
Abstract
Purpose:
The purpose of the study was to understand how patient/family experiences with the diabetes care team impact medical nutrition therapy (MNT) utilization in pediatric type 1 diabetes (T1D).
Methods:
Utilizing a qualitative descriptive research design augmented by phenomenological principles, we conducted supplementary analysis of data collected during semi-structured interviews with caregivers of children with T1D <18 years and youth with T1D ages 12 to 17 years with T1D duration ≥1 year. Interview guides were informed by the socioecological framework, with 1 section dedicated to the exploration of patient/caregiver MNT-based experiences with the diabetes care team.
Results:
Qualitative analysis of data from 18 completed interviews (9 caregivers, 9 patients) yielded important themes with regard to how experiences with the diabetes care team influence MNT utilization in the child with T1D. These included (1) dissatisfaction and confusion regarding nutrition education at the time of T1D diagnosis, (2) misalignment of nutrition goals/lack of perceived utility during outpatient T1D visits, (3) observed gaps in nutritional counseling during outpatient T1D visits, and (4) opportunities to optimize patient/family nutrition experiences with the outpatient diabetes care team.
Conclusions:
This study produced important insights into the impact of patient/caregiver interactions with the diabetes care team on MNT perceptions and experiences. Initiatives aimed at strengthening and individualizing nutrition education are imperative in optimizing MNT utilization in pediatric T1D.
Type 1 diabetes (T1D), often diagnosed in childhood, is a lifelong disease that requires ongoing medical follow-up. As such, the relationships that patients and families establish with the child’s diabetes care team and the education received have a profound impact on all aspects of management, including nutritional. Both the American Diabetes Association and International Society for Pediatric and Adolescent Diabetes recognize the importance of medication nutrition therapy (MNT) in the care of the child with T1D at diagnosis and routinely thereafter.1,2 This should be provided by a multidisciplinary team trained in pediatric diabetes management, which includes an experienced registered dietitian (RD). Both organizations also emphasize the need for individualized nutritional management that considers the child’s needs and activities and family habits, preferences, cultural and religious factors, access, and abilities. MNT should be centered on healthy eating principles, proper prandial diabetes management strategies (including timing of insulin administration, matching the insulin dose to carbohydrate intake, and managing the effect of dietary fat and protein on glycemia), and ensuring that nutritional patterns support optimal weight status, growth, and development.1,2
However, despite the aforementioned recommendations, documented glycemic3-8 and metabolic9-11 benefits with careful attention to nutritional considerations, and concern over rising rates of overweight/obesity in pediatric T1D,12-21 many patients and families demonstrate suboptimal MNT utilization, as demonstrated by subpar dietary quality6,7,22-28 and low annual RD follow-up rates.8,29-31 With regard to key nutrition principles, current nutritional guidelines for youth with T1D emphasize increased intake of non-starchy vegetables, whole fruits, legumes, whole grains, nuts and seeds, and low-fat dairy products and less sugar-sweetened beverages, sweets, meat, refined grains, and processed or ultra-processed foods. 2 While a focus on individualization is emphasized, the general recommendations regarding optimal macronutrient composition include 40% to 50% of energy coming from carbohydrates, <35% from fat (<10% from saturated fat), and 15% to 25% from protein. 1 However, studies have found that youth with T1D consumed higher than recommended amounts of refined grains, sweetened beverages, total and saturated fat, and salty snacks and a lower quantity of whole grains, vegetables, fruits, fiber, and calcium.6,7,22-28 It is also notable that recently, an association between obesity and the use of hybrid closed-loop (HCL) systems in youth with T1D was described. 21 Although the reasons for this are unclear, some studies32-35 suggested the presence of increased food freedom and relaxed prandial insulin administration practices (eg, inconsistent pre-bolus dosing and imprecise carbohydrate/insulin matching) with increased reliance on diabetes technologies, which may lead to excess weight gain due to overconsumption of energy dense foods and delivery of higher insulin doses (ie, insulin is an anabolic agent). This underscores the importance of nutritional education within the context of advanced diabetes technologies. With regard to RD follow-up, as noted, at least annual follow-up is recommended for youth with T1D (and more frequently within the first year of diagnosis).1,2 Based on previously published data, average annual RD follow-up rates among children with T1D ranged from ≈12% to ≈71% (higher rates based on survey responses).8,29-31
As the diabetes care team plays a crucial role in supporting optimal self-management36,37 in T1D, it is important to understand how early and longitudinal experiences with RDs, endocrinologists, and non-RD certified diabetes care and education specialists (CDCESs) impact the way patients and families approach MNT in the child’s T1D care. This qualitative study involving supplementary analysis of data previously collected from interviews with caregivers and pediatric patients with T1D focuses on exploring these concepts. The future goal is to design interventions aimed at optimizing the nutrition-focused approaches and interactions between youth with T1D, their families, and the diabetes care team to improve MNT utilization and child health outcomes.
Research Design and Methodology
Study Design, Setting, and Selection of Participants
In the parent study, 35 we utilized the socioecological framework38,39 and a phenomenological research design augmented by a grounded theory approach40-42 to explore the lived participant experiences with MNT and to identify knowledge gaps in our understanding of factors contributing to MNT underutilization. In that study, we had explored themes within 5 domains (individual, shared child/caregiver-specific, interpersonal, institutional, and societal) to generate a theoretical model depicting the intricate process that connects the family unit encompassing the child with T1D and suboptimal MNT utilization. 35 Within the institutional domain, we had previously focused on school-related considerations and challenges. For the purposes of the current article, we had performed supplementary analysis of previously collected data by employing a qualitative descriptive research design 43 augmented by phenomenological principles to expand upon the institutional domain and to answer the research question of how experiences with the diabetes medical community may impact MNT utilization in pediatric T1D.
As part of primary data collection, we conducted separate 1:1 semi-structured interviews with patients and caregivers of children with T1D followed in the Outpatient Diabetes Program at Boston Children’s Hospital (BCH), a large, pediatric, tertiary care, academic medical center that serves approximately 2200 children with diabetes. In our multidisciplinary model, youth with T1D receive counseling and education from endocrinologists, non-RD CDCESs, RDs, and social workers both at the time of the initial diagnosis and during subsequent outpatient longitudinal care. We included English-speaking caregivers of patients with T1D <18 years and youth with T1D 12 to 17 years of age with T1D duration of ≥1 year and ≥1 diabetes medical visit at BCH in the past year. Participants were recruited via email/telephone outreaches, flyers posted in diabetes clinics and on the private BCH Diabetes Facebook and Instagram pages, and aid from the diabetes medical providers (endocrinologists and non-RD CDCESs). We employed both maximum variation purposive (ie, to recruit participants with diverse characteristics) and theoretical (ie, based on emergent themes during analysis) sampling strategies until data saturation was achieved. If a caregiver-patient dyad was enrolled for separate interviews after being referred by the diabetes medical team or self-initiated outreach to the study team, the interviewers (SA, HM) performed 1 interview each prior to any analysis to avoid bias. A more detailed description of our inclusion/exclusion criteria and recruitment strategy has previously been published. 35
Data Collection
To facilitate data collection in the parent study, extensive interview guides (Supplemental Files 1 and 2) were developed by a research team comprised of pediatric endocrinologists with expertise in T1D and nutrition, a qualitative research specialist, and a research assistant with a background in psychology and public health and a strong interest in studying and understanding human behavior. The guides covered 4 major topics: (1) general questions about the child’s T1D history, (2) general thoughts about the role of nutrition in a child’s T1D care, (3) patient-specific nutrition-related questions, and (4) experiences with nutrition-focused discussions and recommendations encountered during visits with dietitian/nutritionist and medical providers. Whereas the parent study covered the first 3 topics, 35 this last section forms the basis for the supplementary analysis published herein. Semi-structured interviews, lasting an average of 60 minutes, were conducted virtually by 2 trained interviewers (SA, HM) between October 2023 and April 2024 using the Zoom platform (Version 5) and subsequently transcribed for analysis using Hoffman Transcription. A more detailed description of the data collection process was previously published. 35
Data Analysis
A multidisciplinary research team of pediatric endocrinologists, experts in qualitative research, and a research assistant created a draft codebook informed by the socioecological framework for the parent study, which was also utilized for this supplementary analysis. 39 Prior to analysis, interview transcripts were reviewed and edited for accuracy. The analysis consisted of 3 phases, including (1) independent, blind Level 1 coding (utilizing a combination of inductive and deductive coding approaches) of each interview transcript by 2 trained coders, followed by collaborative review and reconciliation of the codes and amendment of the codebook as needed; (2) axial coding to expand upon core concepts and connect Level 1 codes into broader categories; and (3) identifying major themes and their interconnections to enhance our understanding of how experiences with the diabetes care team impact MNT utilization among children with T1D and their families. This is different from the parent study, where identified themes were used to build a theoretical model of factors mediating the relationship between the family unit encompassing the child with T1D and MNT utilization within the socioecological framework. 35 All analyses were performed by the same study team members (SA, HM), and additional coders (DW, KG) were available to resolve any discrepancies and disagreements in the coding. Data collection and analyses were completed when thematic saturation was achieved in the parent study. Analyses were performed using Dedoose software (Version 9.0.107, SocioCultural Research Consultants, LLC, Los Angeles, CA). 44 Additional details have been published previously. 35
Results
Participant Characteristics
Qualitative analysis was based on data collected from a total of 18 participants included in the parent study (9 caregivers, 9 patients). There was only 1 self-referred caregiver-patient dyad that participated in the respective interviews. In brief, among child characteristics in both cohorts, there was a slight female predominance (67% in caregiver group, 56% in youth with T1D group), many had favorable average hemoglobin A1c values (6.7% ± 0.8% in caregiver group, 7.8% ± 0.8% in youth with T1D group), and the majority were using a continuous glucose monitor (100% in both groups) and HCL technology (78% in caregiver group, 67% in youth with T1D group). The children in the youth with T1D group were expectedly older than those in the caregiver cohort (15.5 ± 1.6 years vs 12.0 ± 5.2 years). Only 33% of children in both groups had a single 1-on-1 RD visit in the prior year. A more detailed description of the participant characteristics in both the caregiver and youth with T1D groups was previously published. 35
Qualitative Analysis
Our iterative analysis identified several key themes regarding how experiences with the diabetes care team impact MNT utilization in the child with T1D (Figure 1). These included (1) dissatisfaction and confusion regarding nutrition education at the time of T1D diagnosis, (2) misalignment of nutrition goals/lack of perceived utility during outpatient T1D visits, (3) observed gaps in nutritional counseling during outpatient T1D visits, and (4) opportunities to optimize patient/family nutrition experiences with the outpatient diabetes care team.
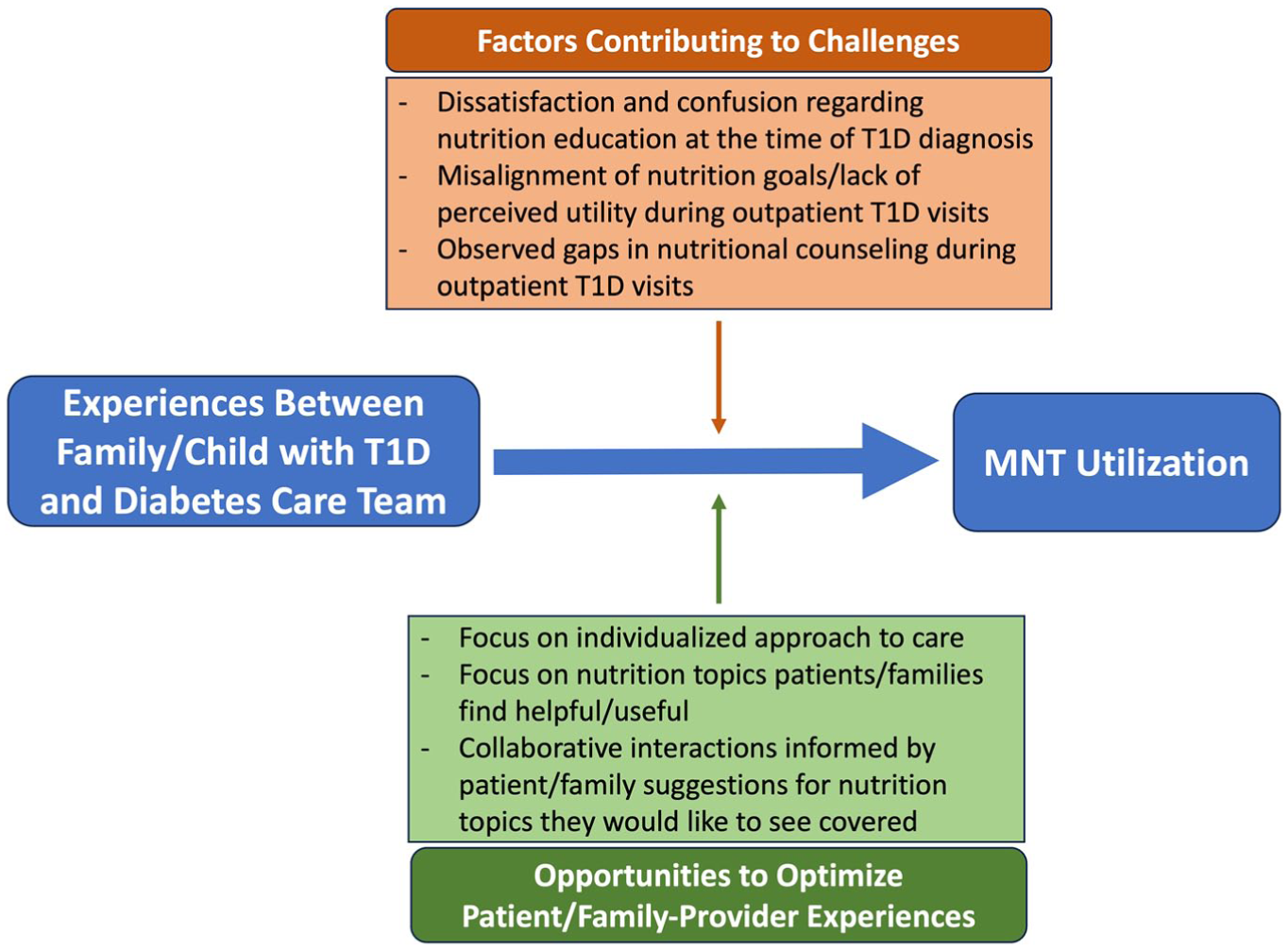
A diagram depicting key themes with regard to the impact of family/child experiences with the diabetes care team on MNT utilization in pediatric T1D.
Theme 1: Dissatisfaction and Confusion Regarding Nutrition Education at the Time of T1D Diagnosis
Some participants described their experiences with nutritional education at the time of T1D diagnosis, highlighting both gaps and impacts on the child’s relationship with MNT.
When we first got diagnosed, I remember saying to the nutritionist, I was like, “You’re okay with the food that they’re providing in the hospital? Like my kid just got diagnosed with diabetes, and you just gave him pancakes and like the most disgusting syrup ever known to man.” Like it literally is toxic, and I wasn’t trying to be like rude to her, but like at the same time, it’s like, “You’re a nutritionist. This is not nutritional.” (ID 7C; caregiver response) It seems to me like what I heard from our nutritionist at the hospital was, “Don’t change anything, keep doing what you’re doing.” . . . [Before] she even knew what we were doing, basically she wanted him to be able to eat like a typical kid and teach him how to manage that versus telling us what’s more important on how to keep it [T1D] regulated better and what the right things to eat are. . . . After years of experience watching [patient], the most important thing is the consistent meals, well-rounded meals. She did not mention that. (ID 9C; caregiver response) I got this book from somebody that was talking, . . . and it was very, very strong on . . . how like if you eat less, then it’ll keep your blood sugar lower, . . . and when your blood sugar is lower, that will make you feel better. I remember asking so many questions about how eating less food will make your blood sugar stay lower and how that will make you feel better. . . . I remember I was very confused. . . . [Dietitians also] taught me to like read the carbs and not like the other nutrition info, that it doesn’t matter as much. . . . That it like matters about the carbs and like not like the calories and . . . fats as much. (ID 9P; patient response)
Theme 2: Misalignment of Nutrition Goals/Lack of Perceived Utility During Outpatient T1D Visits
Participants had variable nutrition experiences when it came to their interactions with (1) RDs and (2) endocrinologists and non-RD CDCESs in the outpatient setting following the child’s T1D diagnosis. A common theme was misalignment of goals between the patient/family and the diabetes care team and perceived lack of new/useful information. This was at times associated with decreased desire for further engagement in nutrition-focused discussions. Caregivers were more likely than patients to endorse a lower/declining utility associated with nutritional counseling.
She [RD] made a couple of offhand comments about like limiting carbs, which I immediately was like, “No, that’s not something that I feel like I want to do.” (ID 7C; caregiver response) They [RDs] were trying to help us understand how to manage diabetes as best we can eating a typical American diet. . . . And honestly, the truth is, that’s why I didn’t really want to talk to her anymore because we’re coming from two different places. She’s trying to help kids that are just going to graze all day and eat junk, and we’re trying to like have our kids eat healthy and make his [patient’s] diabetes as manageable as possible and keep it in like the healthy range. . . . In addition, . . . it just seems like in the beginning, . . . [non-RD CDCESs and diabetes doctors were] trying to talk to us about how to manage it [diabetes] with junk, and then they realized what we were doing, and they were like, “Oh, okay.” . . . I guess if we continued to further it, it just didn’t seem like it was going to be beneficial. (ID 9C; caregiver response) When it comes to like everyday common-sense-type things and the way that food and nutrition interact with a typical teenager, . . . sometimes the advice from the endocrinologist’s perspective has been a little bit too like technical and textbook and not really thinking about real life, and what I’ve noticed with her DNE [diabetes nurse educator] and nutritionist has been a focus on balancing real life with the nutrition aspect. (ID 11C; caregiver response) I’ve tried a diabetic nutritionist, and she didn’t really help very much. It was kind of stuff like I know, like stuff I’ve picked up and learned on my own. . . . It didn’t really benefit me. (ID 1P; patient response)
Simultaneously, many participants expressed the desire for a more individualized approach to care.
It’s really important for a nutritionist to learn who the family is . . . , what their family life looks like, what their meals look like . . . I think is just really important before suggestions and changes because you want the family to go with you, right? . . . [Then] making small steps there because it’s so overwhelming to make these big changes to your life, and I think that if you don’t take the small steps, people are going to be more resistant to massive changes. (ID 2C; caregiver response) I like the idea, though, of having an initial visit to talk about diet and nutrition with a nutritionist and then maybe having some goals and meeting with that person once a year or something to say like, “Here are my goals as a person with type 1. Here’s what I want to work on. Maybe I want to add new foods. Maybe I want to balance foods. Maybe I just want to work on my bolusing strategy.” (ID 7C; caregiver response) Do I think that they [non-RD CDCESs and diabetes doctors] should provide more nutritional information? Yes, to the people that need it. Like I would hope that they’d be equipped to answer the questions if that conversation needed to be had. . . . [If] somebody is there and their numbers are all over the place and you know that nutrition is a component here where we could tighten that up and be better at doing, you know, whatever foods they eat, then I think that conversation would need to be had with that patient. (ID 8C; caregiver response) Once a year is probably enough [for a child with T1D to meet with an RD] unless they’re like struggling with that aspect of like carb counting and eating and stuff like that. . . . I think that maybe a little more frequently if you’re new to diabetes. (ID 2P; patient response)
Theme 3: Observed Gaps in Nutritional Counseling During Outpatient T1D visits
Aside from general perceived lack of utility, caregivers and patients gave examples of specific gaps in nutritional counseling by their outpatient diabetes providers. Among endocrinologists and non-RD CDCESs, this included lack of encouragement to engage with an RD. Some participants alluded to either provider- or patient-/family-driven reasons for this limited engagement.
They [DNE and doctor] don’t talk to us about going to see one [an RD], no. We do talk a little bit about like what she eats and stuff like that when we go just to kind of get an overall view, and I’m sure if they had concerns, they would send us that way, but it has not been recommended to us as of right now. (ID 5C; caregiver response) The dietitian that we saw admittedly did not have a lot of experience with diabetes, which surprised me because I thought it was more like of a specialized person we would be meeting with. . . . [So] she kind of went down the path of, you know, “You need to eat a low-carb diet,” and then when I asked about it, she was like, “Well, I don’t really have—diabetes is not my specialty,” and I was like, “I don’t feel like I’m comfortable in this conversation.” (ID 7C; caregiver response) No, I wouldn’t say they [physician and non-RD CDCES] do [discuss any nutritional topics or provide any dietary recommendations]. . . . [For] me, that’s not why I go there. . . . I don’t think it’s like really been a topic because we’ve had such a good handle on things. . . . So where his A1c is great and it’s really more of a timing thing than it is a nutritional thing, then they’re not going to have a conversation with me about nutrition. (ID 8C; caregiver response) I would just like to see like more education around what really is sustainable for kids and how to really keep it [blood glucose] in range, you know, but then it’s a whole family lifestyle change, so I understand why they [RDs] don’t do it. (ID 9C; caregiver response) We don’t usually talk about nutrition that much, or I’ll tell them [non-RD CDCES and diabetes doctor] about like what I do with my nutrition and what I eat and stuff, and if I ask for like recommendations, they’ll at that point give recommendations, but otherwise I feel like it’s not the main topic of discussion when I meet with them. . . . [Also,] if I wanted to [go see an RD], I would like ask, but as far as their worries go, I feel like they don’t like encourage that unless I wanted to. (ID 6P; patient response)
Theme 4: Opportunities to Optimize Patient/Family Nutrition Experiences With the Outpatient Diabetes Care Team
In addition to advocating for individualized approach to care, caregivers and patients also provided examples of helpful advice that they had received during outpatient visits with their diabetes care team and suggested topics they would like to see covered. These examples and suggestions are depicted in Figure 2.
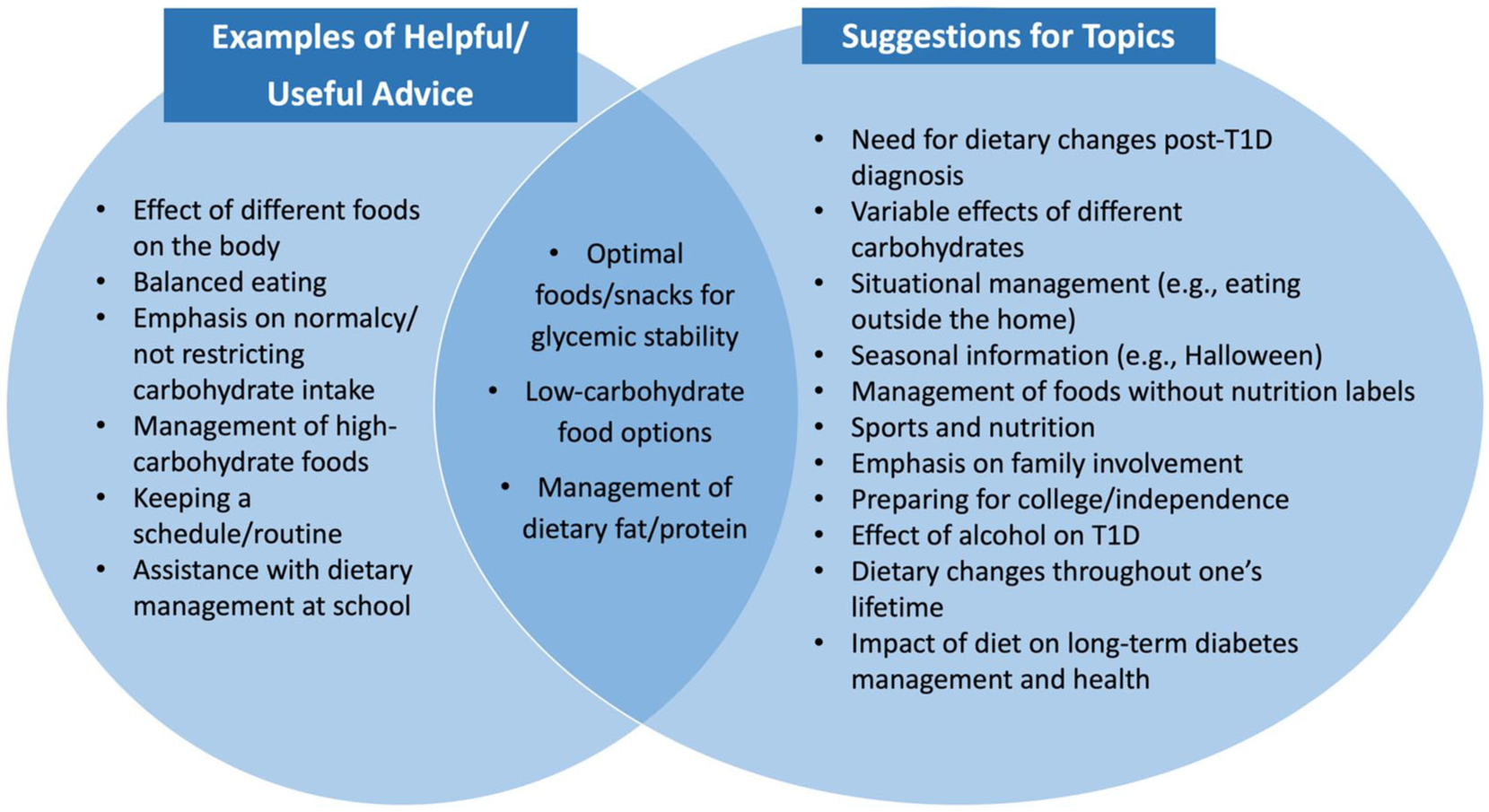
Examples of helpful covered and suggested nutrition topics during outpatient T1D visits with the diabetes care team.
Examples of helpful/useful advice
She [RD] had to help us quite a bit in terms of when [the patient] started school. . . . [The RD] had to go on and explain that you can’t have a carb-only meal, that there had to be fat and protein because the type 1 diabetes was being really impacted by food choices that the school was giving her. (ID 2C; caregiver response) She [RD] basically talked about, you know, keep them eating the same. She suggested a schedule and a routine for things. . . . I think it was definitely helpful just to hear and know that like we didn’t have to do anything crazy. It is life-changing, but it doesn’t have to be like exhausting. . . . [In addition,] one of the things . . . [non-RD CDCES and doctor] said was, “Don’t take carbs out. They need to be in there. Kids need them to grow,” and so like hearing that was really encouraging. . . . I think the let your kid be a kid and let them have cake and those kinds of things is really helpful because, you know, she doesn’t have to just eat, you know, green vegetables and meats and cheese . . . , but those are important to have too. (ID 5C; caregiver response) A lot of the [RD] recommendations have been in terms of just preparing for what certain types of foods will do in the body of a type 1 diabetic and, you know, recommendations for certain foods, for example, like those proteins and fats that might need an extended bolus or might need you to set that alarm clock for 3 am, you know, to check on your blood sugar and address things throughout the night. (ID 11C; caregiver response) So my doctor . . . would recommend stuff to eat like to help keep my blood sugar stable. . . . My diabetic educator used to tell me like high carbs, if I have like pasta or pizza, then she said like, “Extend your bolus.” (ID 1P; patient response) I’ve been introduced to some . . . nice alternative, more low-carb foods because of it [experiences with an RD]. . . . [Going] to appointments of that nature has helped me to learn to manage my diabetes, find foods that are, you know, more agreeable with my condition, and snack more sustainably. (ID 5P; patient response)
Suggestions for topics participants would like to see covered
I remember it was helpful like getting lists of candy right before Halloween. . . . [So] . . . seasonal information. . . . [Also,] talking about nutrition with food, with sports and activities, that’s probably helpful, snacks that have been really working well. (ID 6C; caregiver response) That’s a huge piece that I think that nutritionists and dietitians can help with, . . . like how you may deal with your food at home versus when you’re out or when your parents are helping you and when you’re out at a party with your friends if you’re older, like situational management. (ID 7C; caregiver response) I think education on . . . how the American diet is not ideal for diabetics or anyone really, but especially for diabetics, like I think that’s important to talk about. You know, it might enlighten them [RDs] to say, “Hey, maybe we should start making changes.” . . . It’s really training the whole family. . . . I’d [also] be interested in hearing [from CDCECs and diabetes doctors] anything other than information about them trying to tell us how to manage his [patient’s] diabetes based on the American diet. . . . If we’re talking about French fries and chips and soda, I don’t want to hear it. It doesn’t mean anything to me because we don’t do any of that. (ID 9C; caregiver response) [Patient’s] planning to live away when she goes to college in the fall, so we thought that this would be a really good time to kind of reconvene [with an RD] . . . [because it is] a different level of independence when you’re getting ready to live on a college campus. . . . I’m hoping that her nutritionist will also be able to offer her some thoughts on, you know, how drinking typically affects a type 1 diabetic just for learning and for awareness. (ID 11C; caregiver response) I would be interested in hearing about more like low-carb and carb-free options[,] . . . the effects that diet can have on long-term diabetes management and . . . health . . . as I age, and . . . health relating to other parts of my body that may be affected as a result of having diabetes. . . . [Last] thing I’d really like . . . to know about is how to, you know, calculate, count for food that there is no nutrition label . . . and learning how to, you know, eat with less boundaries. (ID 5P; patient response) I think that our nurse educator told us—it was honestly pretty recently, like a year or so ago—that protein eventually turns into carbs, and we never knew that, so . . . it would be really helpful I feel like to tell people that that are newly diagnosed. . . . They . . . [also] say like a carb is a carb, and as far as my body goes, that’s definitely not the case. . . . I feel like you have to ask the questions for yourself to get an answer whereas I think that a lot of like really helpful information, like if they provided you with it, would save a lot of like time and like worry and confusion. (ID 6P; patient response) I would just probably ask . . . how my eating is going to change as I get older, ’cause like I’ll start high school next year, and then like when I go to college, . . . if like my eating’s going to change throughout my life and if there’s going to be like different ways to deal with it. (ID 9P; patient response)
Conclusions
Our qualitative analysis of previously collected data from semi-structured interviews with caregivers and youth with T1D at a large pediatric academic medical center identified important themes related to the lived experiences of patients and families when it comes to nutrition-focused interactions with the diabetes care team. In addition to enhancing our understanding of this complex relationship and its impact on MNT utilization in pediatric TID, this study also helped us identify opportunities to optimize patient-/family-provider MNT-based experiences. While other studies may have explored patient-/family-provider nutrition-focused interactions within a specific niche (eg, the use of a low-carbohydrate approach for T1D management45,46), our current article was among the first to highlight more comprehensive experiences applicable to the broader pediatric T1D population and to specifically elicit youth perspectives as opposed to just that of the caregivers.47-49
As T1D is a lifelong disease that requires ongoing medical follow-up, patients and families’ relationship with the child’s diabetes care team undoubtedly has a profound impact on all aspects of management, including nutritional. In fact, this impact starts to take shape early on in the child’s diagnosis, at the time of the initial education. Several patients and caregivers described their experiences during that critical time period, focusing on perceived gaps and misalignments between their own perceptions regarding optimal dietary management and the education that was provided. These experiences may have not only raised confusion regarding proper nutritional management of the child’s T1D but also led to dissatisfaction with the education provided, potentially creating a sense of mistrust directed at diabetes care providers and affecting the likelihood of further engagement in nutrition-focused discussions and/or RD visits in the outpatient setting.
In general, establishment of therapeutic relationships with the child’s diabetes care team is an important component in ensuring optimal self-management.36,37 This concept can be extended to include nutritional management. When it comes to experiences during outpatient RD visits, many patients and caregivers described limited or declining utility of the counseling provided, attributing it to such factors as misalignment of goals and perceived lack of new/useful information and individualization. Specific gaps in counseling were also recognized, perceived to be due to limited RD experience and/or comfort. These insights support prior findings described by our group, who focused on exploring experiences with nutrition education among caregivers of youth with T1D.47,49 In addition to impacting the therapeutic rapport, these experiences and perceptions may decrease the possibility of future RD follow-up. In fact, despite the recommendations by the major diabetes organizations for annual RD visits among youth with T1D,1,2 the rates remain low.8,29,30 This was consistent with our findings, where only 33% of children in both cohorts had an RD visit within the prior year, which was in fact higher than the recently reported average annual rate of RD follow-up among all youth with T1D ≥1 year at our institution (20.8%), 8 reflecting the need for increased efforts to optimize this component of MNT.
While RDs play a pivotal role in the nutritional management of children with T1D, diabetes medical providers (endocrinologists and non-RD CDCESs) are also integral in incorporating MNT into the care of their patients. This is especially true because children with T1D do in general tend to have closer follow-up with their diabetes medical providers 2 and only variable engagement with RDs, as noted.8,29,30 Similar to experiences with outpatient RDs, participants described limited utility of nutritional counseling by diabetes medical providers, owing to such factors as misalignment of goals, challenges with implementation, and repetitiveness of information. Notable gaps in MNT-based counseling were failure to incorporate nutrition discussions into routine clinical visits and to recommend annual RD follow-up. This was at times attributed to perceived absence of need for nutritional counseling by either the patient/family or diabetes medical provider, suggesting the need for targeted education involving all stakeholders. In addition, sometimes, patients/families encountered differential experiences with different diabetes care team members when it came to nutritional counseling. This may have reflected differences in visit-specific goals and priorities and/or variable experiences, comfort, and perceptions with regard to MNT-based discussions among diverse diabetes care team members.
An important finding worth noting is how participant perceptions about and approaches to the child’s way of eating may have impacted the perceived connections with members of the diabetes care team, especially if there was misalignment of goals. Caregivers and patients who focus on maintaining a sense of normalcy and avoidance of dietary restriction in the child35,48,50 may have better rapport with diabetes care team members who support and encourage food freedom and choose not to follow up with care team members who push for more stringent nutritional modifications. Conversely, families who desire more prescriptive guidance on dietary changes that may further optimize the child’s glycemic outcomes and health may develop mistrust of providers who provide recommendations that they perceive as not aligning with mindful eating practices. This concept extends to the experiences and education received at the time of T1D diagnosis, as discussed above, potentially leaving a long-lasting imprint on how patients/families approach future interactions with the diabetes care team. This underscores the importance of individualized treatment approaches and the use of patient-/family-centered counseling techniques when trying to motivate dietary changes from the time of T1D onset onward, something that our participants advocated for.
Despite reports of limited utility and perceived gaps when it comes to MNT-based discussions with the diabetes care team, both caregivers and youth with T1D also provided helpful insights on how these experiences may be optimized to increase MNT utilization in the pediatric T1D population. In this study and others, 49 patients and caregivers gave examples of helpful advice that they had received and also provided informative suggestions for nutrition topics that they wish to be covered, with an emphasis on healthful eating habits and optimal diabetes management prandial practices, situational management, and helping to support transition to independence. This once again underscores the importance of having an individualized treatment plan, tailored to the specific interests and needs of the patient/family.36,48,49 In addition, assessment of provider comfort with and barriers to facilitating targeted nutrition-focused discussions with children with T1D and their families are imperative in identifying potential gaps in knowledge and opportunities for improvement. When it comes to diabetes medical providers (endocrinologists and non-RD CDCESs), dedicated training on MNT, including the need for annual RD follow-up, is especially important because these clinicians often provide routine, frontline care to children with T1D.
This study has several limitations. The focus on 1 academic medical center, albeit with a large diabetes program, may not accurately reflect broader patient/family MNT-based experiences with their diabetes care teams. This may be especially true considering variation in nutrition education across different diabetes centers, 30 emphasizing the need for multicenter collaborations to help answer questions posed by this research. The lack of diversity may have also limited the transferability of our findings. However, the comprehensiveness of the data collection, the inclusion of both caregivers and patients, and robust sampling strategies allowed us to gather wide-ranging insights regarding patient/family experiences with the diabetes care team when it comes to nutrition discussions, thereby achieving data saturation. In addition, the potential for interviewer bias and power differential should be considered. Both interviewers made efforts to build rapport and ensure participant comfort (eg, emphasizing participant confidentiality and avoiding wearing a white coat) while maintaining professional distance to ensure data validity. Researcher biases were continually examined through the use of reflexivity, 42 engaging in reflective analytic memo writing following each interview and during every stage of the analysis.
Implications for Diabetes Care and Education Specialists
In conclusion, this qualitative study of children and caregivers of youth with T1D provided informative insights into the impact of patient/family experiences with the diabetes care team on their perceptions about and approaches to MNT utilization. In addition to describing patient-/family-provider interactions characterized by misalignment of goals and perceived gaps in knowledge, participants also identified areas for improvement, centered around individualized care tailored to their specific interests and needs. These concepts are important to consider in both the research and clinical settings as interventions to improve patient/family MNT-based experiences at the time of diagnosis and during outpatient T1D visits are piloted and tested. The goals are to improve the rapport between patients/caregivers and their diabetes care team when it comes to nutritional counseling through patient-centered approaches and to enhance MNT appreciation and utilization among youth with T1D and their families, aiming to optimize child health outcomes.
Supplemental Material
sj-docx-1-tde-10.1177_26350106261450921 – Supplemental material for Caregiver and Patient Experiences With the Diabetes Care Team Impact Utilization of Medical Nutrition Therapy in Pediatric Type 1 Diabetes
Supplemental material, sj-docx-1-tde-10.1177_26350106261450921 for Caregiver and Patient Experiences With the Diabetes Care Team Impact Utilization of Medical Nutrition Therapy in Pediatric Type 1 Diabetes by Svetlana Azova, Hannah Michelson, David Williams, Belinda Lennerz and Katharine Garvey in The Science of Diabetes Self-Management and Care
Supplemental Material
sj-docx-2-tde-10.1177_26350106261450921 – Supplemental material for Caregiver and Patient Experiences With the Diabetes Care Team Impact Utilization of Medical Nutrition Therapy in Pediatric Type 1 Diabetes
Supplemental material, sj-docx-2-tde-10.1177_26350106261450921 for Caregiver and Patient Experiences With the Diabetes Care Team Impact Utilization of Medical Nutrition Therapy in Pediatric Type 1 Diabetes by Svetlana Azova, Hannah Michelson, David Williams, Belinda Lennerz and Katharine Garvey in The Science of Diabetes Self-Management and Care
Footnotes
Acknowledgements
The authors thank the patients and caregivers who participated in this study and shared their insights and experiences.
Authors’ Note
Hannah Michelson has moved to another institution since completing the research and has a new affiliation (Real Chemistry, Boston, MA, USA).
Ethical Considerations
The study received ethics approval from the Boston Children’s Hospital Institutional Review Board.
Consent to Participate
All caregivers signed written consent form,s and child participants signed written assent forms.
Consent for Publication
Informed consent for publication was provided by the participant or a legally authorized representative.
Author Contributions
SA, HM, BL, and KG designed research; SA and HM conducted research; DW provided essential qualitative research support; SA and HM analyzed data; SA wrote manuscript; SA had primary responsibility for final content. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible with support from Grant No. K12DK133995 (David Maahs, Linda DiMeglio, Multi-Center Program Directors) from the National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Physician-Scientist Career Development Award to Dr Azova. Dr Lennerz receives salary support from NIDDK R01DK135884.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated during and analyzed in the current study and the coding dictionary used are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.