
Abstract
Purpose:
The purpose of the study was to assess a culturally tailored, family-focused diabetes self-management education and support intervention with community health worker (CHW) support among Black families with prediabetes and diabetes.
Methods:
The study enrolled 70 Black family members and assigned them CHWs for a 20-week diabetes prevention and self-management education and support intervention. Family members and CHWs were interviewed, and thematic analysis identified 4 themes associated with family-CHW dynamics that affected program outcomes: (1) family and CHW communication, (2) health literacy support, (3) technology support, and (4) program adherence support. The communication dynamics were bidirectional, and the health literacy, program adherence, and technology support flowed from CHWs to families.
Results:
Participants appreciated that their CHWs were empathetic, relatable, adaptable, and good communicators, and both families and CHWs spoke of strong emotional and task-based bonds. CHWs’ positive impact on adherence was confirmed. Data on health literacy and technology support activities identify families’ additional needs to be successful in these programs.
Conclusions:
The study results on family-CHW dynamics add to the literature on family-based diabetes prevention and self-management education and support programs and the limited literature on how participants and CHWs interact, communicate, and share information during lengthy chronic disease programs. Expanding the public health impact of diabetes programs for Black adults may come from innovations in family-based programs supported by positive CHW interactions.
Introduction
Type 2 diabetes is a multigenerational, multipronged disease, and a family history of type 2 diabetes is one of the strongest predictors of receiving a diagnosis. 1 Researchers have proposed that the role of families in diabetes management and outcomes needs more scholarly attention.2 -4 A core strength within Black families is “strong kinship bonds and extended family relationships.” 5 This strength can positively impact health behaviors within families. Focusing research and prevention efforts at the family level offers the opportunity to address the disproportionate rates of diabetes that Black adults experience.
Evidence-based lifestyle change and diabetes self-management education and support programs are effective in helping individuals reduce the risk of developing diabetes and experiencing the worst complications when living with diabetes. 6 Despite program effectiveness, only a small proportion of people eligible for the programs enrolls and completes the programs, which limits their public health impact and motivates the need for program innovation. A 2024 systematic review identified 4 studies that used innovative family-based approaches to diabetes lifestyle change programs, with 2 studies showing positive intervention results and 2 studies showing no intervention effects. 7 Sorkin et al8,9 tested family partner participation in lifestyle change programs and reported positive results in program retention, completion, and meeting program goals. Ritchie et al 10 found that people from the same household who enrolled in the National Diabetes Prevention Program were more likely to attend sessions and remain in and complete the program. A 6-site Maryland-based study of diabetes Lifestyle Change Programs found people who joined with a family or friend partner were motivated and successful and had higher program success rates. 11
Family members are not the only source of support for people trying to prevent or manage diabetes. Community health workers (CHWs), who are clinical and public health field workers like or from the communities where they work, can be part of teams for diabetes prevention and self-management programs. 12 Functionally, among other activities, CHWs provide education and resources to program participants; refer participants to resources, including health care providers; and help implement interventions.13,14 In addition to this material support, researchers note that the bond or “therapeutic alliance” that CHWs build with clients creates trust and may improve clients’ program participation and completion. 15
Multiple studies have examined the impact of CHWs on diabetes program outcomes, but few studies have examined how clients and CHWs interact during a program and build relationships to achieve these outcomes.12,16 CHW-client interactions can include communicating about the program; sharing information about experiences, challenges, progress, and resources; and problem-solving to be successful in the program. Because diabetes prevention and self-management education and support programs last several months, the CHW-client dynamic may be a key factor in helping clients meet personal and program goals. A CHW interview study on their trust-building and communication practices during the COVID-19 pandemic in the United States concluded that CHWs spend significant time on relationship cultivation, active and empathetic listening, and demonstrating care and concern for the community members they work with. 17
The study reported in this article was a pragmatic trial of a culturally tailored, family-focused diabetes self-management education and support intervention with CHW support for Black families with prediabetes and diabetes. The study team conducted a thematic analysis of family and CHW interview data to understand the dynamic between the families and CHWs and how this dynamic might have affected study outcomes of weight loss, physical activity, healthy eating, medicine and testing adherence, self-efficacy, intrafamily communication, beliefs about diabetes, and awareness of and readiness to change environmental influences.
This article summarizes the thematic analysis and reports 4 themes that capture the Black families’ and CHWs’ interactions: communication, health literacy, technology, and program adherence during the diabetes intervention. In response to the call for research on CHW-client interactions, 13 these data provide new insights about how culturally matched Black family participants and CHWs interacted during a diabetes intervention, what participants valued about CHWs, and what CHWs can do to facilitate participants’ success in diabetes prevention and management programs.
Methods
Study Design
Between 2021 and 2024, the study team implemented a novel intervention called “Black Families Defying Diabetes Together” (BFDDT) with Black families in the metro Washington, DC/suburban Maryland/northern Virginia area. The intervention is based on the Centers for Disease Control and Prevention (CDC)-approved National Diabetes Prevention Program Lifestyle Change Program and an American Diabetes Association (ADA)-accredited diabetes self-management education and support program, both delivered virtually over 20 weeks. The study team supplemented these programs with original culturally relevant materials to support intrafamily communication and support.
The BFDDT study was a nonrandomized pragmatic trial with an intervention group of enrolled Black families who participated in the diabetes prevention and self-management education and support programs and worked with their assigned CHWs and a control group with enrolled individuals who did not have CHWs. The community organization employed 7 CHWs in total, with 4 assigned to families at any one time. Their purpose was to facilitate intrafamily communication about program activities, respond to questions and concerns, and generally encourage family members to complete the BFDDT program. The study team provided CHWs with a guide that described roles and responsibilities and provided directions and templates about how to communicate and interact with families during the intervention. The study design included 2 virtual discussion sessions on culturally relevant topics (intervention weeks 1 and 3) and at least 5 virtual check-in meetings (intervention weeks 5, 7, 9, 14, and 19) between families and their assigned CHW during the intervention, which CHWs scheduled directly with the families. Families called and texted their CHWs outside scheduled meetings, although this was not in the original study design. This article is about the intervention group with families and assigned CHWs and the qualitative interview data that the team collected about the family and CHW interactions and experiences during the intervention.
Sample and Recruitment
Eligible study participants were self-identified Black families in the metro Washington, DC/suburban Maryland/northern Virgina area and consisted of 1 family member with a diabetes diagnosis and 1 to 2 family members at risk of diabetes. Family members could be biological or chosen family. Using these criteria, the community organization used its partnership networks to recruit convenience samples for 3 waves from November 2022 to April 2023. Possible participants were referred from partnering physicians’ offices in the metro Washington, DC/suburban Maryland/northern Virginia area and from a community-based residential program whose residents participated in the organization’s remote patient monitoring intervention. Additional recruitment occurred at community health screenings at churches, senior centers, residential facilities, and community events during which CHWs asked individuals if they met eligibility criteria and then provided information about enrollment procedures and program objectives. The BFDDT project manager also attended targeted screenings and distributed program and diabetes-related materials to support recruitment. The program manager and CHWs presented at churches in collaboration with health ministry leaders who assisted in identifying potential participants. Existing classes offered by the organization provided another recruitment venue; announcements were delivered at the start of each class, and digital flyers with a QR code linking to the program website were displayed and sent with class recordings. Text messages and email blasts followed by follow-up telephone calls were also used. Daily staff meetings further supported recruitment by disseminating materials and identifying community events suitable for outreach. Families were recruited in 3 waves and assigned to the cohort that was open at the time of their recruitment.
Intervention Content and Team
In addition to the CDC- and ADA-approved content, the study team created and provided families and CHWs with supplemental materials to promote intrafamily discussions about health generally and diabetes specifically. The family-CHW interactions emerged as a factor affecting the primary outcomes, which prompted the thematic analysis of interview data about their interactions.
The project team included a nonprofit research agency; an academic team from 2 universities composed of health communication, health literacy, and Black cultural and family studies experts; and a community-based organization that provides information, programs, and services for Black residents in Montgomery County, Maryland, and Washington, DC.
Outcome Measures
The primary behavioral outcomes were weight loss, amount of physical activity, healthy eating, and medicine and testing adherence; increase in self-efficacy was a health belief outcome; positive intrafamily communication about diabetes was a family communication and dynamics outcome; positive beliefs about preventing and managing diabetes were a family attitude outcome; and awareness of and readiness to change environmental influences on diabetes were environment and diabetes outcomes. A secondary outcome was positive family-CHW dynamics.
Data Collection
To understand family-CHW dynamics, the research team conducted a series of 3 separate semistructured interviews with each CHW and most families in 2023. During the intervention period, each family was assigned 1 CHW. Families participated in the interviews together, and they were interviewed separately from CHWs. This approach allowed for various perspectives of the intervention and reduced the chance that each group’s responses influenced the other. Each of the 3 interviews asked participants about their CHW and family interactions and their response to intervention content until that point in the intervention.
The research team developed the family and CHW interview guides based on the academic literature on prior diabetes prevention and management programs, CHWs’ client support roles in other diabetes programs, family systems theory, and evaluation models that centered race, culture and equity. Data collection was conducted by 2 research team members with expertise in qualitative study designs, community engagement, and semistructured interviews and focus groups. Both team members had worked with communities of color, specifically focusing on health equity and health disparities in public health practice and research within Black adult populations. This research background offered a culturally responsive approach to the interviews to foster trust in facilitating discussions on sensitive topics.
Interviews were up to 90 minutes in length and conducted virtually through the Zoom video conferencing platform. All sessions were audio-recorded including transcription. Each family member and CHW received a $50.00 electronic gift card per interview completed. The study was approved by the FHI 360 Office of International Research Ethics.
Data Analysis
Research team members extracted the interview data from Zoom-recorded transcripts and used spreadsheets to organize family and CHW responses by interview question. The first and second authors of the article applied an inductive approach to a thematic data analysis based on the interview questions. To ensure intercoder reliability, the 2 coders independently coded the data and then discussed and reviewed the codes. Four rounds of reconciliation occurred until both coders agreed on the final data set. The first and second authors proposed 4 themes based on their analysis of the data, and all authors and the CHWs involved in the intervention reviewed and confirmed the themes.
Results
The results are organized by family and CHW demographics and the 4 themes that the research team identified in the interview data. Each section heading in Results is a theme.
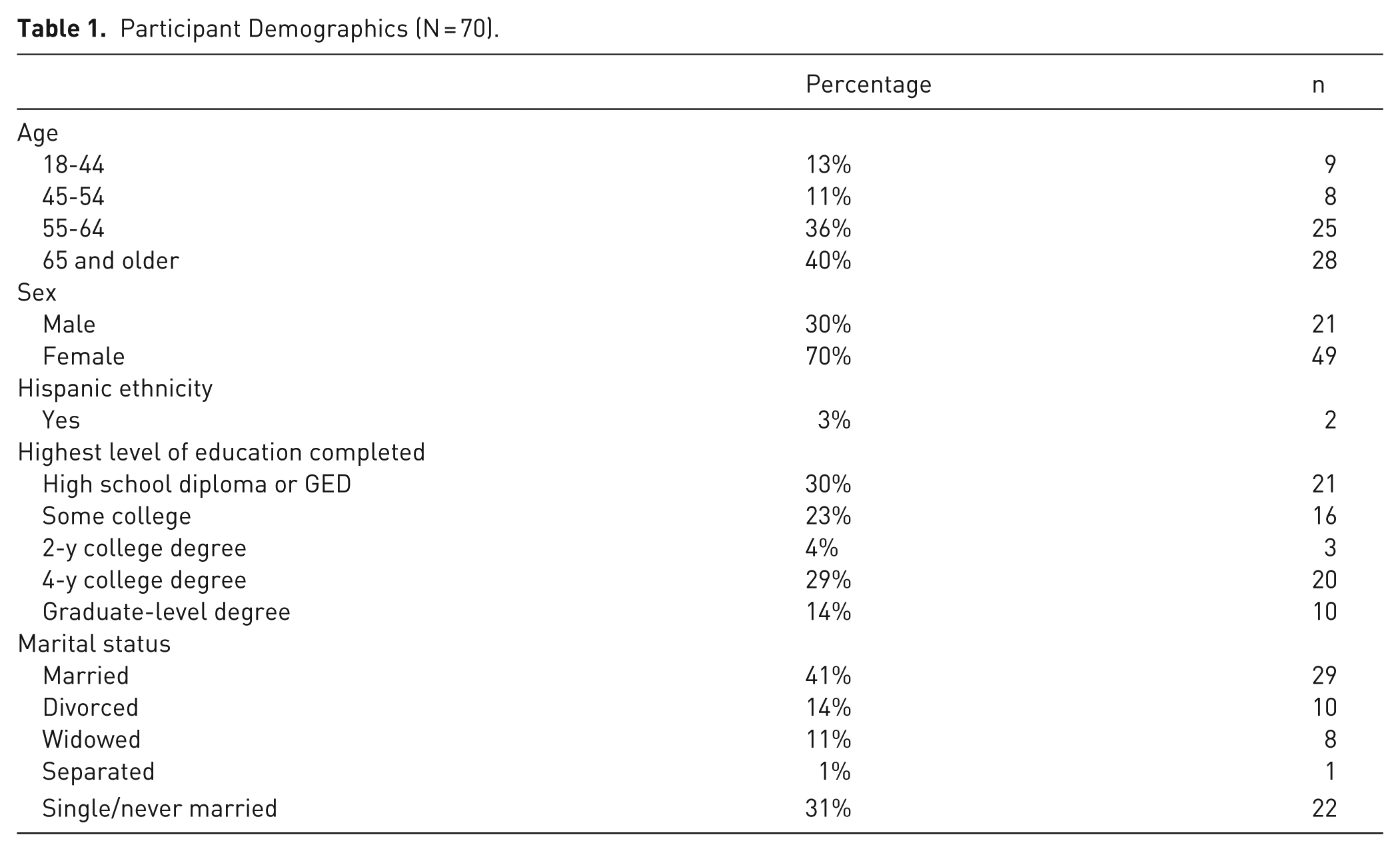
Seventy people enrolled in the intervention, and 64 (91%) completed it. Of the 70 participants, 34 had diabetes, and 36 were family members at risk of diabetes. Participant demographics are in Table 1. The study included up to 7 Black CHWs employed by the community organization, and their demographics are reported in Table 2. Three of the 7 CHWs left the intervention at different time points and were replaced by new CHWs.
Participant Demographics (N = 70).
CHW Demographics (Based on 4 of the 7 CHWs Who Worked Longest in the Program).
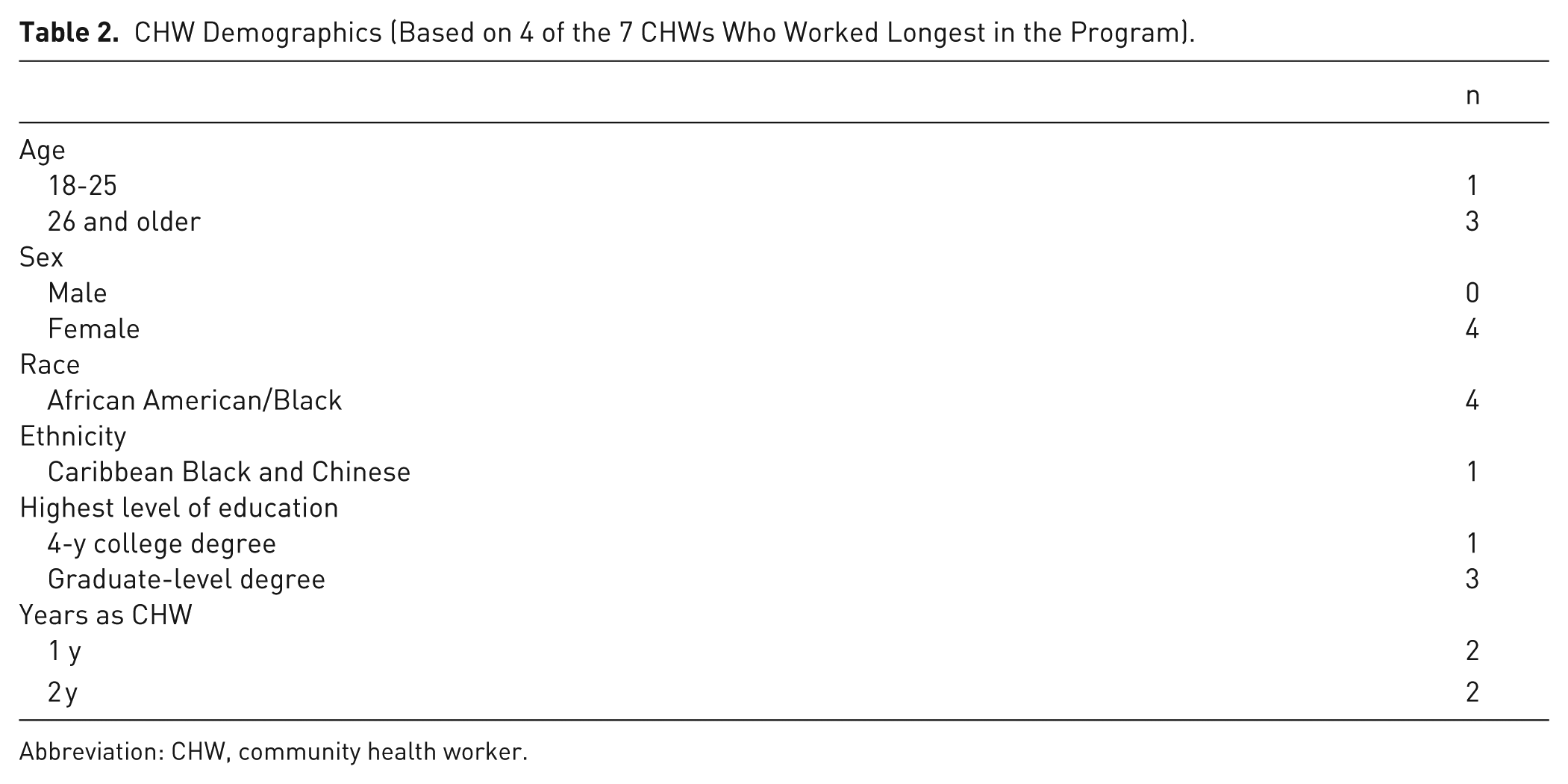
Abbreviation: CHW, community health worker.
The team synthesized 4 themes from the interview data that were associated with family and CHW dynamics: (1) family and CHW communication, (2) health literacy support, (3) technology support, and (4) program adherence support. The communication dynamics were bidirectional, and the health literacy, program adherence, and technology support flowed from CHWs to families.
Theme 1: Family and CHW Communication
The team-created study materials were designed to facilitate intrafamily communication about “defying diabetes together” (the project name that CHWs chose), but the interview results showed that communication between CHWs and family members predominated. Both CHWs and family members reported that they talked about the assigned program topics, such as healthy eating, physical activity, shared goal setting, and stress management, as well as how to use program materials, including worksheets and videos about lifestyle changes.
Family members and CHWs commented frequently on the communication techniques of question-asking and answering and active listening. Although CHWs used question-asking to engage family members in program activities and materials, the interview data reflected both the families’ and CHWs’ experiences that questions flowed from families to CHWs and CHWs were responsible for providing answers. CHWs noted that when families were prepared for the sessions, the CHWs could use active listening and follow rather than lead the discussions.
I would say 3 of my families are always very prepared. They have always read the material, they have always met together at least once during the week, and they’re ready to proceed with the conversation.” [CHW 6]
CHWs commented on the volume of families’ questions. The CHWs scheduled virtual meetings with families to answer questions, facilitate conversations among family members, and review program materials. The CHWs also provided their phone numbers to families so they could call and text outside the meeting times. The CHWs noted that the calls and texts took a lot of time.
I’ve been able to answer their questions. It’s just, I will say it becomes very time-consuming because they like to call and ask a lot of questions, everybody is very inquisitive. [CHW 2]
Family members confirmed that they looked to their CHWs for answers and that their CHWs were easily accessible. One family member stated,
I can call her at any time just to ask a question or text her at any time to ask a question, and she will respond. [Cohort A Family 1]
A family commented on the value of their CHW’s question-asking, information sharing, and signposting to prepare the family. They called it “keep[ing] us on our toes,” which speaks to the program engagement that CHWs were intended to foster.
And then she [the CHW] said, “Okay, this is what we are going to talk about.” And then after we talk, she says, “Okay, the next week we are going to meet to talk and share where you are [how the family is progressing in the program].” And then she’ll share information with us . . . ask us questions and ask if we are having any hurdles, any problems. So she keeps us on our toes. [Cohort C Family 2]
Both the CHW and family interview data illustrate how they used question-asking and answering and active listening to seek, exchange, and clarify information. The next section on health literacy support elaborates on families’ information and services needs and the types of support they sought and received from CHWs.
Theme 2: Health Literacy Support
Families asked their CHWs for help understanding and using program materials as well as for additional, easy to understand information about program topics. Healthy People 2030 defines personal health literacy as the “degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others.”
18
Interview data illustrate how CHWs worked with families to address their health literacy needs and build their knowledge and skills. One CHW commented on how they broke down program information to respond to families’ specific questions.
I sent out that resource guide [from the program]. I don’t send it all out at once. I send it out separately because they asked me at random times for stuff that’s not even related to the session in that week, so I have to look in a future session or a past session and look at the resource guide, and I pull that document or link out, and I’ll share that with them. [CHW 2]
CHWs also walked through materials with families to make sure that the concepts and words were clear. A CHW noted:
There were . . . some phrases and stuff that I guess I didn’t catch that they didn’t really understand, so I kinda had to explain it in different words. And so after I did that with the first family, I just would make each one after that better or just change the words from there on out and that, I guess, it improved the experiences that I had with the other families. [CHW 1]
The data showed that families needed help understanding the program components and flow. A CHW explained what they told families to expect.
I gave them a really good breakdown of what DSMES [the diabetes self-management education and support program] is in the beginning, what HALT [the diabetes prevention program] is, how their schedule is, where their schedule is in their emails I sent, and the flow of the meetings in terms of sessions. And then some potential other resources and references that they can use if they want to, you know, dive a little deeper, and then also the worksheets. [CHW 2]
Family comments confirmed that the CHWs’ efforts to explain information in simple terms were necessary and helpful. They positively noted that CHWs took time to explain information.
Even if we don’t understand it, she’ll [the CHW] break it down to the simplest form. [Cohort B Family 5]
The CHW and family interview data about health literacy issues show that CHWs and families engaged in a give-and-take about the information the families needed to be successful. Sometimes, families asked CHWs for additional information, and other times, CHWs anticipated and provided information they thought families would appreciate. The next section illustrates the technology support families needed from CHWs to navigate program activities.
Theme 3: Technology Assistance
All portions of the program were conducted by telephone or online using Zoom, Teams, YouTube videos, Qualtrics survey system links, and the HALT platform to access the diabetes prevention program elements. CHWs met virtually with families for discussion sessions and learned that families varied in their digital literacy skills. Some families could access the platforms and were comfortable, while others had challenges accessing or navigating the platforms. One CHW said,
That [setup of devices] took a lot of time out and I had to schedule extra virtual meetings to assist them with that. The issue really was with them working on their phones to get the app. [CHW 2]
Families recognized they needed to use technology to be successful in the program, and they appreciated that CHWs offered navigation help. Family members commented that the CHWs added ways of communicating, such as text and phone calls, when computer access and use were issues. For example, one family said about their CHW,
She’s been very helpful and making things a lot . . . easier, . . . when you’re not computer savvy. [Cohort A Family 4]
Another family needed phone calls to connect with their CHW.
I said, “I’m not technology, savvy.” And she said, . . . “We’ll work it out.” I said, “Well, if you work it out, you got me. But if we can’t work it out, I’m just lost, ’cause you know I’m just not there.” So that’s why we’re on the phone. [Cohort B Family 5]
If a family member could not help with technology, CHWs were the only option, making them frontline tech workers. In addition to health literacy and technology support, families and CHWs talked about the support needed to stay in the program and engage with materials and activities.
Theme 4: Program Adherence Support
CHWs guided families to stay in the program and on track with activities, such as using the worksheets and videos and changing lifestyle behaviors. For example, a CHW stated that their involvement was necessary to help a family complete intervention activities.
I know that the worksheets are definitely meant for my families to engage together outside of my role, as a community health worker, but I find that they won’t do it unless I’m there running through that with them . . . and encouraging them to do this again outside of our meetings together, as a way to make their efforts sustainable. [CHW 7]
Families reported that CHWs recognized the challenges in adhering to the diabetes programs and the support that could make adherence easier. One family noted the ways the CHW used to keep them engaged.
She really stays on us and she keeps us encouraged, and that’s very helpful. A lot of people don’t know how important that is. . . . Because it’s very easy to lose interest, you know, but with her you can’t lose interest. . . . If she has not heard from you, she will call you up, she will text you. She lets you know what’s going on. She keeps you up to date, and I really appreciate that. [Cohort B Family 6]
Family participants observed that CHWs showed a high level of commitment to the BFDDT program and helping families succeed. They said CHWs used encouragement and accountability to retain participants.
I felt like she really cared, that she was really concerned, and really committed to this work. So the connection was there, the passion, you know, for working for our health as a family and celebrating our successes, but also, calling on us when maybe we weren’t moving in the direction that we had committed to moving into. [Cohort C Family 7]
Collectively, the family and CHW interview data that coalesced around the themes of communication, health literacy, technology, and program activities indicate that the functional and therapeutic bonds identified in prior CHW research also developed for family members and CHWs.
Conclusions
The BFDDT study adds qualitative results to the growing literature on family-based diabetes prevention and self-management education and support programs and the limited literature on how participants and CHWs interact, communicate, and share information during lengthy chronic disease programs.7 -10 Because the team collected comparable real-time data from family members and CHWs, both sides of the interaction can be examined, and the impact of the support activities and family members’ and CHWs’ program experiences can be considered. Also, the intervention involved 2- to 3-person family groups instead of individual participants, and the data illustrate additional relationship and communication skills CHWs may need when working with small groups and a range of needs.
As in other CHW studies, program participants recognized and appreciated that their CHWs were empathetic, relatable, adaptable, and good communicators, and families and CHWs spoke of strong emotional and task-based bonds.13,17 The data on health literacy and technology support activities identify additional critical support needs. CHWs recognized how unfamiliar diabetes program content and procedures can be for participants, according to the data. CHWs’ positive impact on participants’ program adherence appears in family members’ comments and complements similar results in other studies.
Key limitations of the study relate to using a convenience sample from only 1 metro area, the nature of semistructured interview data, and the lack of a control group that also had CHWs. As noted previously, though, the intent was not to study CHWs as an independent variable. The research team’s interest was family dynamics and chronic disease, and the family-CHW dynamic data emerged organically in participants’ responses. The study’s qualitative data help fill a gap in knowledge about CHW-client interactions and provide insights into why this can be a powerful relationship with positive impacts on health and program outcomes. 17
Diabetes prevention and self-management education and support programs should innovate to expand their appeal, reach, and public health impact. The study results speak to the promise of family-focused diabetes programs to effectively engage small groups who influence each other’s lifestyle behaviors. The combination of family enrollment and positive CHW support may create a positive dynamic that motivates Black families to enroll and be successful in diabetes prevention and self-management education and support programs. Health literacy and technology support are emerging areas that CHWs may need to address with families. Family teams and CHWs working together may expand the appeal and reach of underused diabetes prevention and self-management education and support programs and help them realize their potential in improving the public’s health.
Supplemental Material
sj-doc-1-tde-10.1177_26350106261450912 – Supplemental material for Black Family and Community Health Worker Dynamics in a Family-Centric Diabetes Prevention and self-Management Education and Support Intervention
Supplemental material, sj-doc-1-tde-10.1177_26350106261450912 for Black Family and Community Health Worker Dynamics in a Family-Centric Diabetes Prevention and self-Management Education and Support Intervention by Cynthia Baur, Devlon N. Jackson, Julie Bromberg, Monica Miller, Darlene R. Saunders, Nkossi Dambita and Rebecca Ledsky in The Science of Diabetes Self-Management and Care
Supplemental Material
sj-doc-2-tde-10.1177_26350106261450912 – Supplemental material for Black Family and Community Health Worker Dynamics in a Family-Centric Diabetes Prevention and self-Management Education and Support Intervention
Supplemental material, sj-doc-2-tde-10.1177_26350106261450912 for Black Family and Community Health Worker Dynamics in a Family-Centric Diabetes Prevention and self-Management Education and Support Intervention by Cynthia Baur, Devlon N. Jackson, Julie Bromberg, Monica Miller, Darlene R. Saunders, Nkossi Dambita and Rebecca Ledsky in The Science of Diabetes Self-Management and Care
Footnotes
Acknowledgements
The authors thank Cecile Bah, MPH; Joyceta Cole, MSEd; Mahalet Samson, BS; and Autumn Simone Williams, MPH, the main community health workers who worked with the Black families in the project. We also thank the Black families who participated.
Ethical Considerations
The study was reviewed and approved by the FHI360 Office of International Research Ethics. Family participants provided written consent, and community health workers provided verbal consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded 100% by the US Department of Health and Human Services Office of Minority Health through Grant 6CPIMP211319-02-02 to FHI 360.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data in this article are based on survey responses and interviews with family members and community health workers. We have deidentified the data and will make the data sets available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.