
Abstract
Purpose
The purpose of the study was to assess self-efficacy among adolescents with type 1 diabetes mellitus and to identify its contributing factors using a new measure based on the International Society for Pediatric and Adolescent Diabetes Guidelines: the Type 1 Diabetes Mellitus Self-Efficacy Scale (T1DM-SES).
Method
A descriptive, cross-sectional design was used to collect data from 161 adolescents ages between 12 and 18 via an online questionnaire survey, including demographic and management-related variables and the 21 items of T1DM-SES.
Results
Results demonstrated that adolescents had high self-efficacy levels regarding the basic needs to manage their diabetes and relatively moderate and low levels regarding more sophisticated needs, such as adjusting insulin dose to correct fluctuated glucose levels, covering carbohydrates, and managing ketoacidosis at home. Adolescent females and adolescents who have working mothers or caregivers demonstrated higher levels of self-efficacy, whereas adolescents who have another family member with T1DM reported lower levels.
Conclusion
Assessing adolescents’ self-efficacy using evidence-based measures is crucial for informing health education plans. There should be a greater focus on acquiring the advanced knowledge and skills necessary for adolescents to manage the constantly evolving challenges of diabetes management. Access to health care and sufficient health insurance coverage that encompasses modern technology are fundamental for the effective management of T1DM.
The incidence of type 1 diabetes mellitus (T1DM) has increased globally in recent decades. However, the exact causes remain unclear. Multiple factors have been linked to the likelihood of developing T1DM, such as early life infections, dietary composition, and perinatal influences. 1 In 2020, a meta-analysis of 193 studies showed that the prevalence of T1DM was 9.5%, and the incidence was 15 per 100 000 people. 2 In 2021, it was estimated that around 8.4 million individuals globally were living with T1DM, of which 18% (1.5 million) were younger than 20 years, with approximately 500 000 new cases reported that year. Predictions suggest that by 2040, the number of people living with T1DM could range between 13.5 million and 17.4 million. 3
In Jordan, the incidence of T1DM has progressively increased throughout the past few years. The incidence rate in 1992 through 1996 increased from 2.8 to 3.6 per 100 000 populations, where the maximum incidence was during the winter months. At that time, the incidence of T1DM among Jordanian children ages 0 to 14 years was among the lowest in the region, however, it continued to rise. 4 Later, in 2008, there was a 31.5% increase in the prevalence of both types of diabetes among Jordanians. 5 T1DM commonly develops during adolescence or early adulthood, although it can occur at any age. It arises when pancreatic β cells fail to produce insulin, often due to an autoimmune origin. This results in an elevated blood glucose level, requiring insulin therapy for management. Common manifestations include increased urination, thirst, and weight loss. The autoimmune process responsible for causing T1DM can also impact various other organs, leading to the development of further autoimmune conditions, such as autoimmune thyroid disorders and celiac disease, which can hinder the effective management of diabetes. 6 So, managing comorbidities is a considerably important aspect of self-efficacy among patients with T1DM. In Jordan, the prevalence of celiac disease among pediatric patients with T1DM is 9.1%, which is mainly diagnosed at the onset or during the first 5 years of diagnosis. 7 Moreover, diabetic ketoacidosis (DKA) may result from persistently high blood glucose levels, leading to cerebral edema. 8 Also, inappropriate management and impaired awareness of hypoglycemia among adolescents could lead to seizures and unconsciousness. 9 In addition, long-term complications include microvascular and macrovascular diseases. Overall, managing T1DM is focused on bringing blood glucose levels toward targeted ranges to address short-term and long-term complications. 10 This could be achieved by enhancing self-efficacy regarding diabetes management, as reported by Sangruangake et al. 11 Due to the escalating rates of diabetes at both national and international levels, researchers have extensively explored various aspects of diabetes management, such as lifestyle changes, behavioral modifications, and the patients’ abilities to comprehend knowledge and to perform specific skills. Managing effectively becomes particularly challenging, especially during the pubertal phase, which is characterized by rapid physiological and psychological changes inherent in adolescent growth and development. 12 Guo et al 13 concluded that enhancing self-efficacy is an important strategy for reinforcing diabetes self-management among adolescents with T1DM.
In this assertion, self-efficacy was defined by Rasbach et al 12 as one’s perceived ability to follow a diabetes treatment program, and the authors recommended that educators recognize the concept of self-efficacy and the instruments by which they can assess self-efficacy among adolescents with T1DM. 12 Also, Law et al 14 concluded that dietary self-efficacy and perceived consequences of poorly managed diabetes are important aspects to consider in evaluating and managing diabetes among adolescents.
The Diabetes Management Self-Efficacy Scale (DMSES) was initially developed to assess the abilities of patients with diabetes in Western populations regarding their diet, blood glucose, and physical exercise. 13 The scale was most commonly used to evaluate self-efficacy among patients with type 2 diabetes,11,15-20 and other researchers have used the same scale to assess both types of diabetes. 21 However, fewer studies used the scale to assess the concept of self-efficacy among patients with T1DM.22-24
Messina 25 used the Italian version of the DMSES to examine the differences in self-efficacy between T1DM and type 2 diabetes. The study revealed significant differences between patients with T1DM and patients with type 2 diabetes in terms of the centrality of self-efficacy aspects and how they are related to each other. This was referred to the higher connection between the patient’s ability to handle nonregular self-management activities in T1DM and other aspects of lifestyle and disease management than in type 2 diabetes.
Rasbach et al 12 conducted an integrative review concerning self-efficacy measurement tools for T1DM within the time frame from 2003 to 2013. They recognized 10 distinct self-efficacy measurement scales predominantly based Bandura’s social cognitive theory and model of self-efficacy as their conceptual framework, and the participants were primarily young individuals with T1DM belonging to the White middle-class demographic. 12 Furthermore, they emphasized the importance of developing valid and reliable instruments for adolescents with T1DM who experience modern technological advances in diabetes management. 12 So, it is of great importance to use an evidence-based measure through which health care professionals could assess the self-efficacy of adolescents with T1DM and hopefully predict their behaviors relevant to diabetes management. Unlike most of the existing measures, the measure used in the current study, Type 1 Diabetes Mellitus Self-Efficacy Scale (T1DM-SES), is designed to evaluate self-efficacy levels among patients with T1DM based on the guidelines of the International Society for Pediatric and Adolescent Diabetes (ISPAD). 26 The ISPAD Clinical Practice Consensus Guidelines provide the only comprehensive set of clinical recommendations for children, adolescents, and young adults with diabetes on a global scale. The used guidelines were about the definition, epidemiology, and classification of diabetes in children and adolescents 27 ; glycemic control targets and glucose monitoring 28 ; insulin treatment 29 ; DKA 30 ; managing hypoglycemia 31 ; sick day management 32 ; exercise in adolescents with diabetes 33 ; complications and associated conditions with T1DM 34 ; nutritional management 35 ; and diabetes technologies and glucose monitoring. 36 These guidelines are authored by experts from around the world and include a chapter specifically addressing limited care in limited resource settings. 37 Thus, the purpose of the study was to assess self-efficacy levels among adolescents with T1DM and to identify contributing factors using a new measure based on the ISPAD guidelines (T1DM-SES).
Methods
Research Design
A cross-sectional design was used to collect data from adolescents via an online questionnaire form.
Setting
The study was conducted in northern Jordan, specifically, at a public pediatric teaching hospital and a university-affiliated teaching hospital. These 2 hospitals serve the vast majority of adolescents with T1DM and are where endocrinologists and education specialists are available.
Population and Sampling
The study targeted all adolescents with T1DM in northern Jordan. An invitation letter was sent to 203 adolescents with T1DM. According to the World Health Organization, 38 adolescence is defined as “the phase of life between childhood and adulthood, from ages 10 to 19.” In this study, researchers targeted adolescents ages 12 to 18 because they hypothesized that this age group would commonly experience physical changes and psychosocial circumstances associated with puberty. Moreover, because adolescents age 19 are likely to attend university, their lifestyles may differ significantly, possibly influencing their way of managing their conditions. Therefore, in the current study, eligible participants were all adolescents with T1DM, ages between 12 and 18 years, with no mental or physical disabilities, and who could read and write Arabic effectively.
Data Collection Procedure and Ethical Considerations
Ethical approval was obtained from the institutional review board of the nursing school at Zarqa University (No. 10/2022). Then, permission for data collection was obtained from the institutional review board of the Ministry of Health and the ethical committee at King Abdullah II University Hospital. The researchers obtained the contact information of eligible participants by collaborating with education specialists and accessing the hospital’s medical records. An informed consent form was sent as a PDF document to the parents of potential participants, and they were asked to return it if they were willing to participate. The document included information about the purpose and significance of the study, actual and potential benefits, a statement that entails voluntary participation and the free choice of skipping any question(s) with no penalty on their treatment plan, a clear statement that assures participants about the researcher’s commitment to the confidentiality of the information provided, and a statement that informs the participants that they are allowed to ask any question before and after data collection via the researcher’s contact information. In addition, information was included about the time needed to fill out the questionnaire, how the data will be treated and discarded, and how the results will be disseminated in the future. At the end, 2 statements presenting the parents’ and adolescents’ agreement to participate were included: “I agree that my son/daughter can participate in the study” and “I agree to participate in the study,” respectively. This was considered the parents’ and adolescents’ consent form and reflected their voluntary participation. The parents were asked to return the document in case of agreement and were asked to determine the method by which the researchers could send the questionnaire survey to their son or daughter. Finally, the link for the questionnaire survey was sent to adolescents through the suggested method.
Data Collection Instrument
The questionnaire survey comprised 2 parts. The first part consisted of background information, including demographic variables (eg, adolescent’s age, gender, and place of residence and employment status of the mother or primary health care provider) and T1DM management-related variables (e., last A1C value [mmol/L]; the number of previous admissions due to DKA, if there are any; the number of daily glucose checks; having records for glucose readings; the history of hypoglycemic episodes, and other variables as shown in Table 2).
Ther second part of the questionnaire included the T1DM-SES items. The T1DM-SES was developed based on the ISPAD guidelines. 39 The scale is composed of 21 items in which the adolescents were asked to report their ability for a specific task using a 5-point Likert scale ranging from 1 (extremely not able) to 5 (extremely able). The items of T1DM-SES measure the participants’ perceived ability to differentiate between T1DM and type 2 diabetes, recognize blood glucose targets, adjust and inject insulin appropriately, manage hyperglycemia and ketoacidosis, manage severe hypoglycemia, manage their glucose levels during sick days, manage their meals, and identify potential comorbidities as indicated in the ISPAD guidelines.30,35 Al-Shorman et al 39 documented that following Yusoff’s 40 recommended approach, the scale-level content validity index of the T1DM-SES based on the universal agreement was 0.95. Additionally, their analysis yielded an internal consistency coefficient of 0.852, as measured by Cronbach’s alpha. 39
Data Analysis
Data were analyzed using SPSS version 28. Initially, descriptive statistics were used to analyze background variables, demographic variables, and diabetes management-related variables and to reveal the mean and standard deviation of T1DM-SES items. Then, a t test and an analysis of variance (ANOVA) were used to detect differences in self-efficacy scores in terms of demographic and diabetes management-related variables.
A hierarchical multiple regression analysis was conducted to find predictors of self-efficacy among adolescent patients with T1DM. The researchers entered the variables into the analysis using the “Enter” method. In the first step, demographic variables were entered: gender, caregiver employment, having a family member with T1DM, having a family member with type 2 diabetes, and comorbidities. In the second step, the management-related variables were entered: glucocheck before meals, A1C check every 3 to 4 months, last A1C level, monthly quantity of purchased glucocheck strips, previous admission due to ketoacidosis, and history of severe hypoglycemia. The researchers considered .1 as the significance level for variable entry in the hierarchical linear regression model.
Results
A total of 161 adolescents completed the questionnaire survey, achieving a response rate of 79.3%. The assessment of internal consistency reliability for the T1DM-SES was conducted using Cronbach’s alpha, which is the most commonly utilized internal consistency coefficient, as recommended by Kalkbrenner. 41 The obtained value was 0.95.
Background Variables
Regarding the participants’ demographic characteristics, the adolescents’ mean age was 13.44 (SD = 1.41) years, and 50.3% of them were females. A percentage of 13.7 had a family member with T1DM, and 72.7% of the participants had unemployed mothers; more details are presented in Table 1.
The Adolescents’ Demographic Variables (N = 161)
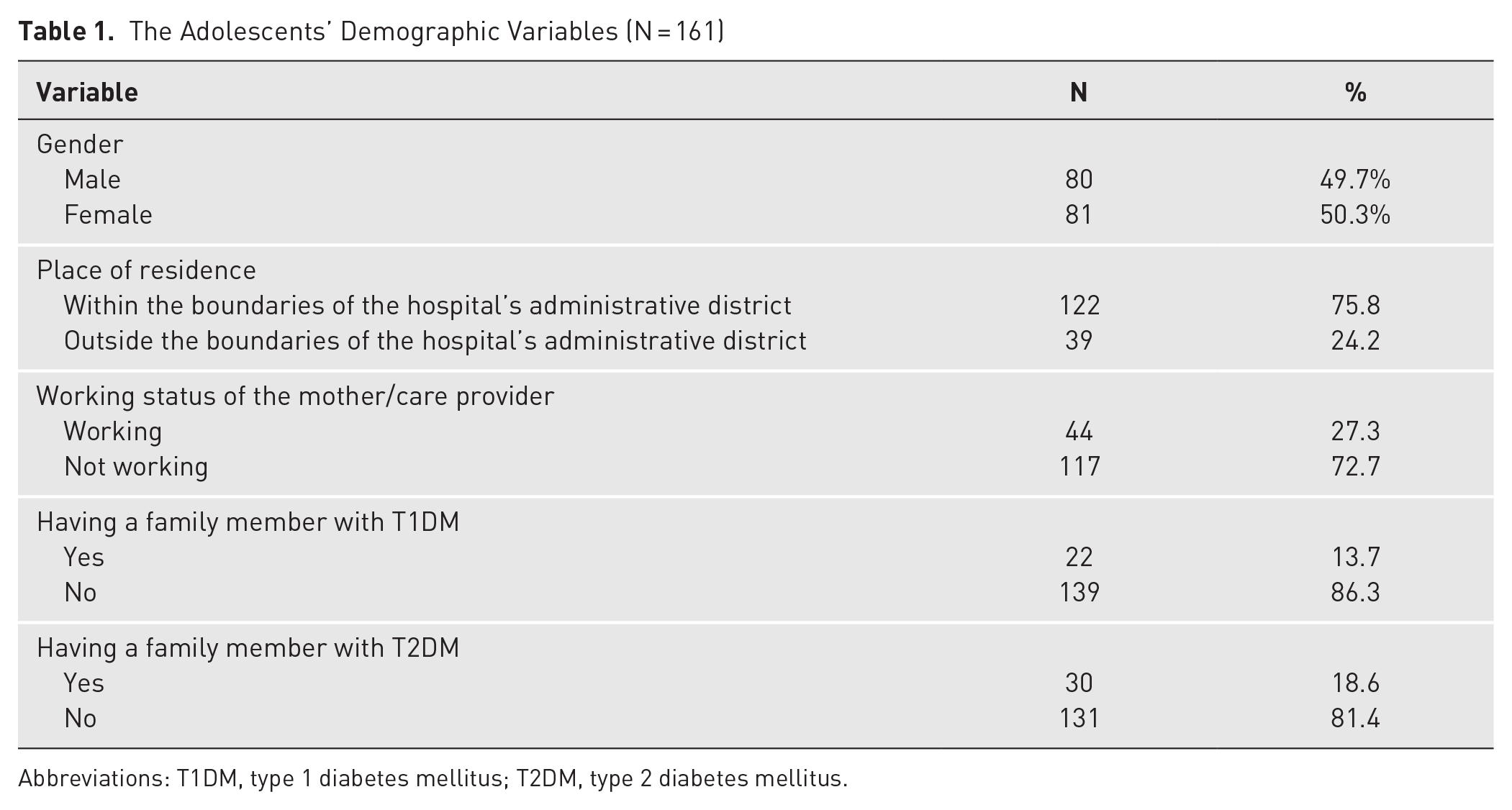
Abbreviations: T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
T1DM Management-Related Variables
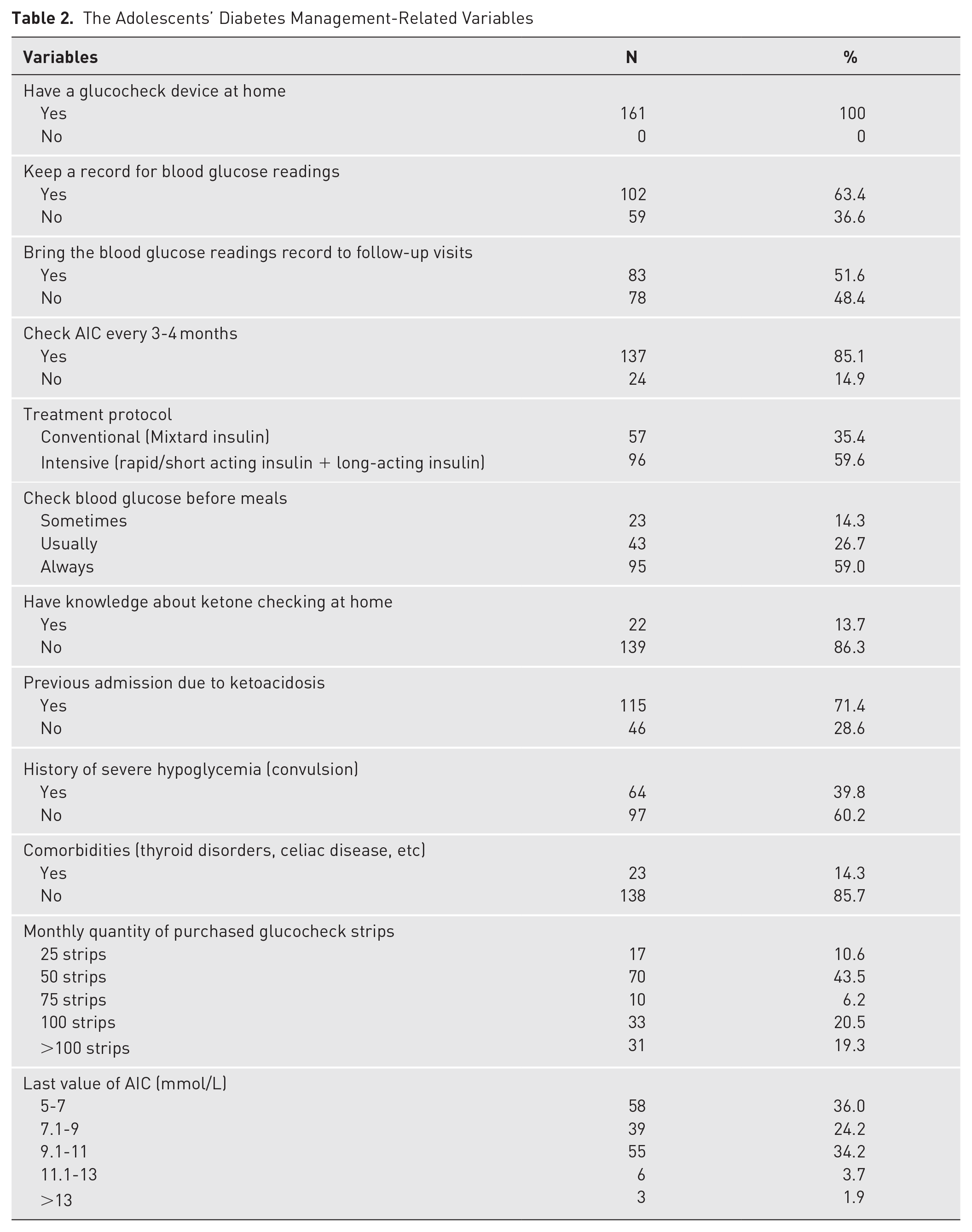
The participants’ mean duration since the first diagnosis of T1DM was 4.35 years (SD = 2.8). All adolescents reported having a glucocheck device at home. A percentage of 63.4 reported having a glucose reading record, and 51.6% brought the record during follow-up visits. A percentage of 71.4% had a previous admission due to DKA, and 39.8% had a history of 1 or more hypoglycemic episodes. In addition, 59% reported that they checked their blood glucose before meals. Although only 13.7% knew about ketone testing at home, more than half of the adolescents (59.6%) were treated by the intensive protocol. Also, 43.5% reported purchasing 50 glucocheck strips monthly. About one-third (36%) had A1C ranging from 5% to 7%, and 14.3% had comorbidities, as shown in Table 2.
The Adolescents’ Diabetes Management-Related Variables
Adolescents’ T1DM-SES Scores
The average mean score of the participants’ self-efficacy was 3.46 (SD = 0.767). We organized the mean scores of the 21 items in descending order, aiming to compare how each item performed within the complete set. Additionally, for a better understanding of self-efficacy levels, we categorized the results into 3 levels based on the range of the revealed mean scores, as shown in Table 3. In this classification, mean values falling within the range of 3.94 to 4.25 denoted the highest relative self-efficacy levels, scores ranging from 3.48 to 3.93 signified the relative middle self-efficacy levels, and mean values spanning from 2.04 to 3.47 indicated the lowest relative levels of self-efficacy.
Means and Standard Deviations of Adolescents’ Self-Efficacy Scores in Descending Order (N = 161)
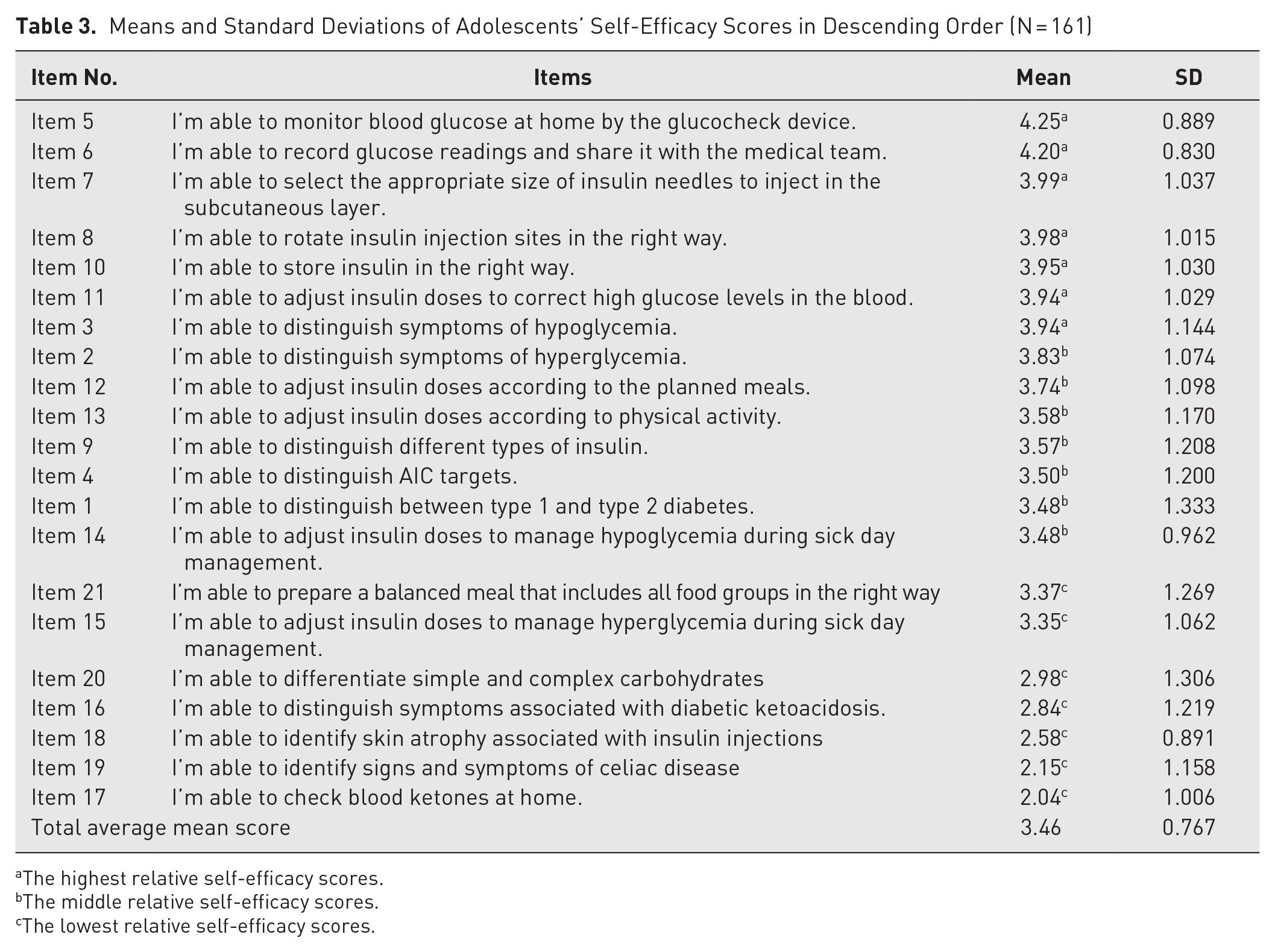
The highest relative self-efficacy scores.
The middle relative self-efficacy scores.
The lowest relative self-efficacy scores.
The highest average score was related to adolescents’ self-efficacy in monitoring their blood glucose levels at home using the glucocheck device. Subsequently, the adolescents’ self-efficacy to record these glucose readings and effectively communicate them to their medical team had the next highest score. Following this, there were 3 items concerning adolescents’ self-efficacy regarding insulin injection: the ability to choose the right needle size, properly rotate injection sites, and ensure appropriate insulin storage. Also, these findings were followed by the adolescents’ ability to correct elevated blood glucose levels and accurately recognize symptoms of hypoglycemia. Conversely, the perception of hyperglycemia symptoms fell within the realm of moderate levels of self-efficacy, alongside the adolescents’ competence in adapting insulin dosages based on planned meals and physical activity and effectively handling hypoglycemia during sick days. Moreover, the adolescents’ ability to distinguish between T1DM and type 2 diabetes, comprehend A1C targets, and differentiate various types of insulin also resided within the boundaries of moderate self-efficacy levels.
Finding from the study disclosed adolescents’ limited abilities when it came to skills such as preparing a well-balanced meal, distinguishing between simple and complex carbohydrates, and modifying insulin dosage to control hyperglycemia during sick days. Furthermore, the results displayed diminished ability among adolescents to recognize symptoms associated with ketoacidosis, identify manifestations of celiac disease, and acknowledge skin atrophy related to insulin injections. Lastly, the lowest level of self-efficacy was revealed in adolescents’ ability to check their blood ketone levels at home. Ultimately, the overall average mean score pointed to a state of moderate self-efficacy among the adolescents, as demonstrated in Table 3.
Differences in Self-Efficacy Levels According to Adolescents’ Demographic and Management-Related Variables
A series of t tests and an ANOVA were performed to examine differences in adolescents’ self-efficacy based on their demographic (Table 4) and management-related variables (Table 5). In terms of demographic characteristics, female adolescents demonstrated significantly higher self-efficacy levels (M = 3.71, SD = .70) than males (M = 3.22, SD = .76), t(160) = −4.22, P < .001. Furthermore, patients who have working mothers or caregivers demonstrated higher self-efficacy levels than others. Having a family member with T1DM or type 2 diabetes also affected the patients’ self-efficacy, t(160) = −6.62, P < .001 and t(160) = 2.31, P = .024, respectively. Surprisingly, those who have a family member with T1DM showed a lower level of self-efficacy than those who do not have a family member with T1DM. On the other hand, those who have a family member with type 2 diabetes showed a higher level of self-efficacy than others.
Differences in Self-Efficacy Scores Based on Demographic Characteristics
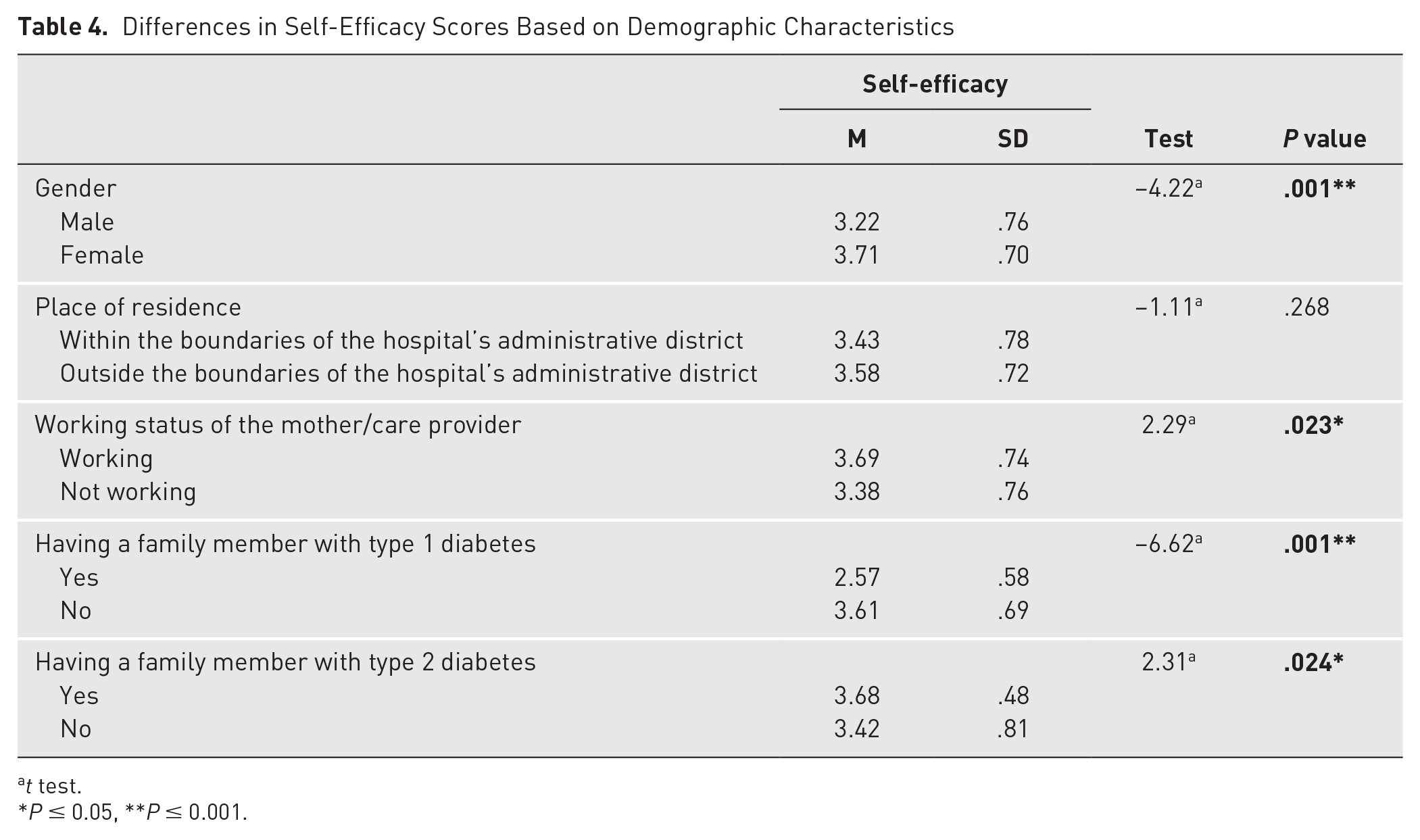
t test.
P ≤ 0.05, **P ≤ 0.001.
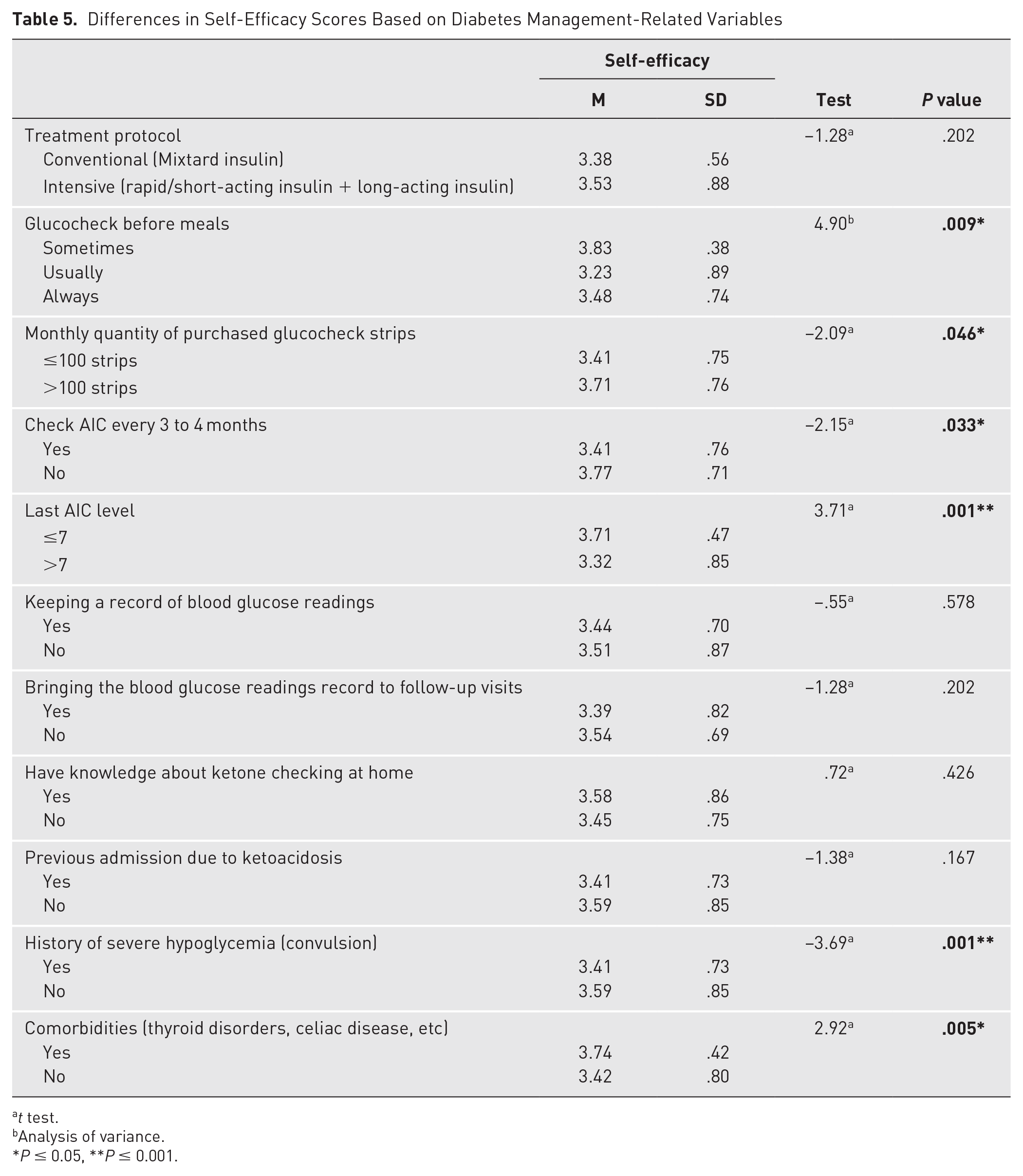
Differences in Self-Efficacy Scores Based on Diabetes Management-Related Variables
t test.
Analysis of variance.
P ≤ 0.05, **P ≤ 0.001.
A one-way ANOVA revealed a statistically significant difference in self-efficacy between patients based on the frequency of measuring their blood glucose levels before meals, F(2, 158) = 4.90, P = .009. Tukey’s honestly significantly different test for multiple comparisons uncovered that the patients who sometimes measure their blood glucose levels before meals exhibit higher self-efficacy levels compared to other participants who measure their levels usually or always. In the same context, a t test revealed that self-efficacy levels differed according to the monthly quantity of purchased glucocheck strips, t(160) = −2.09, P = .046. More specifically, adolescents purchasing over 100 glucocheck strips monthly exhibited elevated levels of self-efficacy compared to those buying fewer than 100 strips per month. Also, patients who checked their A1C every 3 to 4 months exhibited lower self-efficacy levels than those who did not check the A1C levels. Furthermore, patients with a recent A1C measurement of 7 or less exhibited higher self-efficacy levels than those with a reading of more than 7. In the same line, adolescents who reported a history of severe hypoglycemia, including convulsion, exhibited lower self-efficacy levels (M = 3.41, SD = .73) than those who never had a severe hypoglycemic event (M = 3.59, SD = .85), t(160) = −3.69, P < .001. Moreover, patients’ self-efficacy levels varied depending on the presence of comorbidities, such as thyroid disorders or celiac disease. Those with comorbidities demonstrated a higher level of self-efficacy (M = 3.74, SD = .42) than those without comorbidities (M = 3.42, SD = .80).
Predictors of self-Efficacy Among Adolescents With T1DM
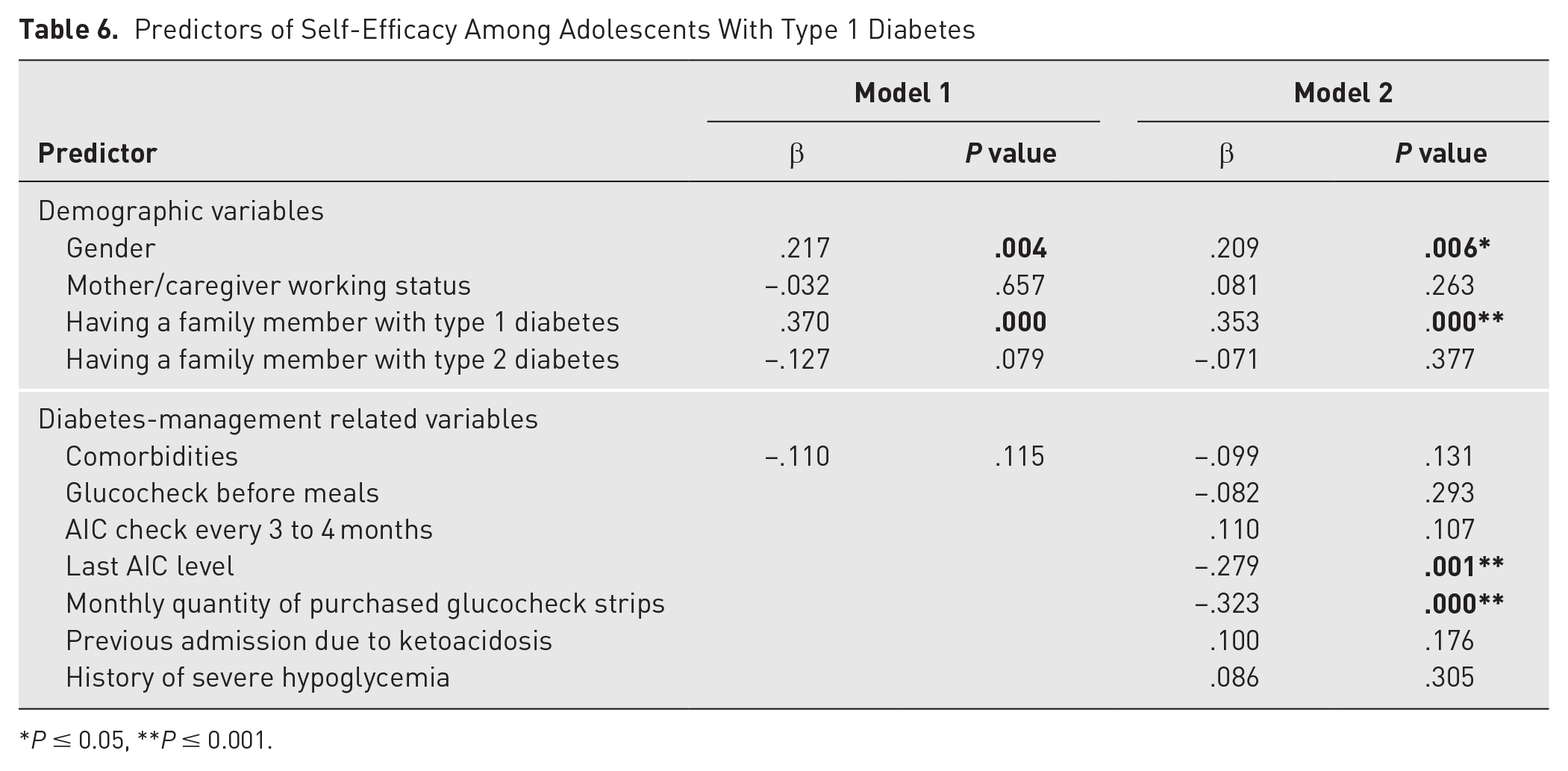
The overall regression was statistically significant, F(11, 149) = 8.63, P < .001. The demographic variables alone predicted 28% of the variation in adolescents’ self-efficacy level, which increased to 39% with the addition of the management-related variables. Significant predictors were gender, having a family member with T1DM, last A1C level, and monthly quantity of purchased glucocheck strips (see Table 6). Female gender, not having a family member with T1DM, a last A1C level of less than or equal to 7, and buying more than 100 strips per month contributed to higher levels of self-efficacy. Having a family member with T1DM was the most important predictor among these variables (β = .353, P < .001).
Predictors of Self-Efficacy Among Adolescents With Type 1 Diabetes
P ≤ 0.05, **P ≤ 0.001.
Discussion
The purpose of the study was to assess self-efficacy among adolescents with T1DM. Findings demonstrated that among various abilities, the highest level of self-efficacy in adolescents was about monitoring blood glucose at home using the glucocheck device. Findings also aligned with results from Al-Shorman et al 39 such that the same item received the highest score in their study. This might be attributed to the significance of glucose level monitoring as a crucial aspect of diabetes management, often emphasized in health education and discharge plans. This is consistent with the results found by Mendez et al 42 in which daily glucocheck was one of the exhibited self-care practices among individuals who received specialized education. This might hold significant validity given that the subsequent items relate to essential needs for managing glucose readings and administering insulin injections. However, the adolescents exhibited moderate and low self-efficacy levels when it came to a more sophisticated understanding of modifying insulin doses to manage hypoglycemia and hyperglycemia during sick days, respectively. Similar results emerged regarding the adolescents’ self-efficacy in calibrating insulin doses to align with scheduled meals and physical activities. This outcome is understandable considering that approximately one-third of adolescents reported that they did not consistently monitor their blood glucose levels before meals. These findings indicated that the adolescents were able to administer fixed insulin doses regardless of fluctuations in blood glucose levels, meal size and composition, and changes in physical activity levels. These results are consistent with lower levels of adolescents’ self-efficacy to prepare a balanced meal that includes all food groups appropriately and to distinguish between simple and complex carbohydrates. This assertion could be confirmed given that only about one-third of the involved adolescents exhibited A1C values that fell within the specified blood glucose target (<7.0%) recommended by the ISPAD guidelines. 28 This could result in the conclusion that even though the majority of adolescents are frequently monitoring their A1C levels, they are still unable to manage deviations from the targeted level because of their compromised abilities regarding the previously mentioned aspects.
Over half of the adolescents were placed on intensive insulin treatment such that they had to receive a single dose of long-acting insulin primarily at night along with multiple rapid or short-acting insulin doses usually before meals. In this treatment protocol, to be effective, adolescents with T1DM should be able to adjust the rapid or short insulin dose to cover the carbohydrate content of the meal and to correct the actual blood glucose level when needed. This is especially crucial considering that rapid and short-acting insulin take effect within 10 and 30 minutes, respectively. 43 Due to its fast onset of action, several studies have highlighted the efficacy of employing continuous glucose monitoring devices to mitigate the potential risk of hypoglycemia.44,45 This technology has become accessible in Jordan over the past few years, but it is still not covered by health insurance. The overwhelming majority continue to rely on finger-prick glucometers. The finger-prick method of self-monitoring blood glucose continues to be an effective method for measuring glucose levels. However, it presents challenges in terms of patient convenience and offers constrained insights into glycemic variability, as highlighted by Moon. 46 For effective management of T1DM, the patient needs a minimum of 4 glucocheck strips per day, totaling around 120 strips per month. Additional strips are necessary to address critical hyperglycemic and hypoglycemic situations resulting from physical or psychological stressors, such as school exams, physical activities, and sick days. As a result, adolescents might require approximately 150 to 200 glucocheck strips per month, amounting to a cost of $50 to $100. However, when comparing this need with the reports from adolescents in the current study, where less than one-fifth purchased more than 100 glucocheck strips per month, it becomes evident that a notable number of adolescents are unable to purchase the necessary strips for effective diabetes management. This discrepancy might be intimately connected to the prevailing financial difficulties encountered by a significant proportion of Jordanians caused by the rising burden of chronic diseases and heightened demand for health care services that is further exacerbated by different factors such as population expansion, the consequence of the COVID-19 pandemic, and an influx of Syrian refugees. 47 These factors have exerted an impact on the gross national income per capita in recent years, leading to the World Bank’s 48 reclassification of Jordan’s economy from a high-middle-income status to a classification of low-middle-income. Accordingly, the estimated average monthly income in Jordan is $355 per capita. 49 So, it is not always possible for adolescents and their families to handle the cost of glucocheck strips and other needed utilities to manage diabetes effectively, which can significantly impact their self-efficacy. Congruently, Dos Santos et al 50 highlighted the cost as an essential aspect that determines the patients’ and health care providers’ choices between frequent finger-pricks taken throughout the day and continuous glucose monitoring. Other studies highlighted the cost-effectiveness of using continuous glucose monitoring devices in reducing the risk of severe hypoglycemia, 51 improving A1C levels, 52 reduction in the risk of hypoglycemia, and decreased hospitalizations due to ketoacidosis. 53
Adolescents reported a compromised ability to recognize the symptoms of DKA, and the majority reported lack of knowledge about checking ketone levels at home. This could strongly explain the rationale behind the hospitalization of approximately two-thirds of adolescents as a consequence of ketoacidosis. This percentage significantly surpasses the figure reported in Canada, where only 32.4% of children and adolescents diagnosed with T1DM encountered episodes of ketoacidosis. 54 Based on the ISPAD guidelines, DKA is a potentially life-threatening complication that typically arises in a minimum of one-third of individuals newly diagnosed with T1DM, 30 and it could considerably cause subtle declines in memory shortly after the diagnosis of T1DM. 55
The current study showed that a small subset of adolescents indicated the presence of comorbidities. These conditions could potentially explain the reported low level of self-efficacy in recognizing the symptoms linked to celiac disease. Comparable outcomes were stated by Odeh et al, 7 in which positive serology results and confirmed celiac disease through biopsy were found in proportions of 16.6% and 9.1%, respectively, among pediatric patients with diabetes. This aligns with a prior investigation conducted in Italy by Camarca et al, 56 where the prevalence of celiac disease ranged from 4.4% to 11.1%.
Findings of the study also revealed that being a female can act as a predictor for higher self-efficacy levels. Consistently, Wilt 57 found that adolescent females had higher self-efficacy levels in relation to self-management of diabetes than males. Also, the current study revealed that adolescents who checked their blood glucose before meals and A1C levels less frequently tend to report higher levels of self-efficacy. This could be due to their ability in controlling their self-management behaviors and accordingly assuming that their glucose levels and A1C levels are under control. Conversely, adolescents who perceive themselves as unable of managing their glucose levels frequently rely on regular A1C values to detect and address any irregularities as needed. This explanation could be supported by findings indicating that adolescents with A1C values within the target range exhibited elevated levels of self-efficacy, whereas those with a history of severe hypoglycemic episodes demonstrated lower levels of self-efficacy. It is possible that maintaining a sense of independence positively influenced the adolescents’ perceived self-efficacy. This is evidenced by the higher levels reported by adolescents with working mothers compared to others. Moreover, the current research revealed that having another family member with T1DM could have a negative effect on the adolescents’ self-efficacy. This may be attributed to the overwhelming climate created by the responsibilities of diabetes management that could possibly lead to psychological distress that affected the adolescents’ self-efficacy levels. This could be supported given that 42.1% and 73.8% of all adolescents in Jordan are experiencing anxiety and depression, respectively, as reported by Malak and Khalifeh. 58
Ultimately, when considering the demographic and diabetes management-related aspects, the overall low self-efficacy levels among adolescents can be attributed to various factors. A significant element in this regard pertains to the adolescents’ limited understanding, which could be heavily reliant on the quality of health education they receive in which the focus is mainly on most fundamental requirements, such as insulin injection and checking glucose levels at home. Another contributing factor could be the absence of a round-the-clock support system, resulting in fragmented and overlooked care. Additionally, financial limitations play a role because insurance coverage for glucocheck strips and modern technological devices, such as continuous glucose monitors and ketone meters, is lacking. In their study, Prahalad et al. 59 reported that the most significant decrease in A1C levels was observed in children with diabetes who recently started using continuous glucose monitoring.
Implications and Conclusion
Assessing adolescents’ self-efficacy with an evidence-based measure like T1DM-SES can reveal areas where their abilities may be compromised or lacking. The results of the current study uncovered that adolescents felt capable of handling basic tasks related to managing T1DM but may need support in more complex tasks, such as correcting fluctuations in blood glucose levels, counting carbohydrates, and accordingly adjusting insulin doses. Additionally, T1DM-SES covers areas not addressed by other measures, such as ketone testing at home and managing diabetes during sick days. Therefore, using T1DM-SES as an evidence-based measure can significantly guide the design of health education plans tailored to adolescents, ensuring effective T1DM management and overall well-being.
Health care policymakers must update current policies to recognize the urgent need for comprehensive health insurance coverage, including various tools and technological devices, to improve the management of T1DM in adolescents. This broader coverage will make it easier for adolescents to maintain their A1C levels within the normal range, eventually preventing or delaying complications, reducing hospitalizations, and improving their overall quality of life.
Limitations and Recommendations
It is essential to acknowledge specific limitations when interpreting the findings of the present study. The study’s descriptive and nonexperimental design precludes the establishment of causal relationships that evolve. To strengthen the credibility of assessments regarding perceived self-efficacy over extended periods, future research should adopt longitudinal methodologies involving more extensive participant cohorts. Longitudinal investigations can capture alterations in adolescents’ perceived self-efficacy within the framework of diabetes self-management during adolescence.
The potential for self-reporting bias could also interfere with the findings, caused by the tendency of participants to present their abilities more positively due to the influence of social desirability. Therefore, it is recommended to adopt quasi-experimental and true experimental designs to diminish bias effects and enhance internal validity.
Another limitation could be related to the area of glucose monitoring. Glucose monitoring has advanced significantly with the rise of continuous glucose monitoring systems, which are becoming more common. However, due to high costs and limited insurance coverage, especially in limited-resource countries, many still rely on self-monitoring blood glucose devices. ISPAD advocates for the increased availability of continuous glucose monitoring for children and adolescents with diabetes, recommending its use as soon as possible after diagnosis wherever it is accessible. 36 Therefore, it is highly recommended, based on evidence, that T1DM-SES includes an item or items about continuous glucose monitoring. Additionally, health policymakers should strive to ensure that continuous glucose monitoring devices are covered by health insurance.
Footnotes
Acknowledgements
The authors extend their gratitude to hospital administrators and education specialists for their vital support in obtaining participant contact information, which facilitated the data collection process. Their dedication and cooperation were fundamental in ensuring the smooth execution of the current research objectives. The study was granted ethical approval to conduct the study by the institutional review board at Zarqa University under approval No. 10/2022. The study was conducted in accordance with the ethical standards noted in the Declaration of Helsinki and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
No conflict of interest.
Funding
The present study did not receive any form of financial support.