
Abstract
Purpose:
The purpose of the study was to evaluate the use of telemedicine for diabetes self-management education (DSME) for newly diagnosed youth and adolescents with type 1 diabetes on glycemic outcomes and health care utilization.
Methods:
A retrospective study of youth <18 years old receiving new-onset DSME between January 1, 2020, and September 30, 2022, was conducted. New-onset DSME includes teaching survival skills at diagnosis and advanced skills 7 to 10 days later, either in person or via telemedicine. A1C levels, readmission rates, emergency department (ED) visits, diabetes clinic visit attendance, and the probability of utilizing telemedicine for outpatient visits in the first year following diagnosis were compared between the in-person and hybrid groups using generalized linear models, adjusted by distance to the hospital.
Results:
Groups included 296 in-person and 246 hybrid participants. Baseline mean A1C improved 1-year post-diagnosis from 11.7% ± 2.1% (15.77 ± 3.27 mmol/l) and 11.8% ± 1.8% (15.93 ± 2.8 mmol/l) to 7.8% ± 1.7% (9.71 ± 2.64 mmol/l) and 7.8% ± 1.3% (9.71 ± 2.02 mmol/l) for in-person and hybrid groups, respectively, with no statistical difference after adjusting for baseline A1C and distance to clinic (difference: –0.06; P = .73). Groups did not differ significantly in ED visits (odds ratio [OR] 0.67; P = .33), readmission rates (OR 0.58; P = .35), or clinic visit attendance (incidence rate ratio 0.97; P = .46). After adjusting for distance from the nearest diabetes clinic, the hybrid group had 89% higher odds of completing a visit via telemedicine (P < .001).
Conclusions:
New-onset DSME via telemedicine is a reasonable alternative to in-person education. Ongoing engagement with telemedicine suggests this modality may help reduce barriers to care.
International clinical practice guidelines recommend that shortly after the diagnosis of new-onset type 1 diabetes mellitus (T1D), youth with new-onset T1D and their caregivers should be provided with age-appropriate and comprehensive diabetes self-management education (DSME) that facilitates successful self-management of diabetes in an outpatient setting.1,2 New-onset DSME involves learning about glucose monitoring and glycemic targets, insulin dose calculations and administration, management of hypoglycemia and hyperglycemia, carbohydrate counting, diabetes care in an early childhood or school setting, and how to manage diabetes when ill or doing physical activity. 2 It occurs at the critical time of diabetes diagnosis and sets the foundation for future education and diabetes management. Comprehensive new-onset DSME requires a multidisciplinary approach and includes pediatric endocrinology providers, a certified diabetes care and education specialist, registered dietician, social worker, and child life specialist to provide education and psychosocial support in a developmentally appropriate format.1,3 Although studies have described new-onset DSME in both the inpatient and outpatient settings, 2 studies on the utilization of telemedicine for new-onset DSME are lacking.
Ambulatory care delivered via telemedicine has been shown to be highly effective for those living with T1D, but most of these studies exclude individuals with new-onset T1D.4 -6 A meta-analysis of 38 randomized controlled trials on the effectiveness of telemedicine in T1D care found an average A1C reduction of 0.18 percentage points; however, the telemedicine visits occurred 5.7 to 18.9 years after initial diagnosis. 4 In addition, telemedicine has been shown to increase patient interactions with their diabetes team and diabetes clinic visit attendance. 7 People with T1D report several benefits of telemedicine for diabetes clinic visits, including personal convenience, time and cost savings, and less time away from work and school.7 -9
There is little known about the safety or efficacy of utilizing telemedicine for new-onset DSME. Case reports have described using telemedicine for ongoing DSME during the COVID-19 pandemic after initial new-onset DSME was completed in person.10,11 One case report conducted all new-onset DSME via telemedicine for a child in isolation due to COVID-19 infection. 12 These small case reports show that new-onset DSME via telemedicine is feasible; however, the efficacy of education and longitudinal impacts on glycemic outcomes, health care utilization, and safety in children, adolescents, and adults are unknown.
The aim was to compare glycemic outcomes and health care utilization for youth receiving new-onset DSME completely or partially through telemedicine versus solely in-person education. The hypothesis was that at 1-year post-T1D diagnosis, there would be no differences in A1C levels, emergency department (ED) visits, readmission rates, or number of diabetes clinic visits for youth receiving at least part of their new-onset DSME via telemedicine (hybrid group) compared to in-person education. The probability of utilizing telemedicine visits for ongoing care based on initial modality used for education was also assessed.
Methods
Study Design
A retrospective chart review was performed of youth <18 years old with new-onset T1D who completed new-onset DSME between January 1, 2020, and September 30, 2022. Since our primary aim was to examine the association between incorporation of telemedicine in new-onset DSME implemented in January 2020 and health care outcomes using routinely collected clinical data, a retrospective design was chosen.
Sample
Participants were identified by a clinical registry of new-onset T1D patients receiving new-onset DSME at the home institution. Inclusion criteria were age <18 years old with new-onset T1D as evidenced by at least 1 positive pancreatic autoantibody and who completed new-onset DSME at the home institution. Exclusion criteria were type 2 diabetes mellitus, age ≥18 years old, and those who received new-onset DSME at outside institutions, due to differences in education timeline, modality, and the composition of the education team.
Setting: New-Onset Diabetes Education Program Description
The diabetes center is part of a tertiary care, urban freestanding children’s hospital with a 5-state referral base. Multidisciplinary new-onset DSME occurs primarily in the outpatient setting at the urban main campus clinic. It includes part 1A, focused on survival skills at the time of initial diagnosis, followed by part 1B, teaching advanced skills 7 to 10 days later (Figure 1). Part 1A education is a full 8-hour day with a pediatric endocrinology provider, a certified diabetes educator, registered dietician, social worker, and child life specialist. It may occur in an inpatient setting, depending on the presence of diabetic ketoacidosis (DKA), other comorbidities requiring admission, patient/caregiver preference, and clinic availability of outpatient education. Part 1B education is a half-day of education with a pediatric endocrinology provider, a certified diabetes educator, registered dietician, and social worker and mostly occurs via telemedicine set up as synchronous videoconferencing but may be completed in person based on duration of hospitalization or family preference. The certified diabetes educators, registered dieticians, social workers, and child life specialist specialize in diabetes DSME and spend over 75% of their time working with diabetes patients. The content and structure of part 1A and part 1B education is the same regardless of how or where it is delivered. Ambulatory diabetes care is provided at the main campus clinic and 7 regional sites throughout the state.
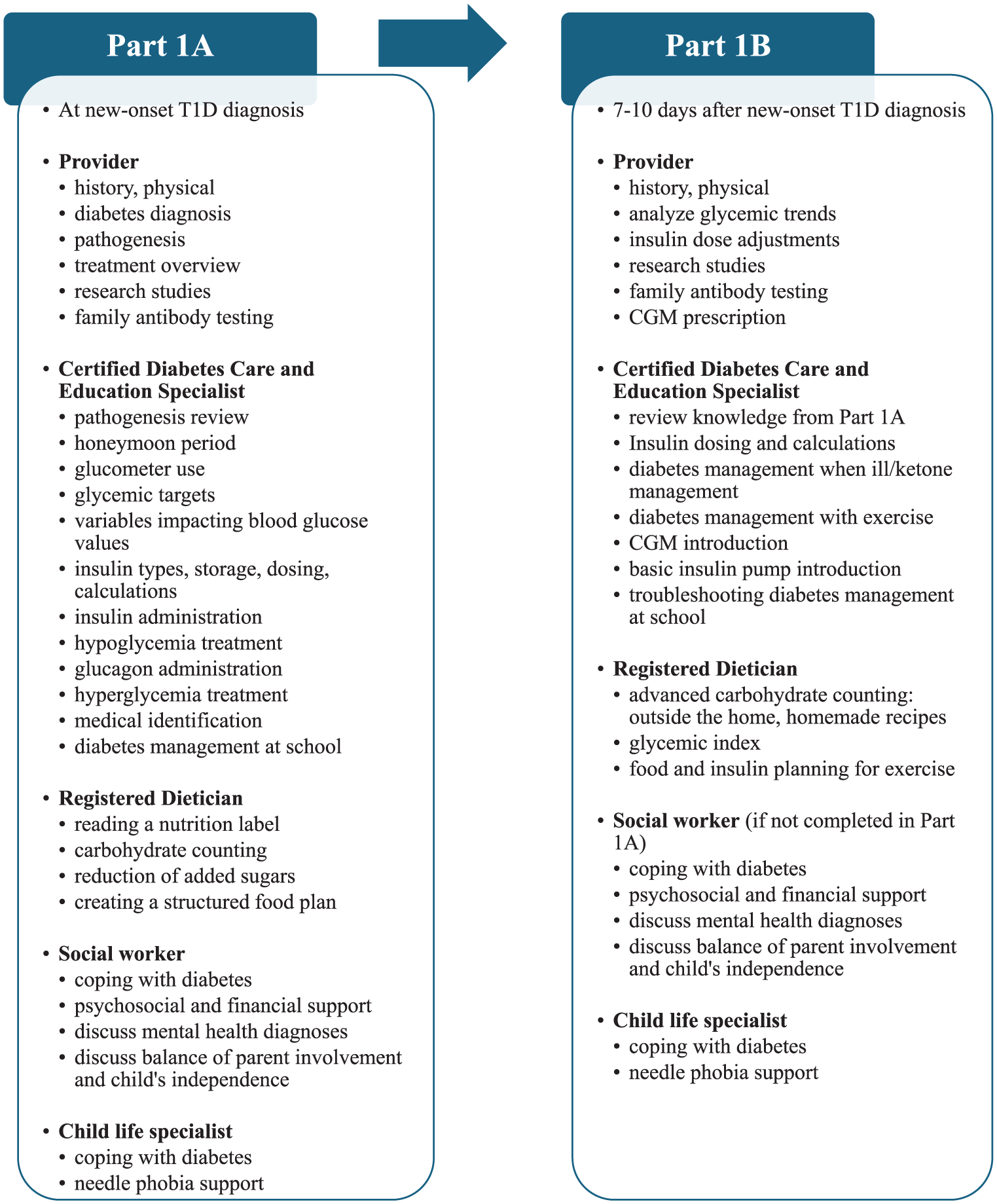
Components of the new-onset T1D DSME program.
Study Groups
Two groups were compared: in-person only education and hybrid education, where at least 1 part of new-onset DSME (part 1A or part 1B) occurred via telemedicine. As described previously and in Figure 1, the structure, content, and educators are the same for part 1A and part 1B education regardless of delivery via in-person or telemedicine modality. The majority of the hybrid group received part 1A in person, except for special circumstances during the peak COVID-19 pandemic, and part 1B via telemedicine. Baseline data were collected at time of T1D diagnosis. Distances to the nearest diabetes clinic and hospital were measured by straight line.
Measures
Patient-reported sociodemographic variables and A1C levels at baseline and 1 year ± 3 months post-diagnosis were collected from the electronic health record. Additional variables included hospital readmission rates, ED visits for DKA or hyperglycemia with ketosis, and number of diabetes clinic visits, both in person and telemedicine, in the first year after new-onset DSME.
Statistical Analysis
Sociodemographic variables were summarized using descriptive statistics. Logistic regression with Firth’s bias correction was used to examine the outcomes of ED visits, readmission rates, and the odds of using telemedicine for diabetes clinic visits; the latter results are also presented in figures as marginal effects on the probability scale. Poisson regression was used to examine the number of diabetes clinic visits. Tobit regression was used to compare change in A1C level from baseline to 1 year; only youth who had a baseline and a 1-year (±3 months) A1C level were included, and those levels were right censored at 14% (19.35 mmol/l). All models except number of diabetes clinic visit counts were adjusted for distance in log-miles from the nearest diabetes clinic (A1C change, telemedicine use for diabetes clinic visits) or from the hospital (readmission rates, ED visits). Statistical analysis was conducted with R version 4.4.
Results
Study Population Characteristics
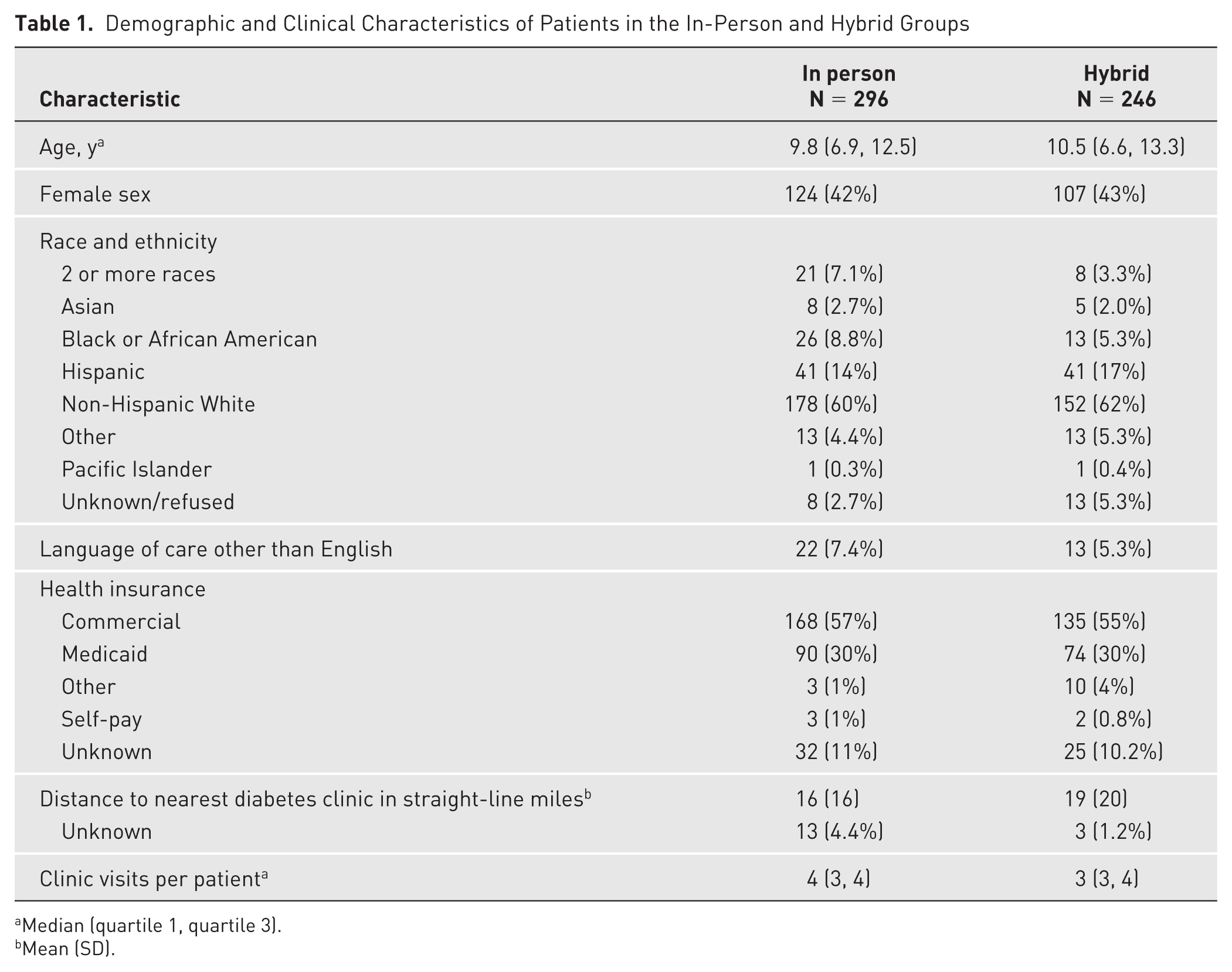
Of the 296 youth in the in-person group, 42% were female, 60% were non-Hispanic White, 7.4% had language of care other than English, and the median age was 9.8 years; of the 246 hybrid subjects, 43% were female, 62% were non-Hispanic White, 5.3% had language of care other than English, and the median age was 10.5 years. Both the groups were similar in terms of distribution by type of health insurance and distance to the nearest diabetes clinic (Table 1).
Demographic and Clinical Characteristics of Patients in the In-Person and Hybrid Groups
Median (quartile 1, quartile 3).
Mean (SD).
Clinical Outcomes
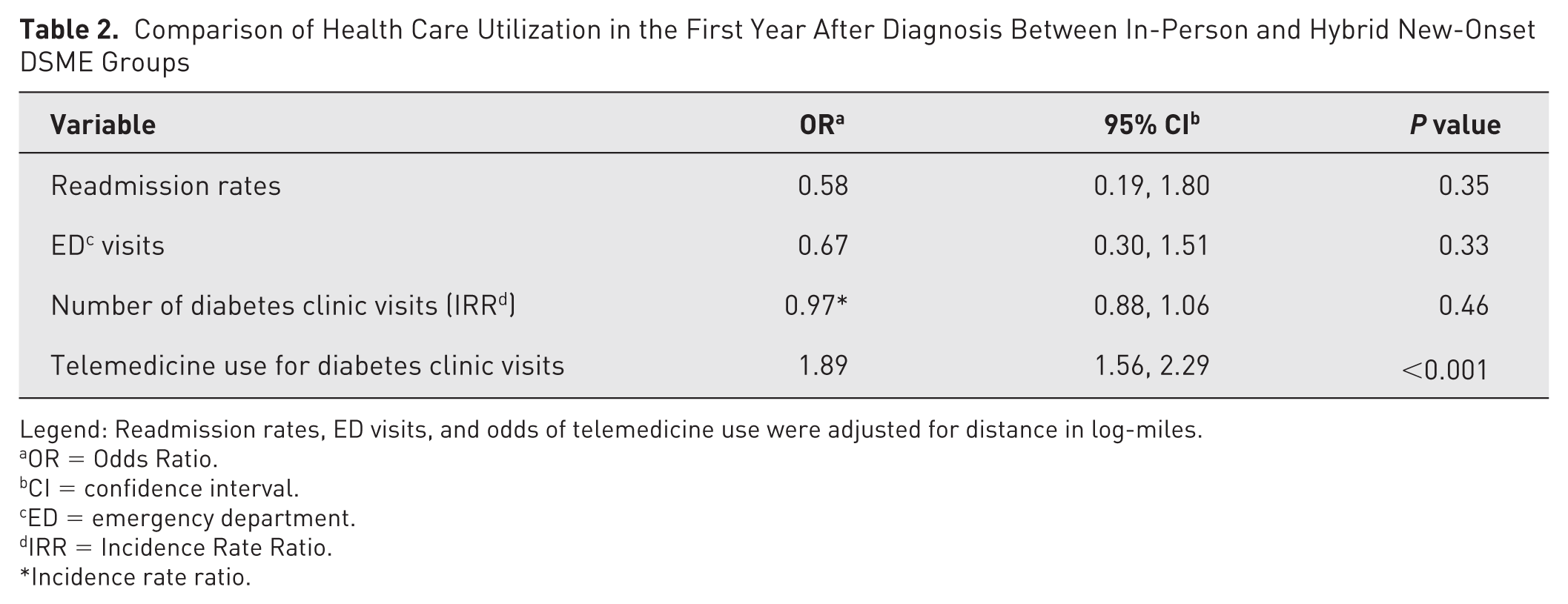
The A1C analyses included 185 in-person and 134 hybrid participants. Baseline mean A1C improved 1-year post-diagnosis from 11.7% ± 2.1% (15.77 ± 3.27 mmol/l) and 11.8% ± 1.8% (15.93 ± 2.8 mmol/l) to 7.8% ± 1.7% (9.71 ± 2.64 mmol/l) and 7.8% ± 1.3% (9.71 ± 2.02 mmol/l) for in-person and hybrid groups, respectively. When adjusted for baseline A1C and distance from nearest diabetes clinic, there was no significant difference in 1-year post-diagnosis A1C between the in-person and hybrid groups (difference: –0.06 percentage points; 95% CI, –0.28 to 0.41; P = .73; Figure 2). There were no significant differences in the rates of ED visits (odds ratio [OR] 0.67; P = .33) or readmission rates (OR 0.58; P = .35) between the in-person and hybrid groups (Table 2).
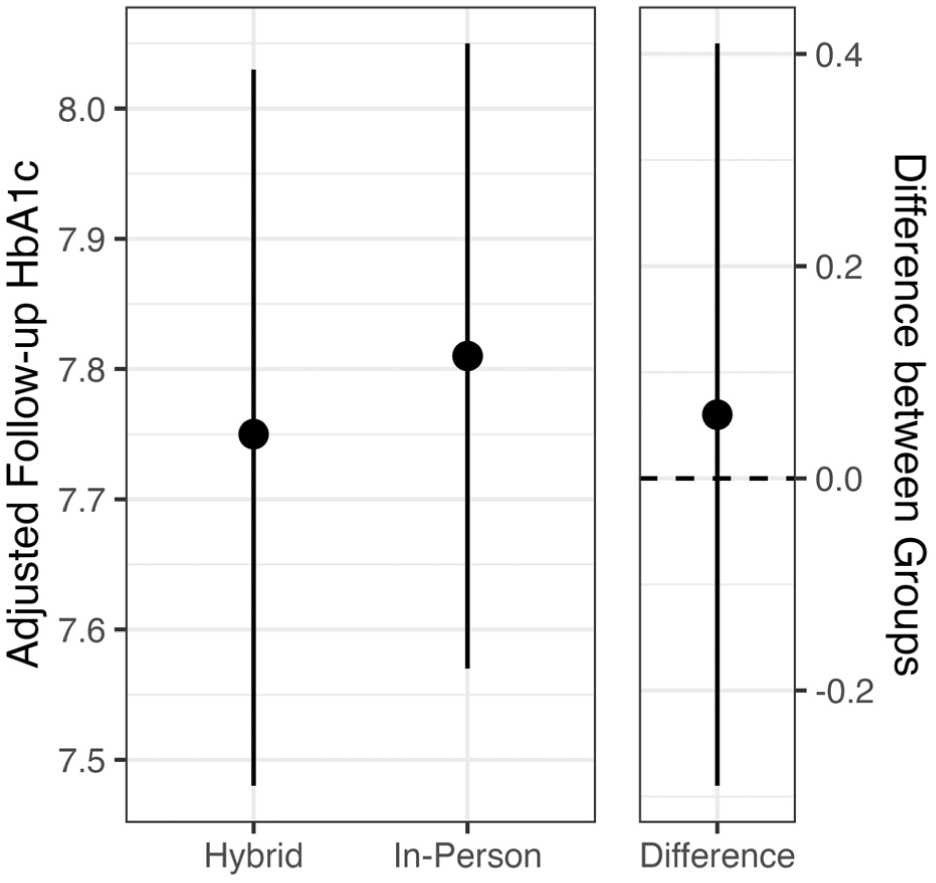
Change in A1C from baseline to 1-year post-diagnosis based on education group and adjusted for distance from nearest diabetes clinic.
Comparison of Health Care Utilization in the First Year After Diagnosis Between In-Person and Hybrid New-Onset DSME Groups
Legend: Readmission rates, ED visits, and odds of telemedicine use were adjusted for distance in log-miles.
OR = Odds Ratio.
CI = confidence interval.
ED = emergency department.
IRR = Incidence Rate Ratio.
Incidence rate ratio.
Clinic Visit Engagement and Modality
Number of diabetes clinic visits in the first year post-diagnosis did not significantly differ between the in-person and hybrid groups (incidence rate ratio 0.97; P = .46; Table 2). The hybrid group had 89% higher odds of completing a clinic visit via telemedicine compared to the in-person group when adjusted for distance from the nearest diabetes clinic (OR 1.89; P < .001; Figure 3).
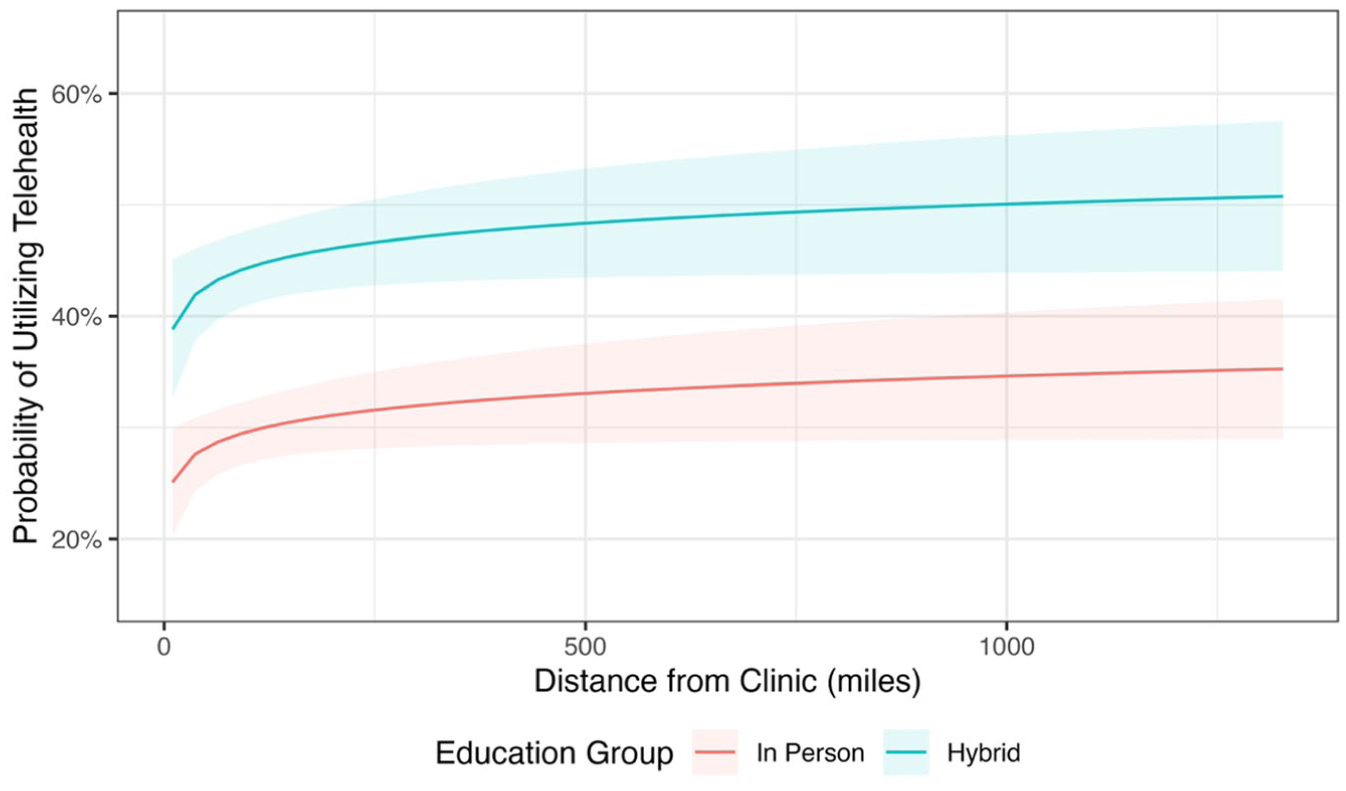
Probability of telemedicine use for diabetes clinic visits by education group and distance to the nearest diabetes clinic.
Discussion
This is one of the first studies to examine the impact of new-onset DSME delivered via telemedicine compared to in-person education on glycemia and health care utilization. In this retrospective study, there were no differences in A1C levels approximately 12 months after diagnosis, frequency of ED visits, or readmission rates between in-person and hybrid new-onset DSME groups. Although the number of diabetes clinic visits in the first year post-diagnosis did not differ, the hybrid group had 89% higher odds of completing diabetes clinic visits via telemedicine.
Several studies have established that new-onset DSME in the outpatient setting is safe and cost-effective compared to inpatient education.13,14 Conducting new-onset DSME in 2 separate sessions is beneficial because it allows time for patients and caregivers to practice skills at home. 13 However, multiple in-person clinic visits for education often require families to travel long distances and thereby limit access to care. 7 To ensure access for the large referral base that the diabetes center serves, a transition was made to increase telemedicine utilization not just for ambulatory care but for comprehensive new-onset DSME as well. Use of telemedicine for new-onset DSME also allowed participation of multiple caregivers from different locations.
Globally, surveys of individuals with T1D or their caregivers have reported high levels of satisfaction with using telemedicine in routine diabetes care. Perceived benefits include effectiveness comparable to or better than in-person visits, reduced time and financial burden, greater convenience, more flexibility, and less time away from work and school.7 -9,15 New diagnosis of diabetes is often stressful and overwhelming for youth and their families. 16 Integrating telemedicine in new-onset DSME could extend these benefits to this particularly vulnerable period by improving accessibility and affording patient-centered care.
Studies evaluating use of telemedicine or hybrid models specifically for DSME have been conducted in adults with diabetes and have shown comparable efficacy to in-person education 17 and 2.59 percentage point reduction in A1C levels in adults with uncontrolled type 2 diabetes. 18 However, mean duration of diabetes in these studies ranged from 11 to 13 years. Data on telemedicine utilization for new-onset DSME in youth with T1D is limited to small case reports (n = 1-8 patients) with minimal follow-up period of an average of 47 days.10 -12 In contrast, this study assessed 1-year outcomes for a large, multistate-based patient population completing new-onset DSME. The 1-year A1C levels in this study are similar to average A1C values (8.0% ± 1.7%; 10.02 ± 2.64 mmol/l) 1 year after new-onset T1D diagnosis in American youth. 19 Moreover, the baseline and distance-adjusted 1-year post-A1C levels did not differ between the in-person and hybrid groups, indicating that incorporating telemedicine in new-onset DSME likely had comparable efficacy to in-person education.
ED visits and readmission rates were used to assess the safety of telemedicine new-onset DSME. The finding that the odds of having an ED visit or being admitted to the hospital were not significantly different between the 2 groups suggests that youth who receive new-onset DSME virtually may not be any more at risk of acute diabetes-related complications as those who receive in-person education.
Equal engagement was noted in diabetes clinic visits in the first year after T1D diagnosis for those who received in-person and hybrid education. Prior studies have demonstrated an increase in diabetes clinic visits, approaching the goal of 4 visits per year, after introduction of telemedicine to routine diabetes care. 7 Bassi et al, 20 who surveyed youth with T1D and their families on the impact of telemedicine, found notably higher satisfaction levels in families living farther from diabetes clinic. In this study, the probability of ongoing utilization of telemedicine was significantly higher in the hybrid group even after adjusting for distance from the nearest clinic. This stark difference may indicate that earlier introduction of telemedicine in their diabetes care led to a favorable perception of this modality and that ongoing use was not just a matter of convenience.
This study has strengths in its large and diverse sample size, adjustments for baseline A1C levels and distance from diabetes clinics, and a follow-up period of 1 year after initial new-onset DSME. These findings are limited by retrospective design at a single institution and a lack of data on long-term clinical outcomes including diabetes complications, such as nephropathy, retinopathy, and dyslipidemia. Although ED visits and readmission rates were assessed only at the home institution, rates were adjusted for distance from the hospital to account for youth who lived farther away and may seek care closer to home. The generalizability of this education model may be limited by institutional resources and infrastructure for utilizing telemedicine and trained multidisciplinary staff. Future work should include long-term examination of metabolic outcomes, complications, health care costs, and patient/family satisfaction with telemedicine new-onset DSME.
Conclusions
The integration of telemedicine into ambulatory diabetes care offers new opportunities for the delivery of new-onset DSME to youth and their caregivers, extending the established benefits of telemedicine to this critical time of diabetes diagnosis. In this study, hybrid new-onset DSME that included telemedicine had comparable 1-year outcomes to in-person DSME. The findings suggest that adapting new-onset DSME programs to incorporate telemedicine and hybrid modalities should be considered as a reasonable alternative to in-person DSME, allowing more flexibility for patients, families, and DSME care teams and thus improving access to care.
Footnotes
Authorship
Kelsel Eitel contributed to the study design, interpretation of data, and drafted the manuscript and revisions. Meenal Gupta conceptualized the study design, analysis plan, and supervised the conduct of the study and manuscript preparation. Yasi Mohsenian contributed to data collection, review, and critically reviewed the manuscript. Joy Briggs and Alissa Roberts provided critical review and substantive revisions of the manuscript. Faisal Malik contributed to the study design and provided critical review and intellectual input on manuscript revisions. All authors approved the final version of the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Ethical Considerations
This study was conducted as part of quality improvement and considered exempt from institutional review board review.
Data Availability Statement
This study was conducted as part of quality improvement, and thus data cannot be shared.