
Abstract
Background:
Preterm birth (PTB) is the leading cause of neonatal death and a major contributor to under-five mortality. Women’s awareness, knowledge, and ability to recall PTB-related themes are essential for prevention and care but remain understudied in Europe.
Objectives:
To describe self-appraised awareness of PTB, PTB themes recalled from discussions with health care professionals (HCPs), perception of personal PTB risk, and recognition-based knowledge score.
Materials and Methods:
We conducted a cross-sectional, web-based survey of pregnant women at 12–32 weeks’ gestation in five European countries. Analyses were stratified by country and by PTB risk.
Results:
The analytic sample comprised 247 women, of whom 111 (44.9%; 95% confidence interval [CI], 38.9–51.2) were classified as at higher PTB risk. Among these, 35.1% (95% CI, 26.9–44.4) did not recognize their higher PTB risk in the current pregnancy despite a previous PTB. Differences in awareness were observed between countries, with no differences across PTB risk strata. Recall of PTB themes discussed with HCPs and the recognition-based knowledge score were low and did not differ across PTB risk strata. Topic-specific shortfalls in recall and recognition were identified.
Conclusions:
A disconnect emerged between feeling informed and retaining actionable knowledge. HCPs should reserve time with women to deliver education using evidence-based techniques (e.g., teach-back) to build, maintain, and reinforce recall of PTB knowledge so that women are not only aware but also active participants in prevention, monitoring, and care.
Keywords
Introduction
Preterm birth (PTB) is the leading cause of neonatal death and a major contributor to under-five mortality, with nearly one million neonatal deaths directly attributable to PTB each year.1,2 Neonatal disorders, including those caused by PTB, remain among the largest contributors to disability-adjusted life-years, with little improvement since 1990. 3 Profound survival inequalities persist: in high-income countries, more than 90% of extremely preterm infants survive, whereas, in low-income settings, fewer than 10% do. 2
Converging global crises, including armed conflict, climate change, and the COVID-19 pandemic, weaken health systems, heighten maternal and newborn vulnerability, amplify environmental risk factors, and disrupt evidence-based practices for preventing and managing PTB.4–9 In 2020, an estimated 13.4 million babies were born preterm (9.9% of all live births), and in 2023, there were approximately 2.3 million neonatal deaths.10,11
PTB has lifelong consequences and can propagate susceptibility across generations through genetic and maternal-health pathways.12–14 Survivors face lifelong, multisystem sequelae with associated educational and economic challenges.12–14 For families, a PTB often involves ongoing psychological distress, caregiving burdens, and substantial direct and indirect costs.15–17
Many PTBs are preventable with progestogens and high-quality antenatal care for women at high risk,2,18,19 yet accurate risk assessment, persistent inequities, and implementation gaps leave global PTB rates largely unchanged and high-value care inconsistently delivered.20–25 In response, policy initiatives, including the World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) Every Newborn Action Plan (aligned with Sustainable Development Goal [SDG] target 3.2, ≤12 per 1000 by 2030), and the 2024 World Health Assembly resolution WHA77.5, along with social mobilization through the Global Alliance for Newborn Care (GLANCE), now integrated within initiatives of the Global Foundation for the Care of Newborn Infants (GFCNI), and World Prematurity Day, have advanced efforts to address PTB and raise public awareness.26–29
However, women’s awareness of PTB is pivotal for engaging and empowering women and families, a priority in WHO/UNICEF newborn health agendas, 2 and for enabling timely prevention and care. Direct assessments of awareness remain limited; most evidence comes from small, single-country qualitative studies and, to our knowledge, there are no pan-European data. 30 Accordingly, we conducted a five-country European survey with the primary objective of describing pregnant women’s awareness of neonatal risks associated with PTB (neonatal PTB risk awareness) overall and across five participating countries. Secondary objectives were to: (1) describe sources of information on neonatal PTB risks and themes recalled from discussions with health care professionals (HCPs) (recalled HCP-discussion themes); (2) compare neonatal PTB risk awareness between women classified as at risk (any risk) and those not at risk (non-at-risk) for PTB; (3) report the proportion of the history category, that is, respondents acknowledging prior PTB or preterm labor (PTL) without recognizing current pregnancy risk; (4) among women classified as any risk, describe recognition of personal PTB risk factors and HCP-recommended strategies to manage PTB risk; and (5) among women classified as non-at-risk, describe known PTB risk factors that women recall and strategies to manage potential PTB risk.
Materials and Methods
Study design
This was a cross-sectional, web-based survey of pregnant women in five European countries (France, Germany, Poland, the United Kingdom, and Sweden), conducted between April and May 2025. The study was designed to capture self-reported awareness, perceived risk, and counseling experiences related to PTB.
Setting
The survey was administered online in five countries selected to reflect diversity in health care systems and prenatal care provision. It was accessible on desktop and mobile and compatible with commonly used browsers. Online delivery enabled standardized administration across settings and real-time data capture.
Population and inclusion criteria
Eligible participants were pregnant women aged ≥ 19 years, at 12–32 weeks’ gestation, and residing in one of the five countries. Women outside these criteria were excluded at screening. Eligibility was self-reported in an initial screening questionnaire prior to survey entry.
Sampling and recruitment
Participants were recruited through invitation-only national online panels managed by Listen Lab partner organizations. Panel members are individuals who have previously consented to be contacted for research studies. For this survey, eligible panel members received a direct invitation to participate; no open recruitment or public advertising was used.
Data quality was supported through a combination of automated and manual safeguards implemented at the platform level. These included eligibility screening prior to survey entry, technical controls to prevent duplicate submissions, and postcollection review to exclude incomplete or internally inconsistent records. The same quality assurance procedures were applied across all participating countries.
An information statement preceded the survey; participation was voluntary, anonymous, uncompensated, and completion of the survey indicated informed e-consent.
Questionnaire design and testing
The instrument, developed by clinicians with expertise in maternal–fetal medicine, covered established PTB risk factors, preventive practices, and respondent characteristics. Draft items underwent expert review to support clarity and face validity. Prior to fielding, the survey underwent internal testing focused on technical functionality, including verification of survey logic, skip patterns, and item display on the web-based platform. The questionnaire was translated using forward–back procedures with native-language review to support semantic clarity and cultural appropriateness. Skip logic was applied to tailor item pathways based on eligibility and prior responses. The final questionnaire comprised 30 items in multiple-choice and open-ended formats.
Data collection platform, quality assurance, and privacy
Data were collected on Listen Lab’s platform with prespecified safeguards. Records were retained only if the automated quality score was ≥4 on a 1–5 scale, and ≥95% of essential items were complete (respecting skip logic). Manual review excluded duplicate or inconsistent entries. Responses were anonymized at entry; no identifiers were collected.
Data management and variable coding
Responses were collected in local languages. Closed items used prespecified, cross-country–comparable options. Open-text answers were translated into English and coded with a prespecified codebook, reconciling country-specific phrasings and lexical variants and handling explicit negations. Uniform quality control and deduplication procedures were applied across countries. Variable definitions and recoding rules are summarized below; full details are in Supplementary Methods S1.
Perceived PTB risk status (Q17/Q22): derived from the woman’s self-report of perceived risk status: history of previous PTL or PTB (history); current risk for PTB (current); both a history of previous PTL/PTB and a current risk (both). Evidence-based PTB risk status (recoded): operationalized, for decision-threshold purposes, as any risk (history, current, or both) versus non-at-risk (neither). This threshold-based classification is a pragmatic proxy for elevated versus lower risk and does not imply a dichotomous underlying risk based on self-reported survey data. Within any risk, we report the percentage distribution of history, current, and both. Specifically, we show the history percentage (prior PTB/PTL only) (1) as a share of any risk and (2) as a share of the total sample. The history category is interpreted as recognition of prior PTB/PTL without acknowledging a current pregnancy risk. Personal PTB risk factors (Q18): closed options reflect risk factors communicated by the HCP; the item is multiple-response. Selections are recoded to binary indicators. Risk burden count (RBC, from Q18): sum of fixed-option Q18 indicators to form the RBC (range, 0–15), excluding “other” and “none.” Strategies to manage PTB risk (Q20): multiple-response checklist based on the woman’s self-report of HCP-recommended strategies to manage PTB risk among those identified as at risk. Management strategy breadth—Core set (MSB-Core) and strategy-domain breadth (SDB) (from Q20): two indices derived from the Q20 checklist. MSB-Core assigns one point for each of eight core items (range, 0–8). SDB counts the number of distinct domains represented (range, 0–6). Neonatal PTB risk awareness (Q23): awareness of neonatal risks of PTB is analyzed on the original four-level scale and as a binary recode: high (moderately/very aware) versus low (not at all/somewhat). Sources of information on neonatal PTB risks (Q24): multiple-response item; selections are coded as binary indicators. Recalled HCP-discussion themes (Q25): open-text recall of up to three points regarding PTB discussions with an HCP is coded to predefined categories, allowing multiple themes per respondent. Where a response mixes a minor error with otherwise valid content, only valid themes are coded. Richness and recall quality index (derived measures for Q25): Recall richness is defined as recall of ≥2 distinct valid themes and reported as n/N (%) among nonblank responders. The recall quality index (0–2) combines richness (0/1) with content specificity (0/1); it is calculated among scorable nonblank responses (i.e., those with at least one coded content theme). Known PTB risk factors (Q26) and knowledge-breadth count (KBC): parallel to Q18 for non-at-risk women; same harmonized labels. KBC is the sum of selected Q26 indicators, that is, the number of PTB risk factors selected from a predefined checklist. It reflects recognition-based knowledge breadth rather than objective knowledge. Strategies to manage potential PTB risk (Q28) and indices from Q28: parallel to Q20 for non-at-risk women (using more aggregated labels); mapped to the same domains. MSB-Core and SDB are computed as for Q20. Free-text answers (Q19, Q21, Q27, and Q29): free-text responses are translated and coded to a prespecified framework. No free-text theme met prespecified reporting thresholds; content was pooled as “other (free-text)” and excluded from comparative testing and index construction.
Reporting standards
The study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology checklist for cross-sectional studies 31 and the Checklist for Reporting Results of Internet E-Surveys guidelines. 32
Statistical analysis
Analyses used valid-case denominators with pairwise exclusion of missing data. Categorical associations were tested with Pearson’s chi-square; when >20% of expected counts were <5 or any were 0, we used Fisher’s exact (with Monte Carlo estimation when appropriate). Effect sizes were Cramér’s V. Free-text categories were analyzed descriptively and itemized only if they met prespecified thresholds (at least five mentions in the analytic sample or at least 2% in two groups); where expected counts were <5 across contrasts, no formal testing was performed. Risk-stratified comparisons included country-level tests across perceived PTB risk status (history, current, and both; 3 × 5 chi-square) and any risk versus non-at-risk (2 × 5 chi-square). For selected binary outcomes, we reported prevalence ratios with 95% confidence intervals (CIs) using the Katz method (with a 0.5 Haldane–Anscombe correction if needed). Indices (RBC, KBC, MSB-Core, and SDB) were summarized as median and interquartile range (IQR) and as ordered classes, with chi-square on class distributions. Multiplicity was controlled using Benjamini–Hochberg false discovery rate (FDR) at 0.05 within conceptually related families. Two-sided p values and FDR-adjusted q values are reported. Analyses used IBM SPSS Statistics v28 (IBM Corp., Armonk, NY, USA).
Results
A total of 972 women began the survey across five European countries. Of these, 597 were excluded at the presurvey eligibility screen and 128 after data-quality review. The final analytic sample comprised 247 pregnant women (Fig. 1), by country: France (n = 52), Germany (n = 47), Poland (n = 56), the United Kingdom (n = 52), and Sweden (n = 40).
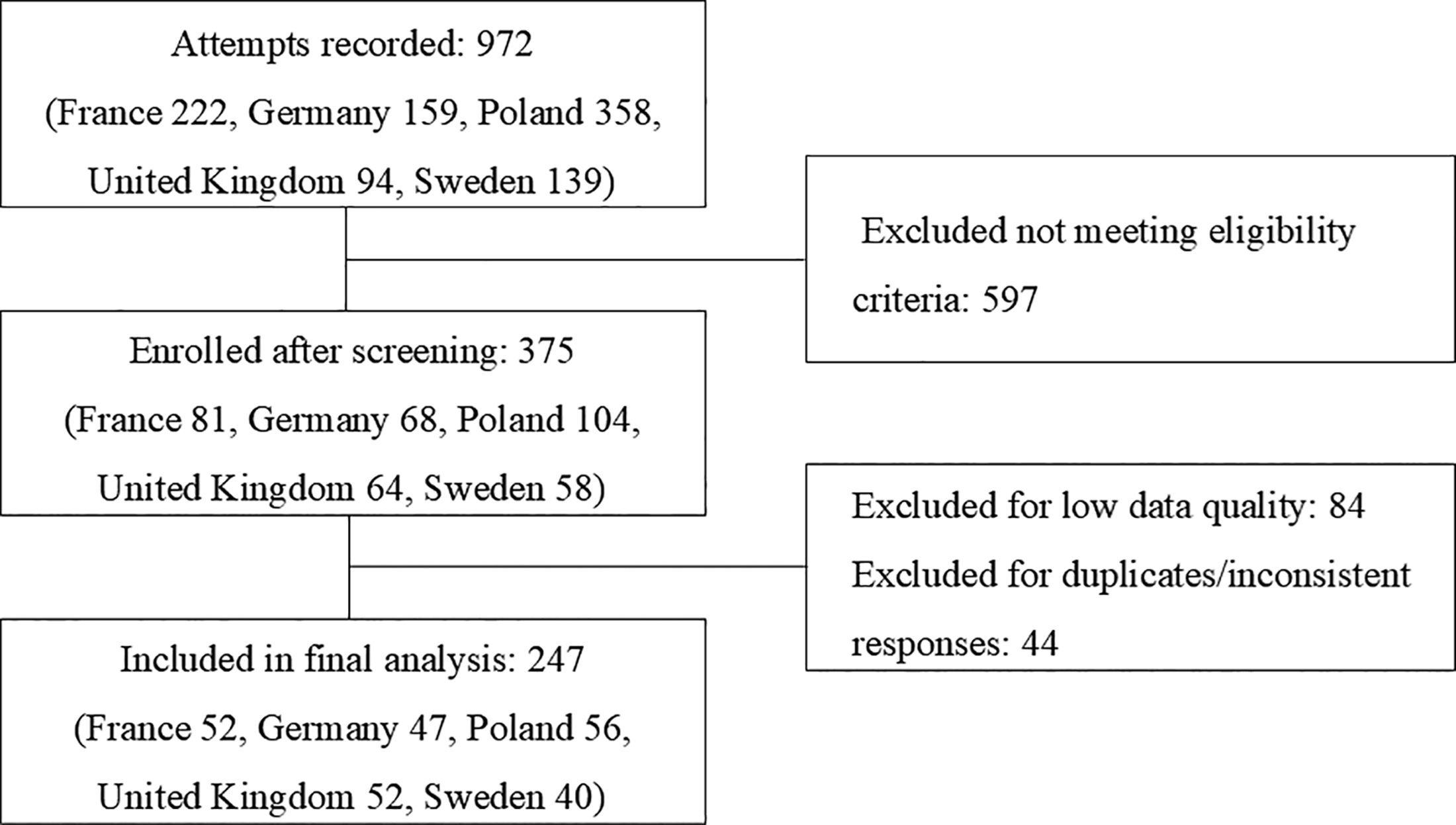
Flow of women through the survey: from attempts recorded to the final analytic sample.
The cohort was predominantly young: 215/247 (87.0%) were aged 19–34 years (Table 1). At enrollment, most were at 12–19 weeks’ gestation (102/247; 41.3%). Just over half were primigravid women (138/247; 55.9%). Further pregnancy characteristics are reported in Supplementary Table S1.
Characteristics of Survey Participants by Country
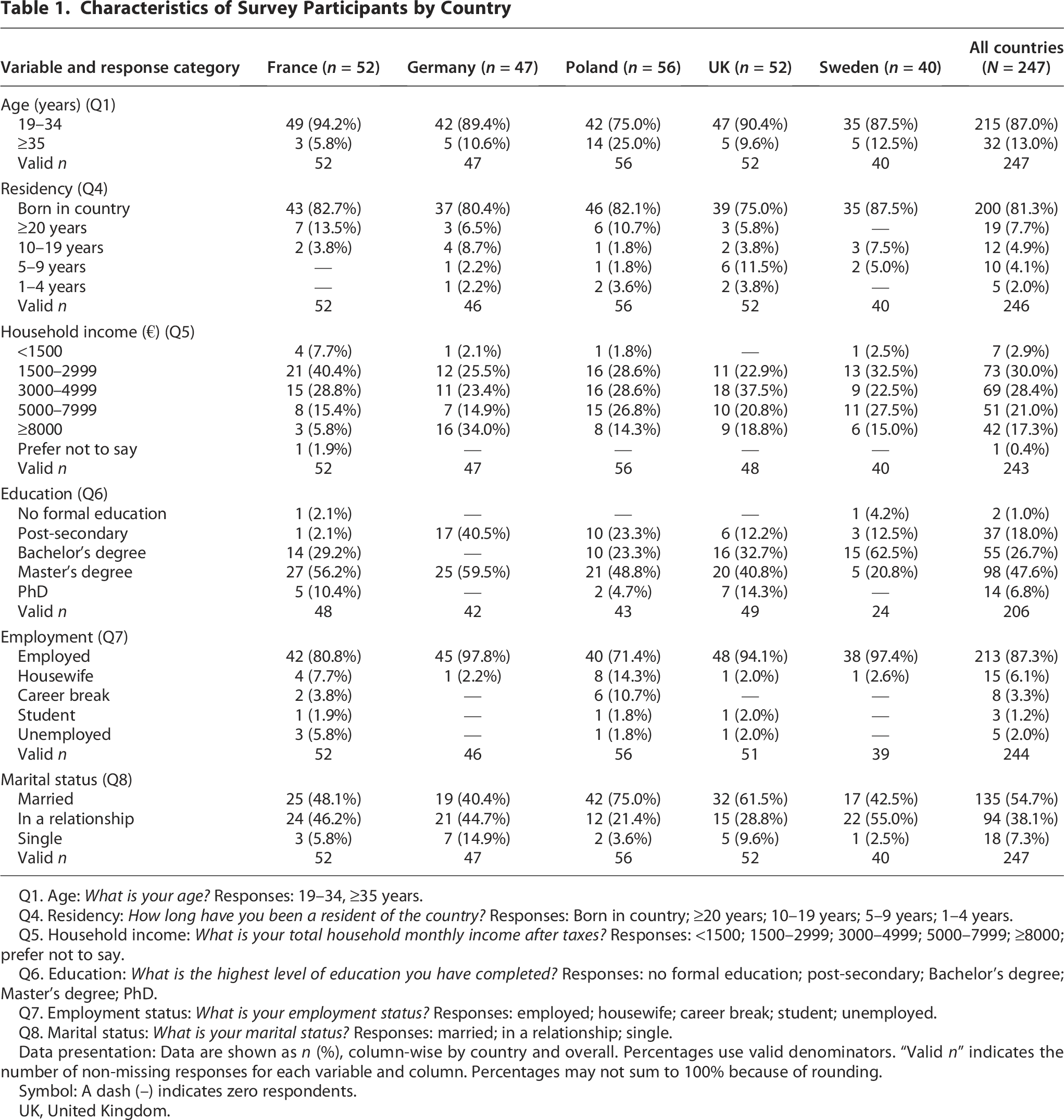
Q1. Age: What is your age? Responses: 19–34, ≥35 years.
Q4. Residency: How long have you been a resident of the country? Responses: Born in country; ≥20 years; 10–19 years; 5–9 years; 1–4 years.
Q5. Household income: What is your total household monthly income after taxes? Responses: <1500; 1500–2999; 3000–4999; 5000–7999; ≥8000; prefer not to say.
Q6. Education: What is the highest level of education you have completed? Responses: no formal education; post-secondary; Bachelor’s degree; Master’s degree; PhD.
Q7. Employment status: What is your employment status? Responses: employed; housewife; career break; student; unemployed.
Q8. Marital status: What is your marital status? Responses: married; in a relationship; single.
Data presentation: Data are shown as n (%), column-wise by country and overall. Percentages use valid denominators. “Valid n” indicates the number of non-missing responses for each variable and column. Percentages may not sum to 100% because of rounding.
Symbol: A dash (–) indicates zero respondents.
UK, United Kingdom.
Results are presented for the overall sample and stratified by country and by PTB risk status, with primary and secondary outcomes reported sequentially.
Primary outcome
Neonatal PTB risk awareness in the whole sample and by country
Overall, self-appraised neonatal PTB risk awareness clustered around mid-level responses, with variation across countries.
Specifically, the most common response for neonatal PTB risk awareness was somewhat aware (88/247, 35.6%), followed by moderately aware (71/247, 28.7%), very aware (71/247, 28.7%), and not at all aware (17/247, 6.9%). On the binary recode, 142/247 (57.5%) reported high awareness and 105/247 (42.5%) low awareness.
Awareness differed by country on both the four-level outcome (4 × 5 chi square test: p = 0.013; q = 0.013; Cramér’s V = 0.16) and the binary recode (2 × 5 chi square test: p < 0.001; q < 0.001; V = 0.30). Somewhat aware predominated in Poland (29/56, 51.8%) and Sweden (20/40, 50.0%), whereas moderately or very aware were the largest categories in France (both 17/52, 32.7%), Germany (both 16/47, 34.0%), and the United Kingdom (both 19/52, 36.5%; Table 2). Sparse cells were noted for the four-level outcome.
Neonatal PTB Risk Awareness and PTB Risk Status by Country
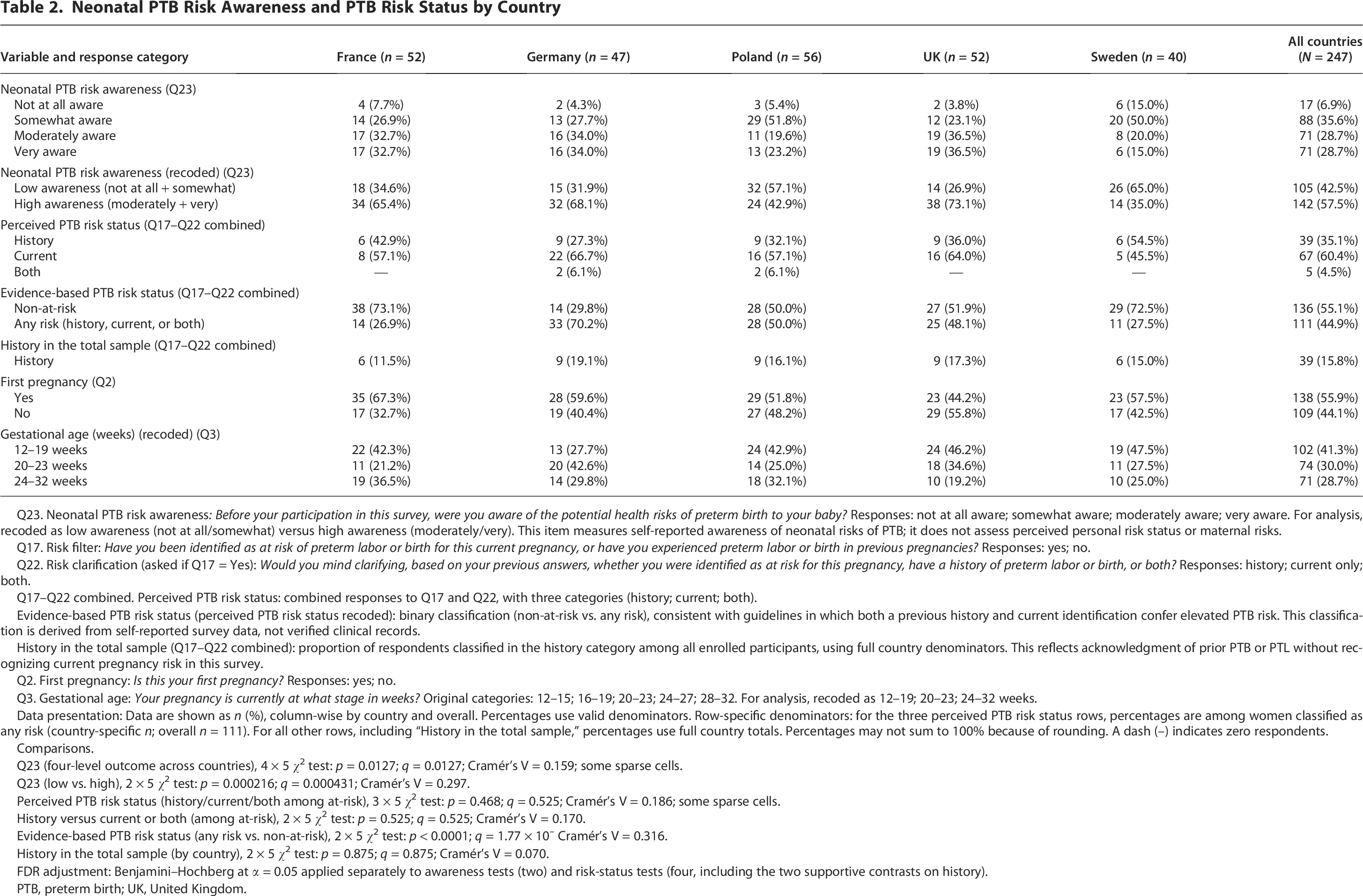
Q23. Neonatal PTB risk awareness: Before your participation in this survey, were you aware of the potential health risks of preterm birth to your baby? Responses: not at all aware; somewhat aware; moderately aware; very aware. For analysis, recoded as low awareness (not at all/somewhat) versus high awareness (moderately/very). This item measures self-reported awareness of neonatal risks of PTB; it does not assess perceived personal risk status or maternal risks.
Q17. Risk filter: Have you been identified as at risk of preterm labor or birth for this current pregnancy, or have you experienced preterm labor or birth in previous pregnancies? Responses: yes; no.
Q22. Risk clarification (asked if Q17 = Yes): Would you mind clarifying, based on your previous answers, whether you were identified as at risk for this pregnancy, have a history of preterm labor or birth, or both? Responses: history; current only; both.
Q17–Q22 combined. Perceived PTB risk status: combined responses to Q17 and Q22, with three categories (history; current; both).
Evidence-based PTB risk status (perceived PTB risk status recoded): binary classification (non-at-risk vs. any risk), consistent with guidelines in which both a previous history and current identification confer elevated PTB risk. This classification is derived from self-reported survey data, not verified clinical records.
History in the total sample (Q17–Q22 combined): proportion of respondents classified in the history category among all enrolled participants, using full country denominators. This reflects acknowledgment of prior PTB or PTL without recognizing current pregnancy risk in this survey.
Q2. First pregnancy: Is this your first pregnancy? Responses: yes; no.
Q3. Gestational age: Your pregnancy is currently at what stage in weeks? Original categories: 12–15; 16–19; 20–23; 24–27; 28–32. For analysis, recoded as 12–19; 20–23; 24–32 weeks.
Data presentation: Data are shown as n (%), column-wise by country and overall. Percentages use valid denominators. Row-specific denominators: for the three perceived PTB risk status rows, percentages are among women classified as any risk (country-specific n; overall n = 111). For all other rows, including “History in the total sample,” percentages use full country totals. Percentages may not sum to 100% because of rounding. A dash (–) indicates zero respondents.
Comparisons.
Q23 (four-level outcome across countries), 4 × 5 χ² test: p = 0.0127; q = 0.0127; Cramér’s V = 0.159; some sparse cells.
Q23 (low vs. high), 2 × 5 χ² test: p = 0.000216; q = 0.000431; Cramér’s V = 0.297.
Perceived PTB risk status (history/current/both among at-risk), 3 × 5 χ² test: p = 0.468; q = 0.525; Cramér’s V = 0.186; some sparse cells.
History versus current or both (among at-risk), 2 × 5 χ² test: p = 0.525; q = 0.525; Cramér’s V = 0.170.
Evidence-based PTB risk status (any risk vs. non-at-risk), 2 × 5 χ² test: p < 0.0001; q = 1.77 × 10⁻ Cramér’s V = 0.316.
History in the total sample (by country), 2 × 5 χ² test: p = 0.875; q = 0.875; Cramér’s V = 0.070.
FDR adjustment: Benjamini–Hochberg at α = 0.05 applied separately to awareness tests (two) and risk-status tests (four, including the two supportive contrasts on history).
PTB, preterm birth; UK, United Kingdom.
Secondary outcomes
Across the secondary outcomes, three main findings are summarized to guide interpretation. Neonatal PTB risk awareness did not differ by evidence-based PTB risk status. Recall of PTB-related discussions with HCPs and recognition-based knowledge remained limited across PTB risk strata. Within the any risk group, the history category identified respondents who reported a prior PTB/PTL without recognizing elevated risk in the current pregnancy. Each secondary outcome is detailed in the sections below.
Information sources on neonatal PTB risks (overall and by country)
Among women who reported at least one source (n = 220), HCPs were the most frequently cited: obstetrician–gynecologist/midwife/other HCP in 141/220 (64.1%) and the general practitioner in 101/220 (45.9%).
After FDR adjustment, several between-country differences persisted. For example, reporting National Health Service (NHS), public-health, or community-organization websites was highest in Sweden (11/34, 32.4%), and the United Kingdom showed the greatest participation in prenatal/childbirth classes (20/49, 40.8%) and the highest use of online research (21/49, 42.9%; Supplementary Table S2).
Recalled HCP-discussion themes (overall and by country)
In the overall sample, the most frequently recalled HCP-discussion themes were risk factors (78/195, 40.0%), preventive lifestyle/avoidance (65/195, 33.3%), and definition/timing (56/195, 28.7%); all other themes were each reported by <13%.
Recall richness (≥2 distinct themes) was 79/195 (40.5%). Among women with a scorable entry, the recall quality index was 0 in 86/184 (46.7%), 1 in 49/184 (26.6%), and 2 in 49/184 (26.6%). Overall, 52/247 (21.1%) provided no open-text response, almost all of whom had previously reported not discussing PTB with an HCP (Supplementary Table S2).
At the country level, no theme remained significant after FDR adjustment, and no between-country differences were observed in recall richness or recall quality (Supplementary Table S2).
Evidence-based and perceived PTB risk status
On the evidence-based PTB risk definition (Q17–Q22), 111/247 (44.9%; 95% CI, 38.9–51.2) were classified as any risk and 136/247 (55.1%; 95% CI, 48.8–61.1) as non-at-risk. Within the any risk subgroup, perceived PTB risk status was history 39/111 (35.1%; 95% CI, 26.9–44.4), current 67/111 (60.4%), and both 5/111 (4.5%) (Table 2). Country proportions for the history category within any risk were France 6/14 (42.9%), Germany 9/33 (27.3%), Poland 9/28 (32.1%), the United Kingdom 9/25 (36.0%), and Sweden 6/11 (54.5%).
There was no evidence of between-country differences in the history percentage within any risk. Considering the full distribution of perceived PTB risk status within the any risk group (history, current, and both), there was no evidence of between-country differences, with interpretation cautious owing to small counts in both. In the total sample, the history category represented 39/247 (15.8%; 95% CI, 11.8–20.9), with no evidence of between-country differences (Table 2).
Neonatal PTB risk awareness by evidence-based PTB risk status and perceived PTB risk status
By evidence-based PTB risk status, the four-level awareness distribution was similar in any risk and non-at-risk, and the binary recode (high vs. low) did not differ. By perceived PTB risk status, patterns were likewise comparable across history, current, and both; only history showed moderately aware as the most frequent category (43.6%). Formal comparisons are summarized in Supplementary Table S3: none remained significant after FDR adjustment.
Perceived PTB risk status and personal PTB risk factors
Among women classified as any risk, 37/111 (33.3%; 95% CI, 25.3–42.5) reported previous PTB/PTL on Q18 (personal PTB risk factors) (Table 3). By perceived PTB risk status, previous PTB/PTL was reported in history 13/39 (33.3%; 95% CI, 20.6–49.0), current 23/67 (34.3%; 95% CI, 24.1–46.3), and both 1/5 (20.0%; 95% CI, 3.6–62.4; Table 3).
Recognition of PTB Risk Factors and HCP-Recommended Management Strategies by Risk Status, with Summary Indices
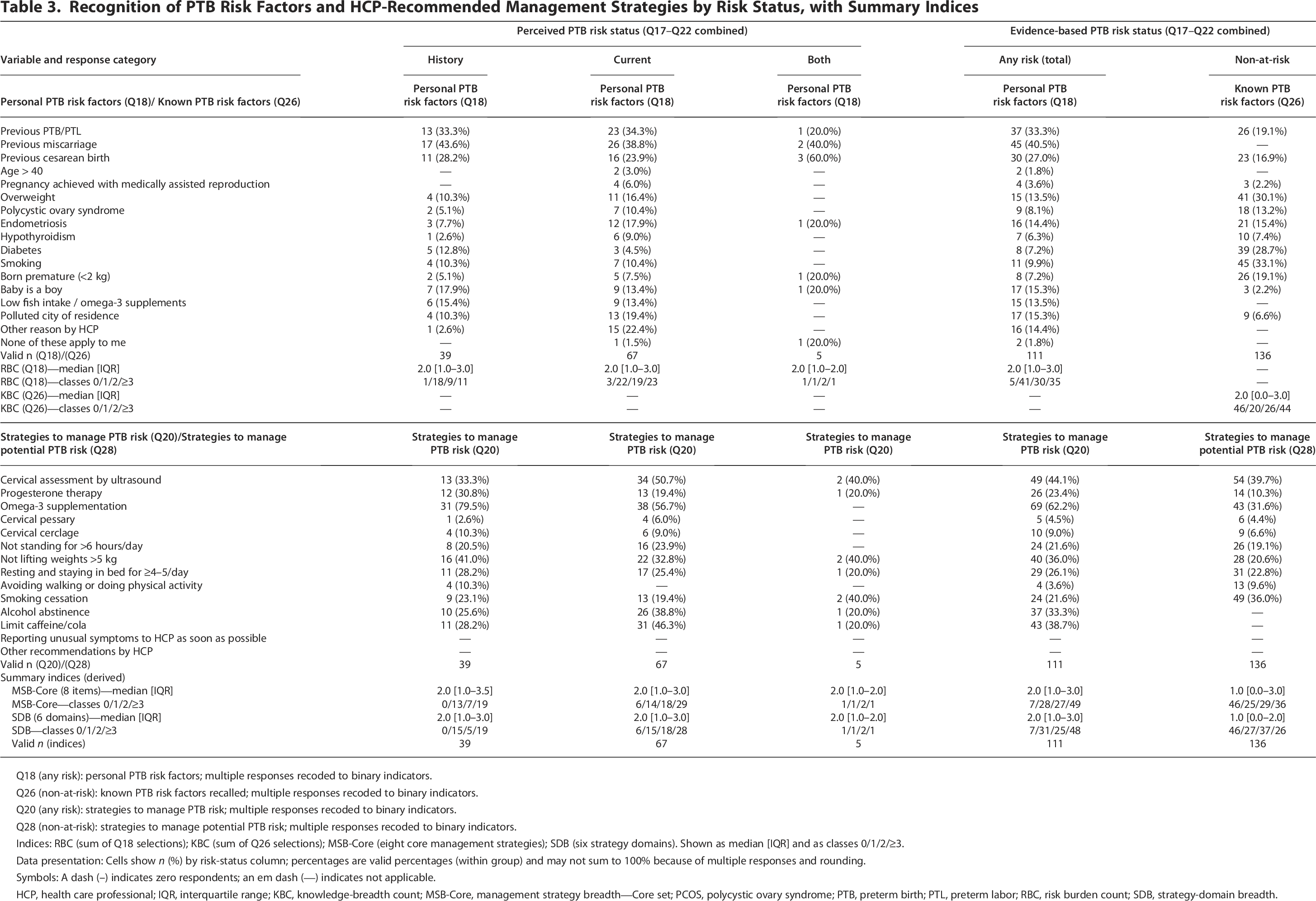
Q18 (any risk): personal PTB risk factors; multiple responses recoded to binary indicators.
Q26 (non-at-risk): known PTB risk factors recalled; multiple responses recoded to binary indicators.
Q20 (any risk): strategies to manage PTB risk; multiple responses recoded to binary indicators.
Q28 (non-at-risk): strategies to manage potential PTB risk; multiple responses recoded to binary indicators.
Indices: RBC (sum of Q18 selections); KBC (sum of Q26 selections); MSB-Core (eight core management strategies); SDB (six strategy domains). Shown as median [IQR] and as classes 0/1/2/≥3.
Data presentation: Cells show n (%) by risk-status column; percentages are valid percentages (within group) and may not sum to 100% because of multiple responses and rounding.
Symbols: A dash (–) indicates zero respondents; an em dash (—) indicates not applicable.
HCP, health care professional; IQR, interquartile range; KBC, knowledge-breadth count; MSB-Core, management strategy breadth—Core set; PCOS, polycystic ovary syndrome; PTB, preterm birth; PTL, preterm labor; RBC, risk burden count; SDB, strategy-domain breadth.
Other frequently selected factors were previous miscarriage (45/111, 40.5%) and previous cesarean birth (30/111, 27.0%), with smaller proportions selecting endometriosis (16/111, 14.4%), overweight (15/111, 13.5%), polycystic ovary syndrome (9/111, 8.1%), and hypothyroidism (7/111, 6.3%). The RBC (sum of Q18 selections) had a median of 2.0 [IQR, 1.0–3.0]; 35/111 (31.5%) had RBC ≥ 3 (Table 3; Supplementary Table S4).
Information sources on neonatal PTB risks by evidence-based PTB risk status and perceived PTB risk status
Among women classified as any risk, the most frequently reported sources were obstetrician–gynecologist/midwife/other HCP (68/98, 69.4%) and the general practitioner (53/98, 54.1%), compared with 73/122 (59.8%) and 48/122 (39.3%), respectively, among non-at-risk women (Supplementary Table S2). Those with neither HCP nor institutional sources were 19/111 (17.1%) in any risk and 32/136 (23.5%) in non-at-risk. By perceived PTB risk status, obstetrician–gynecologist/midwife/other HCP were cited by 26/35 (74.3%) in history, 40/59 (67.8%) in current, and 2/4 (50.0%) in both (Table 4).
Sources of Information on Neonatal PTB Risks and Themes Recalled from HCP Discussions by PTB Risk Status
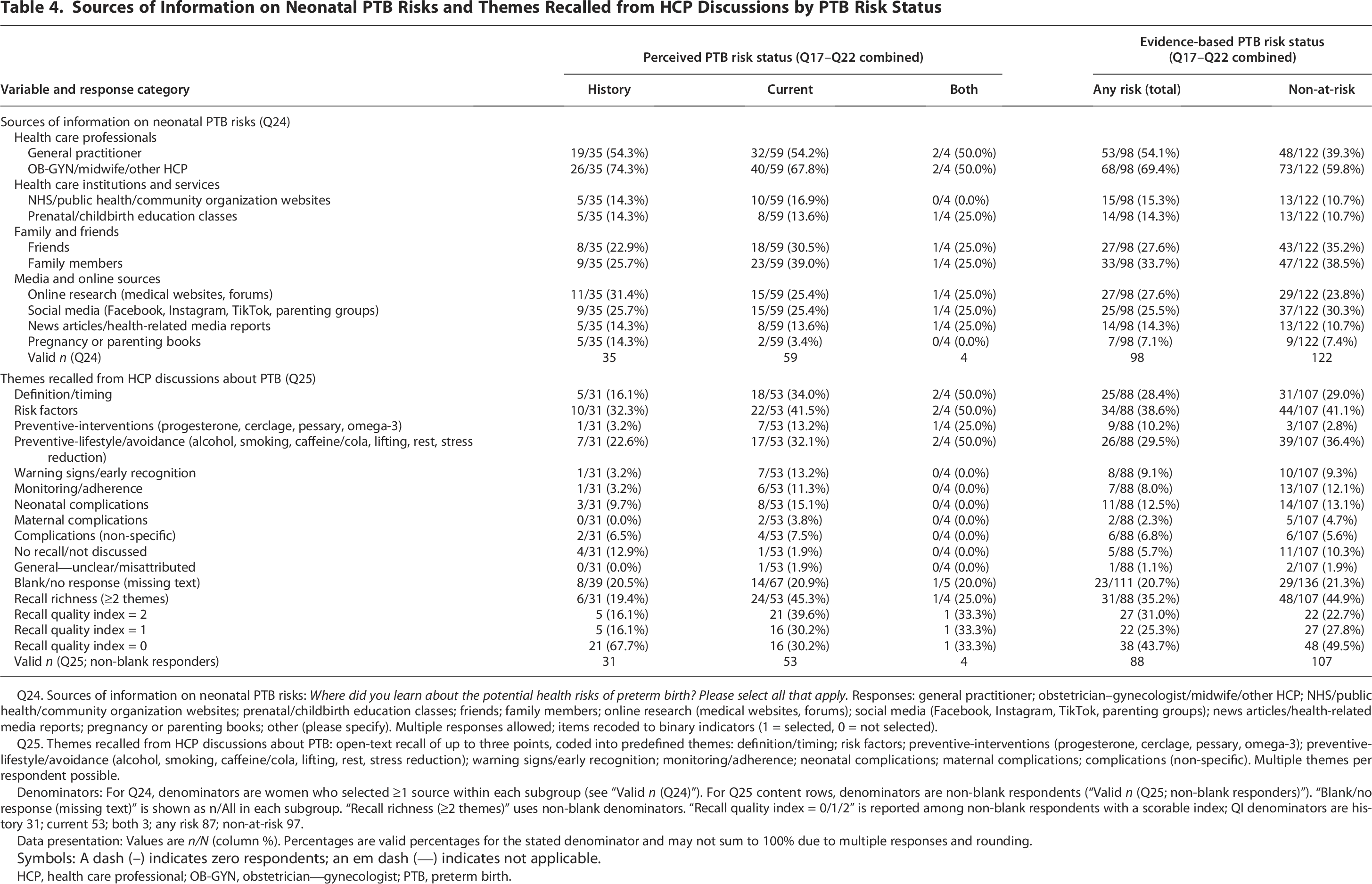
Q24. Sources of information on neonatal PTB risks: Where did you learn about the potential health risks of preterm birth? Please select all that apply. Responses: general practitioner; obstetrician–gynecologist/midwife/other HCP; NHS/public health/community organization websites; prenatal/childbirth education classes; friends; family members; online research (medical websites, forums); social media (Facebook, Instagram, TikTok, parenting groups); news articles/health-related media reports; pregnancy or parenting books; other (please specify). Multiple responses allowed; items recoded to binary indicators (1 = selected, 0 = not selected).
Q25. Themes recalled from HCP discussions about PTB: open-text recall of up to three points, coded into predefined themes: definition/timing; risk factors; preventive-interventions (progesterone, cerclage, pessary, omega-3); preventive-lifestyle/avoidance (alcohol, smoking, caffeine/cola, lifting, rest, stress reduction); warning signs/early recognition; monitoring/adherence; neonatal complications; maternal complications; complications (non-specific). Multiple themes per respondent possible.
Denominators: For Q24, denominators are women who selected ≥1 source within each subgroup (see “Valid n (Q24)”). For Q25 content rows, denominators are non-blank respondents (“Valid n (Q25; non-blank responders)”). “Blank/no response (missing text)” is shown as n/All in each subgroup. “Recall richness (≥2 themes)” uses non-blank denominators. “Recall quality index = 0/1/2” is reported among non-blank respondents with a scorable index; QI denominators are history 31; current 53; both 3; any risk 87; non-at-risk 97.
Data presentation: Values are n/N (column %). Percentages are valid percentages for the stated denominator and may not sum to 100% due to multiple responses and rounding.
Symbols: A dash (–) indicates zero respondents; an em dash (—) indicates not applicable.
HCP, health care professional; OB-GYN, obstetrician—gynecologist; PTB, preterm birth.
The general practitioner was cited more often in any risk than in non-at-risk (54.1% vs. 39.3%; chi square (1) = 4.75, p = 0.029, q = 0.292, Cramér’s V = 0.15), whereas all other information sources showed no significant subgroup differences after FDR adjustment (Supplementary Table S4).
Recalled HCP-discussion themes by evidence-based PTB risk status and perceived PTB risk status
By evidence-based PTB risk, profiles of recalled HCP-discussion themes were broadly similar between any risk and non-at-risk across themes (Table 4). Risk factors were the most frequently recalled theme in both groups (any risk 34/88, 38.6%; non-at-risk 44/107, 41.1%). The only notable numerical difference was preventive interventions (10.2% vs. 2.8%), but it did not survive FDR adjustment. Recall richness (≥2 themes) and the highest tier of the recall quality index likewise did not differ (Supplementary Table S4).
Across perceived PTB risk strata, current showed a higher proportion at the highest tier of the recall quality index than history (39.6% vs. 16.1%), but between-group contrasts were not robust after FDR adjustment, and the both subgroup was too small for inference (Table 4; Supplementary Table S4).
Strategies to manage PTB risk in any risk women
Among women classified as any risk (evidence-based PTB risk status), the most frequently HCP-recommended strategies to manage PTB risk were omega-3 supplementation (69/111, 62.2%), cervical assessment by ultrasound (49/111, 44.1%), and avoiding lifting >5 kg (40/111, 36.0%); progesterone therapy was reported by 26/111 (23.4%). By perceived PTB risk status, history and current showed broadly similar profiles (history vs. current: omega-3 supplementation 31/39, 79.5% vs. 38/67, 56.7%; cervical assessment by ultrasound 13/39, 33.3% vs. 34/67, 50.7%; avoiding lifting >5 kg 16/39, 41.0% vs. 22/67, 32.8%; progesterone therapy 12/39, 30.8% vs. 13/67, 19.4%). The both subgroup (n = 5) was too small for inference (Table 3).
Strategies to manage potential PTB risk in non-at-risk women
Among non-at-risk women, commonly reported strategies to manage potential PTB risk were no alcohol (57/136, 41.9%), cervical monitoring by ultrasound (54/136, 39.7%), smoking cessation (49/136, 36.0%), and omega-3 supplementation/dietary advice (43/136, 31.6%).
Known PTB risk factors in non-at-risk women
In non-at-risk women, the most frequently recalled risk factors were smoking (45/136, 33.1%), overweight (41/136, 30.1%), diabetes (39/136, 28.7%), previous PTB (26/136, 19.1%), and previous cesarean birth (23/136, 16.9%). The KBC had a median of 2.0 [IQR, 0.0–3.0] (Table 3).
Discussion
Main findings in context
Self-appraised awareness of neonatal PTB risks was centered on the mid-low level (about one-third “somewhat aware”), with more than half “moderately/very aware,” and no significant difference between any risk and non-at-risk women. At the country level, higher awareness did not translate into richer or higher-quality recall. Within risk strata, higher self-ratings in history likewise did not translate into stronger recall, whereas current showed greater recall richness and a higher top-tier recall quality index, a difference that did not remain significant after FDR adjustment.
At the whole-sample level, recalled HCP-discussion themes were few and unevenly distributed across domains, with notable gaps for neonatal and maternal complications, warning signs and early recognition, monitoring and adherence to HCP recommendations, and intervention-specific content (e.g., progesterone and cerclage). Fewer than half recalled risk factors, about a third recalled preventive lifestyle, and fewer than one in three recalled definition/timing.
A notable finding was the sizable proportion of women classified as at elevated risk (any risk) who identified themselves in the history category (35.1% of any risk; 15.8% of the total sample). This reflects acknowledgment of a prior PTB but not recognition of current pregnancy risk, despite evidence that a prior PTB confers an approximately twofold to threefold higher risk of recurrence.33–35
Among non-at-risk women, breadth of knowledge about PTB risk factors was modest overall (KBC median 2), with responses clustered at the extremes (0 or ≥ 3 factors more common than 1 to 2).
Overall, recall of management strategies was limited, with few differences between any risk and non-at-risk groups. Omega-3 supplementation and progesterone therapy were reported more often by any risk women, smoking cessation more often by non-at-risk women; cervical ultrasound was commonly mentioned in both, and behavioral strategies were reported by a minority in both.
Strengths and limitations
First, to our knowledge, it is among the few European studies to measure and characterize awareness, knowledge, and recall related to PTB across key domains (risk factors to risk management). Second, the five-country design enhances generalizability and enables cross-country comparisons. Third, by combining women’s self-appraisal with open-text recall of HCP discussions, the study centers the patient perspective and provides granular insight into what information is retained.
The study relied on self-report for all measures, which is susceptible to recall bias. Furthermore, because questionnaire development and testing focused on expert review and technical performance rather than participant-based pretesting, and because country-specific online panels may differ in composition and engagement, residual cross-country differences in response behavior cannot be fully excluded when interpreting cross-country comparisons. Risk factors and exposure to counseling were not verified against clinical records, so misclassification may have occurred. Two cross-item inconsistencies also emerged: in the history group, only a subset indicated a previous PTB/PTL on the risk-factor checklist, whereas in the current group (excluding both), some reported a previous PTB/PTL. Nonetheless, these patterns are consistent with recognized response-process phenomena in survey research (satisficing, primacy effects, present-state anchoring, a frame shift from event listing to status labeling, and response editing to avoid perceived double counting).
The sample was younger than European maternal age distributions; selection bias cannot be excluded and may reflect the panel-based, invitation-only online recruitment and eligibility criteria.
Participants were also characterized by high educational attainment, a profile consistent with greater health literacy, digital access, and survey engagement than in the general pregnant population. Because inclusion required successful completion of a web-based survey, the analytic sample may overrepresent women with higher survey persistence and engagement, supporting internal validity while potentially limiting generalizability. Such a selection would plausibly bias estimates toward greater awareness rather than lower awareness. In this context, the observed discrepancies between self-appraised neonatal PTB risk awareness, perceived PTB risk status, and recall- or recognition-based knowledge are unlikely to be overstated and may, if anything, be more pronounced in less selected populations.
Finally, some subgroups were small, notably the both category, yielding sparse cells and limited power; FDR adjustment further attenuated apparent signals.
Comparison with other studies
Previous studies, although conducted in settings and periods that differ from ours, have reported similar domain-specific gaps in PTB knowledge, particularly in definitions and timing and in intervention-specific knowledge, overlapping with those observed here.36,37
Our observed distribution of perceived PTB risk status within any risk, including the proportion in the history category, is consistent with reports that risk perception is shaped by HCP-mediated explanations and experiential anchoring. 38 This helps explain why women who perceived current risk exhibited richer, higher-quality recall than those in history.
Interpretation
Collectively, the data suggest a disconnect between feeling informed (self-appraised awareness) and retaining knowledge that can support health-related behavior (operational recall). Two mechanisms are plausible: first, experiential anchoring and the salience of the present pregnancy: women who perceive current risk are more likely to receive and encode messages with immediate relevance, whereas those who view their risk as historical may not appraise current vulnerability and therefore under-encode counseling. Second, suboptimal communication renders counseling generic, promoting gist rather than actionable retention and rapid forgetting, consistent with the low recall of interventions and warning signs.
Implication for practice
Health services and HCPs should pilot a brief, evidence-informed approach in routine prenatal care that personalizes communication to culture, language, and health literacy; explicitly labels risk status; uses outcome-oriented framing that links risk to action and neonatal benefit; provides concise action plans with warning-sign triggers and defined follow-up routes; delivers three to five take-home points with verification of understanding; and repeats key messages at standard prenatal contacts.19–21,36–41
Implementation strategies supported by the literature include embedding a standardized communication protocol in the maternity record, whether patient-held or electronic, enabling clinicians to document individualized PTB counseling and plan, the discussion and recommendation of evidence-based preventive strategies when indicated, 40 verification of understanding (e.g., through teach-back),41–44 and the recording of action plans and contact pathways. A brief patient-facing summary, optionally accessible via a QR code, should mirror these elements in plain language and be reinforced at standard prenatal contacts, including booking and major scan visits, aligned with local schedules and WHO ANC guidance. 20 Where a standardized pregnancy booklet is not available, equivalent fields can be incorporated into electronic maternity records to ensure traceable documentation of what was communicated, when, and by whom.45–47
Conclusion
In our study, self-appraised awareness of PTB was mid-low, while operational recall of PTB themes was limited; recognition-based knowledge breadth was similar between high- and low-risk groups across definition and timing, risk factors, and management strategies.
Adopting a record-integrated communication protocol that documents individualized counseling, provides a brief patient-facing summary with teach-back, and reinforces key messages at standard prenatal contacts, with electronic deployment where pregnancy booklets are not available, can standardize delivery and enable measurement across sites.41–47
Future studies should use harmonized, validated measures and triangulate maternal and family self-reports with objective data.
Authors’ Contributions
Conceptualization and supervision: G.C.D.R.; methodology: G.C.D.R. and D.O.C.A.; Formal analysis: S.M. and E.B.; Writing—original draft: E.B.; Writing—review and editing: all authors. All authors approved the final version of the article and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgments
The authors thank the women who participated in the survey and Listen Lab for their professional work.
Ethical Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and applicable national regulations. Before accessing the questionnaire, participants read an information statement and provided electronic informed consent by proceeding. Responses were anonymous at entry and contained no personal identifiers; participation was voluntary and uncompensated, and data were analyzed only in aggregate. Owing to the anonymous, minimal-risk design, Institutional Review Board or ethics committee review was not required under applicable regulations. Data handling complied with the General Data Protection Regulation (GDPR; Regulation [EU] 2016/679).
Data Availability Statement
De-identified data and the codebook are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
No funding was received for this work.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.