
Abstract
Purpose
The purpose of the study was to explore the facilitators and barriers of health behaviors in patients with type 2 diabetes (T2D), providing a reference for the development of health behavior interventions programs.
Methods
A qualitative descriptive research design was adopted, and interviews were conducted with 25 patients with T2D. The interview guide was developed based on the health action process approach theory. The interviews were audio-recorded and transcribed verbatim. Data analysis was performed using thematic analysis.
Results
Through the analysis of interview data, 2 main themes were identified: facilitators and barriers of health behaviors, comprising 18 subthemes. The facilitators included self-efficacy, outcome expectations, risk perception, intention, action planning, coping planning, emotional regulation, proactive and sustained sense of responsibility, and multidimensional social support. The barriers included insufficient disease awareness, insufficient self-control, impact of social activities, low self-efficacy, accessibility of personal conditions, lack of problem-solving skills, lack of disease management knowledge, lack of social support, and cognitive decline.
Conclusions
When designing health behavior intervention programs for patients with T2D, it is crucial to consider both facilitators and barriers to enhance the effectiveness of the interventions to encourage patients to adopt healthy lifestyles, improve their quality of life, and reduce the occurrence of complications.
Diabetes mellitus is a chronic metabolic disease characterized by hyperglycemia resulting from insulin resistance and insufficient insulin secretion. 1 According to the International Diabetes Federation (IDF), the global number of adults with diabetes reached 537 million (10.5%) in 2021, indicating that approximately 1 in 10 adults is affected. 2 The IDF projects that by 2045, this number will rise to 783 million, with the prevalence among adults potentially reaching 1 in 8. 3 In China, the prevalence of diabetes is as high as 11.2%, 4 making it the country with the highest number of adult diabetes cases. Among all types of diabetes, type 2 diabetes (T2D) accounts for over 95% of cases. 5 Over the past decade (2011-2021), the number of persons with diabetes in China increased from 90 million to 140 million, marking a 56% rise. 3 It is predicted that by 2045, the number of persons with diabetes in China will reach 174.4 million. 6 Diabetes has become a major public health issue threatening residents’ health. Poor blood glucose control in persons with diabetes can lead to serious complications, including infections, kidney failure, blindness, and lower limb gangrene, which are major causes of disability and mortality among patients. 7 These complications severely impact patients’ quality of life and impose significant economic and social burdens on the nation and society.8,9 Therefore, effective health management for patients with T2D is crucial.
Guidelines for diabetes prevention and control from multiple countries emphasize that patient self-management is crucial for controlling disease progression.10-12 However, adherence to self-management guidelines among patients is currently suboptimal. 13 Studies indicate that the adherence rate to dietary guidelines among T2D patients is 57.27%, 14 and adherence to blood glucose monitoring and exercise is relatively low, at 48.13% and 49.79%, respectively. 15 Therefore, understanding the facilitators and barriers behind the health behaviors of patients with diabetes can provide valuable insights for developing targeted health behavior intervention programs. Currently, there is a lack of qualitative studies on the facilitators and barriers of health behaviors in patients with T2D.
The health action process approach (HAPA) is a theory proposed by German psychologist Ralf Schwarzer. 16 This theory emphasizes that changes and maintenance in health behaviors result from the interplay between cognitive, affective, and behavioral factors. It understands the transformation from behavioral intentions to actual behavior through mechanisms or strategies that predict intention and translate it into action. 17 HAPA consists of 3 continuous and sequential phases: the pre-intentional phase, the intentional phase, and the action phase (see Figure 1). Compared to other behavior change theories, HAPA places greater emphasis on planning and self-efficacy in human behavior change. Currently, HAPA has been applied in the health management of various diseases, including cancer, 18 diabetes, 19 mental disorders, 20 oral diseases, 21 and gynecological diseases. 22
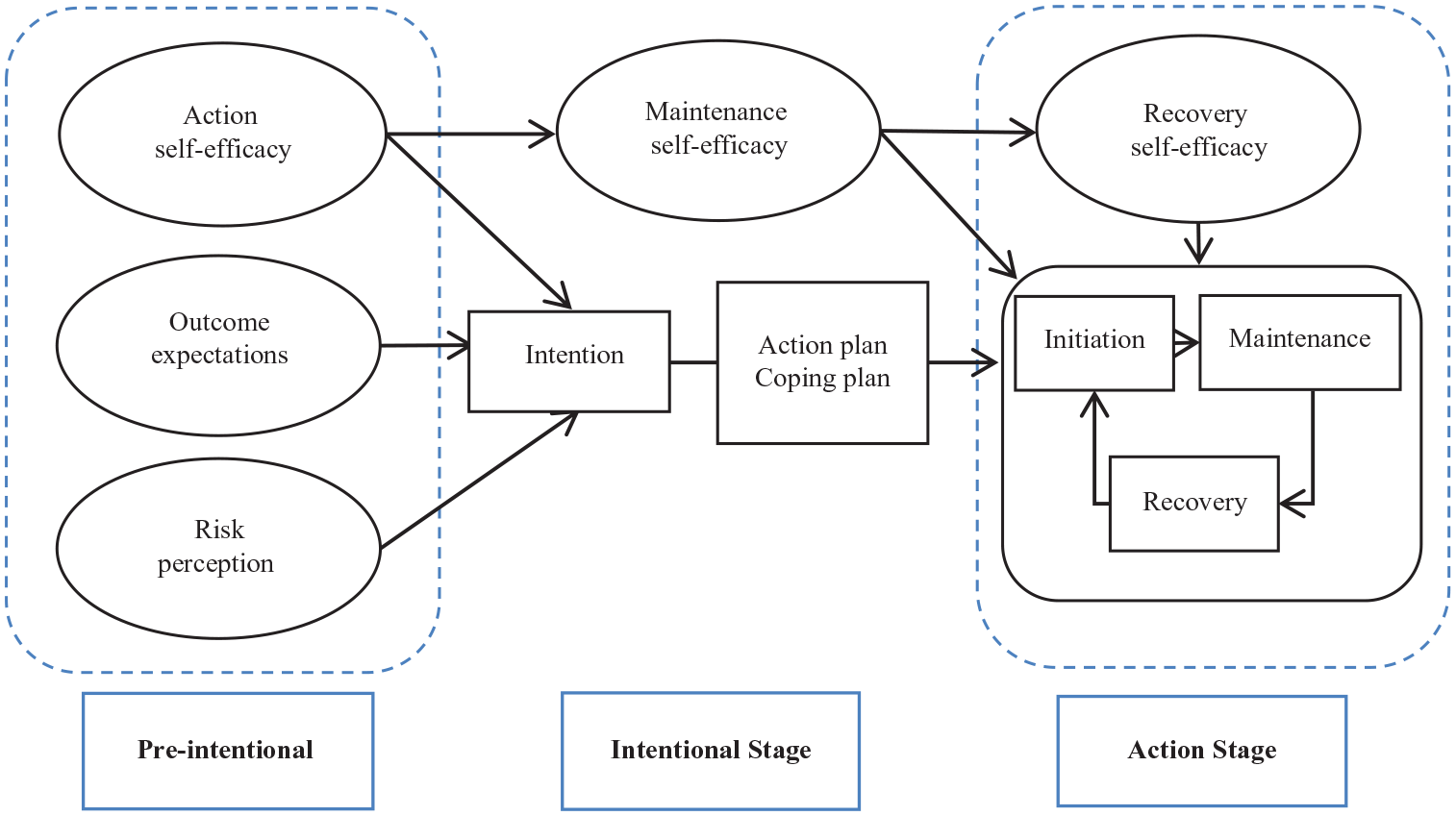
Schematic diagram of the health action process approach (HAPA) framework. 16
The purpose of the study was to explore the facilitators and barriers to health behaviors in patients with T2D within the framework of the HAPA theory, providing a reference for the development of health behavior interventions programs.
Methods
Study Design
This study employed a qualitative method characterized by a descriptive and exploratory design. 23 The qualitative descriptive (QD) research design serves as an effective tool for understanding patients’ perspectives and attitudes regarding T2D-related facilitators and barriers. Its inherent flexibility allows for the use of various data collection methods, capturing participants’ authentic experiences. 24 QD research emphasizes the significance of participants’ voices, uncovering new themes that yield valuable insights for policy formulation and practice improvement. 25
Setting and Sampling
This study was conducted on the platform of an internet hospital in China that holds an internet hospital license. Purposeful sampling was employed to select patients with T2D who had registered with the internet hospital and followed the principle of maximum variation to ensure diversity in participants’ age, gender, education level, and disease duration. Interviews were conducted from May to November 2023.
Inclusion criteria were as follows: patients who meet the 1999 World Health Organization (WHO) diagnostic criteria for T2D, patients with T2D who are using a computer or smartphone and have been receiving health management through the internet hospital for more than 6 months (patients who have fully experienced the current internet hospital-based diabetes health management model), and patients with normal cognitive abilities.
Exclusion criteria were as follows: patients with severe organic diseases of major organs, such as the heart, liver, or kidneys; patients with psychological or psychiatric disorders; bedridden patients or those with mobility impairments who are unable to care for themselves; pregnant women; patients with a recent history of surgery, trauma, acute major vascular complications of the heart or brain, or infectious diseases.
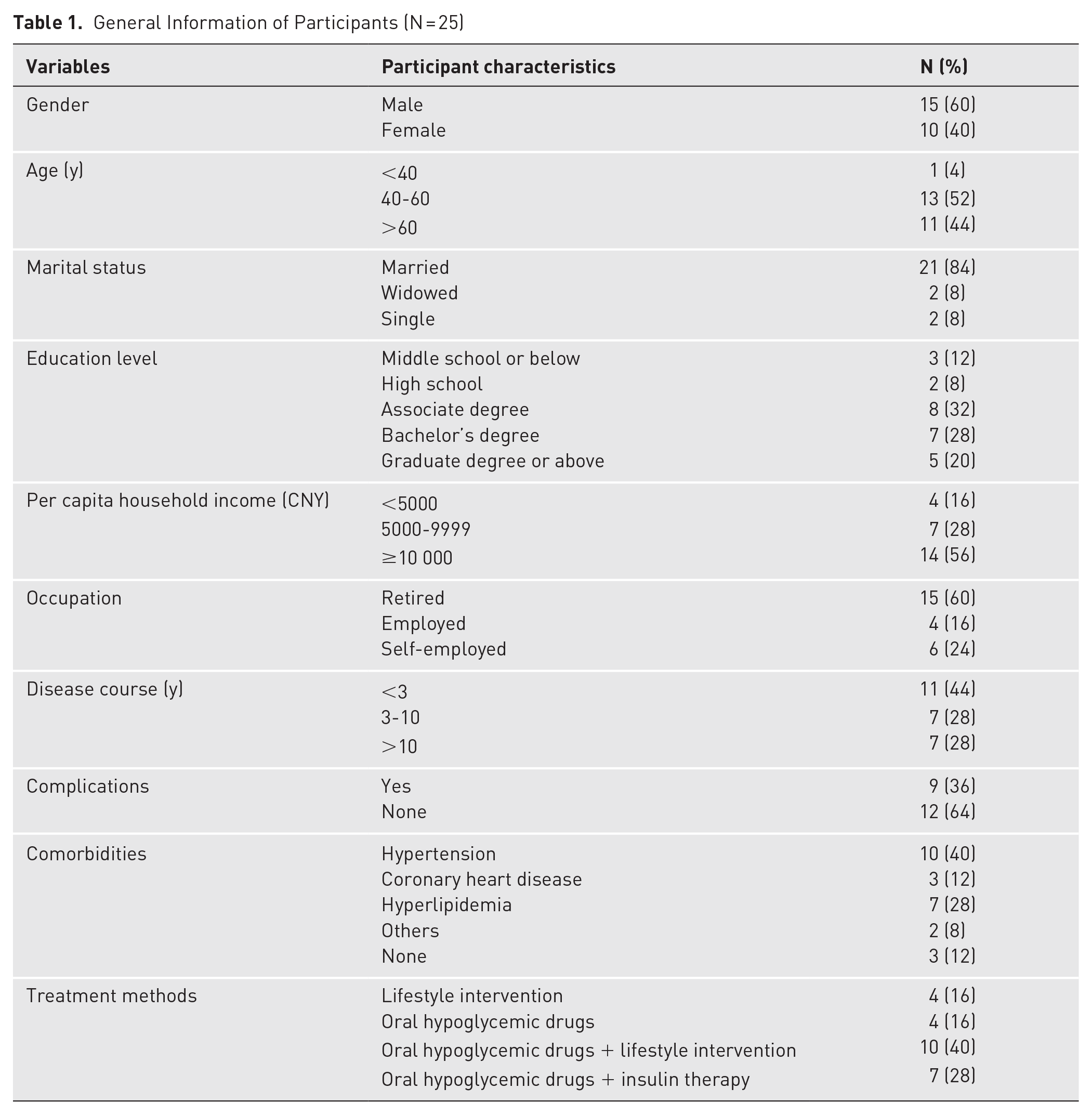
The first author of this article sent an oral invitation to 29 participants through the internet phone on the internet hospital platform. Among them, 25 participants agreed to be interviewed, and 4 declined. Interviews were conducted with 25 participants, and none of the participants withdrew during the interview process. The sample size was determined when no new themes emerged during data analysis, indicating data saturation; saturation was checked from the 23rd case onward, with an additional 2 cases collected for verification. The sample included 10 women and 15 men, with an average age of 57.76 ± 9.98 years. Other general information about the participants is presented in Table 1.
General Information of Participants (N = 25)
Patient Recruitment
The researcher (Wenyan Liu, a graduate student majoring in nursing, who works in an internet hospital and has been trained in qualitative research) visited the patient management interface on the internet hospital work platform to check the patient information and determine patients with T2D who met the inclusion criteria. Subsequently, the researcher contacted these patients via the internet telephone to explain the purpose, significance, and time requirements of the study. If participants verbally agreed to participate in the study, the researcher scheduled a specific time for the video interview.
Data Collection
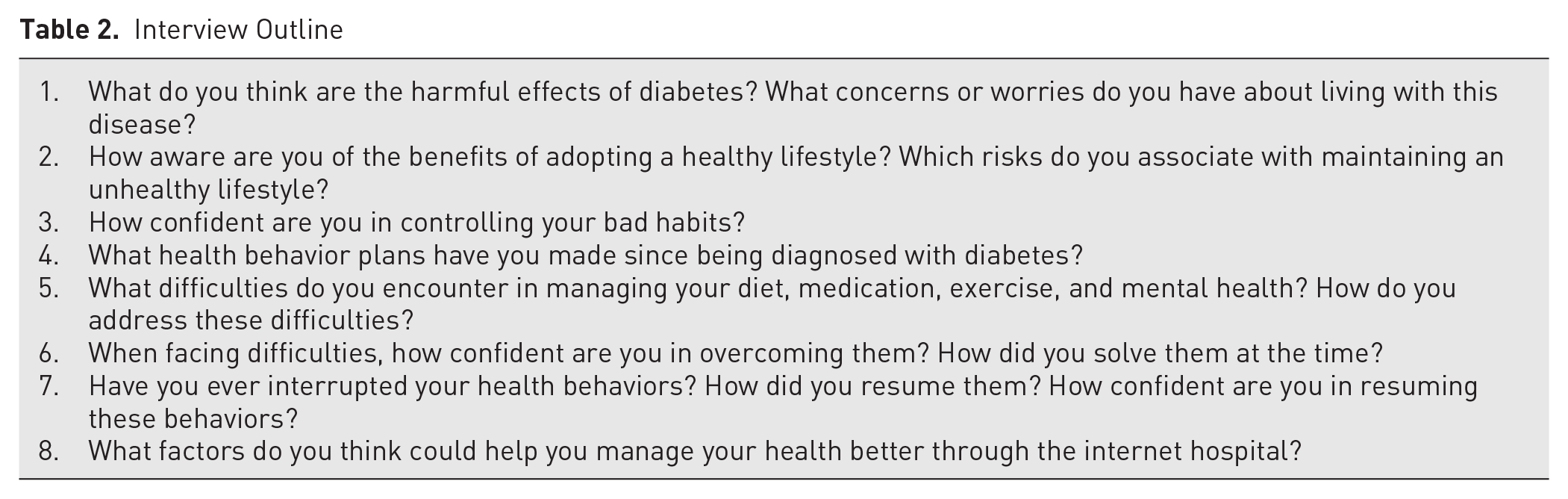
Based on the HAPA theory and the research objectives, an initial interview outline was developed. Subsequently, pilot interviews were conducted with 2 patients with T2D. Because no significant modifications were made to the interview outline, the results of these pilot interviews were included in the final data analysis. The final interview outline is shown in Table 2.
Interview Outline
On the day of the interview, the researcher would log into the internet hospital work platform 5 to 10 minutes before the scheduled time. Prior to the scheduled interview time, the internet hospital platform displayed a “Start Your Video Visit” link to initiate the session. If participants were not using the mobile app, they joined the video visit via a reminder link they received via SMS on their mobile devices. If participants had the mobile app open, they directly entered the video link. The interview officially began when the participant connected to the video call. During the interviews, only the researcher and participant were present. During the interview, the researcher utilized techniques to prompt, listen, and affirm to engage in an in-depth conversation with the participants; avoided leading questions; and took notes on memos regarding nonverbal cues (eg, facial expressions, body language). After the interview, the researcher promptly wrote reflective diaries. The duration of the interviews was typically 30 to 40 minutes.
Data Analysis
The recordings of the interviews were transcribed verbatim within 24 hours of the interviews, and nonverbal information that was recorded during the interviews was integrated into the transcripts. The transcriptions were then sent back to the participants for confirmation. However, the participants did not modify and supplement the interview materials. Two researchers (Wenyan Liu and Qianghuizi Zhang, both female master’s students, with training in qualitative research and experience in conducting qualitative studies) conducted the data collation and analysis independently. In cases of disagreement during data collation and analysis, they consulted a third researcher (Weiwei Liu, a female master’s graduate with extensive experience in qualitative research).
The data were analyzed using thematic analysis. 26 First, the researchers thoroughly read the transcribed texts multiple times to familiarize themselves with the data. Meaningful descriptions were then identified and openly coded. Similar codes were grouped and refined to generate subthemes and themes, which were reviewed and compared with the original data to ensure consistency. The themes were subsequently rephrased using simple and understandable terms. Lastly, the entire process of data analysis was documented. To minimize subjectivity, 2 independent researchers conducted the analysis and held regular discussions until consensus on the coded information was reached.
Validity and Rigor
To ensure the rigor of the study, the researchers strictly adhered to the 4 criteria proposed by Schwandt et al 27 : credibility, dependability, confirmability, and transferability.
Credibility
To ensure the credibility of the results, 2 researchers (Wenyan Liu and Qianghuizi Zhang) independently and repeatedly reviewed the data and regularly discussed any discrepancies in coding with other members of the research team (Weiwei Liu). In cases of disagreement, the original data were immediately reexamined and compared with field notes, reflective diaries, and other materials to accurately reflect the content from multiple perspectives, thereby enhancing the credibility of the data.
Dependability
Transcriptions were verified by an author (Weiwei Liu) who was not involved in the transcription process to ensure the dependability of the study results. Additionally, this study provided a detailed description of the inclusion and exclusion criteria, sampling, data collection, and analysis methods, 28 further enhancing the study’s dependability.
Confirmability
To ensure the confirmability of this study, the entire interview process was documented, allowing researchers to review the records at any time. 29
Transferability
To ensure the transferability of the study results, we employed purposive sampling to recruit participants of different genders and ages, ensuring diversity in the participant pool. 30 This study provides detailed descriptions of the participants’ characteristics and backgrounds to enhance the transferability of the findings.
Ethics Considerations
This study strictly adhered to the principles of the Declaration of Helsinki. 31 Before the commencement of the study, approval was obtained from the Ethics Committee of Capital Medical University (Approval No. Z2023SY081). Before the study began, participants were fully informed about the study’s purpose, methods, expected benefits, and potential risks. Verbal consent was obtained from each participant. Participation in this study was voluntary, and participants had the right to refuse or withdraw from the study at any time without any restrictions. Participants were assured that all information provided would be kept strictly confidential and that all data and results would be used solely for academic research.
Results
Through the analysis of the interview data, 2 main themes were ultimately identified: facilitators and barriers to health behaviors. The facilitators included 9 subthemes: self-efficacy, outcome expectations, risk perception, intention, action planning, coping planning, emotional regulation, proactive and sustained sense of responsibility, and multidimensional social support. The barriers also comprised 9 subthemes: insufficient disease awareness, insufficient self-control, impact of social activities, low self-efficacy, accessibility of personal conditions, lack of problem-solving skills, lack of disease management knowledge, lack of social support, and cognitive decline.
Theme 1: Facilitators to Health Behaviors
Risk perception
The perception of risk by individuals can motivate them to focus on their own risk factors, thereby promoting healthy behaviors. This includes the perception of the severity and likelihood of risk. The perception of severity refers to an individual’s awareness of the harms associated with a disease, including potential complications, declines in quality of life, the suffering caused by diabetes, and the economic burden placed on family and society. This awareness can awaken patients’ self-management consciousness, thereby encouraging healthy behaviors. Meanwhile, the perception of likelihood involves an individual’s recognition of their future risk of developing complications, which also contributes to the promotion of healthy behaviors.
I believe the harm caused by diabetes is considerable. For example, it can lead to complications such as vision loss and diabetic foot. I am concerned about the occurrence of these complications, so I pay close attention to maintaining stable blood glucose levels. (P1, female, 64, diagnosed for 2 years, no complications) I still remember that my father passed away because of complications from diabetes, so I can’t have complications myself. I must control them well and never develop diabetic nephropathy. (P13, male, 59, diagnosed for 5 years, no complications)
Outcome expectations
Expected outcomes refer to patients’ evaluations of the potential consequences of engaging in certain behaviors, which can be categorized into positive and negative outcome expectations. Positive outcome expectations involve patients’ anticipation of favorable consequences resulting from healthy behaviors, such as the ability to establish a regular lifestyle, improve blood sugar control, slow disease progression, enhance quality of life, and reduce the risk of complications. These positive expectations can encourage patients to adopt healthy behaviors. Conversely, negative outcome expectations pertain to patients’ anticipations of adverse consequences stemming from unhealthy lifestyles, such as poor blood sugar control, the onset of various complications, and diminished quality of life. To some extent, these negative expectations may also motivate changes in health behaviors.
Adopting a healthy lifestyle will prevent some complications or delay their onset, which can also improve my quality of life and extend my life span. If my blood sugar is well controlled, I can live like a normal person. (P3, male, 53, diagnosed for 3 years, no complications) Adopting an unhealthy lifestyle, such as overeating and excessive drinking, can lead to unstable blood glucose control. This instability increases the risk of complications at any time. For instance, hypoglycemia can cause fainting, which increases the risk of accidents while driving. On the other hand, hyperglycemia can lead to diabetic ketoacidosis. (P2, male, 72, diagnosed for 20 years, no complications)
Self-efficacy
Self-efficacy refers to an individual’s confidence and belief in their ability to successfully complete specific tasks, encompassing 3 types: action self-efficacy, maintenance self-efficacy, and recovery self-efficacy. Action self-efficacy reflects an individual’s confidence in succeeding in specific behaviors, influencing their motivation, emotions, and actions, especially when facing challenges, thus impacting goal setting, decision-making, and perseverance during adversity. Maintenance self-efficacy manifests as the belief in one’s capability to take necessary actions to achieve goals amid challenges while sustaining that confidence and persistence. Recovery self-efficacy describes the psychological process where a patient’s belief in their abilities temporarily declines after interrupting healthy behaviors, followed by a reinforcement of health beliefs that gradually restores their confidence to its original level.
I believe that by maintaining a regular exercise routine, I can effectively control my blood glucose levels. I exercise for an hour every day after meals. This practice strengthens my belief in my ability to manage my blood glucose and reinforces my confidence in maintaining healthy behaviors and controlling unhealthy ones. (P5, female, 46, diagnosed for 1 year, no complications) As a southerner who has always preferred eating white rice, I have successfully controlled my diet to manage diabetes and have gradually adapted to this dietary change. I believe I can keep going. (P8, male, 60, diagnosed for 1 year, no complications) After injuring myself in a biking accident, I rested at home for a while. During this time, my blood glucose control was poor. As my leg gradually healed, I started to resume exercising. I began with basic walking, covering over 10 000 steps daily, and added running twice a week. I am confident that I can continue this routine and maintain a reasonable diet, which will help me keep my blood glucose levels well under control. (P22, male, 46, diagnosed for 1 year, no complications)
Intention
Once individuals become aware of their issues, they begin to develop a willingness to change. This intention marks the starting point of behavior change, driving people to seriously consider and plan the necessary actions in order to improve their situation or achieve their goals.
I fully understand the severity of diabetes and am determined to treat it as a significant priority from now on, changing my previous attitude of neglect or indifference. I will approach diabetes with a more serious and responsible attitude to ensure my health is effectively managed. (P3, male, 53, diagnosed for 3 years, no complications)
Action plan
An action plan is a specific implementation strategy and timeline that individuals formulate based on their behavioral goals during the process of health behavior change. Developing a practical and feasible health management behavior plan is essential for patients to achieve behavioral change.
Because I understand the significance of glycated hemoglobin for diabetics, I plan to get tested every 3 months, monitoring at least 4 times a year. Based on the results, I can adjust my medication or lifestyle accordingly. (P22, male, 46, diagnosed for 1 year, no complications) Due to being overweight and having difficulty controlling my blood glucose levels, my doctor recommended increasing my physical activity. I plan to walk more than 15 000 steps daily and jog for half an hour after each dinner. (P11, male, 65, diagnosed for 25 years, with complications)
Coping plan
When patients encounter factors that impede their healthy behaviors during lifestyle changes, they implement corresponding coping plans. These plans may include choosing low glycemic index foods and adhering to dietary substitutions, utilizing management tools to assist in health management, controlling calorie intake during social dining, altering the order of food consumption, changing cooking methods, engaging in exercise at fixed times, and adjusting their diet, exercise, and drugs according to blood glucose feedback. These strategies help them overcome self-management difficulties and maintain healthy behaviors.
I enjoy eating rice, so I specifically bought a rice cooker designed to automatically separate the water from the rice. After eating, my blood glucose levels are around 7-8 mmol/L, which is really good. I recommend that other diabetic patients who love eating rice try this method as well. (P16, male, 34, diagnosed for 1 year, with complications)
Emotional regulation
In the process of diabetes self-management, patients often experience diabetes-related distress, including anxiety, depression, fear, and stigma. This distress can arise from various negative events, medication side effects, and complications. These emotional challenges can hinder patients from engaging in healthy behaviors. Emotional regulation, which involves a series of methods and techniques, helps individuals manage and control their emotions more effectively. By achieving a positive emotional state and improved psychological well-being, patients can better cope with the challenges posed by the disease. Actively adjusting their emotions enables them to maintain healthy behaviors more effectively.
Many times, I struggle to control my blood sugar well due to a lack of persistence, leading to thoughts of slacking off. Therefore, managing diabetes requires me to constantly adjust my emotions, overcome all difficulties, and move forward step by step. (P21, female, 51, diagnosed for 11 years, with complications) After my wife passed away, I found solace in sweets. During that time, I may have felt lonely and depressed, and eating something sweet made me feel a bit better. (P12, female, 73, diagnosed for 4 years, with complications) Sometimes when I go out to eat with friends, I feel embarrassed taking my diabetes medication in front of them. This action, though necessary for my health, affects my sense of dignity. (P24, female, 41, diagnosed for 1 year, no complications)
Proactive and sustained sense of responsibility
Patients’ psychological recognition of the importance of diabetes management is reflected in their sense of responsibility toward their own behavior and health. This sense of responsibility can motivate patients to engage more actively in the self-management of diabetes, thereby enhancing adherence to long-term treatment plans. It involves patients proactively acquiring knowledge about disease management, improving their understanding of the condition, and subsequently, increasing their motivation for healthy behaviors and confidence in disease treatment. It also includes actively self-regulating during the self-management process, monitoring their own health status, and analyzing the causes of abnormal indicators based on the monitoring results to adjust their health behaviors accordingly.
It is essential to take your disease seriously by paying close attention to your condition and regularly monitoring your blood glucose levels. Additionally, if your blood glucose is elevated, it’s important to manage your diet and increase physical activity. If it is too low, be sure to carefully adjust your medication and diet. (P7, male, 60, diagnosed for 25 years, with complications) If my blood glucose levels are abnormal once or twice, I might not pay much attention. However, if these abnormalities persist, I will focus on understanding why they occur and analyze the reasons. Reflecting on them is an important part of my health management strategy. (P11, male, 65, diagnosed for 25 years, with complications) It is essential to acquire a solid grasp of the basic knowledge about diabetes. If you have diabetes, taking the time to learn about it is a must. Understanding the condition is the first step to effectively managing it. As the saying goes, “Know yourself and know your enemy, and you can win a hundred battles.” (P22, male, 46, diagnosed for 1 year, no complications)
Multidimensional social support
Social support refers to the totality of emotional, material, informational, and functional assistance that individuals receive from various social networks, including family, friends, communities, and professional institutions. It encompasses various forms of support, such as emotional comfort, material aid, guidance, practical assistance, and social engagement, aiming to meet individuals’ needs at different levels.
When I visit hospitals, I need to book an appointment in advance and wait in line, leaving very little time for actual communication with the doctor. However, my experience with your online hospital is different and has been very helpful. You are like my family doctors, always accessible through my phone. It is thanks to the online hospital that I have gained a deeper understanding of diabetes, and my diabetes management has been ongoing. (P8, male, 60, diagnosed for 1 year, no complications) My family has actually provided some encouragement and assistance during my diabetes management. Sometimes, when my blood glucose levels are high, they remind me that I might have overeaten recently and need to pay more attention to my diet. (P11, male, 65, diagnosed for 25 years, with complications) Our community often organizes various activities, such as diabetes education, psychological counseling, and brisk walking. These activities not only bring the residents together for enjoyable experiences but also provide a platform for mutual encouragement and shared learning. (P18, female, 66, diagnosed for 9 years, with complications) As a fellow patient, Mr. Zhang frequently shares his insights on blood glucose control with me. We constantly encourage each other, remind each other to take our medications on time, and regularly monitor our blood glucose levels. Through our mutual support, I have successfully managed my diabetes, and my condition has significantly improved. (P8, female, 60, diagnosed for 1 year, no complications)
Theme 2: Barriers to Healthy Behaviors
Insufficient disease awareness
Insufficient disease awareness refers to an individual’s inadequate understanding of disease-related information, including failing to prioritize self-management behaviors, difficulty accepting their diabetes diagnosis, adjusting their dietary management to please others, and lacking awareness of the importance of self-management. Patients’ knowledge of diabetes is also influenced by the understanding of diabetes among family members, which, in turn, affects their self-management behaviors. Excessive self-consciousness may lead individuals to overlook practical constraints and real-life conditions, hindering effective diabetes self-management. Such cognitive deficiencies can result in delayed medical consultation, nonadherence to medical advice, or engagement in inappropriate health behaviors, ultimately impacting disease management and health outcomes.
I try my best to adhere to my medication schedule, but it becomes difficult to maintain when urgent matters arise. For example, when I am flying, the timing is beyond my control, and in such situations, I sometimes miss taking my medication. (P15, male, 67, diagnosed for 25 years, with complications) I was suddenly diagnosed with diabetes and have struggled to accept it ever since. I kept asking myself why I had to get diabetes, Before the diagnosis, I had no symptoms at all, and my health check-up two years ago showed no issues whatsoever. (P24, female, 41, diagnosed for 1 year, no complications) We have a little one at home who likes to eat pasta, so sometimes we cook it more frequently. When I eat pasta with broth, my blood glucose levels rise quickly. (P11, male, 65, diagnosed for 25 years, with complications) The doctor has consistently advised me to control my daily intake, but I don’t quite believe it. I think that no matter how much I control my diet, getting enough nutrition for my body is essential. Therefore, I haven’t really controlled my diet much. (P15, male, 67, diagnosed for 25 years, with complications) My mother had diabetes, but she didn’t take it seriously and didn’t manage it. So, when I was diagnosed with diabetes, I didn’t take it seriously either. (P9, male, 54, diagnosed for 15 years, with complications) I value freedom and believe that true life is about being free. I don’t think it is right to let a disease dictate what you can or cannot do in daily life, especially regarding eating and having fun. You should be yourself and do what you enjoy; that is the best way to live. (P15, male, 67, diagnosed for 25 years, with complications)
Insufficient self-control
Self-control refers to an individual’s ability to manage their behavior, emotions, and attention when faced with temptations, impulses, or pressure. Individuals often encounter greater obstacles in adjusting their lifestyles due to long-standing unhealthy habits, such as poor dietary preferences, lack of physical activity, and a mentality of thrift.
Sometimes, I can’t control my diet. When I encounter foods I particularly love, I often can’t resist and end up eating more than I should. (P4, female, 67, diagnosed for 14 years, with complications) I used to enjoy swimming, but I didn’t keep it up. I’ve had several gym memberships, but sometimes I was too busy and didn’t have time to exercise. When things got hectic, I couldn’t fit in workouts, so I didn’t stick with it. (P23, male, 61, diagnosed for 2 years, no complications) Sometimes when there is too much food at home, I worry about wasting it, so I eat more. This leads to an increase in my blood glucose levels. (P18, female, 66, diagnosed for 9 years, with complications)
Impact of social activities
When individuals participate in social activities, such as dining out, they are likely to break their regular eating habits. Especially when faced with the temptation of delicious food, participants often find it difficult to control their diet, which can hinder their adoption of healthy behaviors.
Occasionally, during gatherings with friends, I might eat a bit more and indulge myself. However, these social engagements are unavoidable, and I feel that I must attend. (P3, male, 53, diagnosed for 3 years, no complications)
Low self-efficacy
Self-efficacy refers to an individual’s assessment and belief in their own abilities, specifically, their confidence in achieving goals when handling a task or facing a situation. Due to the impact of their complications, patients can easily lose confidence in their self-management, manifesting as low mood and even susceptibility to depression. These factors can undermine their belief in effective health management, thereby affecting their healthy behaviors.
I have no confidence in managing diabetes in any aspect. I feel like no amount of money can treat this disease [sighs, with a frown]. (P24, female, 41, diagnosed for 1 year, no complications) I don’t think I can fully control my diabetes. Honestly, I am not very confident that I can manage it well or completely break away from these unhealthy lifestyle habits. I guess I have never really thought about making any changes. (P9, male, 54, diagnosed for 15 years, no complications)
Accessibility of personal conditions
The accessibility of personal conditions refers to an individual’s ability to obtain and utilize resources at various levels to promote healthy behaviors. This includes factors such as poor physical health status due to multiple reasons, lack of time, and the safety and accessibility of the individual’s physical environment. Furthermore, when a individual’s living environment changes, their inability to promptly adjust lifestyle habits and routines can hinder the initiation and maintenance of healthy behaviors.
Now, it is somewhat difficult for me to meet my exercise targets. I used to exercise regularly, such as walking and cycling. However, a period of excessive exercise led to joint injuries, which causes joint pain. Consequently, my exercise frequency has decreased compared to before. (P9, male, 54, diagnosed for 15 years, no complications) Currently, I mostly stick to walking and engage in fewer other types of exercise. This is primarily because I am getting older and suffer from leg bursitis, which causes leg pain and back pain, making me reluctant to move. (P12, female, 73, diagnosed for 4 years, with complications) If it rains, I don’t go out to exercise because I might get wet. I think it’s better to just stay at home. (P18, female, 66, diagnosed for 9 years, with complications) I went on a trip for about 20 days, and during that time, I couldn’t bring my insulin injections. As a result, I stopped taking them and haven’t resumed them since. (P16, male, 34, diagnosed for 1 year, no complications)
Lack of problem-solving skills
When individuals face problems or challenges, their inability to effectively identify issues, generate solutions, evaluate options, and implement actions can hinder healthy behaviors to a certain extent.
When it comes to diabetes, I always struggle with how to reasonably control portion sizes and choose the right foods. As a result, my blood glucose levels are either too high or too low. This is my biggest challenge, and I find it very difficult. (P4, female, 67, diagnosed for 4 years, with complications) Since being diagnosed with diabetes, it has significantly impacted my life. When I eat more, my blood glucose becomes difficult to control; when I eat less, I feel hungry. Therefore, the most troubling aspect for me now is managing my diet with diabetes. (P7, male, 60, diagnosed for 25 years, with complications)
Lack of disease management knowledge
Before engaging in diabetes management, patients should have a solid understanding of the disease. A lack of knowledge about the disease and self-management can cause confusion during the disease management process, leading to poor blood glucose control and significantly hindering the adoption of healthy behaviors.
When I was first diagnosed with diabetes, my understanding of diet was inadequate, and I took extreme measures. I thought that having diabetes meant I couldn’t eat anything, and I was afraid to eat, fearing it would raise my blood glucose levels. (P14, male, 62, diagnosed for 1 year, no complications) As nonprofessionals, we really don’t understand our condition very well. We can only describe the symptoms of diabetes but don’t fully understand the intricacies of the disease. Initially, I tried to learn more about it, but I didn’t persist. (P25, female, 50, diagnosed for 2 years, no complications)
Lack of social support
During disease management, insufficient support and resources from family, friends, community, or professional organizations can hinder patients’ ability to engage in healthy behaviors.
My spouse does not face the challenges of diabetes and blood glucose management with me. He only focuses on his own matters; he is very selfish, and our lifestyles are completely different. (P4, female, 67, diagnosed for 14 years, with complications) My family doesn’t understand much about diabetes, so I have to manage it on my own. They’re preoccupied with their own matters and don’t have time to support me. (P20, female, 50, diagnosed for 2 years, with complications)
Cognitive decline
As patients grow older, their cognitive functions may be affected to varying degrees, which can hinder their adherence to medication management.
As I get older, I sometimes forget things I need to do. Occasionally, if I wake up late in the morning or have to go out unexpectedly, I might forget to take my medication. (P12, female, 73, diagnosed for 4 years, with complications)
Conceptual Framework for Facilitators and Barriers of Healthy Behaviors in Patients With Diabetes
After analyzing the interview data, a conceptual framework of the facilitators and barriers to healthy behaviors in patients with T2D was extracted, as depicted in Figure 2. In the pre-intentional stage, perception of risk, outcome expectations, and action self-efficacy can promote the formation of behavioral intentions. Conversely, insufficient disease awareness, low self-efficacy, accessibility of personal conditions, and deficit disease management knowledge can impede the formation of behavioral intentions. In the intentional stage, sustaining self-efficacy aids in devising action plans and coping plans, thus promoting the initiation of healthy behaviors. During the action stage, emotional regulation and proactive and sustained sense of responsibility for disease management can foster the maintenance of healthy behaviors. On the other hand, insufficient self-control, the impact of social activities, lack of problem-solving skills, and cognitive decline can obstruct the maintenance of healthy behaviors. When individuals encounter setbacks in their healthy behaviors, recovery self-efficacy can help patients in resuming behavior change. Social support plays an indispensable role throughout the entire process of health behaviors.
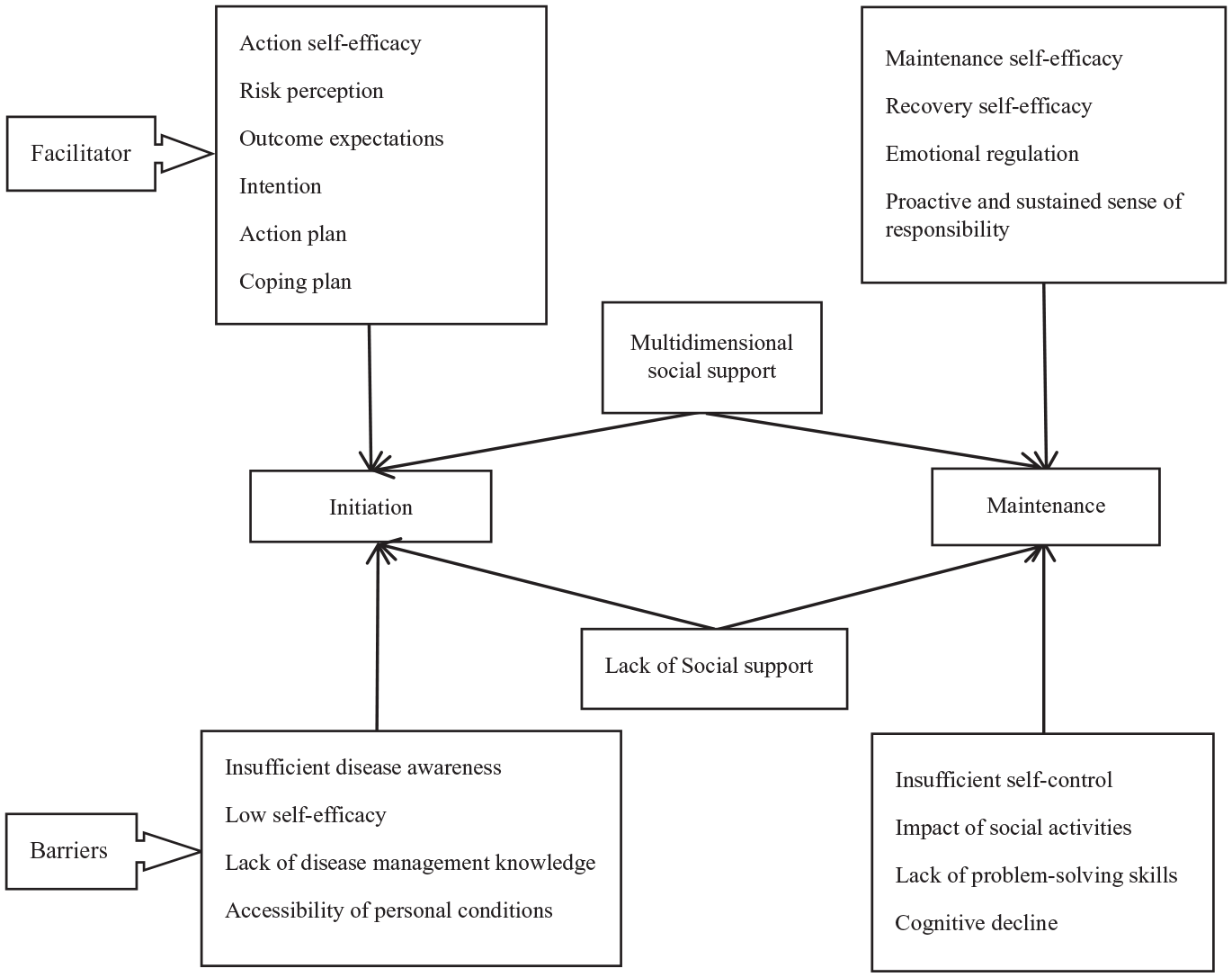
Conceptual framework for facilitators and barriers of healthy behaviors in patients with diabetes.
Discussion
Main Findings
This study employs a qualitative descriptive approach, conducting in-depth interviews with patients diagnosed with T2D to analyze the facilitators and barriers to their health behaviors. In this study, we conducted thematic analysis within the framework of the HAPA theory, which provides essential information for the initial data examination. Additionally, the method offers flexibility, allowing researchers to go beyond the theoretical framework, incorporating any information or descriptions outside its scope into the study results, thus ensuring a more comprehensive understanding of the factors influencing health behaviors. 32 Through analysis, 2 main themes and 18 subthemes were identified. Among the facilitators of health behaviors, risk perception, outcome expectations, self-efficacy, intention, action planning, and coping planning aligned largely with the HAPA framework; emotional regulation, a proactive and sustained sense of responsibility, and multidimensional social support emerged as new facilitators. Additionally, all barriers to health behaviors were newly identified, including insufficient disease awareness, insufficient self-control, impact of social activities, low self-efficacy, accessibility of personal conditions, lack of problem-solving skills, lack of disease management knowledge, lack of social support, and cognitive decline. These findings can serve as a reference for developing interventions aimed at promoting healthy behaviors in patients with T2D.
Comparison With Other Studies
This study found that the perception of risk can drive behavioral change in patients, which may help initiate healthy behaviors in those with T2D. Li et al 33 conducted a survey assessing both risk perception and self-management in middle-age and young patients with T2D. Their findings similarly demonstrated that the higher levels of risk perception in patients with T2D correlate with stronger self-management capabilities. However, other studies 34 have indicated that risk perception may not consistently encourage healthy behaviors among diabetic patients because their overall risk perception tends to be low, making it insufficient to instigate changes in their healthy behaviors. It is recommended that health care professionals (HCPs) educate patients on the risks associated with diabetes complications in the future and immerse them in firsthand experiences of these complications. This strategy could heighten patients’ awareness of health risks, thereby elevating their risk perception levels and consequently, bolstering their commitment to healthy behaviors.
In this study, outcome expectations played a crucial role in the formation of healthy behaviors in patients with T2D. If behavioral changes are anticipated to yield positive outcomes, they are more likely to foster the intention to engage in healthy behavior. Conversely, negative outcome expectations can impede the emergence of healthy behaviors. This finding aligns with the conclusions reached by Reisi et al, 35 who posited that if patients with T2D perceive these behaviors as yielding beneficial outcomes (enhancing positive consequences and minimizing negative consequences), they will exhibit greater motivation to adopt these behaviors. In forthcoming educational initiatives for patients with T2D, HCPs should highlight the benefits of adopting healthy behaviors and the harmful consequences of not doing so. This strategy would foster patient engagement in the proactive management of their condition.
This study found that self-efficacy can promote the initiation and maintenance of healthy behaviors among patients with T2D. The research by Xie et al 36 demonstrated a strong correlation between self-efficacy and compliance with self-management behaviors, including diet, physical activity, and medication regimens in T2D patients. Patients possessing higher levels of self-efficacy typically have greater confidence in their self-management capabilities, consequently, investing more effort into these practices. It is advised that HCPs routinely evaluate patients’ levels of self-efficacy. For patients exhibiting low self-efficacy, professionals may encourage them to reflect on past successes, thereby bolstering their confidence in their capabilities. Employing patients who have successfully managed their blood glucose levels as exemplars can reinforce their belief in their own capabilities. Furthermore, prompt positive reinforcement and support from health care providers acknowledging patients’ endeavors to adopt healthy behaviors can inspire continued commitment to a healthy lifestyle.
This study indicates that the formulation of health action plans and coping plans can facilitate the adoption of healthy behaviors among patients. This finding is consistent with the conclusions of studies by Ranjbaran et al 19 and Döbler et al, 37 which found that action plans and coping strategies are effective in improving patients’ health behaviors. It is advisable for HCPs to devise individualized health behavior plans that are customized to each patient’s unique circumstances. Throughout the implementation of these plans, HCPs should routinely monitor progress and adjust strategies in response to the patient’s evolving needs. Furthermore, strategies to overcome challenges should be developed to help establish healthy habits.
This study indicates that emotional regulation is a key factor in maintaining healthy behaviors during the action stage. Leukel et al 38 suggest that emotional regulation is a persistent process that requires continuous effort and practice from patients. Support from doctors, family, and nurses is also crucial because they can provide the necessary encouragement and guidance to enhance patients’ healthy behaviors. Nurses, in particular, play a significant role in educating and supporting these patients and their family members. It is recommended that HCPs regularly assess patients’ mental health and emotional states and provide personalized psychological support and interventions, such as cognitive-behavioral therapy and motivational interviewing. For patients with emotional issues, professionals should assist them in actively regulating their emotions and encourage them to seek and utilize social support to alleviate their psychological burden, helping them better adopt healthy behaviors. Additionally, HCPs can help patients develop self-management skills, such as stress management, time management, and problem-solving techniques, to improve their self-management capabilities in managing T2D.
Acquiring knowledge related to disease management is beneficial for patients with in self-managing their condition and reducing the incidence of complications. 39 This study found that the proactive acquisition of disease management knowledge by patients with T2D has a positive impact on their healthy behaviors. Fritschi et al 40 noted that for patients with low levels of diabetes management knowledge and physical activity, active learning can improve their knowledge of diabetes management, thereby enhancing their healthy behaviors. It is recommended that HCPs provide educational resources and encourage patients to actively learn about diabetes management to foster healthy behavior habits.
The study found that patients’ sense of responsibility for managing their diabetes is a significant factor influencing their healthy behaviors. Williams et al 41 conducted qualitative interviews with adolescent patients with diabetes, and their results indicated that the use of continuous glucose monitors enhanced the adolescents’ sense of responsibility for managing their disease. This improvement in responsibility enabled them to better adhere to diabetes care plans, manage their behaviors, and achieve better treatment outcomes. It is recommended that HCPs emphasize the importance of diabetes management to patients, reinforcing their awareness of being responsible for their own health and their critical role in disease management. This approach can enhance patients’ sense of responsibility for managing their disease, leading to improved treatment outcomes and management quality.
Social support can provide patients with T2D with more confidence to cope with and overcome the disease and to maintain healthy behaviors. In this study, social support is a promoting factor for healthy behaviors in patients with T2D. This finding is consistent with the results of Goins et al, 42 who conducted a qualitative study with 28 elderly individuals and found that patients can receive emotional, instrumental, informational, and appraisal support from family, professionals, community, and cultural sources. This support enhances patients’ motivation for disease treatment and promotes healthy behaviors. Otanga et al 43 pointed out that peer support can significantly improve the clinical outcomes of patients with diabetes during self-management. Onyango et al 44 conducted a cross-sectional study with 405 patients with diabetes in Eastern Uganda, showing that family support is positively correlated with diabetes self-management. It is recommended that HCPs fully mobilize the strengths of family members, medical staff, and the community to build a comprehensive support system. This approach can enhance patients’ sense of belonging and recognition, helping them better manage their health.
Disease perception refers to an individual’s understanding and feelings about their illness. Patients with T2D who hold a positive perception of their disease are more likely to adhere to healthy behaviors. 45 In this study, disease perception was identified as a significant factor influencing healthy behaviors in patients with diabetes. The study by Saudi et al, 46 also points out that cognitive misconceptions may lead patients to neglect the importance of self-management, thereby affecting the control of the disease and treatment outcomes. This cognitive misconception can lead to patients neglecting the importance of self-management, thereby affecting disease control and treatment outcomes. Therefore, it is recommended that HCPs assess patients’ perceptions of their disease and provide relevant health education. Strengthening patients’ awareness of risks and guiding them to correctly understand their disease can enhance their willingness to engage in healthy behaviors.
Self-control refers to an individual’s ability to exhibit rational judgment and behavior execution when faced with decisions. 47 This study reveals the importance of self-control in the health management of patients with T2D, finding that a lack of self-control often becomes a hindering factor in the implementation of healthy behaviors. Previous research supports this view, indicating that effective self-control in patients with diabetes significantly promotes disease management and reduces the risk of complications. 48 It is recommended that HCPs guide patients with diabetes in setting clear goals and plans. Tools such as mobile applications can assist patients with diabetes in self-monitoring, helping them enhance their self-control abilities, manage their disease more effectively, reduce the risk of complications, and improve healthy behaviors. Additionally, HCPs can use psychological interventions, such as cognitive-behavioral therapy, to help patients identify and change thoughts and behavior patterns that hinder self-control.
High-sugar, high-fat foods and irregular eating patterns, which are prevalent in social activities, can cause fluctuations in patients’ blood glucose levels, affecting their overall health. The challenges posed by social activities are not only about food choices but also about adhering to a healthy eating plan without harming interpersonal relationships. This study shows that social activities can influence patients’ dietary habits, making it difficult for them to stick to healthy eating plans in social settings. This finding is consistent with the results of Raghavan et al, 49 who found that social activities are associated with obesity, irregular eating patterns, reduced physical activity, and an increased risk of diabetes complications in patients with T2D. HCPs should assist patients in effectively communicating their health needs and boundaries during social interactions. They should teach patients strategies for making healthy food and drink choices in social situations and provide guidance on how to politely decline unsuitable food invitations.
This study indicates that the accessibility of individual resources has a significant impact on health behaviors among patients with T2D. Ratter-Rieck et al 50 also observed that patients with diabetes may struggle to maintain prior health behaviors when facing changes in their living environment. Similarly, Sharma et al 51 emphasized the influence of physical health status on exercise participation among patients with diabetes. Therefore, it is recommended that HCPs assess the physical environment surrounding patients’ residences when developing health management plans for those with T2D. Collaborating with community organizations to create exercise-friendly environments and improve community sports facilities is encouraged. Additionally, a comprehensive health assessment should be conducted, allowing for personalized exercise plans tailored to the patient’s specific conditions. This approach can help patients overcome physical-health-related exercise barriers, enhance exercise participation, and ultimately, improve blood glucose control and overall health outcomes.
Problem-solving ability, which refers to the capacity of individuals or teams to find effective solutions through analysis, thinking, and innovation when faced with complex situations or problems, is a critical skill. 52 The American Association of Diabetes Educators emphasizes that problem-solving ability is a core skill in diabetes self-management education. 12 This study indicates that insufficient problem-solving ability can affect the healthy behaviors of patients with T2D. Similarly, Wu et al 53 found that problem-solving ability is crucial for patients to successfully master self-management skills. It is recommended that HCPs regularly assess patients’ problem-solving abilities and understand the difficulties and challenges they encounter in disease management. Providing specialized training and guidance can help patients improve their problem-solving skills, thereby enhancing their capacity for effective self-management.
In this study, it was discovered that a lack of disease management knowledge among patients with T2D impacts their healthy behaviors. Nazir et al 54 posits that this lack of knowledge is a key factor contributing to poor adherence to treatment regimens. Implementing educational interventions can foster a deeper understanding of the disease, leading to improved adherence to treatment plans. HCPs are encouraged to develop targeted health education plans and engage in regular health education activities. Such initiatives can empower patients to better manage their disease and sustain healthy behaviors.
Cognitive decline is an age-related cognitive impairment that occurs in individuals whose cognitive functions decline beyond the normal range of aging. 55 The study found that cognitive decline hinders medication adherence in patients with diabetes. Ganmore et al 56 demonstrated that if cognitive function continues to decline in elderly patients with T2D, they will also experience a gradually deterioration of motor function, thereby affecting disease self-management. It is recommended that HCPs strengthen the screening for cognitive decline in elderly patients with diabetes. Measures such as cognitive training and lifestyle interventions can be implemented to slow the progression of cognitive decline and improve patients’ behaviors.
Strengths and Limitations
The participants in this study were drawn from diverse groups across different provinces and cities in China, providing us with a rich array of perspectives and enhancing the generalizability of our findings. However, there are some limitations to this study. Although the participants came from various regions within China, the sample did not include individuals from other racial and cultural backgrounds, which may limit the general applicability of our results. Additionally, the interviews were conducted via video through an online hospital platform, rather than in person, which could affect the quality and depth of the interactions. Furthermore, because the interviewer was conducting interviews for the first time, there may have been limitations in the depth of data collected and the interview techniques used.
Conclusion and Practical Implications
Guided by the HAPA framework, this study conducted semistructured interviews with 25 patients with T2D to identify the facilitators and barriers to their healthy behavior. The findings provide valuable information for HCPs to develop intervention programs aimed at enhancing patients’ adherence to self-management, thereby improving their quality of life and preventing complications.
In designing intervention programs for healthy behavior in patients with T2D, future efforts can adopt a stage-specific approach based on the stages of behavior change. In the initiation stage, interventions can focus on enhancing patients’ self-efficacy to boost their confidence in adopting healthy behaviors. It is essential to educate patients about the benefits of healthy behaviors and the risks of unhealthy ones. Highlighting the severity and likelihood of the risks associated with diabetes can also be beneficial. Providing standardized health education will foster a positive understanding of the disease, promoting the formation of intentions. It is important to consider the influence of patients’ health status and physical environment on their behavior. HCPs can guide patients in developing specific action plans based on their goals to encourage active participation in healthy behaviors. Creating coping plans to address potential barriers that might impede the implementation of healthy behavior is also essential. Moreover, HCPs can encourage the involvement of family members, the community, and peers in the patients’ management of their disease, which can provide significant support.
In the maintenance stage, it is vital to reinforce patients’ sense of responsibility for managing their disease and to encourage active learning about diabetes to enhance problem-solving skills. HCPs should guide patients effectively communicate their health needs during social activities and improve their self-control. Regular assessments of patient’s mental health and emotional states can aid in enhancing their emotional regulation and self-regulation. HCPs should screen elderly patients with T2D for cognitive decline and implement interventions to slow its progression. By adopting these stage-specific strategies, HCPs can significantly improve the self-management capabilities of patients with T2D, leading to better health outcomes and improved quality of life.