
Abstract
Purpose:
The purpose was to determine if negative or stigmatizing language and messaging have an impact on diabetes distress, outcomes, or care behaviors in people with diabetes. Since 2012, when the first language position statement was published, the way health care professionals talk to people with diabetes has been an ongoing topic of discussion. However, there have been no recent literature reviews evaluating the impact of problem language on outcomes among people with type 1 and type 2 diabetes.
Methods:
An integrative review was conducted using 4 electronic databases: CINAHL, Embase, Web of Science, and Medline (Ovid). Studies reporting on diabetes, language, stigma, diabetes distress, glycemic outcomes, and self-care behaviors were included.
Results:
The review included 9 studies, all of which were of high quality. The impact of negative or stigmatizing language on self-care behaviors was the most commonly addressed outcome. Whereas some studies revealed no change, others reported a decrease in self-care behaviors by people with diabetes who had negative perceptions of provider messages. Actual or perceived use of negative or stigmatizing language is linked to higher A1C. Four studies reported an association between messages and diabetes distress.
Conclusions:
Negative/stigmatizing language has both an immediate and long-term effect on people with diabetes. The inconsistent approaches to studying language in diabetes makes it challenging to compare outcomes and identify themes. Future research is needed to identify effective interventions to change the messages in diabetes.
The way health care professionals (HCPs) talk to and about people with diabetes (PWD) is an important topic that is getting more and more attention. In 2012, the first language position statement was published by Diabetes Australia, 1 and several more language guidelines publications have followed over the past decade.2 -5 Words and messages have potential to inspire PWD to engage in disease management or, conversely, feel defeated and give up. 6
Findings from the landmark DAWN studies established that PWD want the emotional side of diabetes to be acknowledged by HCPs and that HCPs want and need a better understanding of emotional problems and diabetes distress.7,8 In fact, one of the goals identified from the findings of the DAWN study was to “enhance communications between PWD and HCPs.” 7
At least 1 focus group study 9 and 2 survey studies10,11 have found that PWD feel that many of the words and messages used in diabetes care are problematic. To date, no large intervention trials have been conducted to find ways to mitigate the problem.
The DAWN2 study revealed that 61.4% to 92.9% of HCPs thought PWD needed to improve self-management activities. Meanwhile, less than one quarter of respondents reported being asked by HCPs how diabetes impacts their life. 12 Diabetes distress leads to decreased self-management, which leads to negative glycemic outcomes and increased complications, 13 and in DAWN2, 44.6% of participants reported high diabetes distress. In addition, participants rated the availability of person-centered care as low. 12
Stigma
People with diabetes report that stigma is a very real concern and has an impact on many aspects of their lives. 14 Stigma has been defined as a distinguishing, labeling, and categorizing of people according to their differences. It also involves linking those categories to negative stereotypes. 15 Liu et al 16 found that being perceived as having a character flaw or a failure of personal responsibility was the most widely reported experience of diabetes stigma. This was followed by being perceived as a burden on the health care system. Although stigma can manifest through body language, such as “looks of contempt,” 16 most often, stigma is communicated through words.
Diabetes Distress
Diabetes distress is a “generic term that captures the primary sources and intensity of emotional distress associated with diabetes and its management over time.” 17 Diabetes distress involves the fears, concerns, and worries individuals with diabetes experience from living with a demanding disease. 18 Diabetes distress has been negatively associated with both glycemic outcomes 17 and self-care behaviors. 19
Glycemic Outcomes
Diabetes management requires a daily effort to achieve and maintain glucose levels in a safe range. A1C < 7% has been a standard glycemic target for decades, 20 and more recently, HCPs are using time in range as a substitute or additional glucose target. 21 In research reports, “glycemic control” is often used as a convenient catchall to mean glycemic outcomes. People with diabetes have shared that this term is not helpful and even potentially harmful to their diabetes management.9,11
Diabetes Self-Care Behaviors
Diabetes self-management comprises the tasks and health behaviors PWD engage in to manage glucose levels in an attempt to avoid or delay chronic complications associated with diabetes. These self-care behaviors, referred to as the ADCES7, include healthy coping, healthy eating, being active, taking medications, monitoring, reducing risk, and problem solving. 22 In addition to the ADCES7, PWD are responsible for scheduling and getting themselves to multiple appointments; getting prescriptions for, purchasing, and storing medications; identifying and treating acute complications, such as hypoglycemia; and carrying necessary supplies at all times.
Language and messages that address or discuss PWD can not only influence diabetes distress, but they may also affect how PWD engage in diabetes self-management. Messages can create or promote stigma and can influence glycemic outcomes. Each of these are concerning in and of themselves, and when combined, the effect that language can have may be detrimental. The ADCES7 framework guides the work of diabetes care and education specialists; therefore, understanding the impact of language and messages on diabetes self-care behaviors is critical to effective practice. Until now, it has been largely unknown what research has been conducted on the impact of negative, stigmatizing words and messages on diabetes distress, glycemic outcomes, and diabetes self-care behaviors. The purpose of this integrative review, therefore, was to answer the following research question: Does negative or stigmatizing language and messaging have an impact on diabetes distress, glycemic outcomes, or self-care behaviors in people with diabetes?
Research Design and Methods
Search Strategy
To determine if negative or stigmatizing language has an impact on diabetes distress, glycemic outcomes, or self-care behaviors in PWD, the authors conducted an integrative review. 23 The research team selected the terms and their derivations for diabetes, language, stigma, patient, clinical, and communication; a medical science librarian conducted a search using CINAHL, Embase, Web of Science, and Medline (Ovid) databases. The review was registered with the National Institute for Health Research, International Prospective Register of Systematic Reviews, registration number 322670.
To be included in this review, articles needed to address diabetes (type 1 diabetes [T1DM], type 2 diabetes [T2DM], or gestational diabetes mellitus [GDM]), report on quantitative research findings, be available in English, and have been published between January 2013 and March 2023. Systematic and scoping reviews were excluded, as were articles not in English or focused on language barriers (e.g., English as a second language) or cultural competence, case studies, research protocols, or qualitative research. Qualitative studies were excluded because they cannot answer the research question.
Screening
All of the identified records were uploaded into the Covidence platform, 24 where duplicate articles were removed. Covidence streamlines the production of literature reviews through web-based collaboration software. This software helps authors manage the review process through prompts and reminders. Initial screening of titles and abstracts was performed by the 4 authors; 2 authors reviewed each article, and a third author resolved any conflicts.
After articles meeting criteria were identified, the process of data extraction began. Data were extracted from each article for the following criteria: author, year of publication, location of study, study design, overall study objective, and sample size and characteristics. For the language variable, source of language/stigmatization, measurements and instruments, and findings were extracted (Table 1).
Characteristics of Included Studies
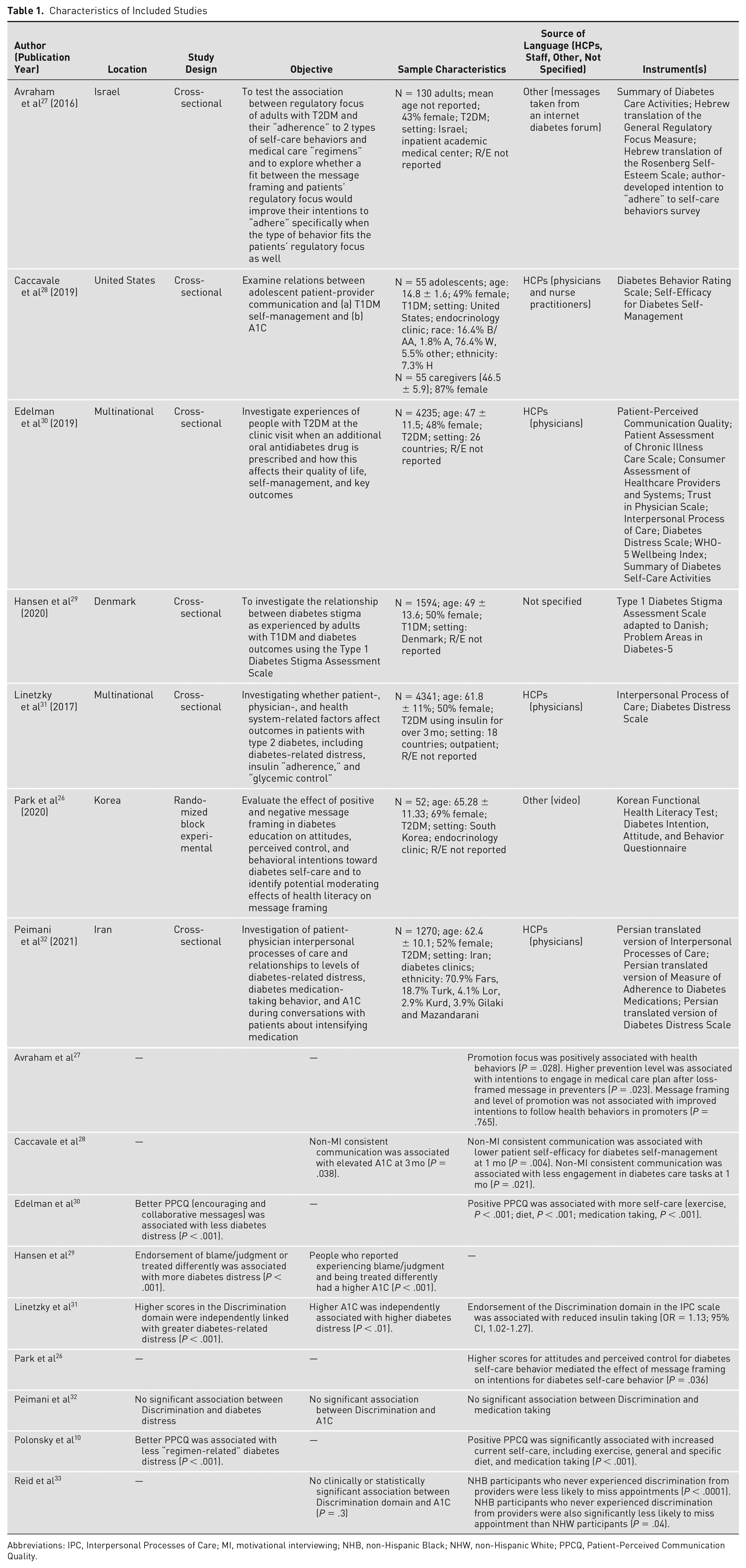
Abbreviations: A, Asian; B/AA, Black/African American; H, Hispanic; HCP, health care professional; R/E, race/ethnicity; T1DM, type 1 diabetes; T2DM, type 2 diabetes; W, White.
Data extraction was further refined to focus on outcome variables: diabetes distress, glycemic outcomes, and self-care behaviors. The goal was to determine relationships between provider communication and the outcomes variables (Table 2).
Target Outcome Variables of Included Studies
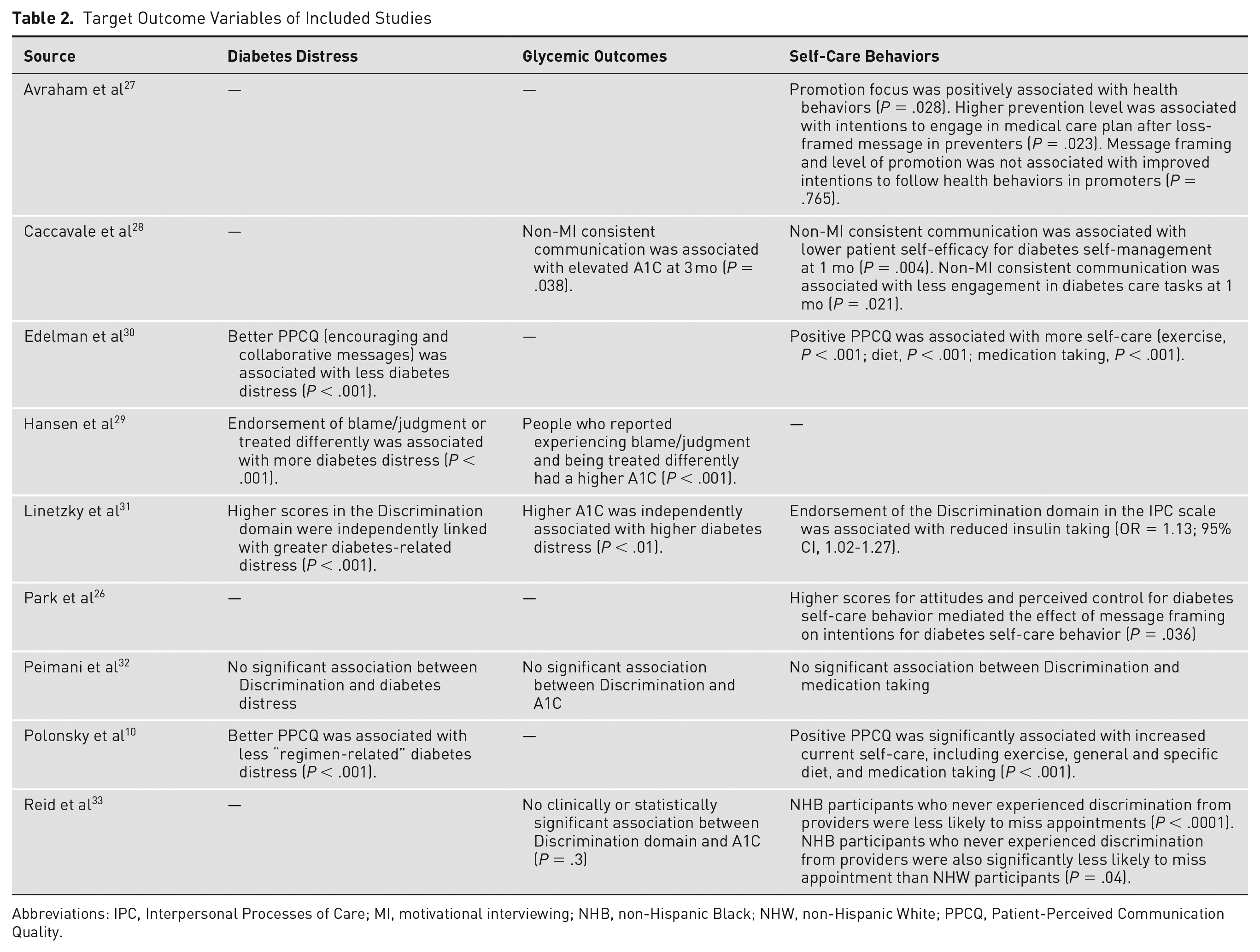
Abbreviations: IPC, Interpersonal Processes of Care; MI, motivational interviewing; NHB, non-Hispanic Black; NHW, non-Hispanic White; PPCQ, Patient-Perceived Communication Quality.
Quality Appraisal
The research team employed the Joanna Briggs Institute (JBI) critical appraisal tools 25 to assess the trustworthiness, relevance, and results of included articles. Each study was scored on the JBI questions (1 = yes, 0 = no, UC = unclear [unscored]; Table 3). All individual scores were summed and then divided by the number of items scored for a total quality score. Total scores >80% were considered high quality.
Quality Assessment Using Critical Appraisal Tools Adapted from Joanna Briggs Institute a
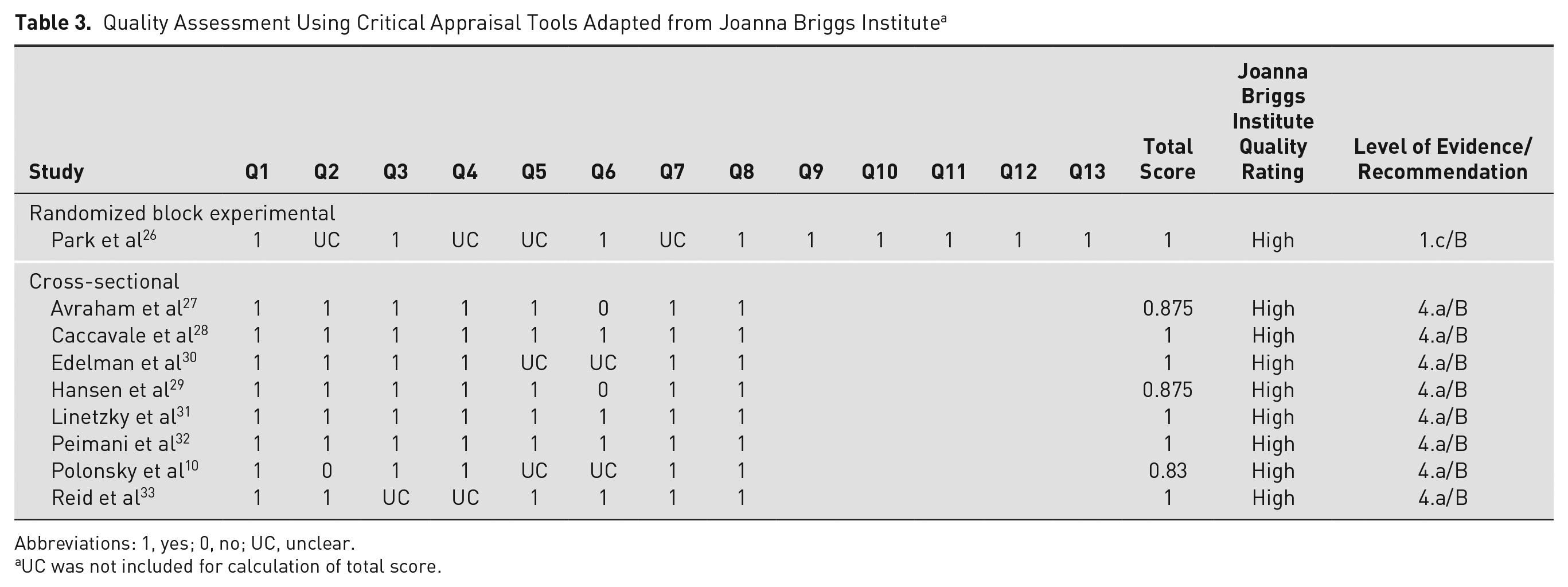
Abbreviations: 1, yes; 0, no; UC, unclear.
UC was not included for calculation of total score.
Of the 9 studies included, 1 was a randomized block experimental, 26 and 8 were cross-sectional.10,27 -33 Using the JBI levels of evidence and recommendations, 1 study received a level of evidence of 1.c, and the others were 4.a. All 9 studies were given a grade B, indicating a weak recommendation. All of the studies met high quality thresholds,10,26 -33 (Table 3).
Results
Characteristics of Included Studies
A total of 1993 journal articles meeting search criteria were imported into Covidence. After screening for title and abstract, 32 articles were retained for full text review. Nine articles were included in the integrative review10,26 -33 (Figure 1).
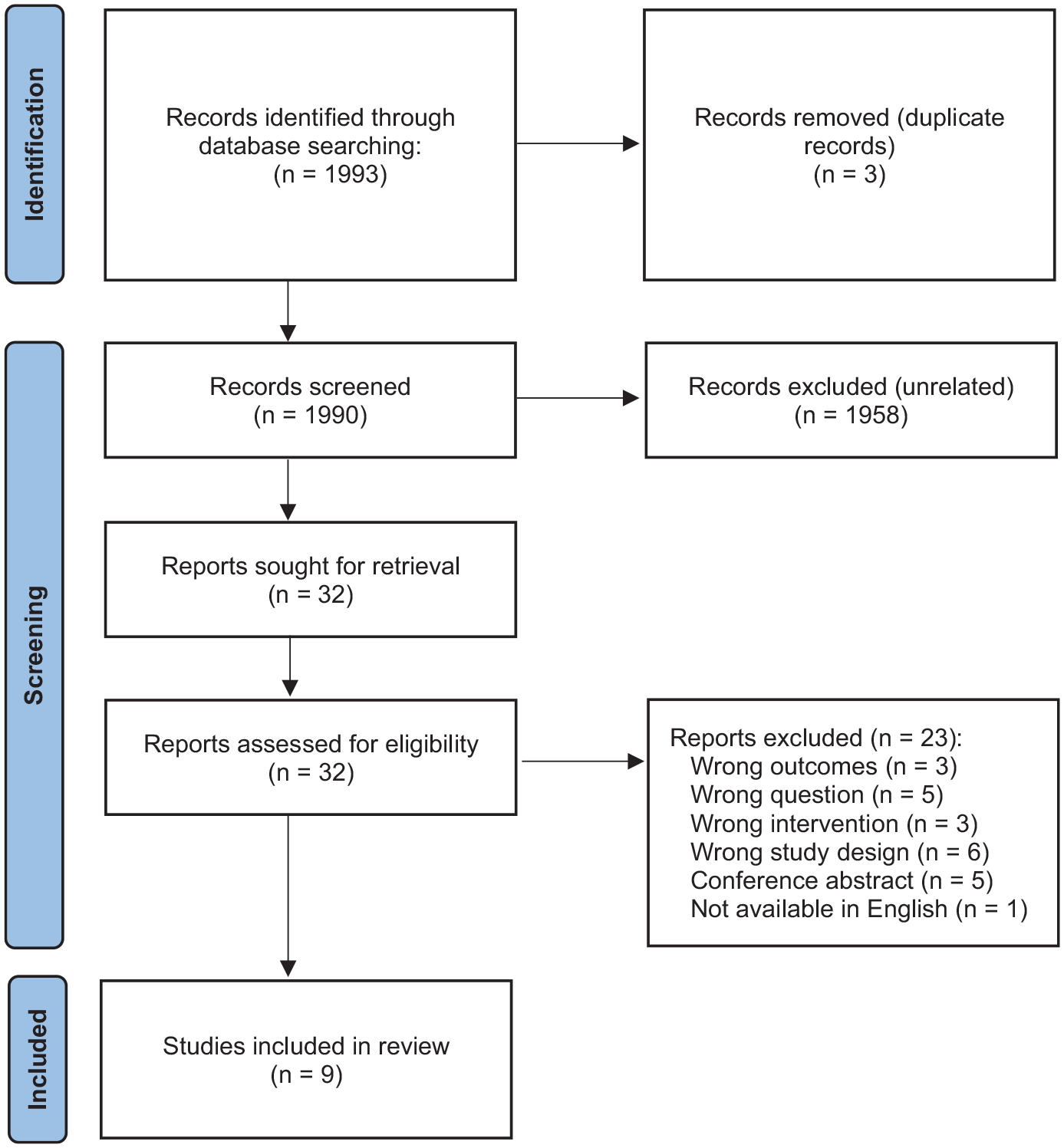
PRISMA 2020 flow diagram including databases and registers.
Included articles were published between 2016 and 2021. The reviewed studies were conducted in 5 countries (Denmark, United States, Iran, Israel, Korea), and 3 were multinational studies.10,30,31 The number of participants in the included studies ranged from 52 to over 4000 (for the multinational studies), with a total of 15 586 participants across the 9 studies. The average age of participants was 51.26 years. Only 1 study included adolescents. 28 Seven studies included participants living with T2DM,10,26,27,30 -33 whereas 2 examined participants living with T1DM.28,29 A single study examined race associated with stigmatizing language. 33
A variety of recruitment methods were used: health record review after hospitalization, email, recruitment of health care professionals at division meetings, letters to eligible clients, and direct request from physicians. Communication/messaging being evaluated in the studies was delivered by health care professionals, office staff, and messages that participants read or watched on videos (see Table 1).
Outcomes-Related Findings of Included Studies
Diabetes distress
Five studies looked at diabetes distress.10,29 -32 Two of these studies identified that positive communication during diagnosis and when an additional oral glucose-lowering agent was prescribed was associated with less diabetes distress.10,30 Greater diabetes distress was associated with negative communication in 2 studies.29,31 Peimani et al, 32 on the other hand, did not find an association between participants feeling discriminated against by their health care professional and diabetes distress.
Glycemic outcomes
Five studies examined glycemic outcomes with respect to clinician-patient relationship and found that negative messages resulted in anywhere from no change32,33 to increased A1C.28,29,31
Self-care behaviors
Eight studies examined self-care behaviors, including food choices,10,28,30 exercise,10,28,30 medication taking,10,28,30 -32 and missed appointments. 33 Two studies revealed that negative communication reduced insulin-taking behaviors.28,31 Peimani et al 32 did not find a change between participants feeling discriminated against by their health care professional and medication-taking behavior. One study revealed that positive communication at the time of diagnosis had a positive impact on making healthy food choices, engaging in exercise, and taking medications. 10 Similarly, Edelman et al 30 found that when positive communication was used at the time of adding an oral glucose-lowering medication, participants reported a positive impact on food, exercise, and medication-related self-care behaviors. In contrast, Park et al 26 observed no change in diabetes self-care behavior intentions for those who watched negatively framed videos. Avraham et al 27 also found no relationship between message framing and intentions to follow health behaviors. Finally, non-Hispanic Black participants were less likely to miss an appointment when they did not experience “discrimination” from their health care professional. 33
Discussion
Findings from this integrative review are consistent with a systematic review that examined both quantitative and qualitative studies and found that patient-perceived communication quality may be an approach to improving outcomes for people with T2DM. 34 The current review examined more recent literature, included studies with participants who had T1DM, and focused on intervention studies.
Impact of Negative or Stigmatizing Language on Diabetes Distress
The existing studies addressing diabetes distress indicate that positive communication decreases diabetes distress10,30 and that perceived stigma and discrimination increase diabetes distress.29,31 These findings are consistent with those from a recent study by Holmes-Truscott et al, 35 who reported a positive association between diabetes stigma and diabetes distress. People experiencing more stigma reported increased diabetes distress. A common element of diabetes distress is “burnout,” 17 which may manifest as decreased self-care behaviors.
In a recent study, Dickinson et al 11 found that 87.9% of people with T1DM and 76.4% of people with T2DM reported feeling hopeless when HCPs use scare tactics. It is possible, although not yet studied, that when health care professionals use negative, judgmental language, they contribute to diabetes distress.
Impact of Negative or Stigmatizing Language on Glycemic Outcomes
Three of the 4 studies included in the review that addressed glycemic outcomes reported an association between negative or stigmatizing language and A1C.28,29,31 However, each of the authors used a different method to determine the presence of problem language. Hansen et al 29 employed surveys by which the participants self-reported feelings of blame, judgment, and being treated differently. Linetzky et al 31 used items from the Interpersonal Processes of Care Survey (IPC) to identify stigmatizing language based on “hurried communication” and “perceived discrimination.” Lastly, Caccavale et al 28 used “motivational interviewing non-adherent behaviors” to define negative/stigmatizing language. Despite these differences in the measurement of problem language, the findings revealed that actual or perceived use of negative or stigmatizing language is linked to higher A1C. These findings are consistent with those reported by Liu et al. 16 Of note, Liu et al 16 also reported that females with graduate or professional degrees reported increased perception of stigma.
Impact of Negative or Stigmatizing Language on Self-Care Behaviors
Most of the included studies (89%) addressed self-care behaviors. Of these, medication taking was the most addressed behavior, followed by food choices and exercise. In this review, overall findings showed that when communication was positive and patients did not feel discriminated against or stigmatized, there was an increase in self-care behaviors. This reinforces the findings from a study by Holmes-Truscott et al, 35 who reported a small association between stigma and dietary behaviors but not physical activity.
Strengths and Limitations
A strength of this integrative review is the inclusion of studies conducted among samples of people with T1DM and T2DM. Also, the impact of language was evaluated from the perspective of the patient and/or their parents (pediatrics).
However, there were several limitations to this review. First, although each of the studies explored some aspects of negative or stigmatizing language, the objectives of the studies were disparate. The authors sought to examine regulatory focus and self-care behaviors, 27 the association between patients’ perceptions of care and medication taking, 33 the impact of motivational interviewing, 28 the impact of adding an additional oral glucose-lowering agent on quality of life, 30 and messaging within diabetes education. 26 The differences in the objectives made it challenging to compare outcomes.
Another limitation was the lack of a standardized measure for stigma and diabetes distress. The Type 1 Diabetes Stigma Assessment Scale and the Problem Areas in Diabetes were used by Hansen et al. 29 Avraham et al 27 used the Rosenberg Self-Esteem Scale, and Edelman et al 30 used the WHO-5 Wellbeing Index. The Diabetes Distress Scale was used by Edelman et al, 30 Polonsky et al, 10 Peimani et al, 32 and Linetzky et al. 31 Several studies used the IPC.31 -33 Attention to self-care behaviors was also evaluated using a variety of different instruments: Extent of Adherence Survey, 33 Adherence to Prescribed Medications, 32 Summary of Diabetes Self-Care Activities, 27 and Self-Efficacy for Diabetes Self-Management measure. 28 Synthesizing the findings from each of these scales into a central “theme” was therefore challenging. Lastly, the sample size for the majority of the studies was small, and only 1 study included a pediatric sample. 28
Implications and Future Research
Findings from this review emphasize the need for intervention studies that examine the impact of using positive (person-centered, strengths-based, empowering) messages on diabetes distress, glycemic outcomes, and self-care behaviors in people living with diabetes. This review emphasizes the paucity of research focused on problem language and its effect on PWD. In particular, well-designed studies that examine the impact of negative or stigmatizing language on diabetes distress, glycemic outcomes, self-care behaviors, and other patient-reported outcomes among people with T1DM and T2DM across the life span are needed. These studies need to be conducted using a standardized tool for the assessment of diabetes distress and a framework for the assessment of diabetes self-care behaviors.
Future studies also need to take into account differences in patient and HCP perceptions. Often, people with diabetes have higher body weight, and the perception is that they developed diabetes as a result of lacking self-control, which implies that they “did this to themselves.” 36 Identifying and implementing methods by which to decrease stigmatizing messages addressed to and about PWD could, in turn, lead to less social stigma experienced by people with diabetes.37
During the review process, the research team noted that authors reporting studies on problem language in diabetes frequently used negative or stigmatizing language in their articles. Words most often seen in the diabetes language research include “glycemic control,” “adherence,” and “regimen,” all of which are listed as problem words in the language guidance paper jointly published by the American Diabetes Association and the Association of Diabetes Care & Education Specialists. 3 This alone indicates there is still work to do toward changing messages used in diabetes.
Conclusion
Findings from this review reinforce the need for additional studies, specifically using experimental designs, that focus on the impact of messages on diabetes outcomes. Findings from published studies show that people with diabetes often feel judged and blamed for living with a chronic disease. Negative messages from HCPs may convey or perpetuate stigma and lead to deleterious effects on self-care and other outcomes in PWD. Future research should focus on interventions that teach health care professionals about problem language and measure adoption of more effective communication and its impact on patient outcomes.