
Abstract
Purpose:
This purpose of the study was to describe recent diabetic ketoacidosis (DKA) incidence data in youth with type 1 diabetes using insulin pumps and the impact of continuous glucose monitors (CGMs) on DKA rates.
Methods:
DKA data were obtained through a retrospective chart review of insulin pump users (ages <26 years) between December 2019 and June 2021 in an academic pediatric endocrinology practice where 68% of patients were pump users.
Results:
Among 591 pump patients, 28 events occurred (3.16 events per 100 patient-years). Mean age was 13.6±3.4 years; 85.7% ranged from 12 to 19 years. Mean A1C was 10.2±2.3%, diabetes duration was 6.1±4.0 years, and 57.1% used CGM. Admission pH levels ranged between 7.0 and 7.31, with 28.6% of events classified as “moderate” and 46.4% “severe.” There was no significant difference in the DKA severity between those who wore a CGM and those who did not (ie, pH, serum bicarbonate, mentation alteration, length of stay, intensive care unit admission, and hospital admission). DKA events were attributed to concurrent illness (10.7%), insulin omission (14.3%), pump site failure (57.1%), or other pump malfunctions (14.3%).
Conclusion:
DKA events in pump-treated patients were relatively uncommon; most episodes occurred in adolescents with higher A1C levels, and notably, most events could have been avoided if users followed standard troubleshooting guidelines. Thus, DKA prevention education should be reinforced at each encounter, particularly for teens with higher A1C levels. Moreover, more than 50% of those with DKA episodes wore a CGM, suggesting that pump users using CGM require frequent reinforcement of this education and that the development of such educational materials is critical.
While insulin pump therapy as a treatment for type 1 diabetes (T1DM) was introduced more than 40 years ago, 1 very few pediatric patients initially used these devices. However, results of the Diabetes Control and Complications Trial demonstrated that improved diabetes control was achievable with intensive insulin regimens. 2 Moreover, with advancement of insulin pump technology, many children are now treated with insulin pump therapy. For example, data from a large European database have shown that the percentage of pediatric patients using insulin pumps increased from 1% in 1995 to 53% in 2017. 3 In the United States, the percentage of patients using an insulin pump in the Type 1 Diabetes Exchange Registry of over 22 000 people with T1DM increased from 7% in 2010–2012 to 63% in 2016–2018, with a greater than 10-fold increase specifically in children. 4
Despite the technological advances in insulin pump therapy, diabetic ketoacidosis (DKA) remains a potential risk of all insulin regimens, including insulin pumps. DKA has long been recognized as a potentially fatal, acute complication of T1DM in children, 5 and earlier studies have suggested that the use of an insulin pump places one at increased risk for DKA compared with injection regimens. 6 However, more recent studies have found DKA rates to be either lower than7-10 or similar 11 among youth using insulin pumps compared with those on injection regimens. Furthermore, among the 22 697 participants in the Type 1 Diabetes Exchange registry from 2016 to 2018, those who wore an insulin pump (63% of participants) were less likely to report a DKA event within the 3 months prior to the data collection. Of note, the highest rate of DKA events occurred in participants who were 26 years of age or less, and rates were higher across the whole cohort in patients with higher A1C levels. 4
In addition, there has also been a significant increase in the use of continuous glucose monitors (CGMs) among insulin pump wearers. In fact, use of sensor technology has increased in participants of the Type 1 Diabetes Exchange Registry from 6% in 2011 to 38% in 2018. 4 One could theorize that using a CGM might decrease the risk of DKA because the device would alert the user when the blood glucose level was persistently high and motivate the user to take preventive action steps. Indeed, CGM users who participated in both the Type 1 Diabetes Exchange Registry in the United States4,12 and the large European registry, the Diabetes Prospective Follow-up (DPV), 13 had fewer DKA events compared with those who did not wear a CGM. However, a recent meta-analysis of 21 different studies 14 did not show that CGM use influenced the incidence of DKA events. The purpose of this study therefore was to obtain more recent DKA admission data over an 18-month period in youth with T1DM using insulin pumps and the impact of CGM on DKA rates. Specifically our research questions were: (1) What is the incidence of DKA events in youth wearing insulin pumps? (2) Are there patient characterisitcs, such as age, disease duration, level of metabolic control, etc., that make youth wearing insulin pumps more at risk for DKA? and (3) Does wearing a CGM impact the rate of DKA events among youth? The results can provide critical information for both clinicians and diabetes educators to guide the diabetes education they provide to insulin pump users and their families regarding DKA prevention.
Methods
Design
A retrospective chart review was completed to obtain DKA data in insulin pump users with T1DM from all hospitalizations occurring between December 29, 2019, through June 29, 2021, at a large academic pediatric endocrinology practice. Given the relative rarity of DKA events, a retrospective chart review over an 18-month period was the ideal methodology for this study to examine the incidence of DKA events in pump patients. This design allows clinicians to learn from their rich, readily available clinical data, which can inform future practice and diabetes education.
Recruitment
Local investigational review board approval was obtained in accordance with the Declaration of Helsinki. The investigator completing the chart review (EAD) obtained the list of charts to review daily from the standard Emergency Room/Hospital Admission Notification Protocol (provided to all diabetes providers daily) already in place at this practice. For this protocol, the on-call endocrinology fellow sends a daily, secure, electronic daily update to all diabetes clinicians affiliated with the practice describing any activity in emergency rooms and hospital admissions involving diabetes patients.
Setting
The study was conducted over an 18-month period in a large pediatric diabetes clinic located at an academic center in Connecticut. This diabetes center cares for approximately 870 youth with diabetes, among which 591 (68%) wear an insulin pump to manage their diabetes.
Participants
The sample consisted of all patients with T1DM from the pediatric endocrinology practice admitted with the diagnosis of DKA to either the emergency department or hospital during an 18-month period (ie, December 29, 2019, to June 29, 2021). Inclusion criteria included age less than 26 years, diagnosis of T1DM, treated with insulin pump therapy, and admitted to the emergency department or hospital with a diagnosis of DKA. Any patient with type 2 diabetes was excluded.
Data Collection
One investigator (EAD) completed a chart review for all subjects meeting the inclusion criteria using a standardized data collection form. The following data were collected: date of DKA occurrence, duration of diabetes, number of past DKA events, age, gender, race, ethnicity, most recent A1C level, type of insulin pump used, type of CGM used (if applicable), and type of insulin used. Specific data regarding the presentation and treatment of the DKA were collected, including whether or not participants were admitted, length of stay, whether or not they required admission to the intensive care unit, DKA severity classification (severe, moderate, or mild as designated by treating endocrinologist), admission pH, serum bicarbonate (HCO3), whether or not there was a concurrent infection/illness, presenting signs and symptoms, and the treating endocrinologist’s assessment of the likely cause of the DKA event. All data were de-identified. Data were collected electronically using Microsoft Excel (version 16.52) and stored in password-protected files on a university encrypted laptop computer.
Data Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 28 (IBM Corporation, Armonk, NY). Statistical significance (α) was defined as a probability level of less than or equal to 5% (P ≤ .05). Descriptive statistics were used as appropriate to describe the sample. Student t tests and chi-squares were used to compare data between those subjects who used a CGM versus those who did not.
Results
Among 591 youth and young adults with T1DM wearing an insulin pump, 4% experienced a DKA event during the 18-month data collection period, for a total of 28 events (3.16 events per 100 patient-years). The majority of these events (85.7%) occurred in adolescents, ages 12 to 19 years. Approximately 60% of those who had an event were male, 53.6% were White, 29.6% were Hispanic, and the mean age was 13.6 ± 3.4 years. Youth who had a DKA event had an average duration of diabetes of 6.1± 4.0 years, and metabolic control was suboptimal (mean A1C level of 10.2 ± 2.3% [88 ± 2 mmol/mol]; range 7.0%-16.7% [53->151 mmol/mol]). Fifty-seven percent of subjects were wearing a CGM at the time of the event, and only 1 subject was using a hybrid closed loop (HCL) insulin delivery system. In 28.6% of the events, the subject was new to pump therapy (ie, wore an insulin pump <12 months).
DKA events were classified by the treating endocrinologist according to severity: mild, moderate, or severe. This classification was based on arterial pH, serum bicarbonate level, and/or mental status. Only 1 subject had a significant acute mental status change. Approximately 21% (21.4%) of the events were classified as mild, 32.1% as moderate, and 46.4% as severe. Admission pH levels ranged from 7 to 7.31, with a mean of 7.18 ± 0.09, and serum bicarbonate level was 10.76 ± 3.70 mEq/L, with a range of 3.0 to 18 mEq/L.
The treating endocrinologist attributed the cause of the majority of the DKA events (57.9%) to pump site failure (ie, bent or displaced catheter) and an additional 14.3% of the events to a pump malfunction. Insulin omission was attributed to 17.9% of the events. Illness only accounted for 10.7% of the DKA events. Alcohol was a potentially contributing factor in 1 event.
It is particularly noteworthy that there was no significant difference in the number of events in those who wore a CGM versus those who did not despite those wearing a CGM having lower A1C levels (9.4% ± 1.6% vs 11.3% ± 2.7% [79 vs. 100 mmol/mol]; t = −2.29, df = 26, P < .05). CGM wearers also had a shorter duration of T1DM (4.8 ± 3.7 vs 7.8 ± 3.8 years; t = −2.11, df = 25, P < .05; Tables 1 and 2).
Characteristics of Pump Users With DKA Events
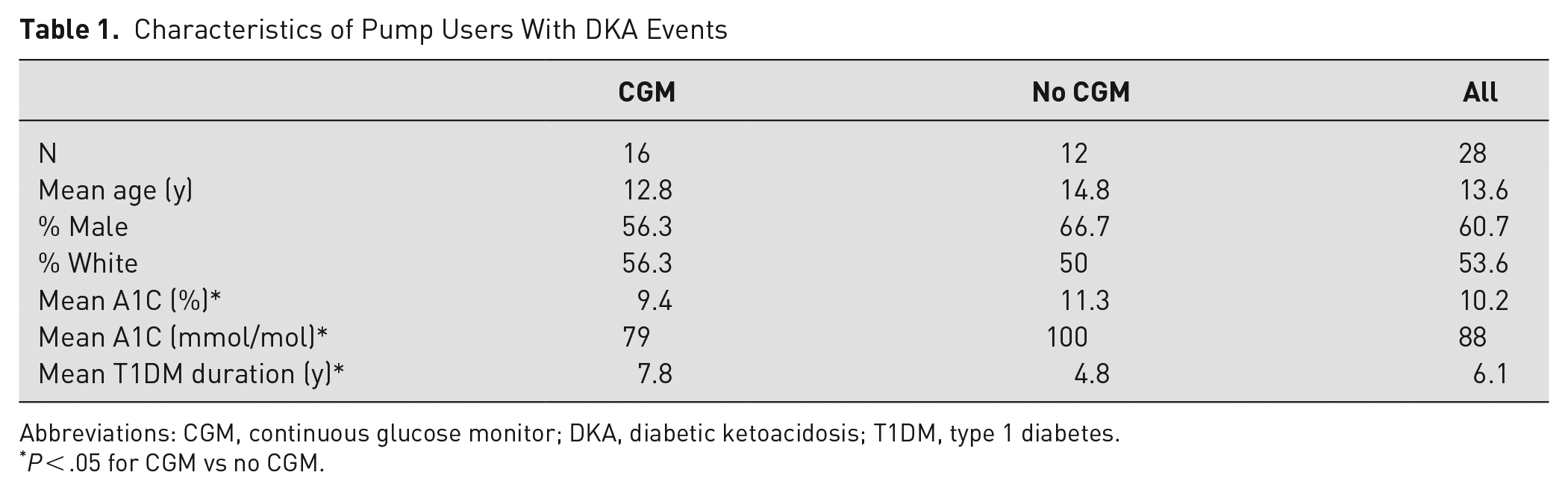
Abbreviations: CGM, continuous glucose monitor; DKA, diabetic ketoacidosis; T1DM, type 1 diabetes.
P < .05 for CGM vs no CGM.
Characteristics of DKA Events
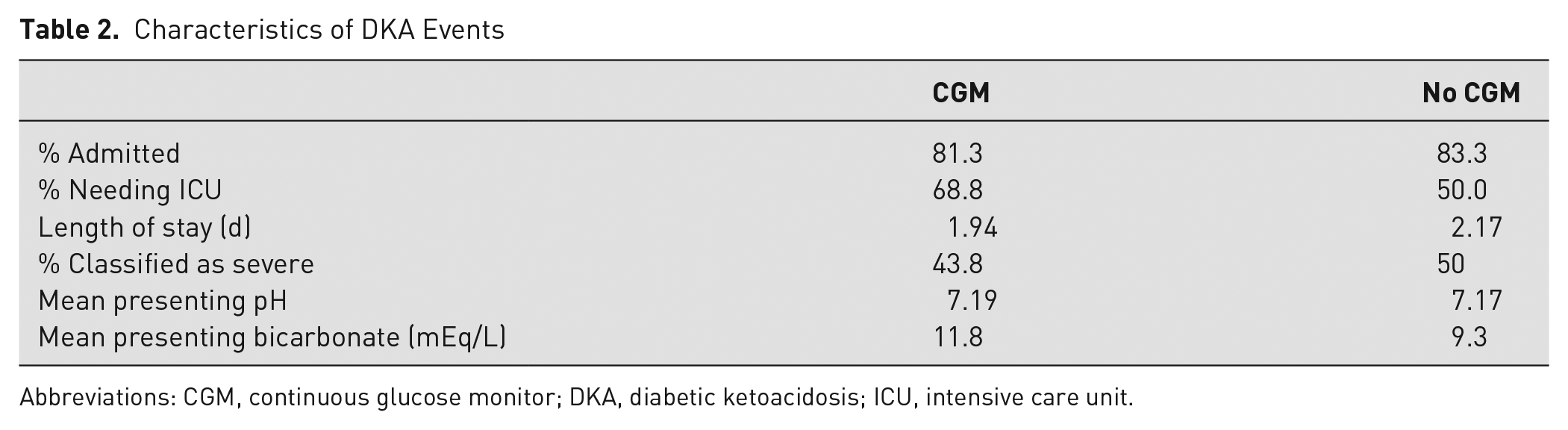
Abbreviations: CGM, continuous glucose monitor; DKA, diabetic ketoacidosis; ICU, intensive care unit.
Discussion
In this clinical practice, where 68% of paitents utilize insulin pump therapy, only 4% of pump patients less than 26 years of age were admitted to a tertiary hospital or emergency department for DKA. With the wide use of sensor technology today in the care of youth with T1DM, one might assume that youth with T1DM wearing an insulin pump and CGM may be at a lower risk for a potentially dangerous DKA episode. However, this is one of a few recent studies that demonstrated that DKA remains a risk for youth on insulin pumps, including those who also wear a CGM. It is also important to note that the data for this study were conducted during the COVID-19 pandemic. Indeed, Lavik et al 15 recently reported that rates of DKA were higher during 2020 than in 2019 in 7 large medical centers in the United States.
In this sample, insulin pump treated youth admitted with DKA had A1C levels well above targets set by the American Diabetes Association. 16 This is consistent with earlier reports 17 and with the more recent US T1DM Exchange Registry 4 data, where there was at least 1 recent DKA episode in 7% of those with an A1C >9% (75 mmol/mol) compared with only 0.7% of the participants with an A1C <8.0% (64 mmol/mol). Moreover, the European DPV Registry also demonstrated a similar correlation with DKA rates and higher A1C levels. 13 Thus, it is critical that clinicians recognize that pump patients in suboptimal control are at higher risk for DKA and reinforce DKA prevention principles as well as the importance of improving metabolic control.
It is also noteworthy that the majority of the DKA episodes (85.7%) occurred in adolescents, similar to earlier reports.4,13,17 Thus, DKA prevention principles must be particularly reinforced with adolescents with T1DM.
In this study, the most common cause of DKA was either a pump site failure or pump malfunction (72.2% of the events). Fewer events were related to insulin omission (17.9%) and infection/illness (10.7%). Thus, the gross majority of these events (89.3%) could have been avoided if youth followed troubleshooting guidelines and DKA prevention principles taught to patients and families when they initiate pump therapy.
With the constant feedback alerting the wearer of hyperglycemia, one might theorize that there would be fewer DKA episodes in patients who wore a CGM because the user would be alerted to take corrective actions. Large registries of patients with T1DM, both in the United States 4 and Europe, 13 have indeed demonstrated this to be true. However, in our sample, 57.1% of pump wearers hospitalized for DKA wore a CGM. Additionally, DKA episodes had similar severity markers (pH, serum bicarbonate, length of stay, and whether or not ICU care was required) whether or not the patient wore a CGM. Thus, given that most of the DKA events that occurred were potentially avoidable if corrective steps were taken earlier, clinicians must continue to reinforce DKA prevention strategies and high blood glucose troubleshooting in all their pump users, including those who also wear a CGM.
Only 1 subject was utilizing an HCL system when the DKA event occurred. In recent studies of children using HCL technology for 3 to 6 months, there were either no18-20 or very few (3.3%) 21 subjects who had a DKA event during the study period. While these studies were of short duration, there may be fewer events of DKA in pediatric HCL pump wearers with this newer technology’s direct insulin delivery feedback and additional alarms for persistent hyperglycemia.
Strengths and Limitations
A strength of this study is the fact that this was a large, diverse, pediatric endocrinology practice in which the majority (68%) of children wore insulin pumps. Clinicians caring for these youth had extensive experience in using pump therapy in youth. However, studies on insulin pump therapy from this center may not be generalizable to all pediatric centers caring for youth with diabetes. Despite the fact that data were collected for 18 months, there still was a relatively small sample size due to the low frequency of these events. Larger, prospective, multicenter studies are needed to better characterize DKA events in children wearing insulin pumps. These studies should characterize not only the events themselves but also the influence of CGM use and HCL technology on DKA incidence rates. Additionally, these data were collected during the COVID pandemic, and therefore DKA prevalence rates may not be representative of time periods without a pandemic.
Implications for Diabetes Education and Clinical Practice
Given that 89.3% of the DKA events were likely avoidable if the youth and their families followed standard guidelines regarding high blood glucose troubleshooting and DKA prevention, this study illustrates the importance of frequently reinforcing this diabetes education at every encounter with the patient. Providing written guidelines can be very helpful to families. An example is provided in Figure 1. Vitale et al 22 demonstrated that a brief educational session on sick day management specific to treatment modality (ie, pump vs injection) and the provision of a take-home flow sheet with guidelines for diabetes sick day management resulted in improved knowledge of signs and symptoms of DKA and proper sick day management and less emergency department visits for adolescents.
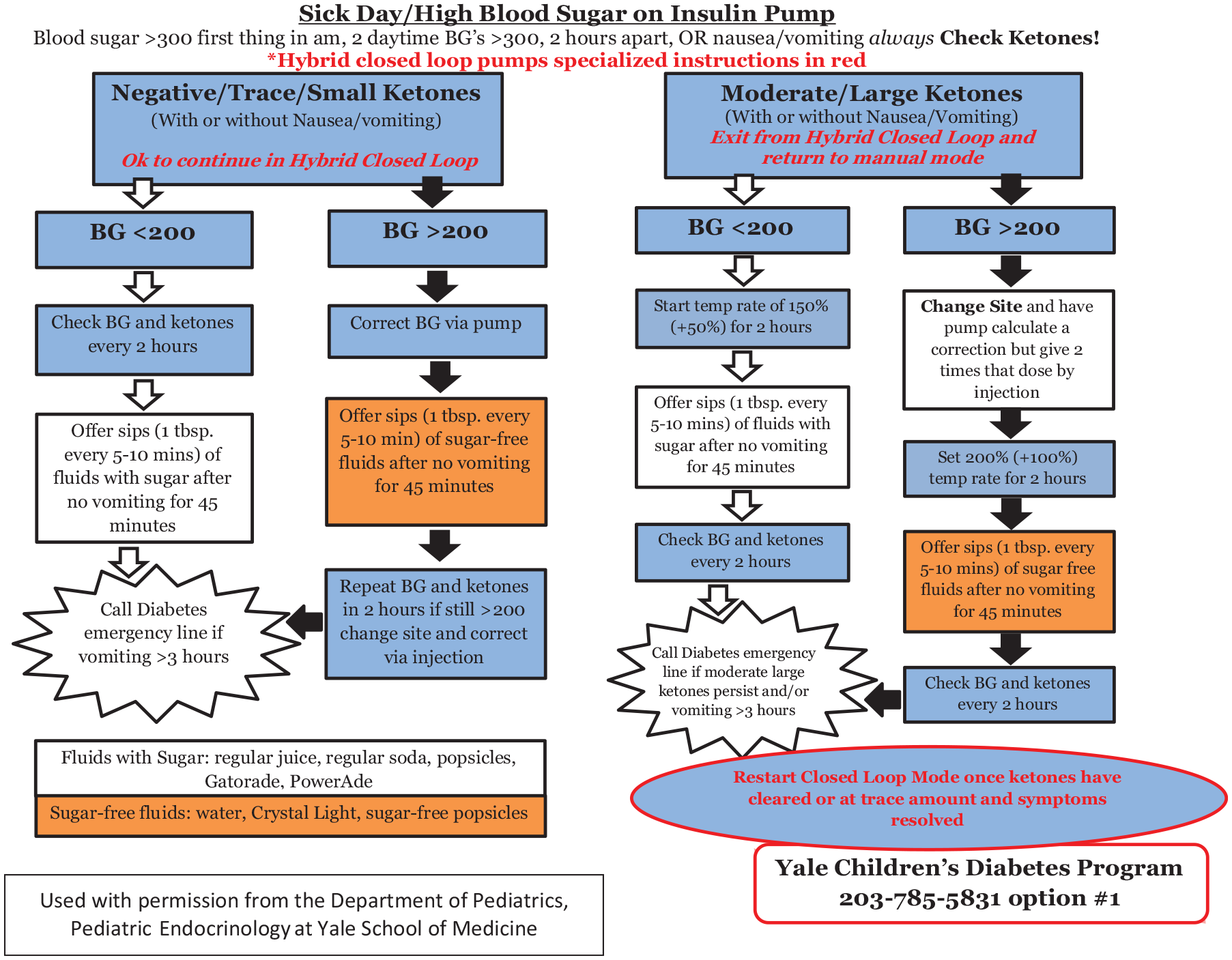
Sample sick day/high blood glucose patient education.
Pediatric patients who wear insulin pumps, including those who also use sensor technology, need frequent reinforcement of basic education regarding DKA prevention and sick day/high blood glucose guidelines. Diabetes educators and clinicians need to modify their education and guidelines provided to pump patients wearing a CGM to include the incorportation of CGM data in DKA prevention. Adolescents and those with higher A1C levels who utlize diabetes technology especially could benefit from more education on DKA prevention. With such education, pump therapy can potentially be an even safer, effective therapy for youth with T1DM.