
Abstract
Background:
Depression is highly prevalent among women, posing a significant public health concern. While the beneficial effects of physical activity on depression reduction have been acknowledged, the influence of socioeconomic status (SES) on this relationship remains unclear.
Methods:
This study utilized cross-sectional data from 14,691 women from the 2007–2020 U.S. National Health and Nutrition Examination Surveys, who were categorized into three SES groups using latent class analysis. Logistic regression analysis was employed to examine the relationship between physical activity and depression.
Results:
The analysis revealed that 11.5% of the participants experienced depression, with only 53.4% engaging in sufficient physical activity. Upon data weighting, the depression prevalence among physically inactive individuals was 12.64% (95% confidence interval [95% CI]: 11.58–13.70). Univariate logistic regression showed a negative correlation between adequate physical activity and depression in women (odds ratio [OR] = 0.64, 95% CI: 0.56–0.73, p < 0.001). Adjusting for SES or other confounders, sufficient physical activity remained associated with lower prevalence of depression (OR = 0.82, 95% CI: 0.69–0.97, p = 0.016). Stratification by SES indicated that adequate physical activity was associated with depression only among women with high SES (OR = 0.65, 95% CI: 0.50–0.86, p = 0.002) but not in middle or low SES.
Conclusions:
This study identified a negative association between physical activity and depression in women. Notably, only high SES women may derive benefits from physical activity, emphasizing the importance of addressing SES disparities to mitigate potential health inequalities.
Keywords
Introduction
According to the World Health Organization, depression is an important mental health problem, affecting 3.8% of the population in 2019. Among female adults, the prevalence rate was 6%. 1 In the United States, 2020 data showed that nearly one-fifth of adults had been diagnosed with depression. 2 Depression adversely impacts quality of life, increases medical expenses, and, in severe cases, can lead to mortality.3–5 Studies have shown that women are twice as likely as men to experience depression. 6 In the United States, the prevalence of depression among adult women increased from 9.3% in 2015–2016 to 11.8% in 2020, compared with 5.4% and 6.4% among men, respectively.7,8 Addressing mental health issues among women is paramount.
Physical activity has been extensively studied and proven to be crucial for mental health. 9 It stimulates the release of neurotransmitters such as endorphins and dopamine in the brain, positively impacting both physical and mental well-being, including emotional stability. 10 As a modifiable lifestyle factor, physical activity offers significant intervention potential. A review indicated that even minimal physical activity can help alleviate depression among young females. 11 In the United States, studies have shown that among adults, only 28.3% of males and 20.4% of females meet the recommended physical activity guidelines. 12
However, research on how physical activity affects depression across different socioeconomic statuses (SES), especially among women, is limited. In the United States, those with the lowest levels of income and education experienced the highest rates of adverse health conditions. 13 Those with lower SES often work long hours under high pressure, leaving little time for leisure physical activities. 14 Alternatively, they may perceive physical activity as less essential due to lower cognitive and self-efficacy. 15 Yet, some argue that lower SES individuals engage in more physical activity due to fewer sedentary behaviors and lower psychological stress.16,17
Physical activity, as a modifiable health behavior, presents a feasible and cost-effective alternative to pharmacological treatments. 18 While numerous studies have well documented the positive impact of physical activity on mental well-being, most have focused on general populations. 19 Although some studies mentioned the influence of SES on health outcomes, studies examining how SES influences physical activity and depression remain limited.20,21 Moreover, the consistency of these findings among women is still unclear.
This study utilizes nationally representative data to investigate how physical activity affects depression in American women across different SES levels. Understanding SES differences can guide future mental health interventions, highlighting the need for culturally sensitive, strategies tailored to individuals with diverse SES backgrounds.
Methods
Study population
The National Health and Nutrition Examination Surveys (NHANES) is a nationally representative cross-sectional survey of the noninstitutionalized civilian population in the United States. 22 Participants signed written informed consent, and NHANES anonymized the results before reporting. Detailed information on survey methods, response rates, and weighting procedures is available on the website. 23 Due to the age restriction on marital status disclosure in NHANES, our analysis focuses on participants aged 20 and above. Initially, 66,148 people were invited to participate from 2007 to March 2020. After excluded those with missing physical activity and incomplete depression data, 14,691 female participants were included in the study. The analysis was conducted in March 2024 (Fig. 1).
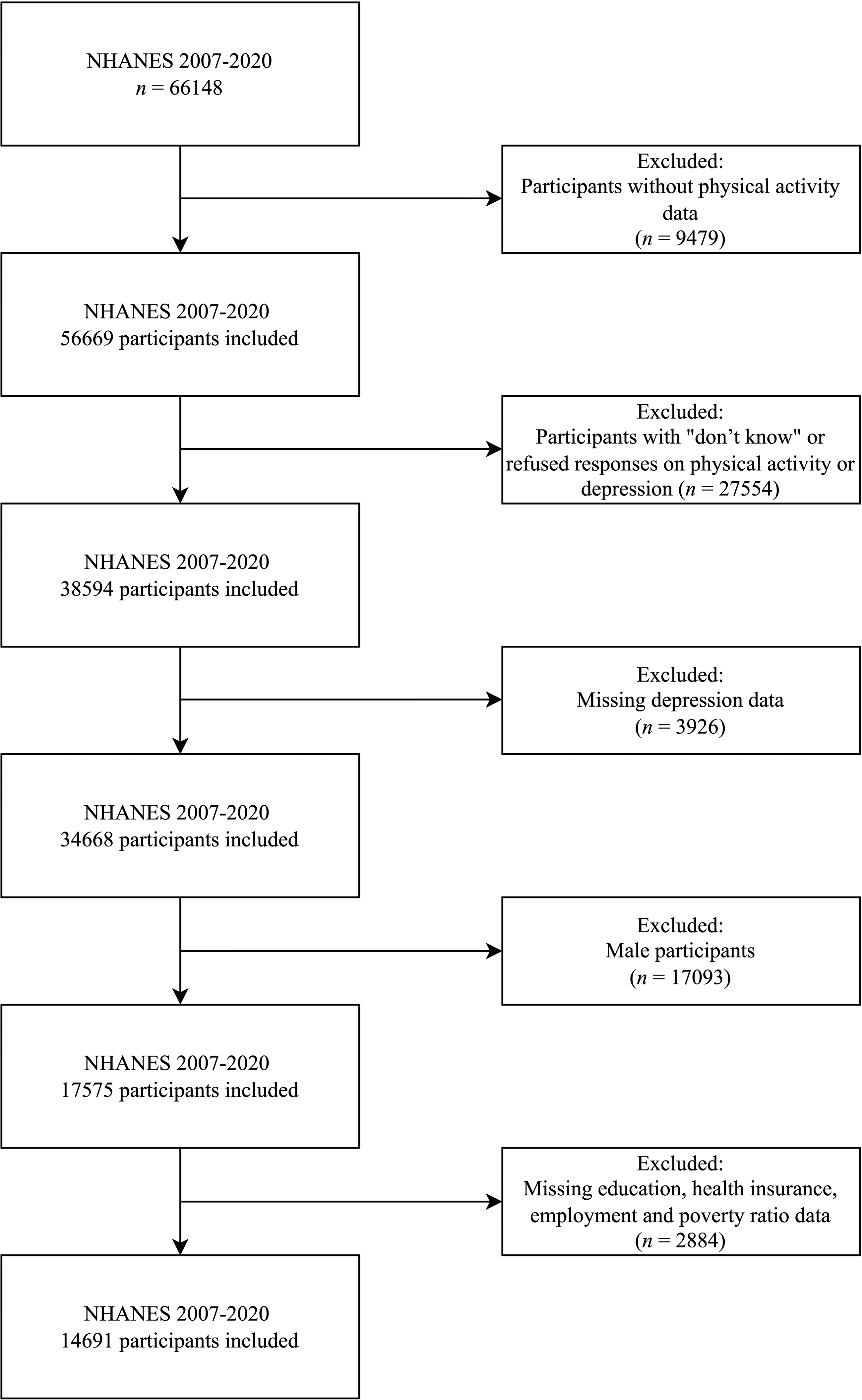
Flow chart of participants’ selection process from the National Health and Nutrition Examination Survey during 2007–2020.
Depression status
To assess depression, NHANES uses the Patient Health Questionnaire-9, comprising 9 self-evaluation questions with a total score ranging from 0 to 27. Among them, scores between 0 and 4 are considered normal, 5 and 9 indicate mild depression, 10 and 14 points signify moderate depression, 15 and 19 signify moderately severe depression, and 20 and 27 represent severe depression. 24 Participants with scores above 10 were classified as depressed, while those with scores below 10 were deemed not depressed. 24
Physical activity
Participants’ physical activity in the past week was calculated in metabolic equivalents (METs) following NHANES guidelines. Utilizing the Global Physical Activity Questionnaire, participants reported the frequency and duration of various activities including vigorous, moderate, walking/cycling, vigorous recreational activity, moderate recreational activity, and sedentary time. 25 Total physical activity MET-minutes/week was computed by multiplying the total minutes of various activities by the corresponding METs. Participants were categorized into “lack of physical activity” and “adequate physical activity” based on whether they achieved 600 METs. Total physical activity MET-minutes/week was included descriptively but excluded from regression due to collinearity with physical activity levels. Sedentary time was categorized as <420 and ≥420 minutes, considering research suggesting that sedentary time exceeding 7 hours daily increases mortality risk. 26
Socioeconomic status
Participants were classified into high, middle, and low SES categories based on education level, health insurance, employment status (unemployed and employed), and the ratio of family income to poverty. Private health insurance includes private insurance, Medi-Gap, and single service plans, and government health insurance includes Medicare, Medicaid, Children’s Health Insurance Program, military health care, state-sponsored health plans, and other government programs, while individuals without coverage are classified as not covered by health insurance. Employed participants were those currently working or involved in a job recently, while unemployed individuals were those seeking employment or not currently working.
Demographics and covariate
Trained interviewers collected sociodemographic data, including age in years at screening, marital status (married/living with partner, widowed/divorced/separated, and never married), race (non-Hispanic White, Mexican American, other Hispanic, non-Hispanic Black, other race—including multiracial), education level (high school graduate/general equivalency degree or equivalent, <9th grade, 9–11th grade, some college or AA degree, college graduate, or above), and ratio of family income to poverty. Participants aged over 80 were recorded as 80, and age was categorized into 20–40, 40–60, and ≥ 60 years. Ratio of family income to poverty calculated by dividing household income by the latest poverty line was categorized as < 1.3 and ≥ 1.3, with < 1.3 indicating eligibility for the Supplemental Nutrition Assistance Program for low-income families. 27 Body mass index (BMI) information was obtained from examination data and further categorized as underweight (<18.5), normal weight (18.5–24.9), overweight (25.0–29.9), or obese (BMI ≥ 30). Antidepressant medication use was classified using the NHANES Multum Lexicon Therapeutic Classification Scheme. Seven relevant classes of antidepressants were identified: miscellaneous antidepressants, selective serotonin reuptake inhibitors, tricyclic antidepressants, monoamine oxidase inhibitors, phenylpiperazine antidepressants, tetracyclic antidepressants, and selective serotonin and norepinephrine reuptake inhibitors. This variable was categorized into two groups, no antidepressant use and antidepressant use. These covariates were selected based on existing literature and adjusted for in the analysis.
Statistical analysis
Following NHANES guidelines, all analyses used weighted samples and were performed using the survey package in R software, version 4.2.3 (R Project Version 4.1.0; Foundation for Statistical Computing, Vienna, Austria). 28 The stratification and clustering of the NHANES design were also considered. Two-sided p < 0.05 was considered statistically significant. Baseline profiles of depression and physical activity were examined using percentages for categorical variables via the Chi-square test and the median with interquartile range for continuous variables due to nonnormal distribution via the Wilcoxon rank-sum test. Logistic regression models were employed to assess independent associations between depression and physical activity across three models: Model 1 (unadjusted), Model 2 (adjusted for SES variables), and Model 3 (adjusted for SES variables, age, race, marital status, BMI, antidepressant medication use, and sedentary minutes). Furthermore, we applied latent class analysis (LCA) to classify participants into three distinct SES groups (low, middle, and high) based on education level, health insurance, employment status, and the family income to poverty ratio. LCA serves as a robust classification method by selecting the best-fitting model based on the lowest Akaike information criterion and Bayesian information criterion values to determine the optimal number of latent classes.29–31 Subsequently, we performed logistic regression analyses (Model 4–6) separately within each SES group to examine the association between physical activity and depression, adjusting for potential confounders, excluding SES-related variables used in the LCA classification.
Results
Basic characteristics of participants
The study included a total of 14,691 female participants, representing 110 million people, with an average age of 49.7 ± 17.6 years. Among them, 1689 (11.5%) had depression. Female participants with depression were more likely to be aged 40–60 (41.0%), married (48.6%), non-Hispanic White (42.1%), covered by government health insurance (42.8%), and obese (55.5%), with a college or AA degree (32.8%), unemployed (64.8%), and below 130% of the federal poverty level (53.1%) and had a lack of physical activity (54.4%). However, in the depressed population, 63.4% reported sedentary time <420 minutes per day, and 63.2% were not using antidepressant medication. All variables showed differences between depression and nondepression at p < 0.05 (Table 1). Participants were also divided into two groups based on whether their MET was >600. Compared with those with a lack of physical activity, participants in the adequate physical activity group were more likely to have higher education levels, be employed, and have a ratio of family income to poverty ≥1.3 (all p < 0.05; Supplementary Table S1). Among the 51,207 participants excluded due to missing information, the majority were non-Hispanic White (33.6%), and approximately 33.7% of them were aged 20–40 (Supplementary Tables S2 and S3).
Characteristics of Female Participants by Depression Status NHANES 2007–2020
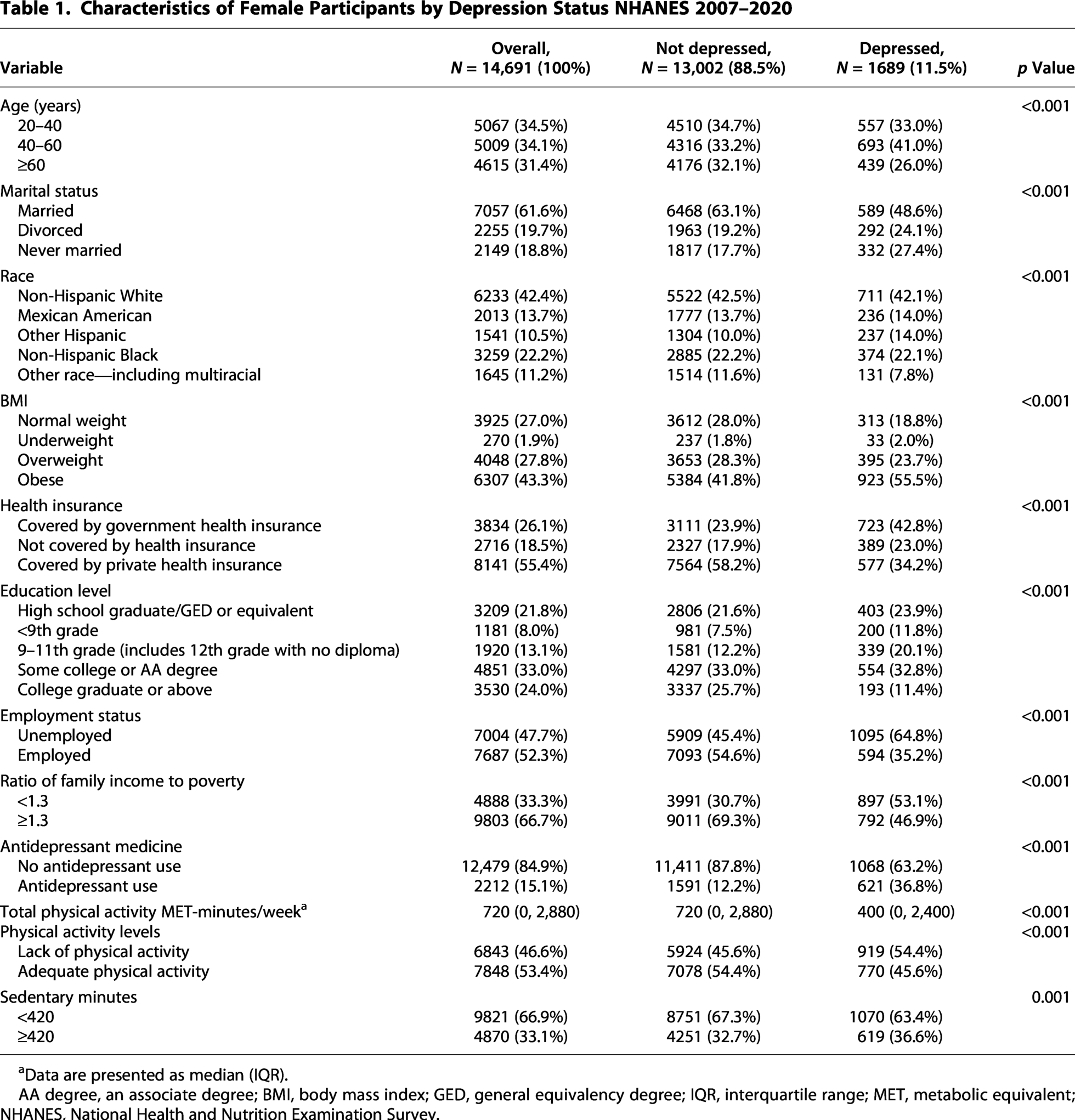
Data are presented as median (IQR).
AA degree, an associate degree; BMI, body mass index; GED, general equivalency degree; IQR, interquartile range; MET, metabolic equivalent; NHANES, National Health and Nutrition Examination Survey.
Prevalence of depression
After weighing, the prevalence of depression in the United States was higher among those 40–60 years old (11.67%), never married (15.02%), other Hispanic (14.51%), underweight (13.77%), and obese (13.41%), covered by government insurance (18.69%), with low education level including 9–11th grade (18.01%) and <9th grade (15.97%), unemployed (14.16%), a ratio of family income to poverty < 1.3 (18.72%), use of antidepressant medicine (23.11%), a lack of physical activity (12.64%), and sedentary minutes ≥420 (11.72%; Table 2).
Prevalence of Depression Among All Participants After Survey Weighting

95% CI, 95% confidence interval.
Univariate and multivariate regression analysis of physical activity and depression
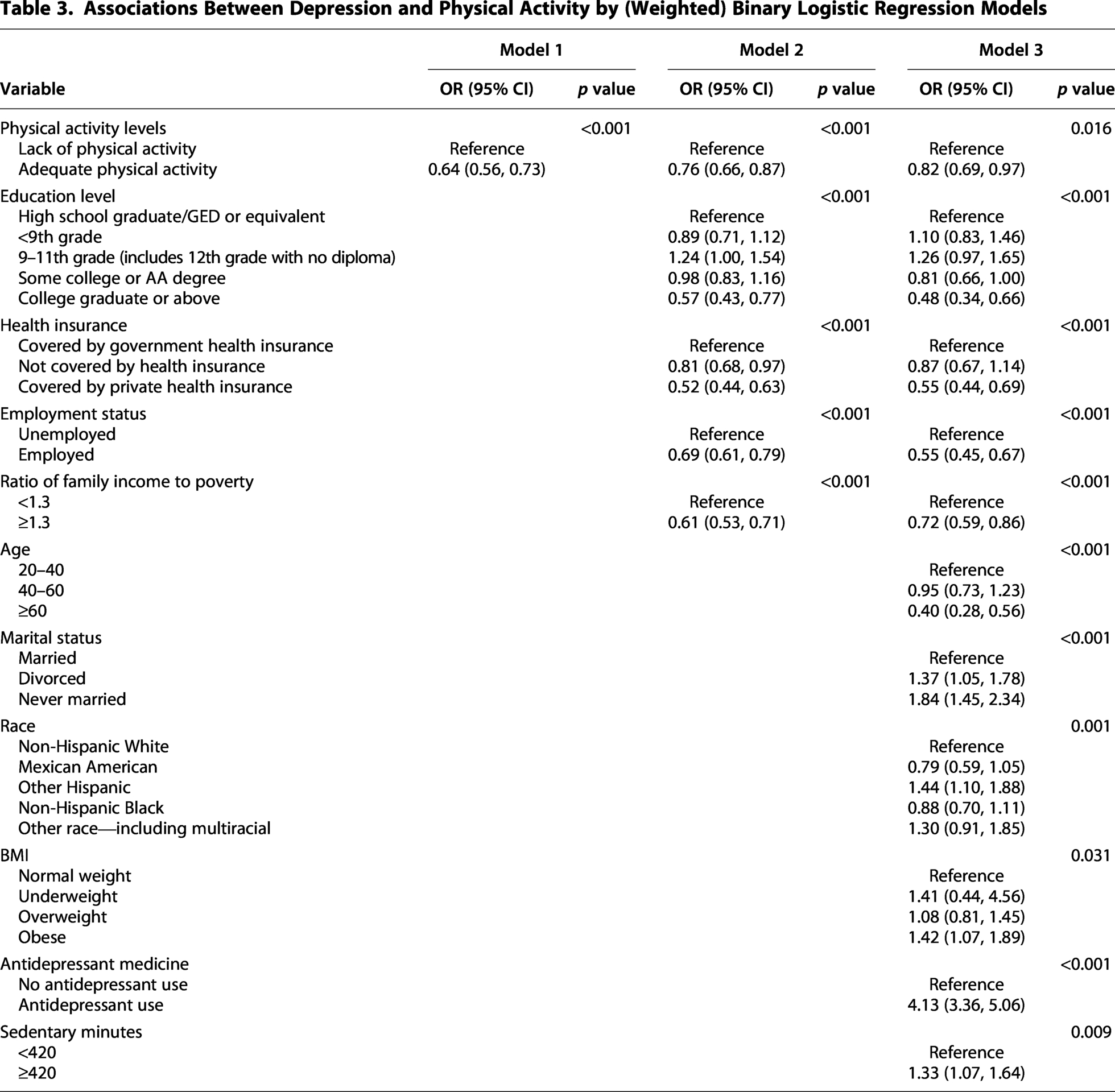
To examine the association between physical activity and depression, binary logistic regression analysis was used. In univariate logistic regression (Model 1), physical activity was associated with a lower likelihood of depression among women (odds ratio [OR] = 0.64, 95% confidence interval [95% CI]: 0.56–0.73, p < 0.001; Table 3). After adjusting for SES (Model 2), the association remained significant (OR = 0.76, 95% CI: 0.66–0.87, p < 0.001). Further adjustment for age, marital status, race/ethnicity, BMI, health insurance status, education level, employment status, ratio of family income to poverty, physical activity level, sedentary minutes, and antidepressant medication use (Model 3) did not substantially alter the relationship (OR = 0.82, 95% CI: 0.69–0.97, p = 0.016).
Associations Between Depression and Physical Activity by (Weighted) Binary Logistic Regression Models
LCA of SES
Individuals in the low and middle SES groups exhibited notable socioeconomic disadvantages across multiple parts. In terms of health insurance coverage, a substantial proportion lacked any insurance (26.14% in low SES and 54.13% in middle SES) or relied on government insurance (60.63% in low SES and 26.46% in middle SES). Educational attainment in these groups was generally lower, with 19.33% (low SES) and 10.64% (middle SES) having less than a 9th-grade education. 22.68% low SES and 19.64% middle SES women had completed only grades 9–11. Very few had completed college or above (2.89% in low SES and 3.55% in middle SES). Employment and income patterns also reflected economic vulnerability. All individuals in the low SES group were unemployed, while all individuals in the middle SES group were employed. However, both groups had high proportions of individuals living below the poverty line, defined by a poverty-to-income ratio < 1.3, 68.24% in low SES and 67.61% in middle SES women. In contrast, the high SES group over 91% was covered by private health insurance. Educational levels were also higher, with 42.67% holding a college degree or above, and only 0.84% having less than a 9th-grade education. The majority were employed (65.96%), and nearly all (97.72%) had a poverty-to-income ratio ≥1.3, indicating financial stability. Proportion and classification resulting from LCA for each variable are illustrated in Supplementary Figs. S1 and S2.
Association of SES with the relationship between physical activity and depression
Figure 2 illustrates the relationship between physical activity and depression across different SES groups. After adjusting for age, race, marital status, BMI, and antidepressant medicine use, adequate physical activity was significantly associated with depression only among women with high SES (OR = 0.65, 95% CI: 0.50–0.86, p = 0.002; Supplementary Table S4), while no significant associations were observed in the low SES (OR = 0.83, 95% CI: 0.65–1.08, p = 0.200) or middle SES groups (OR = 1.12, 95% CI: 0.69–1.83, p = 0.600).
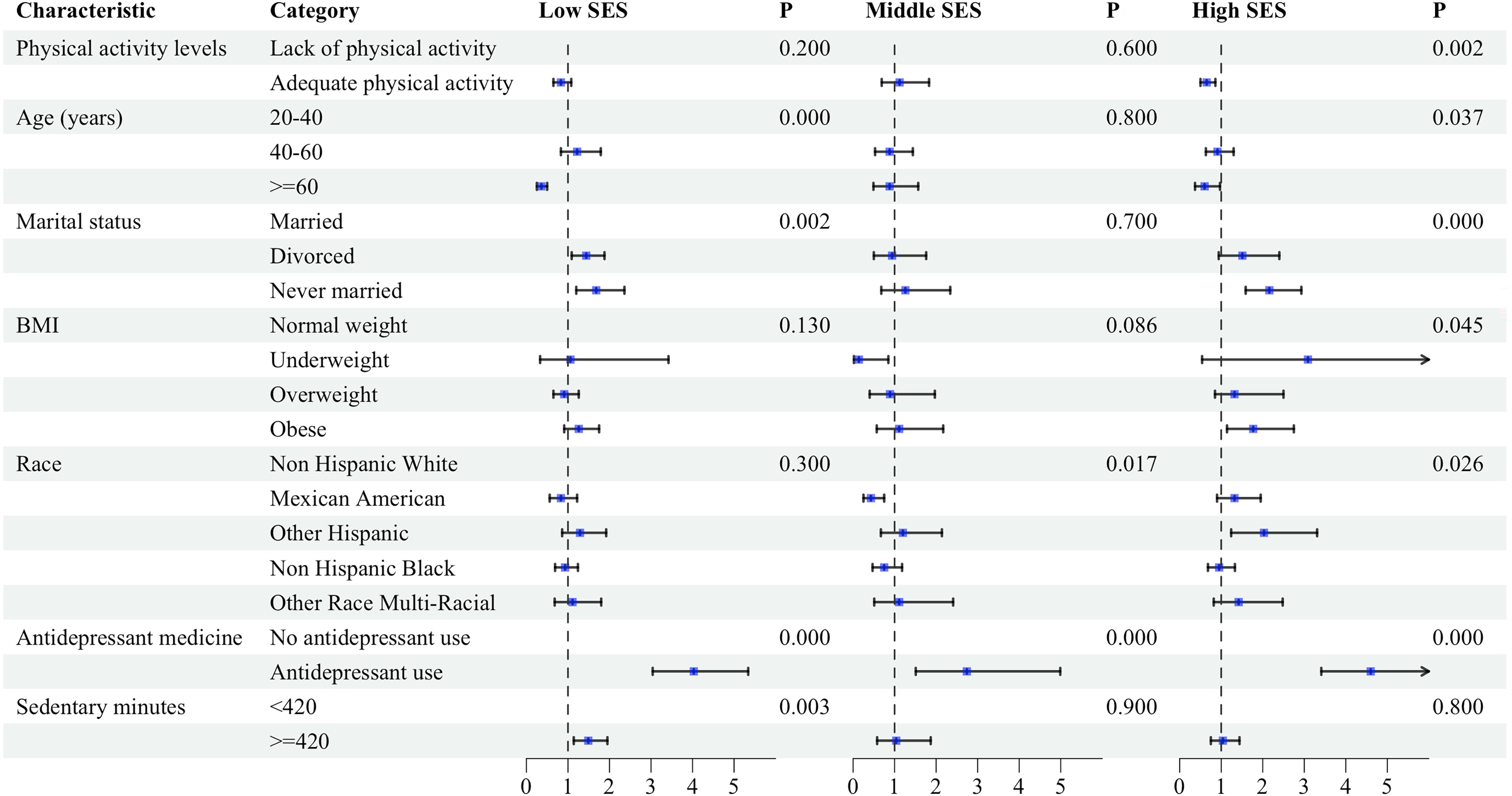
Forest plot of the association between depression and risk factors by SES. SES, socioeconomic status.
Discussion
Our analysis revealed that 11.5% of the total 14,691 participants exhibited depression. This aligns with the NHANES 2013–2016 depression survey by Brody et al., which found a similar prevalence rate of 10.4% among women. 7 Another NHANES study also indicated a higher prevalence of depression in females compared with males, with rates of 9.7% versus 6.3%, respectively. 32 Physiologically, females experience hormonal fluctuations during menstrual cycles and the postpartum period, potentially increasing susceptibility to depression. 33 Additionally, women tend to dedicate more time to household chores and childcare responsibilities, 34 which may heighten stress levels and psychological burdens, thereby amplifying the risk of depression. 35
In our study, the highest prevalence of degression was observed in the age group of 40–60 years (11.67%, 95% CI: 10.49–12.84), consistent with previous findings.7,36 Physiological factors associated with menopause, such as vasomotor symptoms, hot flashes, and night sweats, can adversely affect daily life, closely correlating with mental health problems. 37 Despite expectations, never-married females had twice the depression prevalence of married females (15.02%, 95% CI: 12.50–17.54 vs. 7.43%, 95% CI: 6.71–8.15), 38 possibly due to experiences of loneliness, reduced social support, and financial instability.39,40
Association between physical activity and depression
Our study’s findings align with previous findings highlighting the association between adequate physical activity and lower risks of depression. 41 After adjusting for various confounding factors, we found a significant relationship between physical activity and depression. The prevalence rate of depression was about 1.5 times higher in individuals with a lack of physical activity compared with those with adequate physical activity (12.64% vs. 8.43%). This supports the findings of Rutherford et al.’s cross-sectional study from NHANES 2011–2014, which demonstrated that engaging in at least 150 minutes of physical activity per week is associated with a lower risk of depression. 41 Overall, our study underscores the importance of physical activity in mitigating depression risk, particularly emphasizing the susceptibility of individuals lacking physical activity to depression.
Various mechanisms may contribute to how physical activity improves depression. First, individuals with depression often exhibit elevated levels of proinflammatory markers, such as interleukin (IL)-6 and tumor necrosis factor-alpha (TNF-α). Physical activity can create an anti-inflammatory environment by stimulating the adrenal glands to secrete adrenaline and cortisol, thereby promoting the production of anti-inflammatory IL-10 while reducing TNF-α production. 42 Second, physical activity can enhance body image and positively impact self-esteem, serving as a foundation for generating positive emotions. 43 Moreover, studies indicate that individuals with depression often lack protective social support, sustaining physical activity may increase social interactions, contributing to improved social support.44,45 This is supported by our findings regarding sedentary minutes, which indicate a higher prevalence of depression among individuals with longer sitting times.
Depression physical activity association varies by SES
After examining the relationship between physical activity and depression across different SES levels, our findings indicate that adequate physical activity was significantly associated with depression only among women with high SES, with no significant associations observed in the middle or low SES groups. The worsening health disparity situation in the United States underscores the urgency of addressing SES-related inequalities. 46 SES plays a pivotal role in determining access to resources and is associated with disparities in health threats. Middle or low SES may lead to negative cumulative effects, where repeated exposure to economic stress and consequences impacts mental health, including depression. Research has shown that individuals with lower SES exhibit more cynicism, pessimism, and poorer health outcomes compared with those who have never experienced poverty. 47 Furthermore, individuals with disadvantaged SES may experience a cumulative burden of adversities and trauma, exacerbating mental health issues.48–50 Survey focused on low SES African American and Latino populations has shown that the experiences of discrimination, childhood trauma, and chronic stress contribute to this burden, highlighting the complex interplay between SES and mental health. 48
Our analysis of the influence of SES on depression revealed that each SES component uniquely affects the prevalence of depression. Specifically, adults with higher education levels exhibited a lower prevalence of depression, with those holding a college graduate or above education level demonstrating a prevalence rate of 5.08. This finding is consistent with previous research suggesting that higher education levels are associated with a lower likelihood of depression. 51 For instance, a European study observed a 3% decrease in the probability of experiencing depression for each additional year of education among participants. 52 Moreover, individuals with high SES typically possess high levels of education due to factors such as family environment and self-efficacy. 53 Conversely, those with middle and lower educational levels may have limited knowledge about physical activities and receive fewer reminders about their importance. 54 Additionally, our study found that the prevalence of depression among unemployed individuals was significantly higher than among employed females, consistent with previous research linking worsened mental health to lower levels of physical activity among the unemployed. 55 Furthermore, disparities in depression were evident based on family income to poverty ratio, with females having a ratio of <1.3 exhibiting a higher prevalence of depression. This aligns with prior studies, with individuals below the federal poverty line experiencing twice the prevalence of depression compared with those above. 56 In terms of resource accessibility, individuals with a high SES find it easier to access physical activity facilities and resources, such as organized sports training and fitness coaching. They can afford the financial and time costs of physical activities. 57 However, it is noteworthy that despite relatively low-cost activities such as walking and jogging, individuals with middle and low SES still tend to adopt unhealthy behaviors. 58 In addition, the nature of physical activity may differ across socioeconomic groups. 59 Among women with middle and low SES, physical activity, such as walking or cycling, may largely reflect occupational or transportation-related activity rather than intentional exercise, which may not confer the same benefits as recreational physical activity. 60 Therefore, the observed association between physical activity and depression may be diluted in middle and low SES groups. High SES individuals often have better baseline mental health, greater access to health care, and more robust social support systems, which may enhance the effects of physical activity interventions. 61 These findings provide new insights into the association between physical activity and mental health and underscore the importance of considering socioeconomic disparities in addressing mental health issues.
Implications
While the association between physical activity and depression has been widely studied, our research builds on this foundation using a more comprehensive and recent dataset, NHANES 2007–2020.21,62 Special attention must be directed toward never-married women and women aged 40–60, both of whom are at high risk of depression. Our research underscores the significant association between adequate physical activity and lower depression prevalence, emphasizing the imperative of promoting and advocating for adequate physical activity among middle-aged never-married women.
Additionally, the association between physical activity and depression varies across SES, with a significant effect observed only among women with high SES. Consequently, interventions focusing solely on lifestyle medicine may overlook the needs of middle or low SES women. These findings highlight the importance of considering socioeconomic context in mental health promotion strategies, particularly in designing physical activity interventions for women. Public health programs should prioritize resource allocation and accessibility in middle and low SES communities to address structural barriers. Clinicians and policymakers must recognize that a one-size-fits-all approach may reinforce existing health inequities rather than resolve them. Future initiatives should tailor interventions to diverse SES groups to ensure equity in mental health outcomes.
Limitations
Despite providing insights into the relationship between depression and physical activity in women, there are several study limitations. First, the cross-sectional data limit our ability to infer causality between physical activity and depression, with depression measured at a single point. Second, we must consider hormonal changes during premenstruation and menopause in women’s vulnerability to depression. Third, we did not explore other factors such as social support and community influences. This may limit the comprehensiveness of our conclusions and fail to fully explain the development of depression in participants. Another limitation is that the exclusion of participants with missing data on key variables (physical activity, depression, and SES) may have introduced selection bias, particularly if certain population subgroups were more likely to have missing data, which could affect the representativeness of the analytic sample. Finally, the NHANES physical activity measures do not distinguish whether walking or cycling is performed for occupational, transportation, or recreational purposes, which may introduce bias across socioeconomic groups.
Conclusions
Our study is the latest, most comprehensive, and nationally representative study of women in the United States, highlighting that adequate physical activity is associated with a lower prevalence of depression, with this association reaching significance only among women with high SES. Moving forward, our research contributes to identifying populations at heightened risk of depression, elucidating SES disparities in mental health, and emphasizing the importance of tailored interventions and public health policies.
Authors’ Contributions
Y.Y.: Writing—original draft and formal analysis. J.X. and X.Y.: Conceptualization. L.F.: Methodology. H.L.: Supervision. J.H.: Conceptualization and writing—review and editing.
Data Availability Statement
The data used in the study are publicly available on the NHANES website. https://wwwn.cdc.gov/nchs/nhanes/Default.aspx
Statement of Ethics
The NHANES database was approved by the Institutional Review Board of the National Center for Health Statistics, and all participants provided informed consent.
Footnotes
Acknowledgments
The authors sincerely thank Jiayi Ji for his valuable contributions to this article. His efforts in refining the grammar and providing numerous helpful suggestions have significantly improved the clarity and quality of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.