
Abstract
Background:
Bony Bankart lesions (anteroinferior glenoid avulsion fractures) often occur after anterior shoulder dislocations, with an incidence up to 33% in first-time dislocaters. Detachment of the labrum and underlying glenoid bone piece can lead to recurrent instability, especially with increasing glenoid bone loss. Treatment is generally arthroscopic bony Bankart repair in acute injuries with viable bone fragments and minimal glenoid bone loss (<13.5%). However, there is no gold standard for arthroscopic fixation.
Indications:
Given the acuity of the lesion with a sizeable bony Bankart fracture, a reducible fragment, and the patient's high activity level, arthroscopic reduction and fixation were indicated.
Technique Description:
A high posterolateral viewing portal was created, with the remainder of the portals created under direct visualization. The fracture hematoma was debrided with a shaver. The anterior glenoid fracture was identified with the labrum still attached, and a radial tear of the superior labrum was noted. A combination of instruments was used to release and mobilize the fracture fragment. Two traction stitches were placed into the superior and inferior ends of the fragment to control it during reduction. A hooked guide was used to reduce the fracture back to its origin. A cannulated drill was used to drill through the posterior glenoid through the fracture fragment. The suture and the button were passed anterior to posterior to secure the fragment, tensioned to 100 N, and the fragment was stable in an anatomic position. A luggage tag suture was placed into the capsular-labral complex at the superior aspect of the bony Bankart lesion, and this was impacted just superior to the end of the fracture fragment to secure the labrum back in place.
Results:
The patient was immobilized in a sling for weeks 0 to 4, progressed in range of motion from weeks 5 to 12, and began strengthening at 12 weeks. At the final follow-up, the patient was back to his usual activities without complaints of pain or apprehension.
Discussion/Conclusion:
Arthroscopic reduction and suspensory button fixation of bony Bankart lesions is a viable option for reducing and fixing these injuries to prevent future development of recurrent instability.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.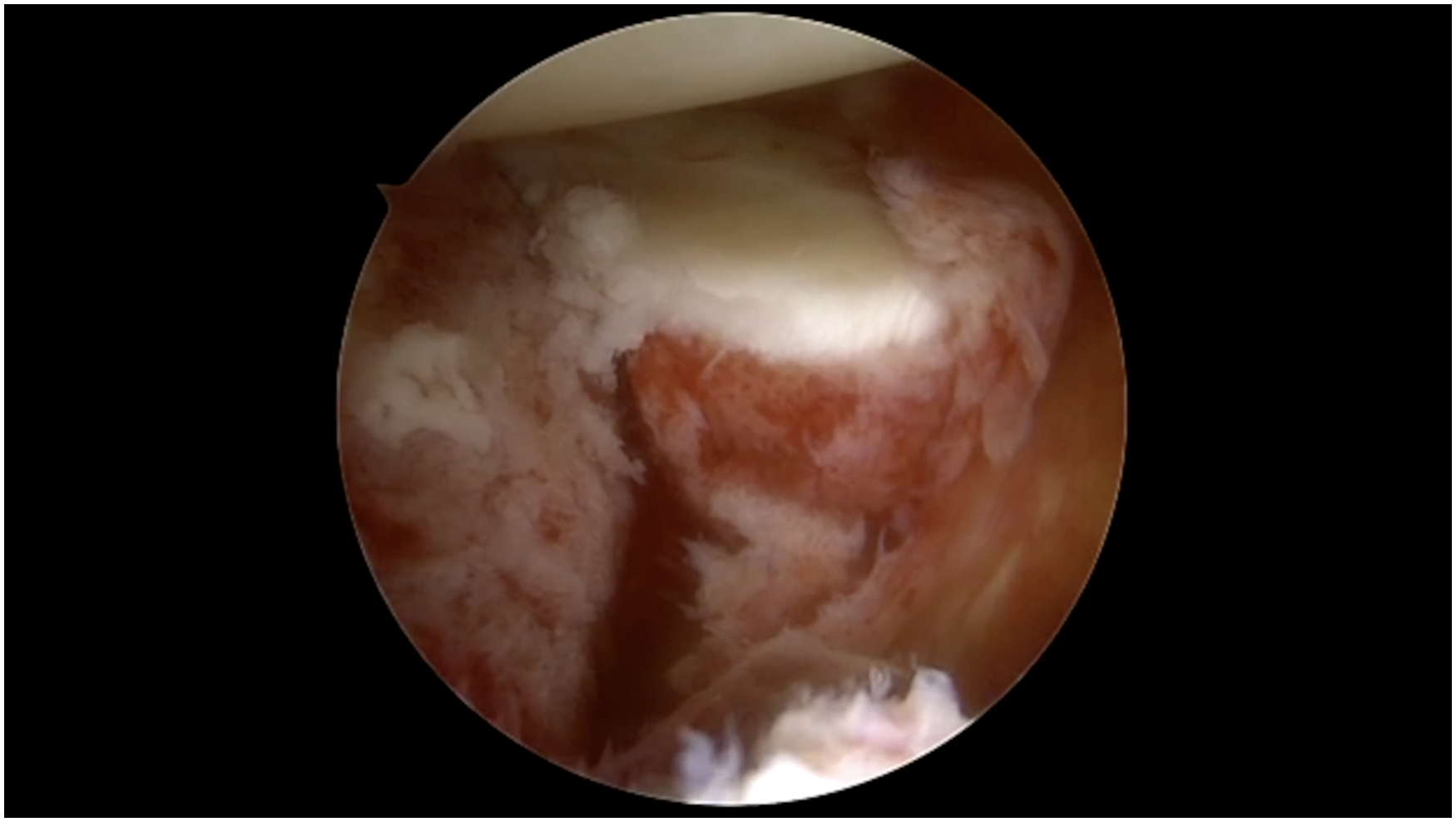
Video Transcript
My name is Joe Tramer. I am one of the orthopaedic sports surgeons at the Cleveland Clinic, and it is my pleasure to share with you a case of arthroscopic reduction and suspensory button fixation of a bony Bankart lesion.
Background
Bony Bankart lesions—or fractures of the anteroinferior glenoid—can occur even after first-time dislocations.4,6 Detachment of both the labrum and the underlying piece of bone can lead to recurrent instability. 2 Thus, treatment for these acute bone fragment injuries is often a Bankart repair. There are multiple methods for fixation—including open and arthroscopic—without a current gold standard for treatment.1,3,5
This patient was a 22-year-old right-hand–dominant male. He fell snowboarding 2 weeks before his clinic visit and dislocated his shoulder, which reduced spontaneously. He presented to an emergency room locally, where radiographs demonstrated this bony Bankart fracture, and he was discharged in a sling to follow up with us at home. He works in health care and is recreationally active in multiple activities.
Physical examination was remarkable mostly for apprehension, even at lower levels of abduction, which may indicate bone loss in the setting of instability.
Outside radiographs from his emergency room visit demonstrate a small anteroinferior glenoid fracture consistent with a bony Bankart-type injury.
A computed tomography scan with 3-dimensional reconstruction was also ordered, which redemonstrates the displaced bony Bankart, which encompasses a large portion of the anteroinferior glenoid.
Indications
In general, indications for reduction and fixation of a bony Bankart fracture include an acute instability event with a reducible fragment of sufficient size. Potential contraindications include a comminuted fragment that may be difficult to accept fixation, or a chronic injury with a partially resorbed fragment, in which case a bone replacement type procedure may be necessary.
Given the size of the fragment and the patient's age and activity level, we discussed that this would be best treated operatively. We elected to proceed with an arthroscopic reduction and internal fixation acutely for this patient. It is also very reasonable to perform this as an open procedure, and this would be left up to the surgeon's discretion.
Technique Description
To perform the surgery, the patient was placed in the lateral decubitus position, with his arm in a suspensory device and a bump utilized for joint distraction. Standard arthroscopic portals were marked out here.
This is a view of the patient's shoulder in the lateral decubitus position from a posterior portal just off the edge of the acromion. We then introduce a spinal needle just superior to the subscapularis to ensure a good trajectory to the anteroinferior glenoid. Then, an 8.5-mm canula is placed in this interval to facilitate instrument passage.
Here, diagnostic arthroscopy is being performed, which shows a fracture hematoma with early scar formation and a sizeable bony defect in the anteroinferior glenoid. We then use a shaver to debride the hematoma and free up early scar formation to mobilize and visualize the fragment. An elevator is also useful for mobilization. To get a better view, an anterosuperior portal is created just behind the biceps tendon, and a camera is switched to view straight down the face of the glenoid.
Here, we gain a better appreciation of the size and location of the fragment and can do further mobilization with a combination of the elevator, as well as electrocautery, to release soft tissue attachments. A curved suture passer is then used to pass a suture around the intact labrum, attaching the fractured fragment to assist with reduction and mobilization.
We are now ready to introduce the hooked guide. Making the initial viewing portal high off the acromion allows us to make this additional posterior portal under direct visualization to ensure it is parallel with the glenoid face. The hooked guide is introduced over a half-pipe, and we can use it to trial an initial reduction. The hook, the traction stitch, and additional instrumentation through the anterior portal can assist in fragment manipulation. Once anatomic reduction is achieved, the capsular-labral complex is elevated off the bony piece to ensure the button sits flush against the bone once deployed.
Here, we have elected to place an additional traction stitch on the inferior aspect to help hold our reduction while we are drilling for the button. With the fracture reduced using the hook, the drill sleeve is advanced to the bone through an additional posterior portal. This will allow drilling across the fracture, with the drill exiting 5 mm medial to the hook tip. There is a hook guide that allows for drilling single- or double-button fixation, but fractures are often amenable only to single-button fixation, as in this case. It is critical to leave the drill sleeve in place as the drill bit is removed. Then, the sutures can be shuttled from an anterior to posterior direction out of the additional percutaneous posterior portal before the sleeve is removed.
Here, you can see the button has been deployed to the bone and sits flush on the anterior cortex. Before final tensioning, you can see that there is still a fracture gap and some mobility of the fragment. To help close this down, a tape is passed through the capsular-labral complex and impacted into the anterior face of the glenoid, utilizing a knotless anchor.
Additional fixation may also be performed above and below the fracture.
We will now demonstrate how to load the posterior button on a Sawbones model. A suture passer is used to pull each suture strand through the button. We then tie a nice knot using the technique shown here, which creates a sliding-knot-type construct. Once the knot is tied, it is dressed, and the button is delivered to the bone. The sutures are then loaded into a tensioner, tensioned to 100 N, cycled multiple times, and the button is secured with alternating half hitches.
Final probing demonstrates excellent fracture reduction, with stable fragments and a well-repaired capsular-labral complex.
Results and Discussion
There are certainly potential complications to this surgery. One would include neurovascular injury. The benefit of the arthroscopic approach is that there is less manipulation around the anterior and inferior neurovascular structures. With the posterior-to-anterior drilling, this is further minimized compared to an open technique. Additionally, fragment resorption can occur over time, potentially leading to recurrent instability if stable fixation is not achieved. Additionally, one should be ready to convert to an open reduction if necessary.
The patient was placed in a sling for 4 weeks and then focused on range of motion from weeks 5 to 12. He was able to perform gradual strengthening at 12 weeks and initiated plyometrics and return-to-sport progressions when he met certain strength measurements.
Return to full contact sports and skiing typically occurs around 6 months.
Initial postoperative radiographs show a well-reduced fracture with appropriately placed hardware.
Lateral and axillary views redemonstrate accurate hardware positioning and anatomic reduction.
A brief literature review on bony Bankart injuries was performed. A recent meta-analysis found that the vast majority of these patients were males, and after surgery, they had improved patient-reported outcomes with solid return-to-sport rates. The recurrent instability rate was about 12%. Predictors of surgical success included bone union after repair and when the final glenoid defect size was <5% of the total surface area. 6
Over time, the patient's radiographs remained stable, and he slowly returned to his activities. He had a greater range of motion and no apprehension at the final follow-up. There has been no repeat instability during the follow-up period, and he is back to his usual activities.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.