
Abstract
Purpose:
The purpose of the study was to adapt and psychometrically evaluate an Indonesian version of the Type 2 Diabetes Stigma Assessment Scale (I-DSAS-2) for Indonesians with type 2 diabetes.
Methods:
A cross-sectional psychometric and correlational study was conducted among 190 participants recruited from outpatient clinics. The Type 2 Diabetes Stigma Assessment Scale was translated and culturally adapted following established guidelines. Psychometric evaluation included exploratory factor analysis, internal consistency testing (Cronbach’s alpha), and test-retest reliability (intraclass correlation coefficient). Clinical outcomes were assessed using A1C, the Indonesian Multidimensional Fatigue Inventory, and the Beck Depression Inventory–2nd Edition. Associations between stigma and clinical outcomes were analyzed using Pearson correlations and multiple linear regression, adjusting for age, gender, diabetes duration, and comorbidities.
Results:
The I-DSAS-2 demonstrated excellent psychometric properties, revealing a 3-factor structure (treated differently, blame and judgement, and self-stigma), strong internal consistency, and high test-retest reliability. Higher stigma scores were significantly associated with elevated A1C, greater fatigue, and more severe depressive symptoms. In multivariate models, stigma independently predicted all 3 outcomes, with the strongest association observed for depression.
Conclusion:
The I-DSAS-2 is a valid, reliable, and culturally relevant instrument for assessing diabetes-related stigma in Indonesian populations. It captures the multifaceted nature of stigma and its significant links to critical clinical outcomes.
Stigma associated with type 2 diabetes mellitus has emerged as a critical barrier to effective disease management and psychosocial well-being.1,2 Individuals living with type 2 diabetes often face negative stereotypes, internalized shame, and social exclusion, which may lead to poor self-care, delayed treatment-seeking behavior, and diminished quality of life.3,4 Stigma has been conceptualized as a complex social process involving labeling, stereotyping, separation, status loss, and discrimination within a context of power imbalance, as originally described by Goffman 5 and further elaborated by Link and Phelan. 6 In the context of chronic illness, stigma is often understood as a multidimensional construct encompassing experienced, perceived, and internalized stigma, reflecting how individuals are treated by others, anticipate judgement, and internalize negative societal beliefs. 7 As global efforts increasingly prioritize person-centered diabetes care, it is vital to understand and measure stigma accurately within diverse cultural contexts, including Indonesia, where type 2 diabetes prevalence is rapidly increasing.8,9
The Type 2 Diabetes Stigma Assessment Scale (DSAS-2) is a well-established tool developed to measure the complex and multifaceted nature of stigma experienced by individuals living with type 2 diabetes. 10 The development of the DSAS-2 was grounded in these theoretical frameworks, aiming to capture the multidimensional nature of stigma. Its 3 domains, treated differently, blame and judgement, and self-stigma, align conceptually with experienced, perceived, and internalized stigma, providing a theoretically informed structure for assessing diabetes-related stigma. While it has demonstrated strong validity in previous research, its application has primarily been confined to English-speaking populations, 10 with adaptations available in Chinese, Arabic, and Spanish contexts.11 -14 Recognizing the need for culturally relevant assessment in Indonesia, this study sought to translate, culturally adapt, and examine the psychometric properties, specifically the reliability and validity, of the Indonesian version of the scale (I-DSAS-2). Conducting rigorous psychometric validation is essential to ensure that the instrument effectively reflects the unique social and emotional dimensions of stigma encountered by Indonesian individuals with type 2 diabetes.
Beyond measurement validation, this study also explored the clinical relevance of diabetes-related stigma by examining its associations with glycemic control, fatigue, and depressive symptoms, 3 important indicators of physical and mental health in individuals with type 2 diabetes.15 -18 Understanding how stigma interrelates with these outcomes will provide valuable insights for clinicians, educators, and policymakers to develop holistic interventions that address not only medical but also psychosocial dimensions of diabetes care in Indonesia.
Methods
Study Design and Participants
A psychometric and correlational study employing a cross-sectional design was undertaken to assess the instrument and its clinical associations. Participants were recruited through purposive sampling from outpatient endocrinology and primary care clinics across Indonesia from November 2024 to February 2025. Eligible participants were adults ages 18 years or older with a confirmed diagnosis of type 2 diabetes mellitus for a minimum of 6 months. Additional inclusion criteria included the ability to communicate fluently in Bahasa Indonesia and a willingness to provide informed consent. Individuals with documented cognitive impairments or severe psychiatric disorders were excluded to ensure the accuracy and reliability of self-reported data.
Ethical clearance for this study was granted by the Joint Institutional Review Board of the Ethical Committee for Medical Research at the Faculty of Dentistry, University of Jember (Approval No. 2311/UN25.8/KEPK/DL/2025). Prior to participation, all individuals provided written informed consent in accordance with ethical research standards. To ensure methodological transparency and adherence to best practices in observational research, the study was conducted in alignment with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (see supplementary Table S1). 19
Study Population
The required sample size was determined based on recommendations for psychometric validation studies and correlational analysis. According to established guidelines, a minimum of 5 to 10 participants per item is recommended for factor analysis.20,21 Given that the original DSAS-2 comprises 19 items, the minimum sample size was estimated at 95 to 190 participants. To strengthen the statistical power and accommodate potential missing data or dropouts, a final sample of 190 participants was targeted and successfully enrolled, ensuring sufficient precision for both validation and regression analyses.
Instrument Translation and Cultural Adaptation
The original DSAS-2 was translated into Bahasa Indonesia by 2 bilingual health professionals using a widely accepted process for instrument adaptation.22,23 Both translators were familiar with the cultural context and psychosocial aspects of diabetes, ensuring that the translation captured conceptual meaning rather than relying solely on literal word-for-word equivalence. After the initial translation, a third independent translator back-translated the scale into English to check for any discrepancies. “Back-translation” refers to the process of translating the adapted version back into the original language to verify semantic and conceptual equivalence between versions. This process ensured that the meaning of the items remained consistent across languages. During translation, minor modifications were made to better fit the Indonesian language and culture. These “minor modifications” involved refining wording to improve clarity, cultural relevance, and contextual appropriateness without altering the underlying constructs of the scale. Some words or concepts in the English version did not have direct equivalents in Bahasa Indonesia. For example, terms related to “stigma” and “self-judgement” were adjusted to reflect how these ideas are understood in the Indonesian context. The translators and an expert panel, including endocrinologists and psychologists, discussed and agreed on these changes to ensure accuracy and cultural relevance.
To ensure the translated version made sense and was culturally appropriate, cognitive interviews were conducted with 10 individuals with type 2 diabetes. Cognitive interviewing is a qualitative technique used to evaluate how respondents understand, interpret, and respond to questionnaire items. Their feedback helped identify any unclear or inappropriate terms. The purpose of cognitive interviewing was to assess item clarity, cultural appropriateness, and potential misunderstandings. Verbal probing techniques were used in which participants were asked to explain their understanding of each item and describe their thought processes when selecting responses. The final version, I-DSAS-2, was adjusted based on this feedback and mutual agreement between the translators and expert panel, ensuring it was both linguistically and culturally suitable. The final Indonesian version retained all 19 items from the original DSAS-2, preserving its conceptual structure.
Measures
The DSAS-2
The DSAS-2, originally developed by Browne et al, 10 comprises 19 items designed to capture the multifaceted experience of stigma among individuals with type 2 diabetes. The scale encompasses 3 distinct dimensions: treated differently (6 items), blame and judgement (7 items), and self-stigma (6 items). Each item is rated on a 5-point Likert scale, ranging from strongly disagree to strongly agree, reflecting the respondent’s level of agreement with each statement.
Specifically, the Treated Differently subscale includes Items 1, 4, 7, 10, 14, and 17, with a possible score range of 6 to 30. The Blame and Judgement dimension comprises Items 2, 3, 5, 8, 12, 16, and 19, with scores ranging from 7 to 35. The Self-Stigma subscale consists of Items 6, 9, 11, 13, 15, and 18, also ranging from 6 to 30. When summed, the total stigma score ranges from 19 to 95, with higher scores indicating greater perceived stigma related to living with type 2 diabetes. 10
Indonesian version of the Multidimensional Fatigue Inventory-20
Fatigue was assessed using the Indonesian version of the Multidimensional Fatigue Inventory-20 (IMFI-20), a validated instrument specifically designed to capture the diverse dimensions of fatigue. 16 The IMFI-20 comprises 20 items distributed across 4 subscales: General and Physical Fatigue, Reduced Motivation, Reduced Activity, and Mental Fatigue. Each subscale contains 4 items rated on a 5-point Likert scale, ranging from 1 (strongly agree) to 5 (strongly disagree). To ensure accurate scoring, 10 positively worded items (Items 2, 5, 9, 10, 13, 14, 16, 17, 18, and 19) were reverse-coded.
Subscale scores were calculated by summing the responses to the relevant items, yielding a possible range of 4 to 20 points per subscale. The overall fatigue score, obtained by summing all 4 subscale scores, ranged from 20 to 100, with higher scores reflecting greater perceived fatigue. The IMFI-20 was selected for its strong psychometric performance and cultural relevance in Indonesian-speaking populations with type 2 diabetes, as evidenced by excellent internal consistency (Cronbach’s α = 0.92). 16
Beck Depression Inventory–2nd Edition
Depressive symptoms were assessed using the Beck Depression Inventory–2nd Edition (BDI-II), a widely recognized instrument comprising 21 items designed to evaluate the severity of subjective depression symptoms experienced over the previous 2 weeks. Each item is rated on a 4-point Likert scale ranging from 0 to 3, resulting in a total score ranging from 0 to 63, 24 with higher scores indicating greater depressive symptomatology. The BDI-II captures a broad spectrum of depressive experiences, encompassing cognitive, emotional, and somatic domains. 25
For this study, the Indonesian version of the BDI-II was utilized. This culturally adapted version has been validated for use in both the general Indonesian-speaking population and among patients with coronary heart disease. Prior research has demonstrated its strong psychometric properties, including high internal consistency (Cronbach’s α = 0.90) and satisfactory convergent validity. In the current study, the Indonesian BDI-II also exhibited excellent internal reliability among participants with type 2 diabetes, with a Cronbach’s alpha of 0.88, supporting its appropriateness for use in this population. 26
A1C levels
Glycemic control was evaluated based on participants’ most recent A1C levels, as documented in their medical records within the preceding 3 months. A1C values were reported as percentages, reflecting the average blood glucose concentration over the past 8 to 12 weeks.
Data collection procedure
Eligible participants were approached during routine clinic visits and provided with detailed study information. Participants were recruited from outpatient endocrinology clinics and primary health care facilities in Indonesia, where they were receiving ongoing diabetes management and follow-up care. These settings typically provide regular monitoring of glycemic control, medication management, and diabetes education services. Upon informed consent, participants completed a structured questionnaire comprising demographic information, I-DSAS-2, IMFI-20, and BDI-II. Trained research assistants assisted participants as needed to ensure complete and accurate responses. Clinical data including A1C were extracted from medical records with participant consent.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics, Version 28.0. Descriptive statistics, including means, standard deviations, frequencies, and percentages, were calculated to summarize participant characteristics and primary study variables. The construct validity of I-DSAS-2 was evaluated through exploratory factor analysis using principal axis factoring with promax rotation, as recommended for identifying latent factor structures in psychometric research.27,28 The suitability of the data for factor analysis was assessed using the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity.29,30 The number of factors was determined based on eigenvalues greater than 1.0 and visual inspection of the scree plot. Factor loadings of ≥0.40 were considered acceptable for item retention. The extracted factors collectively explained a substantial proportion of the total variance.
Internal consistency reliability was assessed by calculating Cronbach’s alpha coefficients for the overall scale and each of the 3 subscales, with values ≥0.70 considered acceptable. 31 Test-retest reliability was examined in a subsample of participants (n = 30) who completed the I-DSAS-2 a second time after a 2-week interval. Stability over time was evaluated using intraclass correlation coefficients (ICCs), with values above 0.75 indicating good reliability. 32
Given that the data were normally distributed, Pearson correlation coefficients were used to examine the linear associations between I-DSAS-2 scores and key clinical outcomes, including A1C, fatigue, and depression. Convergent validity, as a component of construct validity, refers to the extent to which a measure is correlated with other variables that it is theoretically expected to be related to. In this study, convergent validity was assessed by examining whether higher stigma scores were positively associated with poorer clinical and psychological outcomes. Pearson correlation analysis was conducted to determine the strength and direction of these relationships, with statistically significant positive correlations supporting the convergent validity of the I-DSAS-2.
To further assess the predictive value of stigma on these outcomes while controlling for potential confounding variables, such as age, gender, duration of diabetes, and comorbid conditions, multiple linear regression analyses were conducted. Statistical significance was defined as a two-tailed P value of less than .05.
Results
Participant Characteristics
Table 1 presents the demographic and clinical characteristics of the 190 individuals with type 2 diabetes who participated in the study. The mean age of participants was 56.2 years (SD = 9.8), reflecting a middle-aged to older adult population. The majority of participants were female (56.8%), and a substantial proportion were married (74.7%), with smaller groups reporting single (8.4%) or widowed/divorced status (16.8%).
Demographic Characteristics of Participants (N = 190).
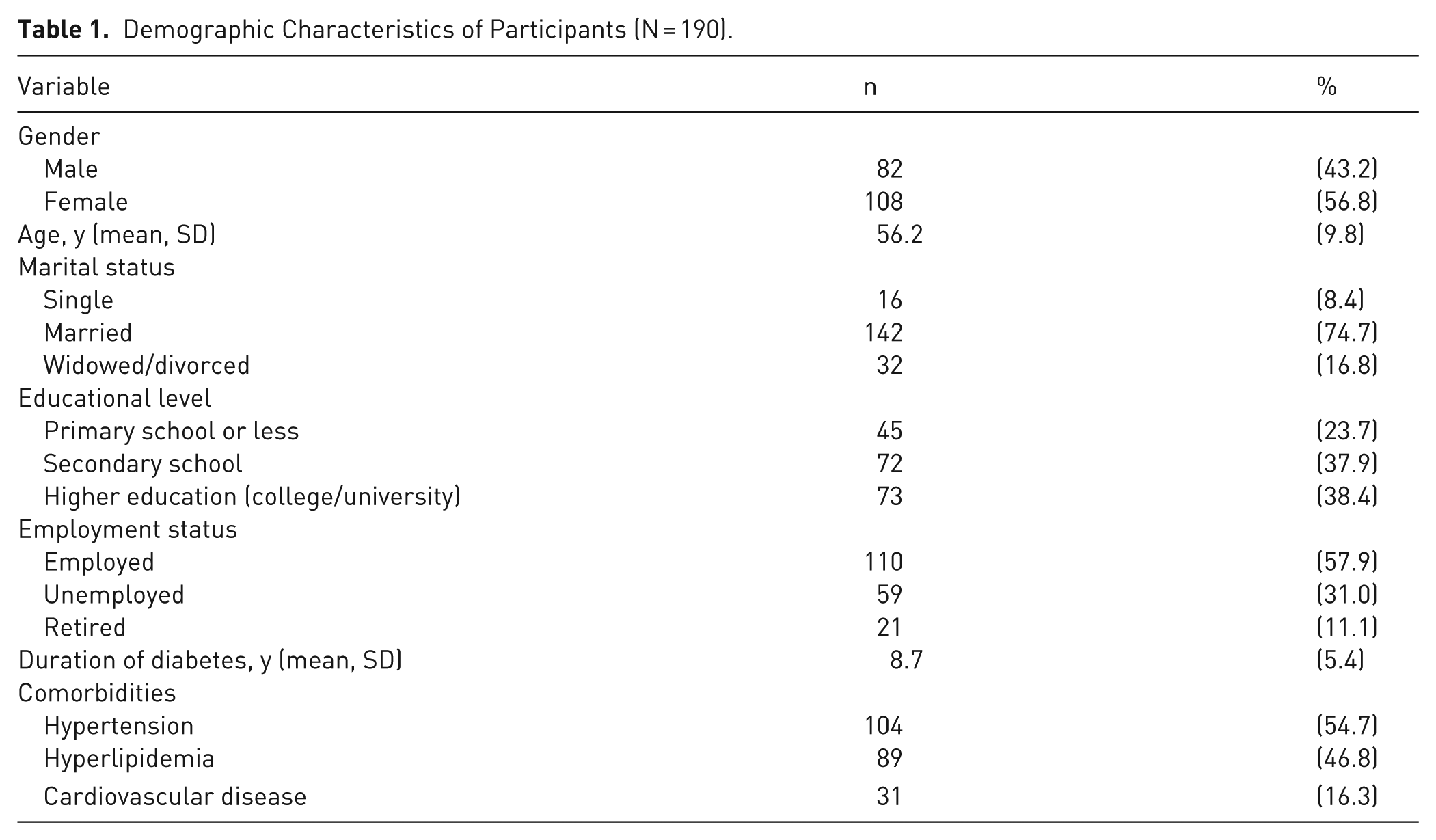
In terms of educational background, 38.4% had attained higher education (college or university level), while 37.9% had completed secondary education, and 23.7% reported primary education or less. Regarding employment, 45.3% were currently employed, 35.3% were retired, and 19.5% were unemployed. The mean duration of diabetes was 8.7 years (SD = 5.4), with a range from 1 to 25 years, indicating a wide spectrum of disease progression among participants.
Comorbid conditions were common, with more than half of the participants reporting hypertension (54.7%) and nearly half reporting hyperlipidemia (46.8%). Cardiovascular disease was also reported by 16.3% of the sample. These clinical characteristics underscore the complexity of managing type 2 diabetes in a population frequently burdened by multiple chronic conditions.
Descriptive Statistics of Key Study Variables
The mean total score of the I-DSAS-2 was 54.6, indicating a moderate level of perceived stigma among participants. Among the subscales, the Blame and Judgement domain yielded the highest mean score (20.4), followed by Treated Differently (18.4) and Self-Stigma (15.8), suggesting that externally imposed stigma may be more prominent than internalized stigma in this population.
The mean A1C level was 8.2%, reflecting suboptimal glycemic control in the overall sample. Participants reported a moderate degree of fatigue, as measured by the IMFI-20, with a mean total score of 61.4. Additionally, depressive symptoms assessed using the BDI-II yielded a mean score of 18.7 (Table 2), suggesting that many participants experienced mild to moderate levels of depression.
Descriptive Statistics of Main Study Variables (N = 190).
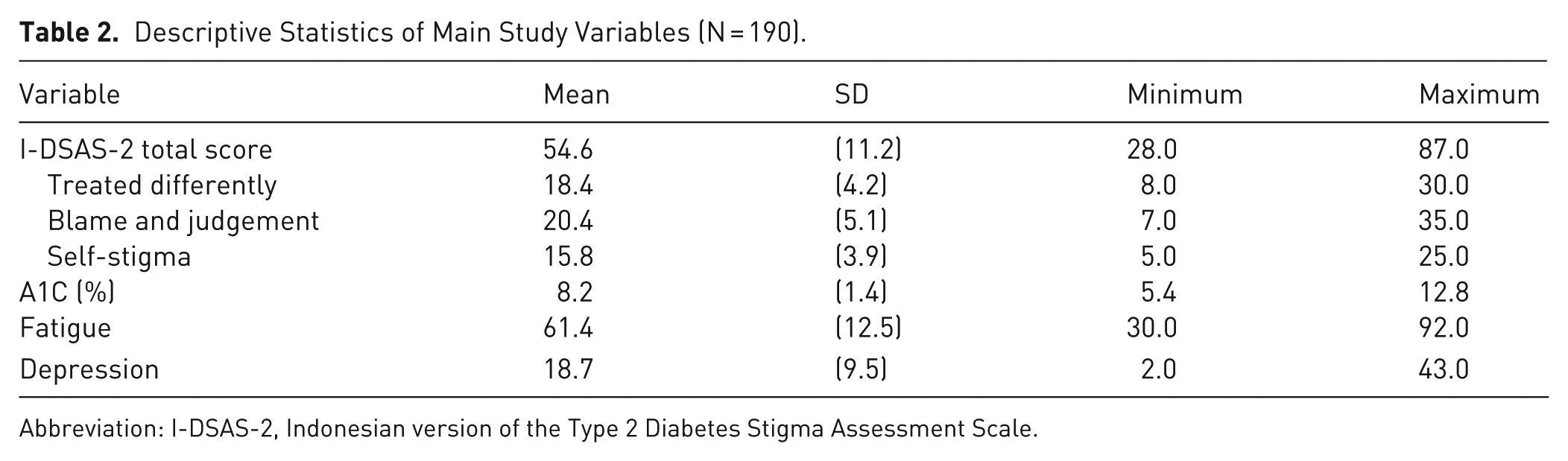
Abbreviation: I-DSAS-2, Indonesian version of the Type 2 Diabetes Stigma Assessment Scale.
Psychometric Evaluation of the I-DSAS-2
Exploratory factor analysis confirmed a 3-factor structure consistent with the original instrument, comprising the subscales Treated Differently, Blame and Judgement, and Self-Stigma. The KMO measure of sampling adequacy was 0.80, and Bartlett’s test of sphericity was statistically significant, χ²(171) = 1523.47, P < .001, indicating that the data were suitable for factor analysis. The number of factors was determined based on eigenvalues greater than 1.0 and inspection of the scree plot. The 3 extracted factors had eigenvalues of 7.12, 2.41, and 1.63, respectively, and together explained 62.8% of the total variance. Factor loadings across items ranged from 0.68 to 0.81 (Table 3), indicating good construct validity.
Psychometric Evaluation of the Indonesian Version of the I-DSAS-2.
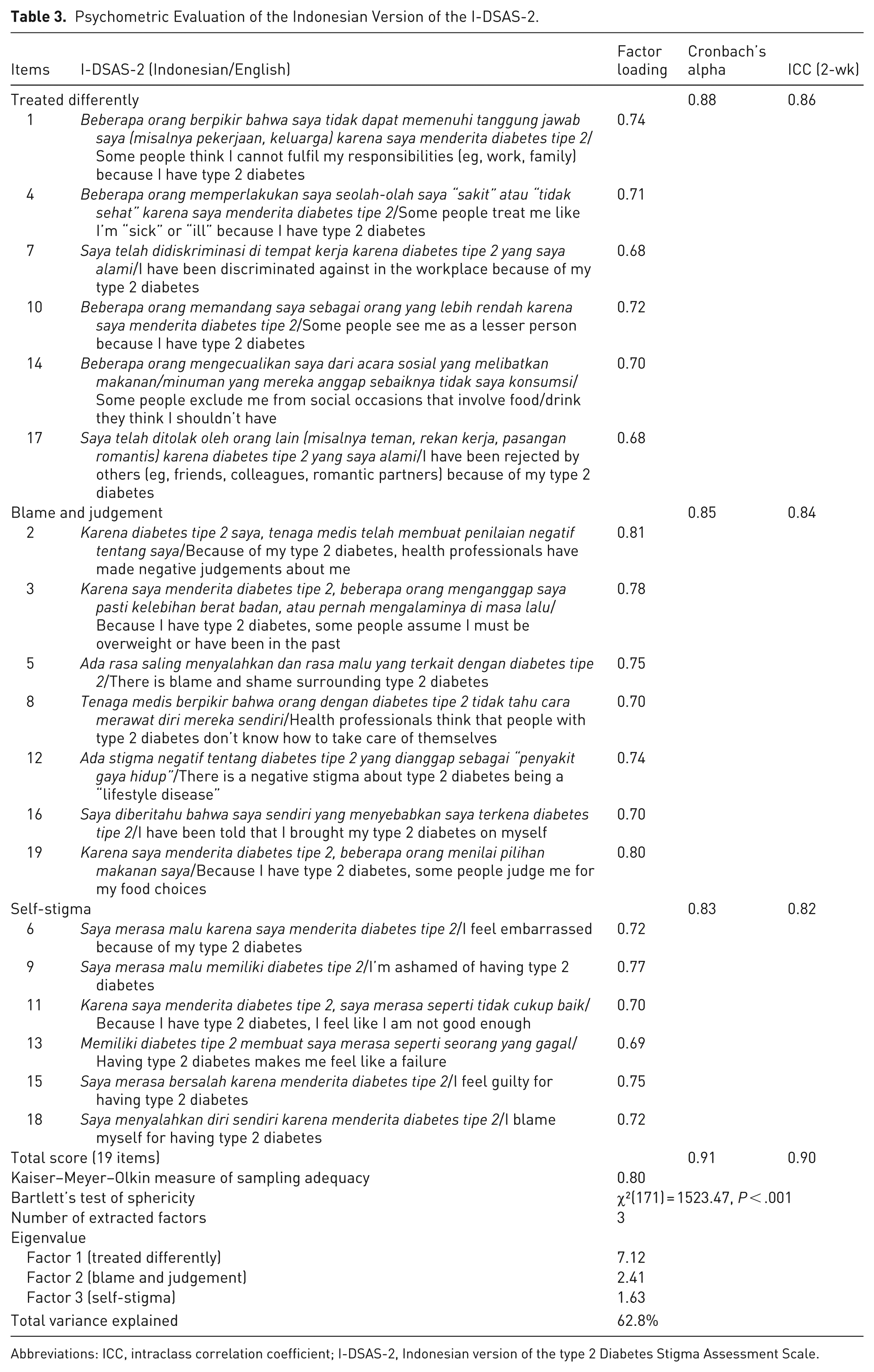
Abbreviations: ICC, intraclass correlation coefficient; I-DSAS-2, Indonesian version of the type 2 Diabetes Stigma Assessment Scale.
Internal consistency, assessed using Cronbach’s alpha, was high for the total scale (α = 0.91) as well as for each subscale: Treated Differently (α = 0.88), Blame and Judgement (α = 0.85), and Self-Stigma (α = 0.83). These values exceed the commonly accepted threshold of 0.70, indicating strong internal reliability of the instrument. Test-retest reliability over a 2-week interval was evaluated in a subsample of 30 participants, with ICCs ranging from 0.82 to 0.86 for the subscales and 0.90 for the total scale (Table 3), reflecting good to excellent stability over time.
Correlations Between Diabetes-Related Stigma and Clinical Outcomes
Table 4 displays the Pearson correlation coefficients between scores on the I-DSAS-2 and key clinical outcomes, including A1C, fatigue, and depressive symptoms. All correlations were positive and statistically significant, indicating that higher levels of perceived stigma were consistently associated with poorer clinical and psychological outcomes. Specifically, the total stigma score demonstrated a moderate positive correlation with A1C (r = .26, P < .01), suggesting that individuals experiencing greater stigma were more likely to have suboptimal glycemic control. In relation to fatigue, the total I-DSAS-2 score showed a stronger correlation (r = .41, P < .01), reflecting the potential psychosomatic toll of stigma in diabetes management. The strongest association was found between stigma and depressive symptoms (r = .54, P < .01), underscoring the significant psychological burden of living with type 2 diabetes in the context of stigma. Among the subscales, Self-Stigma yielded the highest correlation with depression (r = .51), while Treated Differently and Blame and Judgement also contributed significantly to fatigue and emotional distress.
Correlation Between I-DSAS-2 Scores and Clinical Outcomes.
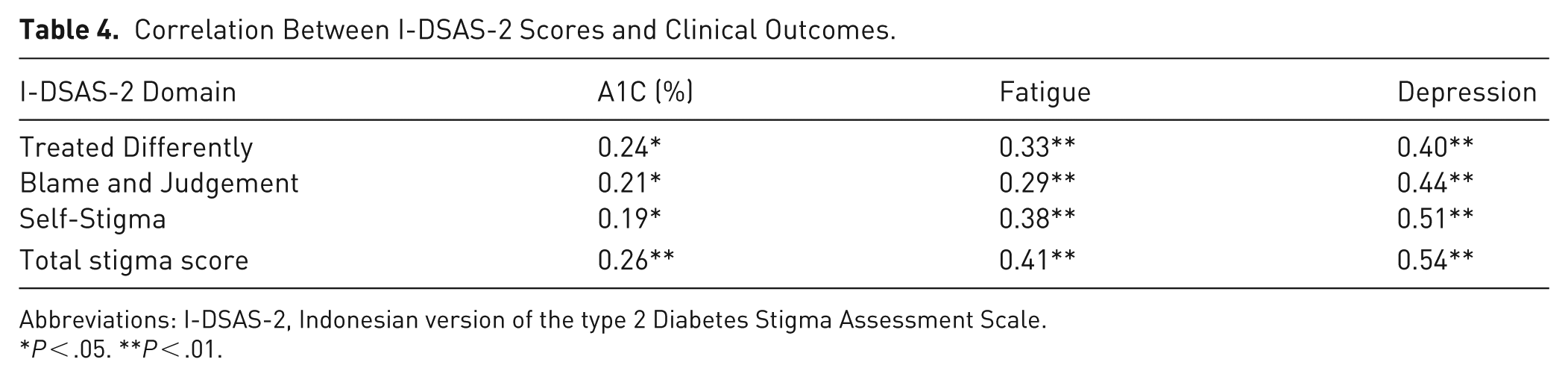
Abbreviations: I-DSAS-2, Indonesian version of the type 2 Diabetes Stigma Assessment Scale.
P < .05. **P < .01.
Multiple Linear Regression: Predicting Clinical Outcomes From Stigma
Table 5 presents the results of multiple linear regression analyses examining the predictive role of diabetes-related stigma, as measured by the total I-DSAS-2 score, on key clinical outcomes: A1C, fatigue, and depressive symptoms. Each model was adjusted for age, gender, duration of diabetes, and comorbidities to account for potential confounding influences. In the model predicting A1C, the total stigma score was a significant positive predictor (B = 0.12, 95% CI, 0.03-0.21, P = .01), indicating that higher perceived stigma was associated with poorer glycemic control. Although other covariates such as age and gender were not significant in this model, the direction of the association suggests that stigma contributes uniquely to metabolic outcomes.
Multiple Linear Regression Analysis Predicting Clinical Outcomes From I-DSAS-2 Score.
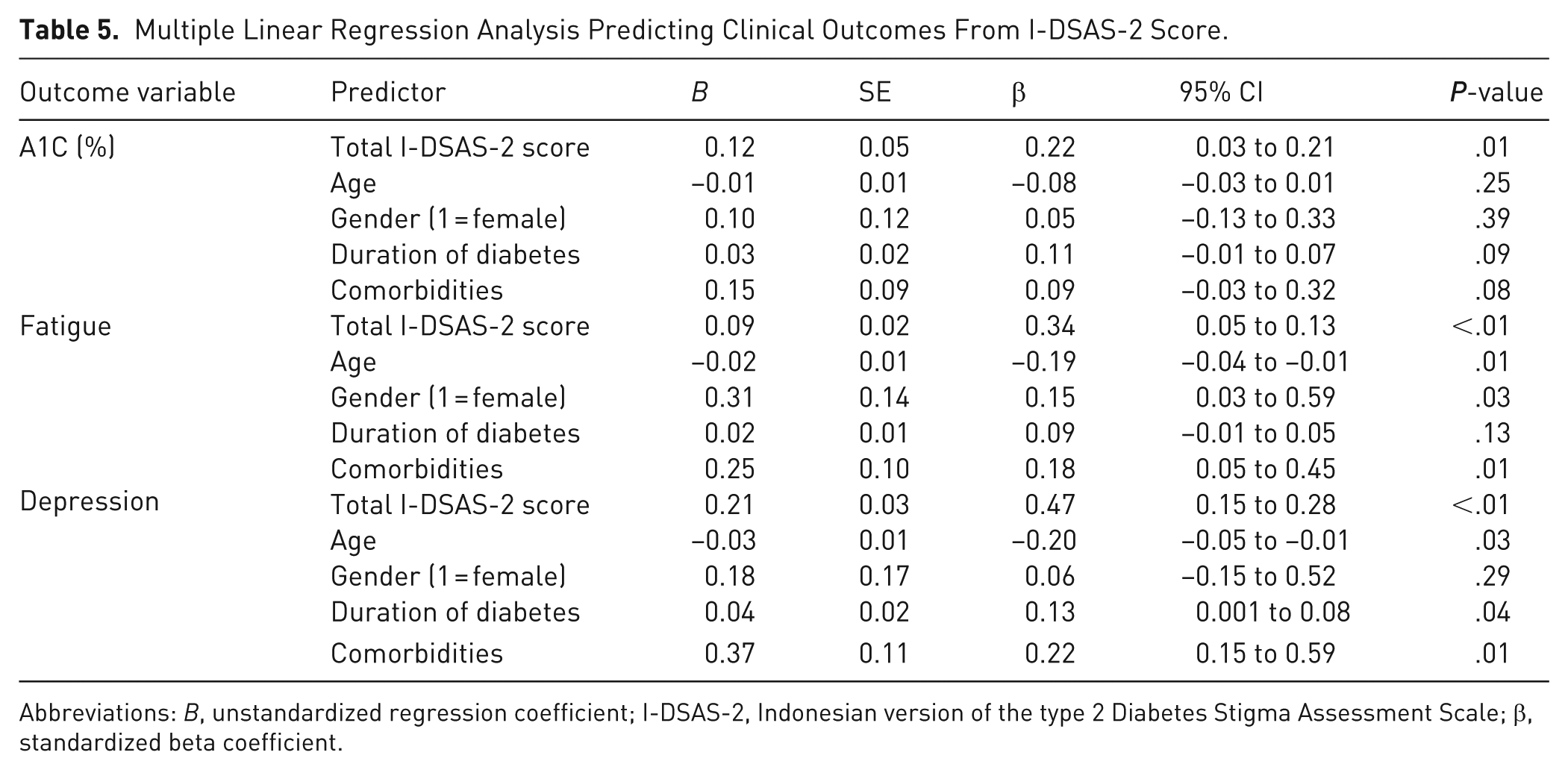
Abbreviations: B, unstandardized regression coefficient; I-DSAS-2, Indonesian version of the type 2 Diabetes Stigma Assessment Scale; β, standardized beta coefficient.
For fatigue, stigma demonstrated a robust and statistically significant effect (B = 0.09, 95% CI, 0.05-0.13, P < .001), with higher stigma levels predicting greater fatigue severity. Notably, younger age (B = –0.02, P = .007) and female gender (B = 0.31, P = .028) were also significant predictors, suggesting demographic vulnerability to fatigue among stigmatized individuals. The presence of comorbidities was independently associated with higher fatigue scores (B = 0.25, P = .01).
The strongest predictive relationship emerged in the model for depression, where stigma showed a large effect size (B = 0.21, 95% CI, 0.15-0.28, P < .001). In addition, younger age, longer diabetes duration, and the presence of comorbidities significantly contributed to higher depression scores. These results suggest that stigma plays a central role in the emotional burden of diabetes beyond demographic and clinical characteristics.
Discussion
The findings of this study demonstrate that diabetes-related stigma is not only prevalent among Indonesian adults with type 2 diabetes but is also significantly associated with key clinical outcomes. Participants with higher levels of perceived stigma tended to report poorer glycemic control, greater fatigue, and more severe depressive symptoms. Notably, depressive symptoms showed the strongest association with stigma, particularly with internalized or self-directed stigma, underscoring the profound emotional toll that stigma imposes on individuals managing a chronic condition.
The I-DSAS-2 exhibited excellent psychometric performance. The scale demonstrated strong internal consistency and temporal reliability, confirming its robustness as a culturally adapted tool for assessing the multifaceted nature of diabetes-related stigma. Exploratory factor analysis supported the original 3-domain structure (treated differently, blame and judgement, and self-stigma) with clearly defined item loadings, indicating that the underlying conceptual dimensions of stigma are relevant and meaningful in the Indonesian context. Consistent with prior validations of the DSAS-2 in Arabic-, Turkish-, Chinesse-, and Spanish-speaking populations,11 -14,33 the current study adds to the growing body of evidence supporting the scale’s cross-cultural applicability and psychometric robustness.
Beyond its measurement properties, the scale proved clinically informative. Correlation analyses revealed consistent positive associations between stigma and all measured outcomes, with particularly strong links to fatigue and depression. These findings align with international literature indicating that stigma can manifest in both psychological and somatic symptoms,1 -3 potentially undermining self-care behaviors, medication adherence, and motivation for health maintenance.34 -37 That stigma also correlated with A1C, a biological marker, suggests that its impact extends beyond perception and emotion, influencing physiological health as well.1,38
Multivariate analyses confirmed that diabetes-related stigma is a significant independent predictor of glycemic control, fatigue, and depression even when accounting for demographic and clinical factors, such as age, gender, duration of diabetes, and comorbidities. These findings reinforce the need to recognize stigma as not only a social issue but also a clinically significant factor that warrants integration into diabetes care protocols. Incorporating stigma screening into routine practice alongside culturally sensitive interventions to reduce both perceived and internalized stigma could contribute to more holistic, equitable, and effective chronic disease management in Indonesia.
The results of this study have important implications for practice. Diabetes care and education specialists should recognize that stigma is a critical barrier to effective self-management and patient engagement. Specialists can integrate stigma-reducing strategies into their practice, such as screening for stigma using tools like the I-DSAS-2. Identifying individuals who experience higher levels of stigma can lead to more targeted interventions that provide not only medical care but also psychosocial support. Incorporating psychosocial support into routine diabetes care can help reduce the negative emotional impact of stigma, improve self-care behaviors, and enhance adherence to treatment regimens.
Additionally, culturally sensitive interventions tailored to the Indonesian context are essential. Diabetes care specialists should be trained to provide a nonjudgemental, empathetic environment, fostering open communication about the emotional and psychological burdens of living with diabetes. Addressing both the physical and psychosocial aspects of diabetes care is critical to improving the overall quality of life for individuals with type 2 diabetes.
Strengths and Limitations
A key strength of this study lies in its rigorous psychometric evaluation of the Indonesian version of the DSAS-2, utilizing robust methodologies, including exploratory factor analysis, internal consistency testing, and test-retest reliability to ensure the instrument’s validity and reliability in a culturally distinct context. Additionally, the inclusion of both psychosocial and clinical indicators (A1C, fatigue, and depression) allowed for a comprehensive assessment of the real-world implications of diabetes-related stigma on patient well-being and health outcomes.
However, this study is not without limitations. First, the use of a cross-sectional design precludes the ability to infer causal relationships between stigma and clinical outcomes, warranting further longitudinal research. Second, participants were recruited from outpatient clinics in specific regions of Indonesia, which may limit the generalizability of findings to broader populations, including those in rural or underrepresented areas.
Conclusion
The I-DSAS-2 has proven to be a valid and reliable instrument for measuring stigma among individuals with type 2 diabetes. Higher stigma scores were significantly linked to poorer glycemic control, increased fatigue, and more severe depressive symptoms. These findings emphasize the importance of addressing emotional and social aspects of diabetes care alongside physical health. By including stigma assessment in routine clinical practice and offering supportive interventions, health care providers can improve both mental well-being and disease outcomes. The I-DSAS-2 offers a practical tool for advancing patient-centered diabetes care in Indonesia.
Supplemental Material
sj-docx-1-tde-10.1177_26350106261451193 – Supplemental material for Psychometric Evaluation of the Indonesian Version of the Type 2 Diabetes Stigma Assessment Scale and Its Clinical Correlates With Glycated Hemoglobin, Fatigue, and Depression
Supplemental material, sj-docx-1-tde-10.1177_26350106261451193 for Psychometric Evaluation of the Indonesian Version of the Type 2 Diabetes Stigma Assessment Scale and Its Clinical Correlates With Glycated Hemoglobin, Fatigue, and Depression by Debby Syahru Romadlon, Samia Salim Alharrasi, Mickael Antoine Joseph, Rudy Kurniawan, Safiruddin Al Baqi and Mario Pratama in The Science of Diabetes Self-Management and Care
Footnotes
Ethical Considerations
Ethical clearance for this study was granted by the Joint Institutional Review Board of the Ethical Committee for Medical Research at the Faculty of Dentistry, University of Jember (Approval No. 2311/UN25.8/KEPK/DL/2025).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ratchadaphiseksomphot Endowment Fund, Chulalongkorn University (The Exchange Faculty Travel Grant; Grant No. RSF-EFT1-69-05-23-02) to DSR.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Specific data files used in the analysis are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.