
Abstract
Purpose:
The purpose of this study is to compare the benefits of a diabetes self-management program led by registered nurses (RNs) versus community health workers (promotores) for Spanish-speaking Mexican Americans with type 2 diabetes (T2DM).
Methods:
Three hundred thirty Spanish-speaking Mexican American adults with T2DM were randomly assigned to “Tomando Control de Su Diabetes” delivered for six 2.5-hour sessions either by promotores or RNs. The primary outcome measure was the Summary of Diabetes Self-Care Activities (SDSCA). Evaluations were made at baseline, 6 weeks, and at 3, 6, and 12 months. Mixed-effects regression models were fit to test if participants had differential changes in the SDSCA total score by group over time, controlling for demographic and clinical factors.
Results:
SDSCA scores were significantly higher at all time points compared to baseline and not statistically different between the 2 groups. Only years of education correlated with improvement in diabetes self-management behaviors. No moderating variables predicted improvement between groups.
Conclusions:
Spanish-speaking Mexican American adults with T2DM who participated in a diabetes educational program with promotores or RNs demonstrated similar improvements. Promotores may increase the accessibility of effective diabetes self-management training for this difficult-to-reach population.
At over 53 million people and constituting 17% of the population, the Latinx population is the largest minority group in the United States, with those of Mexican origin comprising about 65% of this total. 1 Despite having the lowest median age of any racial/ethnic group in the United States, Mexican Americans are overrepresented in their incidence and prevalence of several chronic medical diseases. For example, the rate of type 2 diabetes among Mexican Americans is 16.3%, about twice that of non-Hispanic Whites. 2 Moreover, compared to non-Hispanic Whites, Mexican Americans tend to be diagnosed with type 2 diabetes at younger ages and exhibit higher blood glucose levels; lower insulin sensitivity; higher rates of diabetes complications, including retinopathy, neuropathy, and cardiovascular disease; and a life span shortened by 10 years.2-4
Interventions can improve health outcomes among Mexican Americans with type 2 diabetes. Although genetic predisposition can partially explain the high rates of morbidity and mortality associated with type 2 diabetes among Mexican Americans, 5 many modifiable environmental factors, such as sedentary lifestyle, unhealthy diet, low health literacy, and difficulty accessing health care, play an important role. 6 Over the past 15 years, several diabetes self-management education (DSME) approaches have been developed and shown to improve diabetes self-management behaviors and glycemic control and other health outcomes for Spanish-speaking Latinx with type 2 diabetes.7-12 These approaches share several features: community involvement, face-to-face encounters, ongoing participation of a multidisciplinary treatment team, targeting the development of skills to promote behavior change, the provision of prompts and reminders, the use of a prior needs assessment to inform intervention design, and an explicit focus on social-contextual issues.13,14 A recent meta-analysis examining the effect of culturally tailored diabetes education in ethnic minorities showed that these interventions were effective for improving diabetes self-management behaviors and glycemic control. 15 These findings are consistent with a recent Cochrane review, 16 which concluded that “culturally appropriate health education should be the ‘gold standard’ for health education programs targeted at ethnic minority communities.”
While each of these evidence-based DSME approaches has demonstrated advantages over usual care in Mexican American communities, these interventions differ in their format (individual vs group), the type of provider used to deliver the DSME intervention (health professional vs lay community health worker or promotore), and treatment target (patient vs patient and family). To date, there is little research to guide health practitioners regarding which interventions to apply and when so that resources are used efficiently and treatment outcomes are maximized. Moreover, little is known about which aspects of a culturally tailored DSME makes a difference toward improving the diabetes self-management behaviors and health outcomes of Mexican Americans. An additional gap in the literature stems from the finding that fewer than 40% of subjects offered these treatments achieved levels of A1C in accordance with the standards established by the American Diabetes Association. 6 Identifying nonresponding patients early in the treatment process and implementing more culturally appropriate approaches could forestall long-term adverse consequences.
Several of the culturally appropriate educational and management strategies developed and implemented to address the specific needs of the Mexican American population originally were designed to use registered nurses (RNs), certified diabetes educators, or dietitians as the primary patient educators.9,11,12 The limited availability of such specialized providers in general and bilingual or bicultural providers in particular prompted many DSME interventions to use promotores to handle group educational and skill reinforcement sessions as adjuncts to the primary educators. As such, the promotore functioned as a liaison between the underserved population and the formal medical system, complementing the health services rendered by more formally trained personnel. In some programs, the role of the promotore was modified such that the promotore became the principal diabetes health educator, thus replacing highly educated personnel, such as RNs, for patient education and long-term case management.17-23
Although the role of the promotore as the sole diabetes educator has its supporters17,18 and other evidence for its efficacy11,12,24 and quality 25 is available, some researchers have suggested that having promotores lead intervention sessions is less effective 23 and not acceptable to all Mexican Americans with type 2 diabetes 6 ; patients in these studies expressed a strong preference for a health care professional, most often, a nurse. Given the central role and respect these patients, and Hispanic communities in general, accord to nurses, 6 it is not surprising that the integration of nurses into a DSME program has repeatedly been found to be beneficial.25,26 However, no study to date, with Hispanic or any other population, has compared similar DSME interventions delivered by a community health worker (ie, a promotore) versus a health care professional such as an RN.
Hypothesis
Our study hypothesis was that subjects randomly assigned to RN-led groups would show greater increases in diabetes self-management behaviors than those assigned to promotore-led groups.
Research Design and Methods
Design
As the first phase of a large project designed to construct an adaptive intervention to determine which treatment strategies work to improve diabetes self-management behaviors most efficiently for Mexican Americans with type 2 diabetes, 27 a prospective, randomized controlled, repeated measures design was employed to compare the intervention effects between: (1) an RN-led group that received an evidence-based, DSME program and (2) a promotore-led group that received the same program. After study procedures were thoroughly described by the research coordinator, all patients provided informed consent in Spanish. This was followed by (1:1) assignment to either of the 2 intervention groups using a computer-generated randomization schedule. The investigators, participants, and group leaders were not blinded to group assignment. Recruitment materials, study protocol, and consent documents were approved by the Olive View-UCLA Educational and Research Institute and the David Geffen School of Medicine at UCLA’s Institutional Review Board.
Setting
The study site was Olive View-UCLA Medical Center (OVMC), a safety-net hospital located in the northern part of Los Angeles County and operated by the county’s Department of Health Services. OVMC is a full-service teaching hospital affiliated with the David Geffen School of Medicine at UCLA. OVMC has a primary care outpatient clinic that provides treatment to over 9000 patients with type 2 diabetes per year, including more than 4000 who are Spanish-speaking and of Mexican origin. All patients at OVMC are under the care of a medical home, which includes full- and part-time staff comprised of primary care physicians, residents, interns and medical students, nurses, and nursing assistants.
Study Sample
The sample size determination was based on conservative estimates for the primary outcome in the parent study, change in diabetes self-management behaviors over time. 27 After adjusting upward by 10% to account for expected attrition, the final sample size of 330 subjects was established. This would provide 80% power to detect a treatment group (RN-led vs promotore-led group) by time (baseline; 1.5, 3, 6, and 12 months) interaction corresponding to a change from no difference at baseline to a difference of d = 0.3 at study end. Eligible patients were required to be active clinic clients, 18 to 75 years of age, diagnosed with type 2 diabetes treated with oral agents or insulin, and with a baseline A1C of at least 7.0%. Of those subjects invited to participate, 82% accepted study participation (see Figure 1 for CONSORT diagram). Baseline assessments were completed by 100% of study subjects. Participants were enrolled from March 2017 through September 2020. Follow -up assessments were completed in September 2021.
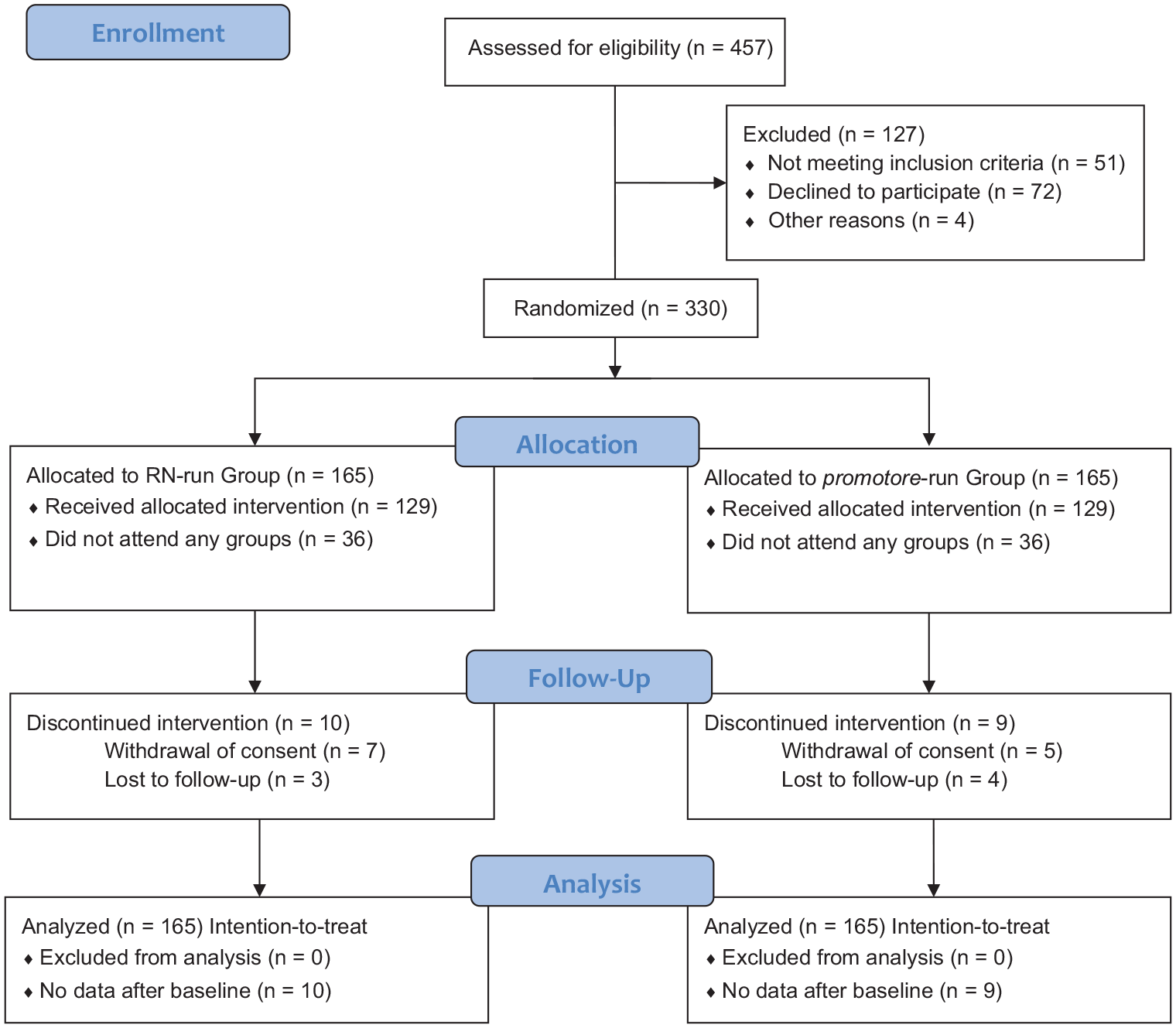
CONSORT flow diagram.
Description of Interventions
The study intervention, called “Taking Control of your Diabetes,” or in Spanish, “Tomando Control de su diabetes,” is based on the Stanford School of Medicine’s Chronic Disease Management Program developed by Lorig et al. 28 This program was culturally tailored for a Mexican American population 29 and demonstrated to improve glycemic control in a randomized controlled trial of over 500 Spanish-speaking adults with type 2 diabetes. 30 The program consists of 6 biweekly sessions lasting 2.5 hours each and led by 2 to 3 trained promotores (promotore-led group) or RNs (RN-led group). All promotores and RNs who took part in this protocol were bilingual and bicultural. Each session includes 10 to 12 patients. Each participant received a copy of the companion book, an audio relaxation tape, and an audio exercise tape with a booklet to supplement the material covered during the workshop sessions. Participants received instruction on how to eat a healthy diet, engage in appropriate physical activity, communicate effectively, and use medications properly. The following topics were covered in sessions: (1) techniques to deal with the symptoms of diabetes and associated condition, (2) appropriate exercise, (3) healthy eating, (4) correct use of diabetes medications, and (5) working more effectively with health care providers in a collaborative partnership. Patients were expected to make weekly action plans, share experiences, and help each other solve problems they encountered in creating and carrying out their self-management strategies. The classes were highly participative and allowed participants to show mutual support and develop confidence in their abilities to manage their health. Each of the group leaders attended a 4-day seminar led by the originators of the Stanford program, successfully completed a course certification exam, and demonstrated 100% fidelity to the model during several observation sessions. The same program content was delivered in each group, with the only difference being the type of group leader: promotore versus RN. Subjects were not paid for their participation in the groups, but all subjects were given token cash incentives in the amount of $10.00 for each completed assessment session. Transportation was arranged as needed for the participants.
Study Measures
At baseline, data were collected from subjects on demographic characteristics, including age, sex (male/female), marital status (never married, married, divorced, widowed, separated), employment status (full-time, part-time, homemaker, retired, disabled, unemployed), educational level (years of schooling), and clinical variables, including the presence of symptoms of psychosis, depression, anxiety, bipolar disorder, alcohol use disorder, and substance use disorders (measured as yes/no responses).
In addition, data on the Summary of Diabetes Self-Care Activities Measure (SDSCA) survey instrument was collected at baseline, 3 months, 6 months, and 12 months. The SDSCA is a well-validated instrument most frequently used for assessing the acquisition of diabetes self-management behaviors.31,32 The SDSCA is formatted to ask on how many of the previous 7 days the individual performed recommended self-management activities: eating healthy foods, following a diabetic diet, engaging in physical activity, self-monitoring of glucose, taking prescribed hypoglycemic medications, and caring for one’s feet. A weekly self-care score ranging from 0 to 7 is generated, with higher scores corresponding to greater number of days. The SDSCA has excellent psychometric properties in several languages, including Spanish.33,34
Statistical Data Analysis
Continuous data were summarized by means and standard deviations for continuous outcomes, while frequency and percentages were used for categorical variables. To test if participants had differential changes in their outcome over the study period by group (ie, RN vs promotore), we used mixed-effects regression models that controlled for participants’ demographic characteristics and clinical factors. Data were collected across 5 time points (baseline; 1.5, 3, 6, and 12 months) nested within individuals. Models were fit for the outcome using MIXED procedure in SAS with the intercept specified as random effect and within-subject residuals specified to have autoregressive structure of degree 1. Model fit and comparisons were conducted using log likelihood test, Akaike information criterion and Bayesian information criterion to select the “best” model. The statistical software SAS version 9.4 was used for the analyses, and P < .05 was considered as statistically significant.
The data sets generated during and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Results
Baseline Characteristics
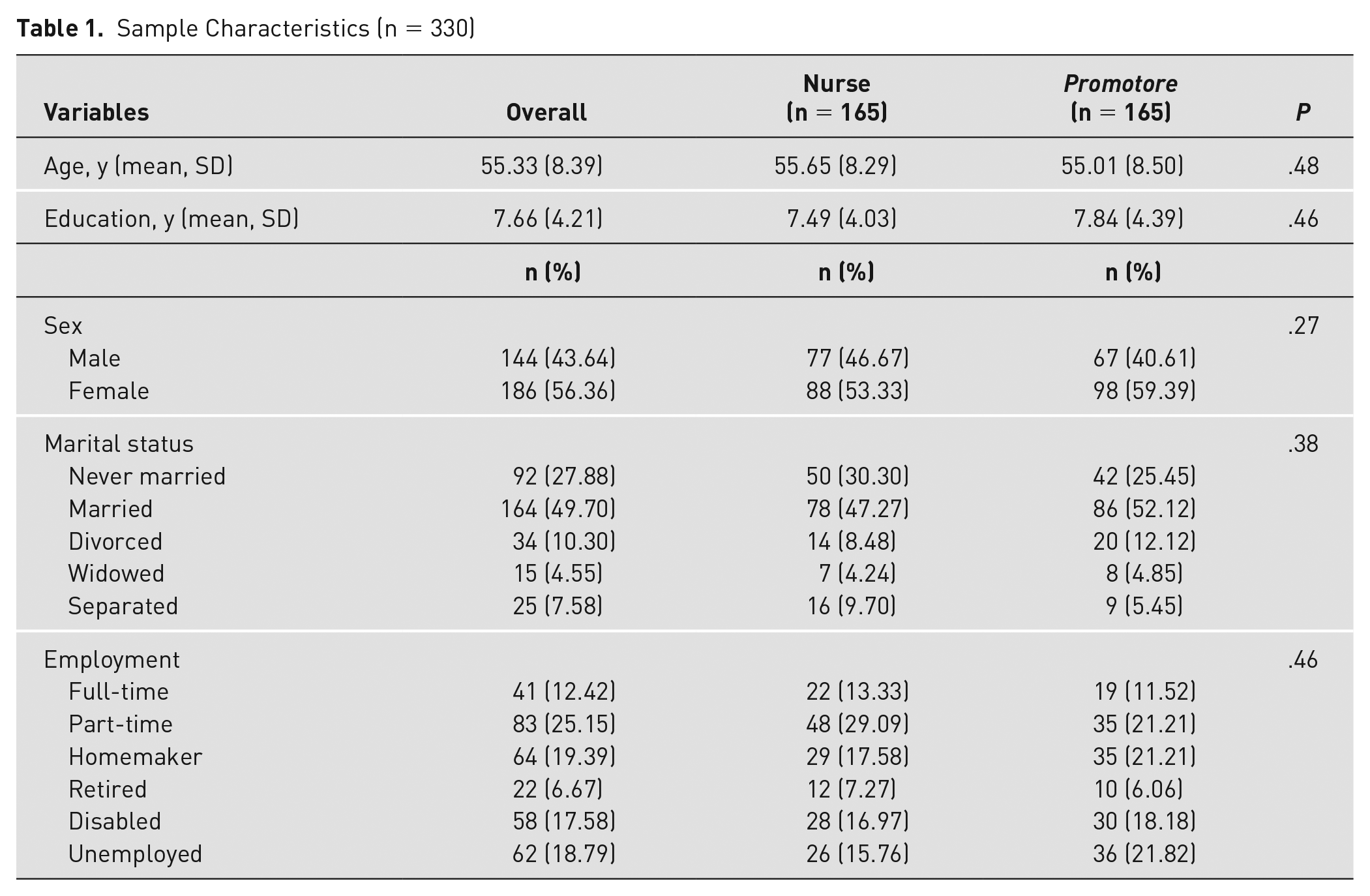
Average age in the sample was 55 years (SD = 8.39). More than half of the sample were females (n = 186, 56.4%), and half were married (n = 164, 49.7%). A third of the sample reported depression disorder (n = 105, 32.1%); few reported alcohol use disorder (n = 29, 8.84%), anxiety disorder (n = 11, 3.35%), and substance use disorder (n = 8, 2.44%); and no one reported psychotic or bipolar disorders. Details can be found in Table 1.
Sample Characteristics (n = 330)
To assess the behavior of SDSCA over the study period, linear mixed-effects models were fit (Table 2). Intraclass correlation coefficient computed from the unconditional random intercept model (Model 1) indicated that 32% of the variation in SDSCA scores was at the individual level (ie, individual differences in mean SDSCA over time) and that the remainder was within-individual variation across time. Model 2 (Table 2) was built by adding time (as a categorical variable because time intervals were not equal) and group assignment (RN vs promotore) to Model 1. Compared to baseline, there were significant increases in the outcome across all time points. However, there was no statistical difference in the outcome between the 2 groups. A random slope was incorporated into Model 2 to get Model 3 (Table 2). The model fit was worse, so we went back to Model 2 and added various demographic and clinical variables as fixed effects to obtain Model 4 (Table 2). We assessed adding interaction terms between group assignment and time and group with other variables, but model fit did not improve. So, based on model fit and parsimony, Model 4 was the final model of choice. In the final model, it was found that the outcome was (a) significantly higher (improved) at all time points compared to baseline (all Ps < .0001), (b) not statistically different between the 2 groups (P = .34), (c) 0.44 units higher for every unit increase in the number of sessions attended (P = .02), and (d) 0.38 units higher for every year increase in education (P = .001), controlling for all other variables in the model. The mean SDSCA scores by group over time can be found graphically in Figure 2.
Parameter Estimates and Model Comparisons for Longitudinal Models of SDSCA Scores a
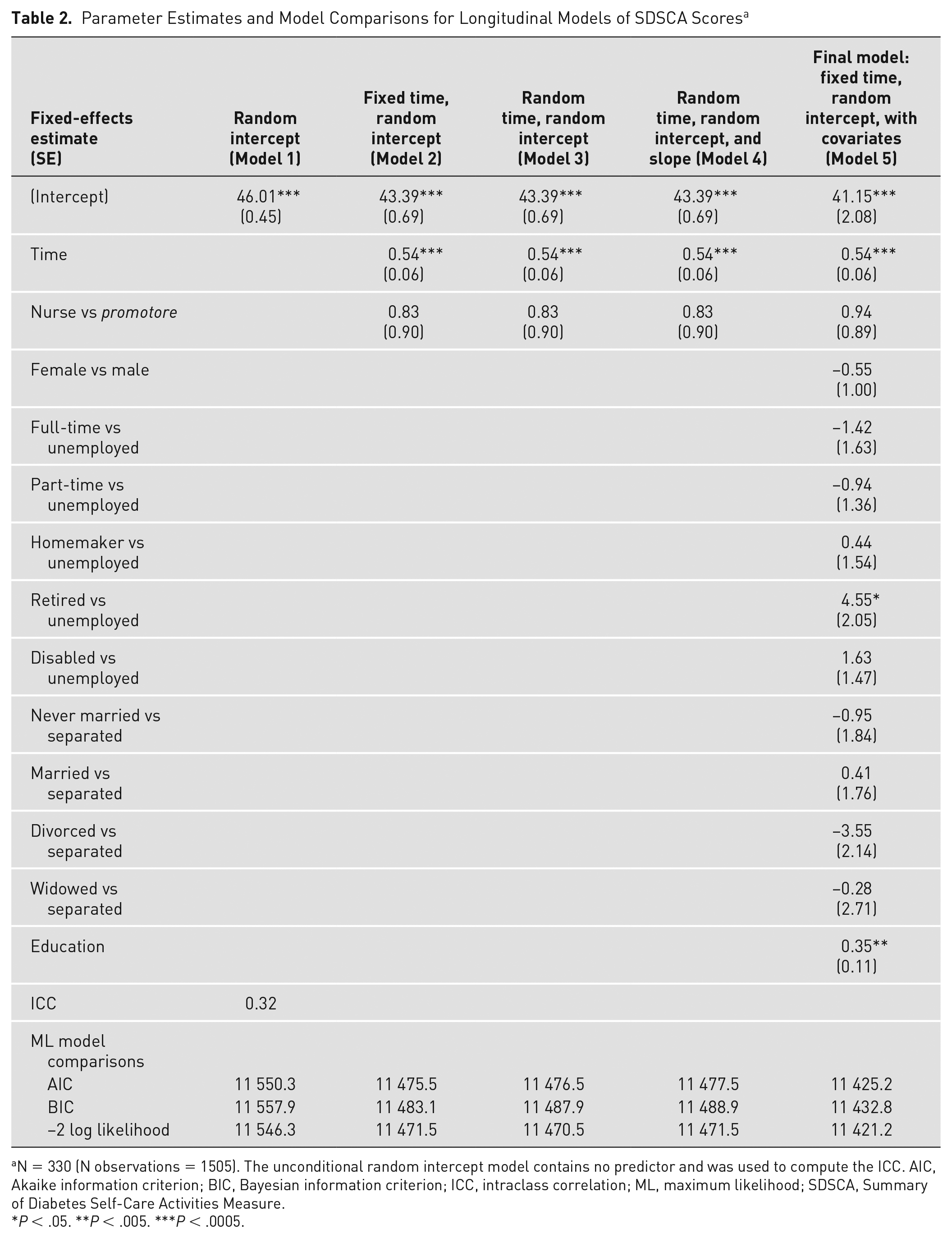
N = 330 (N observations = 1505). The unconditional random intercept model contains no predictor and was used to compute the ICC. AIC, Akaike information criterion; BIC, Bayesian information criterion; ICC, intraclass correlation; ML, maximum likelihood; SDSCA, Summary of Diabetes Self-Care Activities Measure.
P < .05. **P < .005. ***P < .0005.
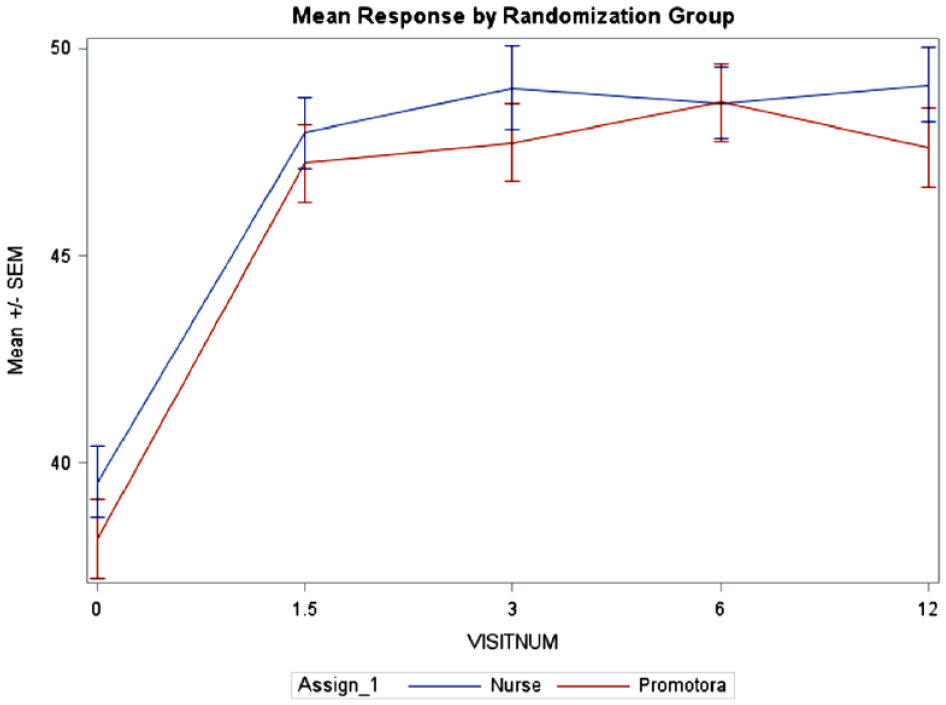
Mean SDSCA scores over time by group.
Discussion
In this large (N = 330) study within a safety-net population, we found that Spanish-speaking Latinx adults with type 2 diabetes who participated in the Tomando Control de su Diabetes program demonstrated significant increases in their diabetes self-management behaviors. While previous tests of this program have yielded improvements in diabetes knowledge and health benefits such as reductions in A1C levels,29,30 this is the first study of Tomando Control to find a statistically significant effect on the direct target of the DSME intervention, namely, diabetes self-management behaviors. On average, study subjects increased their use of self-management behaviors by more than 22%, which corresponds to their engaging in these salutary activities 1.5 days more per week than they had at baseline. Perhaps most importantly, subjects maintained these behaviors over the course of 1 year with almost no dropoff in performance despite the relatively brief duration of the intervention (ie, 6 sessions over 12 weeks).
This study also represents the first head-to-head comparison of an evidence-based DSME program conducted by RNs versus community health workers, or promotores. We found that there was no difference in the use of diabetes self-management behaviors between subjects who were in groups led by either type of instructor. This finding was contrary to our study hypothesis given that we expected RNs to be more highly skilled and thus better able to teach the material more effectively. Moreover, no moderating variables (eg, gender, age, level of education) differentially predicted improvement between instructor types. One explanation for our results is that all the RNs and promotores who participated in this study were exceptionally well trained, having completed a rigorous 4-day workshop on the Chronic Disease Self-Management and Tomando Control programs conducted by its developers at Stanford University, were certified by the developer’s own Self-Management Resource Center,and demonstrated consistent fidelity to the model. 35 The material taught in the Tomando Control workbook is extremely proscriptive and straightforward, which may contribute to its effective use by lay health instructors such as the promotores who served as instructors in this project. As further support for the central role of the Tomando Control curriculum (as opposed to the educational level of the presenter), we found that the number of sessions attended by the subjects, that is, their exposure to the learning material, significantly predicted improvements in diabetes self-management behaviors. The importance of this finding is that the availability of DSME materials that does not require specially trained RNs may facilitate wider utilization of this evidence-based modality and thus increase access to a larger number of patients.
The only moderating variable that did predict diabetes self-management behaviors after the intervention was level of education. In both the nurses’ and promotores’ groups, participants with higher levels of education demonstrated greater increases in diabetes self-management behaviors. For every additional year of education, participants improved their SDSCA score by 0.38 units, which corresponds to a moderately large effect size. 36 This finding suggests that while Tomando Control is clearly a culturally relevant DSME program that addresses the learning needs of many Spanish-speaking Mexican Americans with type 2 diabetes, alternative approaches may be required for patients who do not benefit from standard DSME programs. We are testing an intervention that augments Tomando Control with a multifamily group approach designed to overcome obstacles to the incorporation of diabetes self-management behaviors into everyday activities. 27
This study has several limitations. First, subjects were not blind to their treatment condition because instructors introduced themselves to the participants as either RNs or promotores. However, it is unlikely that this information impacted on the testing of the study’s hypothesis. Second, the primary outcome measure, diabetes self-management behaviors, was based on self-report. Although subjects may misrepresent their performance of self-management activities such as healthy eating and engaging in physical exercise, the SDSCA is a well-validated instrument that has demonstrated high correlation with physiologic measures such as A1C. 33 Third, we did not include more objective measures of diabetes control (BMI, A1C levels, etc) in this study because our focus was strictly on improving behavioral parameters.
Conclusion
We tested the Tomando Control program as part of an effort to determine how best to help Latinx adults with type 2 diabetes improve their illness self-management skills. We found that the Tomando Control program was equally effective in increasing diabetes self-management behaviors among Spanish-speaking Mexican American adults receiving treatment at a safety-net health system when taught by either RNs or promotores. While the use of promotores as frontline diabetes educators can be problematic given the challenging aspects of the material to be learned, the results of this study support the effort to increase the use of well-trained, bilingual, and bicultural promotores in the diabetes education enterprise. Such efforts could greatly increase the availability of this evidence-based practice to a large and growing population of Spanish-speaking Latinx adults with type 2 diabetes.
Footnotes
Acknowledgements
The authors thank the patients who volunteered to participate in this study and the registered nurses and promotores who delivered the intervention (Guadalupe Alcaraz, Alicia Barajas, Jose Buenrostro, Justina Otarola, Sophia Zagon, and Alicia Zuniga). Trial Registration: NCT03092063. All items from the Clinical Trials Registry are available at https://register.clinicaltrials.gov/prs/app/action/SelectProtocol?sid=S0006ZCJ&selectaction=Edit&uid=U00012VO&ts=2&cx=t4ejs5.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
Research reported in this publication was supported by the National Institute of Nursing Research of the National Institutes of Health under award No. R01-NR015809.
Prior Presentation
The study described in this manuscript was presented in part at the 55th Annual Convention of the Association for Behavioral and Cognitive Therapies, via Zoom, on November 19, 2021.