C down by three whole points, which is a huge deal for me. It took a lot of work to get there. And then I got to my appointment and my doctor said, “oh, that’s better, but that’s not good enough.” And to me it was like, oh, he just cares about my numbers. He doesn’t care how hard I worked or anything. And that actually made me feel like I might as well just give up.
PWD wanted their HCPs to acknowledge and discuss emotions, coping, and burnout. They also wanted HCPs to acknowledge how hard they were working with a condition that provided no breaks. One participant described, “I’ve had the health care providers in the past that would not sympathize at all. They just kind of say, here’s what you’re doing wrong, do it better.” Essentially, emerging adults with T1DM wanted HCPs to consider what it would be like to walk in the shoes of someone with diabetes. Additionally, emerging adults wanted their HCPs to be able to provide concrete resources to support psychosocial health, such as support groups (ie, online peer support communities).
Working with a responsive HCP team
Most participants described having access to a multidisciplinary diabetes care team. Team members included endocrinologists, pharmacists, DCESs, and school nurses. PWD saw the role of their HCPs as being a partner or “working together as a team in order to overcome obstacles.” This perceived partnership is valued by emerging adults, and participants reported frustration when HCPs are not responsive to their desires for their own diabetes management. One parent recounted her son’s experience, “He was going to switch over to the Control-IQ, but he didn’t want to right away because he didn’t want to mess up his routine. The nurse practitioner educating him was really condescending about it.”
Participants found that HCPs who made themselves available outside of office hours were particularly helpful in diabetes management. Issues addressed outside of office hours included emergent situations, technology questions, day-to-day challenges (ie, insulin adjustment for exercise), and filling prescriptions. Emerging adults with enhanced access to their HCP team could text message HCPs’ personal cell phones, whereas others would call, page, or email the office. One person with diabetes stated, “I can just text [my diabetes educator] anytime I have a question, which I love.”
Discussion
DSME in its present form is not meeting the needs of emerging adults. Specifically, emerging adults prefer learning from peers as opposed to one-on-one visits with HCPs after initial diagnosis education. Emerging adults wanted to feel better supported in their T1DM by having family, friends, and the general public be more aware of what T1DM is, its distinction from T2DM, and the challenges that people with T1DM face. Barriers to diabetes management include HCPs who lack expertise in T1DM-specific needs and do not provide sufficient mental health support. Facilitators to diabetes management for this age group included HCPs who have a personal relationship to T1DM and who provide immediate diabetes-related feedback.
The ADA recommends DSME be provided to PWD at diagnosis and at regular intervals throughout the life span, particularly during significant life changes and periods of high stress, such as the transition to emerging adulthood. 15 During life transitions, additional diabetes self-management education and support is critical. In this study, emerging adults and parents were not interested in generalized, structured DSME at this stage beyond what was necessary at initial diagnosis. Moreover, emerging adults desired real-world tips and tricks for handling common and rare diabetes situations rather than generalized diabetes education. Thus, effective DSME may be more beneficial when emerging adults initiate relevant discussion topics and work with the HCP and peers to apply real-world problem-solving techniques. These findings show the need for DCESs to be flexible when working with emerging adult populations. An example of this is providing virtual shared medical visits with other emerging adults with T1DM and allowing the emerging adults to pick the discussion topics, which has been found to be highly satisfactory among this population. 16
There was a lack of knowledge in supporting emerging adults with T1DM among HCPs across various settings. HCPs such as medical doctors, nurse practitioners, and physician assistants do not have uniform training in diabetes, and most education is geared toward T2DM management.17,18 Interacting with HCPs who do not have sufficient training in T1DM can be frustrating for emerging adults and can hinder the development of trust in the patient-provider relationship. HCPs may find it challenging to stay updated with the most current standards of care for diabetes, which the ADA updates annually. Also, HCP education may not cover the complexities of T1DM, such as intensive insulin management, navigating diabetes technology, effective coping strategies, and challenges beyond the mechanics (ie, glucose checks, taking insulin) of T1DM management.19,20 Similar to findings in another study, PWD and parents in this study desired good relationships with their HCP and wanted HCPs who were more informed and understood the intricacies of T1DM. 21 Therefore, increasing training about T1DM across HCP specialties is needed. This training is especially important given the increased use of diabetes technology.
Study participants preferred seeing HCPs who were living with diabetes because emerging adults perceived that these HCPs understood the unique challenges of T1DM and could offer helpful insights and useful strategies about diabetes management. To address the need for T1DM-specific training among HCPs not living with diabetes, one study had a novel approach in which they provided HCPs with a high-fidelity simulation of living as if they had diabetes. 22 Innovative ideas to approach this need for T1DM-specific training merit further investigation. An umbrella review conducted by Greenwood et al 23 suggests technology-enabled self-management using a 2-way feedback loop results in A1C reduction. Real-time communication with HCPs can empower emerging adults to adjust their diabetes management as situations arise rather than waiting weeks or months for a formal office visit. Messaging systems between emerging adults and HCPs such as HIPAA-compliant apps and protected emails may be employed as an important measure to improve glycemic outcomes.
Increased access to educational materials geared toward friends and family members of individuals with T1DM is desired. Unfavorable stereotypes of diabetes are often represented in mass media, and combating these pervasive misconceptions can take an emotional toll on PWD.24,25 In this study, emerging adults received unwanted diabetes advice from family and friends that was more specific to managing T2DM. Because of the common misperception that they have T2DM, emerging adults were afraid at times to advocate for themselves because they feared that others would not understand their needs. PWD also reported feeling burdened with teaching others about T1DM. Similar findings were identified in another study where emerging adults worried that people had poor opinions about them due to a belief that the PWD should be able to fix their diabetes with diet and exercise. 26 These emerging adults also reported being treated differently when they informed people about their diabetes, and they therefore limited the number of people to whom they disclosed their diabetes.
Although PWD in both studies did not want to be identified with T2DM, this is in of itself a negative diabetes stigma called “othering.” Diabetes-related stigma has a negative influence on psychosocial well-being and clinical outcomes. Thus, it is critical to find strategies to address diabetes-related stigma. Providing more societal education about diabetes and various causes beyond lifestyle and including PWD in producing mass media can reduce this stigma and improve public messaging about diabetes. It is crucial that diabetes be represented accurately, and not as a punchline, to improve public awareness and decrease stigma. More study is needed in this area to elucidate how the public can support a positive illness identity.
Additionally, peer support was identified as a source of social support to augment mental health needs and stigma. There are regional and national online peer support groups that HCPs may want to familiarize themselves with and refer when indicated. A review of online peer support groups has indicated that misinformation is low when people are engaged in online peer support groups (as opposed to using search engines to seek answers to questions) and is associated with improved behavioral and clinical outcomes. 27 Importantly, peer support with a focus on mental health can mitigate diabetes burnout that is common in emerging adults. 28
Certain limitations were present in the study. The majority of the sample were White, heterosexual, and living in a suburban area. Most of the emerging adults expressed strong family support, which may be dissimilar to many living with T1DM. Many PWD in this study used diabetes technology (88% of participants used an insulin pump, CGM, or both), which may not be representative of all emerging adults living with T1DM.
Clinical Implications
This study supports the need to tailor the delivery of DSMES to better support emerging adults during this transitional life stage. Emerging adults living with T1DM desire diabetes care and education that meets their needs and uses creative strategies such as real-world problem solving and peer support. PWD and their parents want their HCPs to have in-depth diabetes training, greater understanding surrounding emerging adult life challenges, new strategies to tackle the tough problems PWD face, and conversations that are not solely focused on glucose levels. Moreover, DCESs working with emerging adults can engage support persons and peers, consider the impact of stigma on diabetes self-management and emotions, provide education related to daily life and activities relevant to emerging adulthood, and provide additional mental health and social media resources. More research is needed to explore specific practices and their efficacy in diabetes management among emerging adults living with T1DM.
Footnotes
Conflict of interest:
Litchman is PI of an investigator-initiated trial funded by Abbott Diabetes Care unrelated to this study. Allen and Litchman are multiple PIs of an investigator-initiated study that has received a small equipment award from Dexcom. Blanchette is the ADCES/CBDCE Fellow in Integrated Diabetes Management, a consultant for WellDoc, Inc, an independent contractor for Insulet Corporation and Tandem Diabetes, and an Advisory Board Member for Cardinal Health and Prevention Bio; these conflicts are unrelated to this study.
Funding:
This study was funded by the Sorenson Legacy Foundation.