
Abstract
Background:
Bipolar patellofemoral chondral defects in young, active patients present a challenging clinical problem due to persistent pain, functional limitation, and complex biomechanical contributors. While cartilage restoration procedures such as matrix-induced autologous chondrocyte implantation (MACI), osteochondral allograft (OCA) transplantation, and tibial tubercle osteotomy (TTO) have demonstrated favorable outcomes individually, combined restoration strategies addressing both focal cartilage loss and patellofemoral mechanics are less well described. We performed a single-stage, triple-modality comprehensive patellofemoral cartilage restoration, including a trochlear OCA, a patellar MACI, and TTO to offload and realign the patellofemoral joint.
Indications:
The described combined procedure was indicated in a healthy, active 37-year-old female with bilateral symptomatic full-thickness bipolar patellofemoral chondral defects refractory to extensive nonoperative treatment. Imaging demonstrated bipolar patellofemoral cartilage lesions consisting of a full-thickness trochlear osteochondral defect and a full-thickness patellar chondral defect with associated lateral patellar subluxation but without instability, abnormal patellar height, or elevated tibial tubercle–trochlear groove distance.
Technique Description:
The patellar defect was prepared with stable vertical walls for MACI implantation while preserving the subchondral bone. The trochlear lesion was sized, reamed, and reconstructed using a size-matched fresh OCA prepared to achieve flush articular congruity. A TTO with approximately 1 cm medialization and anteriorization was performed to reduce patellofemoral contact pressures and protect the cartilage restoration constructs. The MACI graft was then trimmed to match the patellar defect and secured with fibrin glue. Standard layered closure and structured rehabilitation with protected weightbearing and early motion were utilized postoperatively.
Results:
At 5-month follow-up, the patient demonstrated improved pain, full patellar mobility, and range of motion from 0° to 135°, with return to baseline activities. Radiographs demonstrated healed tibial tubercle osteotomies and well-incorporated OCAs bilaterally. These findings are consistent with the existing literature, which demonstrates significant improvements in patient-reported outcomes after combined cartilage restoration and patellofemoral unloading procedures, including high satisfaction and return-to-sport rates after MACI, OCA, and TTO procedures.
Discussion/Conclusion:
This case demonstrates a comprehensive approach to bipolar patellofemoral cartilage disease that simultaneously addresses focal cartilage pathology and the underlying biomechanical environment. The literature supports the use of MACI for isolated chondral defects, OCA for osteochondral lesions with subchondral involvement, and TTO to improve graft protection and patellofemoral mechanics. Hybrid restoration strategies combining these techniques may provide favorable functional outcomes and joint preservation in appropriately selected patients. Further prospective studies are needed to clarify long-term survivorship, optimal graft selection, and return-to-sport outcomes after combined OCA/MACI reconstruction procedures.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.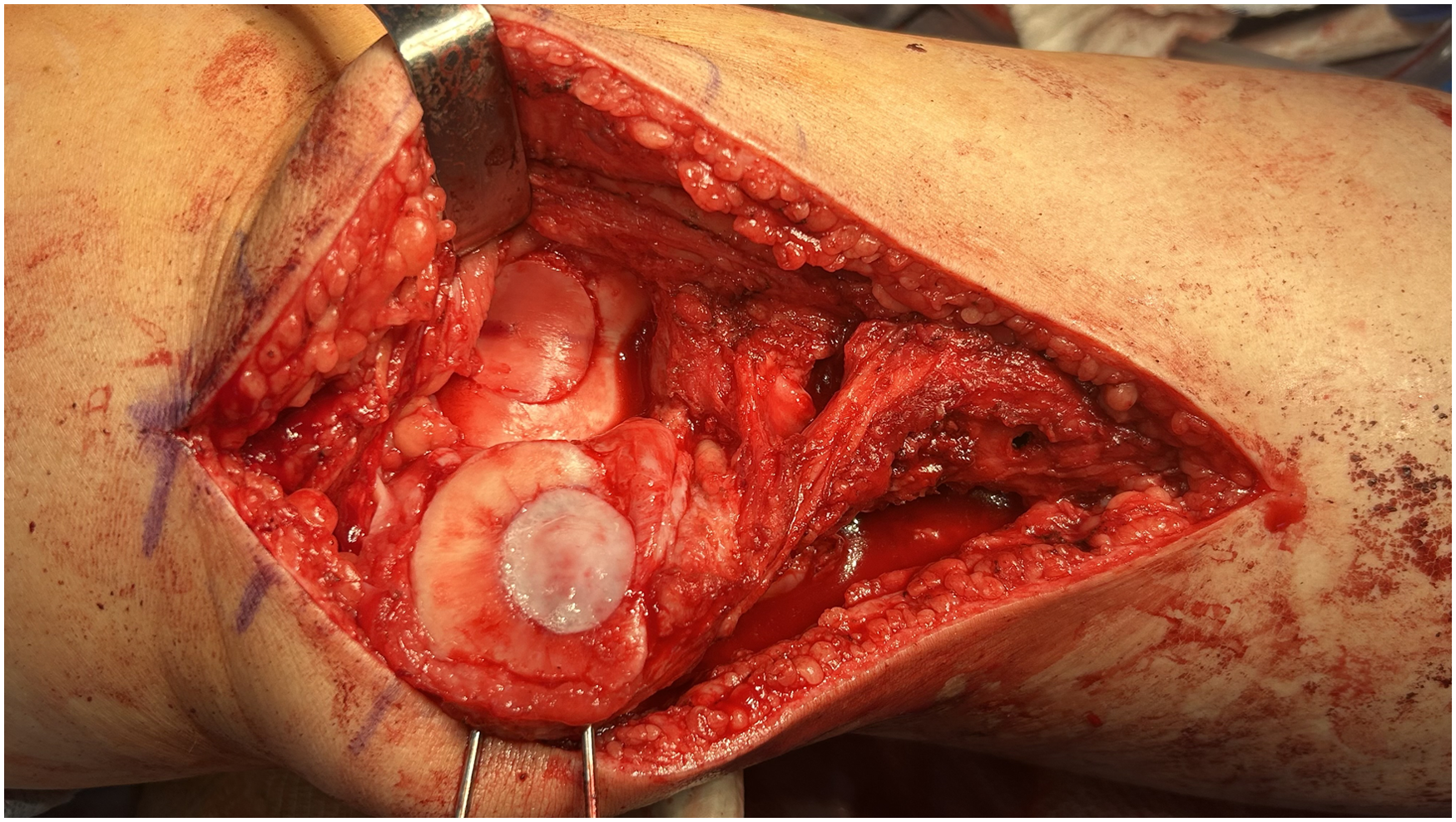
Keywords
Video Transcript
This is Dr Lauren Redler presenting a case demonstrating our technique for managing complex bipolar patellofemoral chondral defects with an unloading tibial tubercle osteotomy, osteochondral allograft to the trochlea, and matrix-induced autologous chondrocyte implantation to the patella.
Background
History
The patient is a healthy, active 37-year-old female with a history of bilateral anterior knee pain. She has failed an extensive conservative management, including physical therapy, anti-inflammatories, bracing, kinesiotaping, and injections of hyaluronic acid.
Physical Examination
On physical examination, she had a mild effusion, patellofemoral crepitus, tenderness on the lateral patella facet, and pain with compression. She had a full range of motion, and her knee was stable to varus and valgus stress. She had good quad activation and no ligamentous instability. Importantly, she had no signs of patellar instability and no J-sign.
Imaging
Preoperative radiographs demonstrate lateral patellar subluxation bilaterally. A magnetic resonance imaging of the right knee shows a full-thickness central trochlear chondral defect measuring 15 × 15 mm, as well as a full-thickness patellar chondral defect on the lateral patellar facet extending to the patellar apex measuring 17 × 20 mm. Her patellar height and tibial tubercle-trochlear groove were normal.
Treatment History
In November 2024, the patient underwent bilateral diagnostic knee arthroscopies to further evaluate her chondral lesions and determine their suitability for cartilage restoration. A matrix-induced autologous chondrocyte implantation (MACI) biopsy was taken at this time. Six weeks later, she underwent surgery on her left knee, including osteochondral allograft (OCA) transplantation to the trochlea, MACI to the patella, and unloading tibial tubercle osteotomy (TTO). After satisfactory recovery, we proceeded with a planned, staged, identical treatment of her right knee.
Indications
The combination of TTO, OCA to the trochlea, and MACI to the patella is indicated in young, active patients with symptomatic full-thickness patellofemoral chondral defects who have failed nonoperative management. Patients with articular chondral defects >2 cm2 without subchondral bone involvement are candidates for MACI. 4 Patients with full-thickness osteochondral lesions larger than 3 cm2 or with advanced degenerative patellofemoral changes are indicated for OCAs. 10 TTO is indicated to unload the restored cartilage by reducing patellofemoral contact pressures, as outcomes with autologous chondrocyte implantation (ACI) or MACI are consistently better when combined with realignment than with cartilage repair alone.1,2 Contraindications include global or multicompartment osteoarthritis, inflammatory arthropathy, active infection, deep subchondral bone defects on the patellar side, and uncorrected ligamentous instability or malalignment. 10
Technique Description
Approach
The patient was placed in the supine position. Tranexamic acid (TXA) was given before incision, which helped prevent the need for a tourniquet. A bump under the ipsilateral buttock can help prevent hip external rotation. A midline longitudinal incision provided adequate length to address patellofemoral cartilage restoration and to provide distal access for the TTO. Alternatively, these can be separate incisions with the more medially based parapatellar incision for the arthrotomy and an incision just off the lateral aspect of the tibial tubercle for the osteotomy. A medial parapatellar arthrotomy was then made, and the patella was everted with the help of two 2-mm K-wires in the medial border as joysticks. It is helpful at this stage to place the lateral facet of the patella in the trochlea to stabilize it during K-wire insertion.
Sizing Patellar Chondral Defect
The patellar chondral defect was then sized. The MACI 20 × 25 cutter best fits the defect. Coloring the edges of the MACI cutter with the marking pen is a useful tool for visualizing lesion boundaries. The lesion bed was then prepared by removing damaged cartilage with a combination of ring curettes and a 15-blade. It is important to avoid damage to the subchondral bone, as this can lead to bleeding. There is a tactile and audible change when you transition from the calcified cartilage to the subchondral bone. It is essential to create circumferential vertical walls. If there is any bleeding, you can place a thin layer of Tisseel, thrombin-soaked gel foam, or neuro patties on the lesion for hemostasis while you proceed with the other steps.
Sizing and Reaming Trochlear Defect
Attention was then turned to the trochlear OCA. The lesion was measured. The 22.5-mm cannulated sizing cylinder had the best circumferential fit. The cannulated sizer was used to place a guide pin in the center of the lesion to a depth of approximately 2 cm. These sizing guides and centralizers are designed to sit flush on the femoral condyles. There is no specific centralizer intended for the trochlea. It is imperative that the guide be placed perpendicular to the articular surface so that an identical anatomic plug can be harvested from the allograft to avoid any angular differences preventing your graft from sitting flush in the recipient site. The matching-sized 3-prong reamer was then used to ream the lesion to a depth of 10 mm at the high points on the medial and lateral edges of the trochlea, ensuring good containment on all sides. The base of the lesion was irrigated, and all debris was removed. Four measurements of the lesion depth were taken at each of the quadrants: 12:00, 3:00, 6:00, and 9:00. These depth measurements are critical and will guide how you prepare the donor graft to ensure flush articulation. A matching-sized dilator was then inserted into the socket to achieve a 0.5- mm socket dilation. The depth guide markings on the dilator were used to confirm the 4 measurements. A slap hammer was used to remove the dilator. The base of the recipient site was then drilled with a 1.6mm K-wire to promote marrow stimulation.
Preparing OCA
We then turned our attention to the fresh OCA on the back table. The matched donor graft was secured to the graft station. In this case, we are using an allograft trochlea. I find it a bit easier to secure the graft to the workstation and map out a matching contoured graft when the entire distal femur is present. It is helpful to position the allograft trochlea to match the patient's leg position on the operating table, accounting for the degree of flexion or extension of the distal femur. The matching bushing is placed into the articulating arm of the work station using the cannulated sizer to ensure we are perpendicular to the graft. The coring reamer was used to a depth of approximately 20 mm. Irrigation is helpful to prevent overheating. A reference mark was placed at the corresponding 12:00 position. Then, a sagittal saw was used perpendicularly to release the plug. Depth marks were placed at the 12:00, 3:00, 6:00, and 9:00 positions, matching the recipient site depths. A circumferential mark was then drawn on the bone corresponding to these depth measurements. The graft was then trimmed to the appropriate length. The graft base was waffled to aid compression, and the edges were bulleted to facilitate insertion. A graft that is too proud leads to increased contact stress; one that is too recessed can lead to instability. You should aim for a flush to 0.5 mm recessed. The plug was then pulse lavaged to remove all storage solution, then soaked in platelet-rich plasma spun from the patient's peripheral blood during the case.
Tibial Tubercle Osteotomy
Attention was then turned to the TTO. The anterior compartment was subperiosteally elevated off the tubercle. Staying subperiosteal and avoiding violation of the anterior compartment at this stage can help prevent bleeding. We want the shingle to be approximately 6 cm in length, so it is measured, and the planned distal aspect of the osteotomy is marked. Two guidewires were then placed from medial to lateral in a 45° trajectory to produce a 1 cm medialization and a 1 cm anteriorization. The sagittal saw was then used to perform the first cut of the osteotomy, staying parallel to the K-wire guidewires. The osteotomy was then completed with the osteotomes, ensuring the distal periosteal hinge remained intact. A small osteotome was used to make the traverse cut just proximal to the patellar tendon insertion. Next, we made an oblique cut laterally to connect the 2 cuts. The shingle was transferred 1 cm medially. We placed 2 K-wires for provisional fixation, and a radiograph was used to confirm length, position, and trajectory. It helps to have the second screw aim slightly inferiorly to diverge from the proximal screw, improving fixation and compression of the shingle. These were then measured and drilled. When drilling, it is important to go through the posterior cortex. Although some screws are self-drilling and self-tapping, I find that they have a hard time engaging the posterior tibial cortex here. One of the pitfalls of this stage is when placing the headless compression screws, as the screws start to engage the posterior cortex. If you approach the hold obliquely, it can start to displace your osteotomy and push the tubercle shingle back up. Keeping direct pressure on this shingle can help prevent this problem. If you encounter it, back the screw out and slightly adjust the trajectory to engage the far cortex in line with the drill tract. After medial translation of the tibial tubercle, check the lateral retinaculum. Here, there was some tension, so a lengthening was performed by separating the lateral retinaculum into superficial and deep layers.
Placing OCA
After the TTO was completed, we implanted the OCA in the trochlea. The recipient site in the trochlea was irrigated, and the OCA plug was placed by hand, using the 12 o'clock reference line to guide correct orientation. The impactor tamp was used with gentle mallet tamps to seat the graft until the chondral surfaces were flush on all sides. It is helpful to have the tamp halfway off the graft to avoid overimpaction, as crushing the cartilage surface can compromise the chondrocyte viability.
Preparing and Placing the MACI Graft
The final step for this complete patellofemoral restoration case was to place the MACI graft in the patella. The membrane was cut to match the exact size and shape of the defects. If the defect does not match one of the round or oval cutters, then a template of the defect can be made using a foil packet from a suture or scalpel blade, and the membrane can be free-cut with the tungsten carbide scissors that come in the set. It is important to orient the membrane correctly on the cutting block with the notch on the bottom left. This ensures that the rough side, the cell side, is up for cutting. This will be flipped when the graft is placed—the rough side will be down, cell side toward the bone, and the shiny side will be up. The same cutting guide that was used to prepare the patellar defect is then malleted into the silicone cutting block to cut the MACI graft. If your tray is missing the cutting block, a great trick is to use a folded blue towel and place a piece of Esmarch on top of it to create your own cutting block, as we did here. As I am preparing these grafts, I am always thinking about how I am going to place the cutter on the graft, particularly if multiple grafts are needed, or to have a backup option if something goes wrong. It is best to place the cutter eccentrically on the membrane. The oval cutter should be malletted all the way onto the silicone cutting block to ensure a complete cut of the MACI membrane. The silicone cutting block is a single-use item. The knee was then irrigated, and the patella chondral defect was patted dry, and a thin layer of fibrin glue was placed in the base of the lesion. The MACI graft was placed securely over the defect, cell side down. Be meticulous about ensuring the graft is flat and well-positioned before applying a thin layer of fibrin glue to the edges to stabilize it.
Closure
The K-wire joysticks were then removed from the patella. Remove them carefully, as they can be bent. The lateral lengthening was then closed with 0 Vicryl sutures, achieving a total of 1cm of additional length. Quickset was then placed at the osteotomy site to aid in healing. The anterior compartment was repaired to the tubercle with 2 figure 8 stitches. A formal anterior compartment fasciotomy was not done because we used TXA to decrease bleeding.
Results
A hinged knee brace was placed, and a continuous passive motion machine was utilized starting on postoperative day 1. The patient was made nonweightbearing for two weeks and partial weightbearing for 2 weeks. At 4 weeks, she started a slow progression to weightbearing as tolerated (WBAT) with a goal of full WBAT between 6 and 8 weeks. At a 5-month follow-up visit, the patient had good patellar mobility and 0° to 135° range of motion and reported improvement in pain. She had returned to all baseline activities. Bilateral knee radiographs demonstrated well-incorporated OCA bilaterally and healed tibial tubercle osteotomies. Her outcome is consistent with outcomes reported in the literature. Statistically significant improvements across multiple clinical outcome scores—including International Knee Documentation Committee, Lysholm, Knee injury and Osteoarthritis Outcome Score, Tegner, and Short Form scores—have been demonstrated in patients undergoing MACI combined with patellofemoral osteotomy, 9 and prospective data demonstrate an 86% satisfaction rate among patients undergoing ACI of the patellofemoral joint with concomitant anteromedialization. Regarding return to sport, 83% of patients return to at least 1 sport at a mean of 7.8 months after TTO for patellofemoral pain. 7 While data for massive OCA of the trochlea remain limited, 100% of patients returned to sport at a mean of 8.2 months after particulated juvenile articular cartilage allograft transplantation for patellofemoral cartilage defects. 8 At 2 years after MACI, 85% of patients were satisfied with their ability to return to recreational activities, and 66% reported satisfaction with their ability to participate in sports. 3
Discussion
This case of complete patellofemoral restoration exemplifies a comprehensive approach that addresses both the cartilage defects and their underlying biomechanical malalignment. Existing evidence supports each element of this strategy. In a landmark 12.6-year follow-up study, Vasiliadis et al 11 demonstrated that patients with patellar malalignment who underwent realignment achieved outcomes comparable to those who did not require realignment—affirming that addressing the mechanical environment is as important as the cartilage repair itself. Krueger et al 6 recently showed that trochlear OCA grafts had greater survivorship than isolated patellar or bipolar grafts, with outcomes comparable to femoral condyle OCA. In a systematic review of 249 knees with bipolar patellofemoral lesions, Gowd et al 5 showed favorable outcomes in at least 80% of patients who underwent ACI at short- to mid-term follow-up. This evidence supports the algorithm demonstrated here: MACI for the purely chondral patellar defect, OCA for the trochlear lesion with subchondral involvement, and TTO to protect both grafts by reducing patellofemoral contact pressures. Prospective studies are needed to define optimal graft selection in bipolar disease and to assess the long-term survivorship of hybrid OCA/MACI constructs. While each component of this combined procedure demonstrates favorable return-to-sport outcomes in isolation, dedicated prospective data on return to sport after the combined procedure is needed to better characterize expectations for this patient population.
Conclusion
This case highlights a combined approach—TTO, trochlear OCA, and patellar MACI—that treats focal cartilage defects while correcting the underlying biomechanics. The current literature supports each component of this strategy, and existing evidence suggests that such tailored, combined techniques can achieve favorable functional results and joint preservation at short- to mid-term follow-up. Further studies are needed to refine indications, procedural thresholds, and long-term durability of these hybrid reconstruction strategies.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: L.H.R. is a paid speaker for ConMed; is a paid consultant for Moximed, GLG, Guidepoint, and Versed; is a board member of PRiSM and FORUM; is a committee member of EOA; and has stock or stock options in Relief Health. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.