
Abstract
Background:
Postpartum depression (PPD) is a mood disorder affecting women during pregnancy or after childbirth, characterized by persistent sadness, anxiety, and difficulty bonding with the newborn. Symptoms range from mild emotional disturbances to severe depressive episodes requiring urgent clinical intervention. Despite the availability of treatments, PPD often remains underdiagnosed and undertreated. This study demonstrates an efficient method to predict the Edinburgh Postnatal Depression Scale (EPDS) scores based on combined acoustic and linguistic features extracted from speech.
Methods:
Pregnant and postpartum women aged 18 years or older were recruited for a structured screening study conducted between 2023 and 2024 (n = 275). Each participant completed the full EPDS questionnaire and provided a single open-ended audio response recorded via a smartphone application. A multimodal approach combining linguistic and acoustic features was used to predict EPDS scores, capturing both semantic content and paralinguistic markers, such as vocal pitch, speech rate, and prosody, reflective of mood and affect. Features from both modalities were combined using a regressor to produce a numeric EPDS score ranging from 0 to 30.
Results:
The model achieved a sensitivity of 84.4% (95% confidence interval [CI]: 77.5–89.5) and a specificity of 76.9% (95% CI: 69.0–82.2) at the ≥10 screening threshold, with an area under the curve of 0.886 (95% CI: 0.845–0.922). Regression performance demonstrated a Pearson correlation of R = 0.749 (95% CI: 0.69–0.80) and a mean absolute error of 3.42 compared with the ground-truth EPDS scores.
Conclusion:
This model demonstrates strong screening performance for identifying PPD risk from brief video responses and can augment clinical workflows by prioritizing follow-up evaluation when elevated EPDS risk is detected.
Introduction
Postpartum depression (PPD) is a serious, often disabling mood disorder affecting ∼12%–15% of mothers globally, with rates varying by population and screening methodology, 1 and has been rising across the last decade. 2 In the United States, ∼600,000 women experience PPD yearly. 3 When left untreated, this condition can have lasting impacts on women’s well-being, early childhood development, 4 and familial stability. Symptoms can range from resentment toward the child, depression, and general irritability and may be as severe as suicidal ideation. These symptoms can begin during the pregnancy process and can persist months after the birth if left untreated. The consequences of untreated PPD extend beyond the mother’s well-being, increasing risks for impaired mother–infant bonding, delays in childhood emotional and cognitive development, and long-term effects on family stability. 4
Despite the availability of validated screening tools such as the Edinburgh Postnatal Depression Scale (EPDS), many cases of PPD remain undiagnosed or are identified late because of barriers such as limited access to mental health professionals, stigma, and lack of routine postpartum follow-up. 5 The EPDS is a widely adopted 10-item questionnaire that can be administered in clinical settings or self-administered by patients. However, speech-based assessments offer complementary capabilities: It enables asynchronous monitoring at multiple postpartum time points without clinic visits, captures paralinguistic markers of affect that are not available through text-based responses, and may feel more natural for patients who prefer conversational expression over structured questionnaires.
The rapid expansion of telehealth and remote care has created opportunities for technology-assisted mental health screening. Early detection of PPD could allow timely interventions, including counseling and pharmacologic treatment, to reduce maternal suffering and mitigate adverse effects on infants and families.
This study evaluates an audio-text multimodal machine learning model designed to predict EPDS scores from brief, open-ended video responses by combining linguistic and acoustic features through a multimodal architecture. The asynchronous nature of video-based assessment enables repeated screening at critical postpartum intervals (e.g., 2 weeks, 6 weeks, 3 months), which is particularly valuable given that PPD symptoms can emerge or intensify weeks to months after delivery. 6 This aims to augment existing clinical workflows by enabling scalable, automated PPD screening while maintaining clinical oversight for diagnostic confirmation.
Although this model is a powerful tool for screening individuals at risk of PPD and estimating EPDS scores, it is not designed to diagnose PPD and should not be used in the absence of professional mental health professionals. It does not replace an in-person assessment by a clinician for definitive diagnosis or management.
Methods
Participants were recruited through Prolific, an online crowdsourcing platform, as part of product development and research. Eligible participants were adult women (18 years of age or older) who were currently pregnant or had given birth within the last 12 months and resided in the United States. All participants provided informed consent prior to participation. Data collection occurred independently of clinical care, with no research-specific interventions. This research was determined by Advarra to be exempt under Category 4 of 45 CFR 46.104.
Although 481 individuals initially registered, 342 (71%) successfully completed both study components (video response and EPDS questionnaire), thereby establishing the eligible participant pool. Participants were excluded for the following reasons:
Platform-related exclusions included incomplete enrollment due to lack of consent, timeout, or personal withdrawal (N = 42). For duplicate submissions in which participants submitted multiple recordings within a single session, only the final submission was retained (N = 95). One participant with missing demographic data (N = 1, 0.2%) who did not respond within the predetermined time window was excluded.
This yielded N = 343 participants (71.3%) who completed both the video and EPDS assessments.
Technical quality screening of the 343 completed responses identified 68 exclusions. First, 13 (20%) assessments were excluded because of technical pipeline errors, including audio-processing errors or transcription failures that produced no usable text. Second, 46 participants produced responses that were clearly nonsubstantive and fragmented, such as “Thank you” or background TV noise. This type of minimal-effort behavior is common in crowdsourced research platforms, where participant compensation may incentivize rapid task completion over genuine task completion. The final subset of nine exclusions had substantive verbal responses but failed to complete the EPDS questionnaire, preventing ground-truth scores necessary for the analysis.
For clinical deployment, the first two categories would be handled differently, processing errors issues would trigger an automatic re-recording. Responses where patients engage in limited verbal content or low-effort responses would be flagged to providers as low-confidence estimates requiring follow-up responses. In a clinical setting, the final subset of nine incomplete questionnaires would not exist, as we would have no need for the counterfactual. We believe that this roughly 20% exclusion rate is therefore largely an artifact of the recruitment mechanism and is not expected to generalize to clinical deployment.
Participants were not tracked longitudinally across their prenatal to postnatal periods; rather, each video recording was used for model training, with the EPDS score associated with that participant and assessment date serving as the ground truth. Participants who appeared in both studies were treated as independent observations rather than being tracked across time. The final sample of N = 275 represents 275 unique assessment sessions.
Prenatal depression encompasses depressive episodes occurring during pregnancy and the postpartum period and is driven by dramatic hormonal fluctuations throughout this continuum. Although the DSM-5-TR defines “peripartum onset” as beginning during pregnancy or within 4 weeks of delivery, clinical experts and researchers have extended this vulnerable period to 12 months postpartum to capture the full spectrum of hormonally moderated mood disturbances.7,8 Given that depression can manifest throughout this hormonally dynamic period, the dataset included N = 208 prenatal women and N = 67 postnatal participants. The model’s performance was evaluated in both groups as described in the “Results” section.
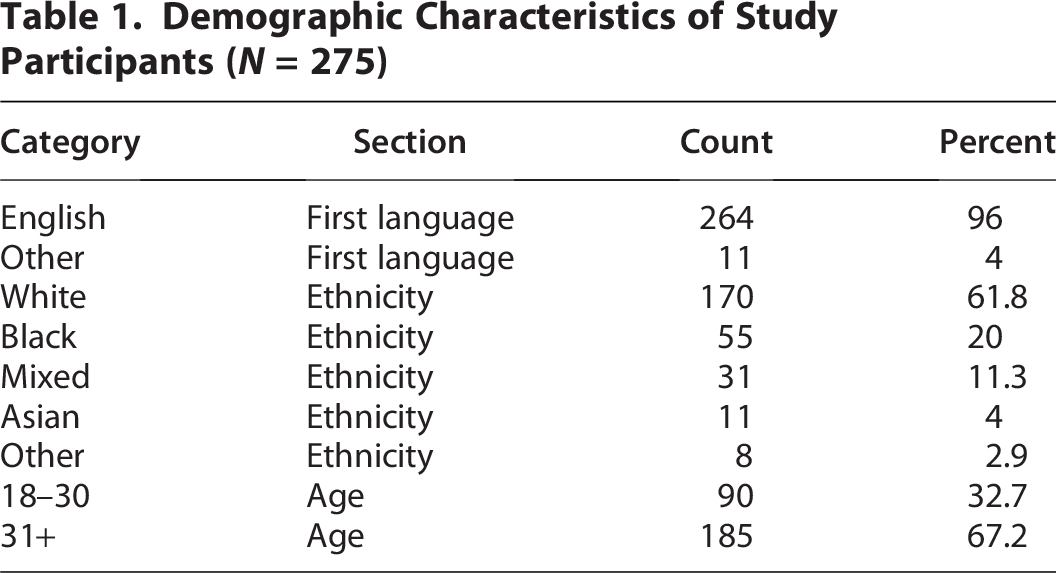
The demographic characteristics of the study participants are detailed in Table 1 (N = 275). Unsurprisingly, given the population of American women, the participant group was largely English-speaking, with 96% reporting English as their first language. The sample was predominantly White (61.8%), with Black participants (20%) forming the largest ethnic minority group. The age distribution reflected a higher proportion of women aged 31 years and older (67.2%), consistent with typical postpartum care-seeking patterns (Fig. 1).
Demographic Characteristics of Study Participants (N = 275)
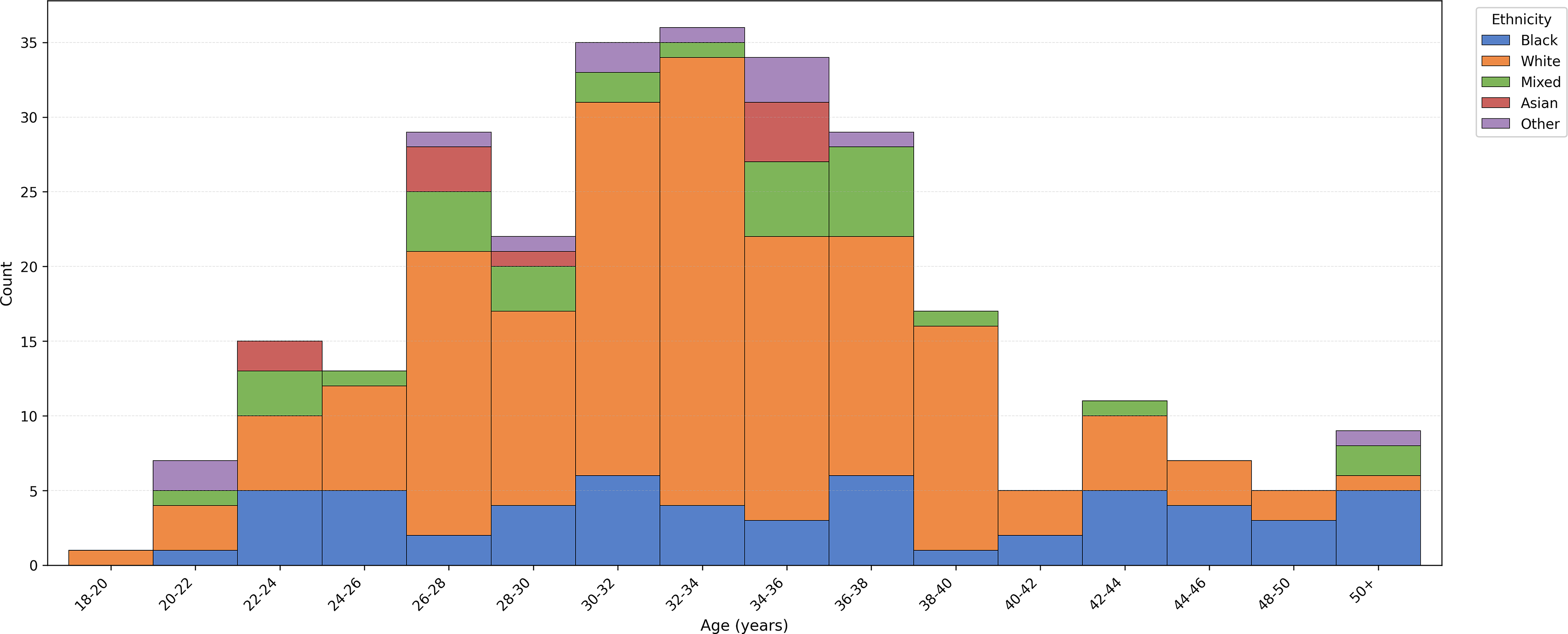
Participant age distribution by ethnicity.
Internal data cleaning allowed for patients to take multiple recordings of their video response within a single assessment session; however, only the last one submitted through the platform was retained. This was done in case the patient was interrupted during a take and as a way to improve the patient experience by building familiarity with the application. Any participants who were in both studies were treated as different observations entirely rather than tracking the same person across time.
Each participant was asked to respond via a video recording to the following prompt:
In the last two weeks have you felt down, nervous, depressed, anxious, hopeless or on edge? If so, please explain in detail how it has bothered you or impacted your life.
Upon completing the video response, each participant completed the EPDS questionnaire, ensuring that any re-recordings were completed prior to the structured self-reflection questions of the survey. This structure ensured the speech would not be influenced by the structured self-reflection survey questions. The EPDS score (0–30 scale) was considered the ground truth, and the data extracted from the video response served as model inputs.
Multimodal model architecture
This model was trained using a multimodal architecture designed to predict EPDS scores from video responses through parallel processing of both textual and acoustic information.
Feature extraction
Video recordings were processed using two parallel pipelines. Text transcripts were generated using the Whisper transcription model (large-v2) and processed using a fine-tuned DeBERTa-v3-base transformer model (learning rate 2 × 10−5, batch size 16, 3 epochs) to generate linguistic embeddings. DeBERTa-v3-base was selected for its superior performance on natural language inference tasks and its ability to capture nuanced linguistic patterns associated with mental health indicators. Raw audio was segmented into 10-second chunks (16 kHz sampling rate) and processed through a pretrained HuBERTtransformer model (facebook/hubert-large-ll60k) to extract acoustic features capturing prosodic patterns, pitch variations, and speech rhythm.
Multimodal fusion and regression
The extracted linguistic and acoustic embeddings were processed through separate neural networks. For linguistic embeddings, the model averaged across token-level representations to create a fixed-size vector. For acoustic embeddings, the model extracted the primary output channel and averaged across time steps. The combined embeddings were then fed into a regularized ElasticNet regression model (α = 1.0, l1_ratio = 0.5) that predicted continuous EPDS scores on a 0–30 scale. ElasticNet was chosen for its ability to handle high-dimensional feature spaces while providing interpretable feature weights.
To assess the relative contribution of each modality, ablation experiments were conducted using ridge regression on frozen embeddings from each modality independently and in combination. These experiments were intended to quantify the relative modality contribution rather than replace the full fine-tuned deep learning pipeline. It is no surprise, therefore, that the absolute metrics differ slightly. The linguistic-only model achieved a Pearson correlation coefficient of R = 0.677 (95% CI: 0.590–0.749), mean absolute error (MAE) = 3.74, and area under the curve (AUC) = 0.860 at the ≥10 threshold. The acoustic-only model achieved Pearson R = 0.378, MAE = 5.54, and AUC = 0.717. The combined model achieved Pearson R = 0.635 (95% CI: 0.526–0.717), MAE = 3.94, and AUC = 0.844 (Fig. 2).
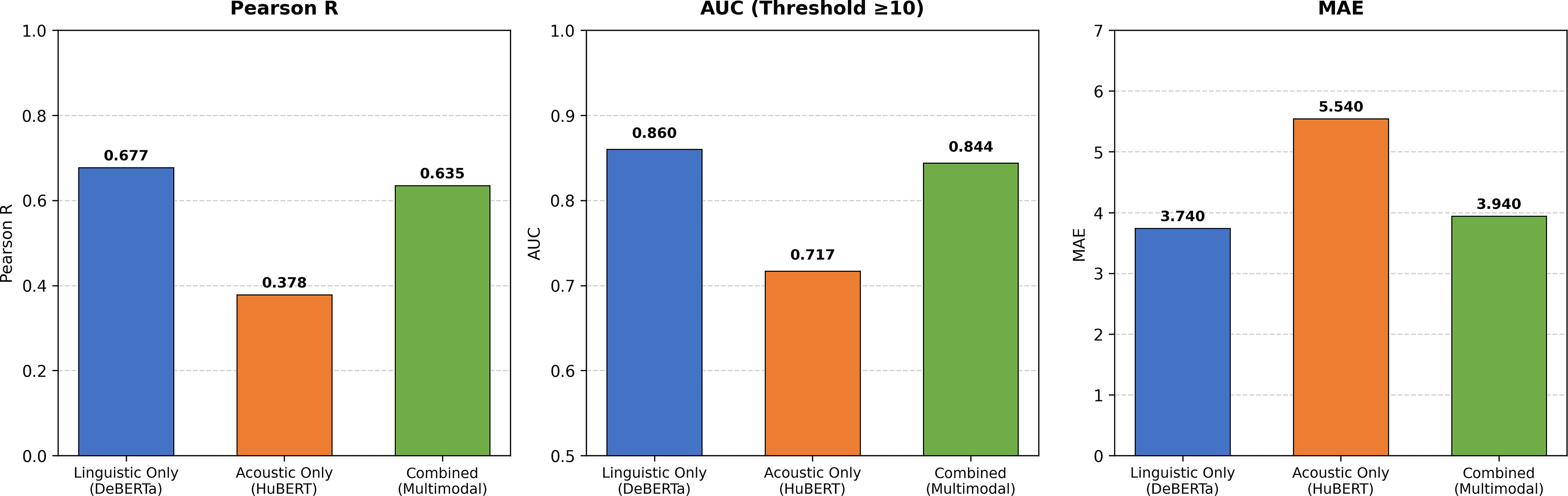
Modality comparison—linguistic vs. acoustic vs. combined.
These findings indicate that semantic content is the dominant predictive signal, consistent with the open-ended narrative prompt eliciting rich linguistic content about a patient’s emotional state. Critically, the linguistic embeddings generated by DeBERTa-v3-base encode contextual semantic relationships across the full response rather than simple keyword frequency counts, capturing nuances such as negation, hedging, and emotional framing that would be invisible to simple keyword tallying. The acoustic-only AUC of 0.782 confirms that paralinguistic features capture a genuine independent signal; however, the marginal gain of the combined model over the linguistic-only model suggests that future work exploring acoustic architectures more explicitly targeting prosodic depression markers may better leverage this complementary modality.
Post hoc calibration
To ensure clinical efficacy, the raw regression outputs underwent distribution-aware calibration to match the empirical EPDS score distribution observed in the training data. Calibration is standard practice in clinical prediction modeling used to align model outputs with clinically meaningful score distributions.9,10 This process addressed the systematic compression toward the mean, a common phenomenon in regression models trained on imbalanced data. The calibration process applied monotonic transformations to map predictions to the clinically appropriate score range (0–30) while preserving discriminative ability (AUC). Calibration parameters were fit exclusively on the training data within each cross-validation fold to prevent information leakage.
Training infrastructure
The linguistic and acoustic components were processed separately and then combined during inference. The architecture supports both single-modality and multimodal prediction modes, with the combined approach demonstrating improved performance by leveraging complementary information from both feature sets. The system incorporated automatic quality checks: when audio quality or transcription confidence fell below minimum thresholds, the model withheld scoring and could prompt for re-recording to ensure prediction reliability.
Statistical analysis
Cross-validation was performed using five-fold stratified sampling based on EPDS score groups to ensure balanced representation across depression severity levels. Participants were grouped by individual to prevent data leakage across folds; this ensured that all recordings from the same participant appeared in only one fold, addressing cases in which individuals contributed multiple recordings at different pregnancy or postpartum time points. Within each fold, the ElasticNet regressor was trained on the training data, after which calibration parameters were fit exclusively from the training fold predictions to map raw outputs to the 0–30 EPDS scale. These parameters were then applied to validation-fold predictions, ensuring no information leakage.
Confidence intervals (CIs) for the correlation coefficient were calculated using Fisher’s z-transformation. CIs for AUC were calculated using bootstrap resampling with 1000 iterations. 11 CIs for sensitivity, specificity, and other classification metrics were calculated using Wilson score intervals.
Results
The model demonstrated strong discriminative performance, with an overall AUC of 0.890 (95% CI: 0.846–0.921) across the full dataset (N = 275), indicating excellent ability to distinguish between depression risk categories. Correlation analysis between predicted and true EPDS scores showed a strong positive relationship, with a Pearson correlation coefficient of R = 0.749 (95% CI: 0.69–0.80), indicating the model’s ability to accurately rank order depression severity across the full 0–30 EPDS range. The model achieved an MAE of 3.42 and a root mean square error (RMSE) of 4.35.
The model’s prediction distribution demonstrated good coverage across the full EPDS range, with predictions tracking true scores at both the low and high ends of the scale. At the primary screening threshold of EPDS ≥ 10, the model achieved a sensitivity of 84.4% and a specificity of 76.9%, as shown in Table 3, representing a clinically appropriate balance for an initial screening tool in which minimizing false negatives or missed cases is the higher priority (Fig. 3).
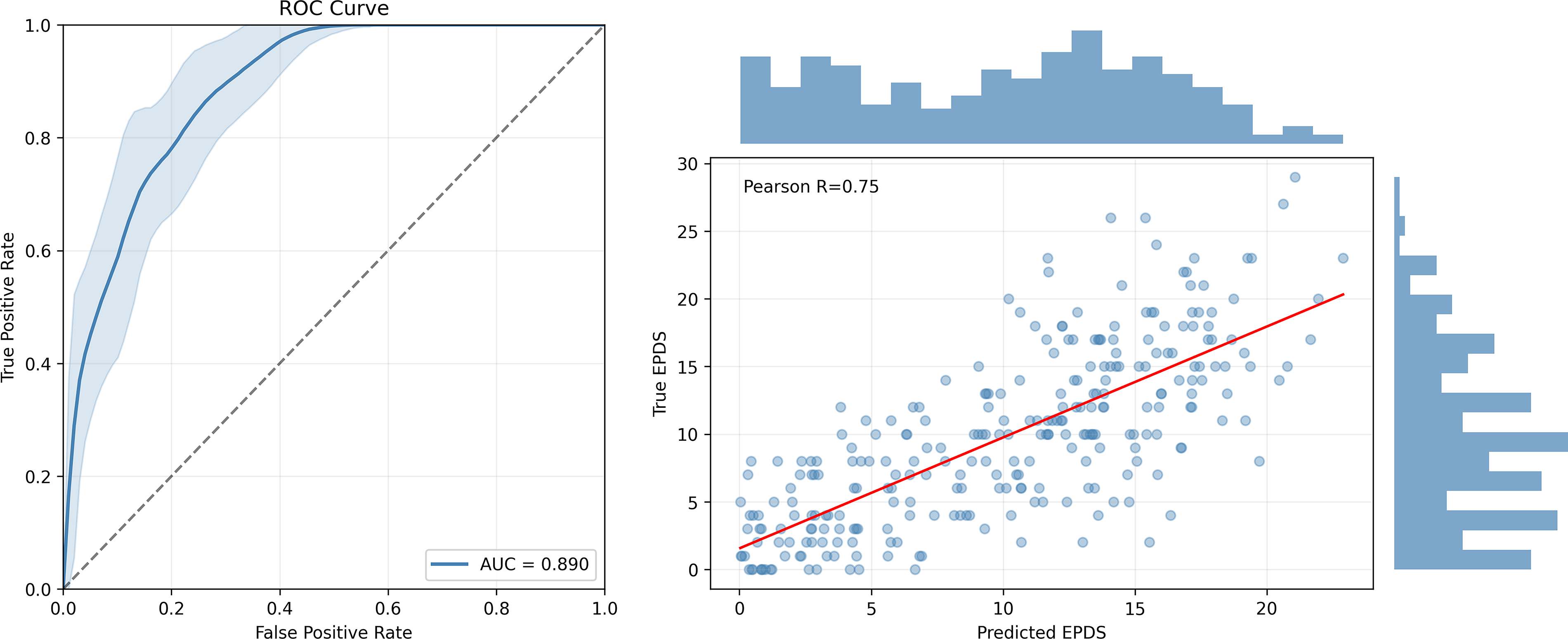
Model performance evaluation.
The 15.6% false-negative rate at this threshold was concentrated among participants with moderately elevated EPDS scores in the range of 10–13 (Fig. 4). Again, this is consistent with the pattern of distinguishing borderline-risk cases from low-risk cases in a clinical setting, which we feel does not discredit the model’s efficacy.

EPDS score distribution (N = 275). EPDS, Edinburgh Postnatal Depression Scale.
At the standard clinical cutoff of EPDS ≥ 13, continuous predictions were converted to binary risk classifications (Table 2). The model achieved 75.3% (95% CI: 65.4 − 83.1) sensitivity and 80.6% specificity (95% CI: 74.4 − 85.7), with 78.9% overall accuracy (CI: 73.7 − 83.3). However, recent meta-analytic evidence and clinical guidelines support the use of lower EPS thresholds in screening contexts where maximizing case detection is prioritized. Postpartum Support International recommends EPDS ≥ 10 as the standard screening threshold, 12 and the largest meta-analysis to date, Levis et al., 13 found this cutoff optimizes sensitivity and specificity for detecting major depression in prenatal women.
Edinburgh Postnatal Depression Scale Prediction Results (N = 275)
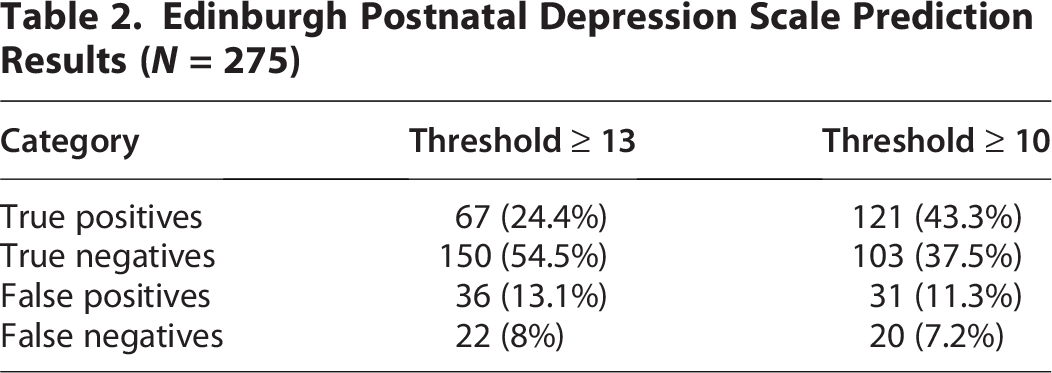
Applying EPDS ≥ 10 to the model predictions improved sensitivity to 84.4% (95% CI: 77.5 − 89.5) while maintaining 76.9%% specificity (95% CI: 69.0 − 83.2) and 80.7% overall accuracy (95% CI: 75.7–85.0). In screening contexts, we prioritize this lower threshold because the cost of missing a woman in need of mental health support substantially outweighs the cost of offering additional assessment to someone at slightly lower risk. This approach aligns with screening best practices that emphasize minimizing false negatives in vulnerable populations.
For practical deployment, we recommend a tiered approach: a low risk, <10, a medium risk range between 10 and 12, and a higher risk cut off of ≥13. This stratification may help identify individuals at the margin and enable early intervention when appropriate.
Table 3 provides the corresponding clinical performance metrics.
Clinical Performance Metrics
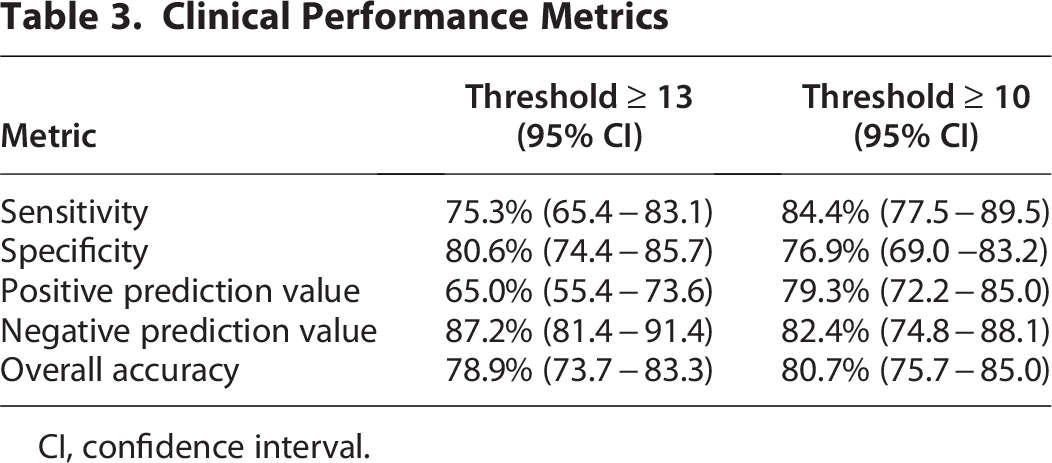
CI, confidence interval.
Comparison to standard EPDS administration
At the optimized threshold of ≥10, the model achieved a sensitivity of 84.4% (95% CI: 77.5–89.5) and a specificity of 76.9% (95% CI: 69.0–83.2). The model’s high sensitivity, paired with moderate specificity, represents a clinically appropriate trade-off for screening applications, where missing cases of PPD carries greater risk than additional follow-up assessments. At the standard clinical threshold of ≥13, the model achieved 75.3% sensitivity and 80.6% specificity, as seen in Table 3.
For context, published meta-analyses report that standard EPDS administration achieves a sensitivity of 66% (95% CI: 58–74) and a specificity of 95% (95% CI: 92–96) when validated against clinical diagnostic interviews at similar thresholds. 10 However, direct comparison is not appropriate: EPDS validation studies measure performance against clinical diagnosis (the gold standard), whereas the present model measures agreement with EPDS scores. The model’s performance metrics therefore reflect its ability to replicate EPDS-based risk stratification from speech, enabling accessible screening without questionnaire administration. Like the EPDS itself, this tool serves as first-tier screening method to identify individuals who may benefit from further clinical evaluation rather than as a diagnostic instrument.
This approach addresses documented gaps in current screening: ∼40% of postpartum women do not attend postpartum visits, 13 and screening is inconsistently performed even among attendees. Smartphone-based assessment relieves barriers 14 (transportation, childcare, clinic availability), enables repeated screening at multiple time points without clinic visits, and captures paralinguistic markers (prosody, pitch, rhythm) not available from questionnaires.
This tool augments, rather than replaces, clinical assessment, serving as first-tier screening method to prioritize follow-up for at-risk patients by sending additional telehealth resources. Women flagged as high risk would still complete formal clinical evaluation.
Performance across demographic subgroups
Researchers evaluated the model’s discriminative performance across demographic subgroups to assess potential bias and ensure equitable accuracy (Table 4). Overall, performance remained strong across most groups. Among White participants (N = 181), the model achieved an AUC of 0.915, whereas performance among Black participants (N = 53) was at 0.834. The difference was not statistically significant (p = 0.127, 95% CI: −0.012 to 0.094). Those identifying as Mixed ethnicity (N = 18) achieved an AUC of 0.838 (95% CI: 0.639–1.00); however, the wide CI reflects the limited sample size of this specific subgroup.
Model Performance By Demographic Group (N = 275)
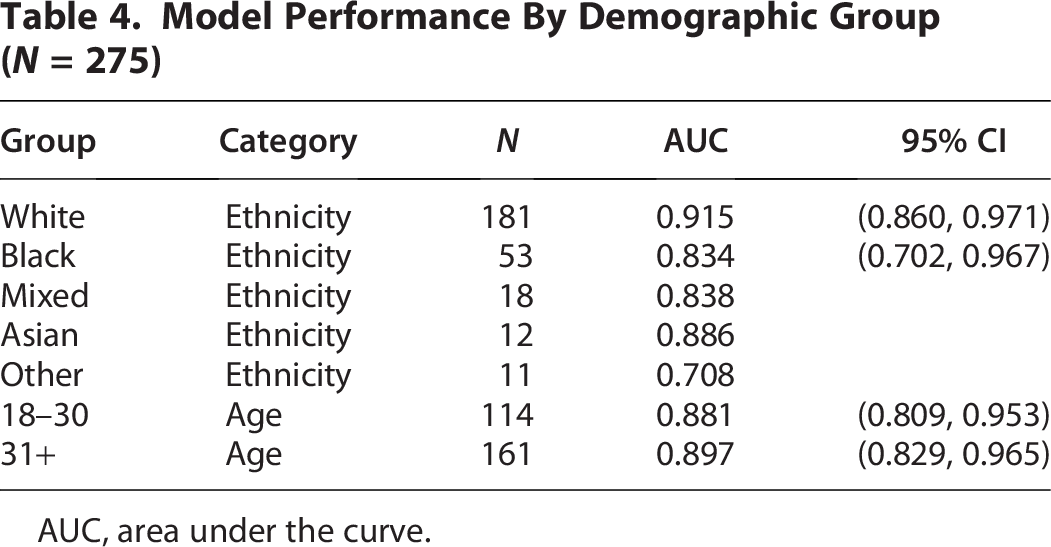
AUC, area under the curve.
Smaller subgroups also had inadequate sample sizes for reliable performance assessment. The Asian (N = 12) and Other (N = 11) subgroups were severely underrepresented, limiting the precision of performance estimates in these groups. To address statistical power limitations while testing for systematic bias, researchers compared White participants (N = 181, AUC = 0.900, 95% CI: 0.893–0.907) to all non-White participants aggregated (N = 94, AUC = 0.838, 95% CI: 0.752–0.925). The 0.077 difference in AUC was not statistically significant (p = 0.141, 95% CI for difference: −0.026 to 0.018), indicating no evidence of systematic performance disparities between White and non-White participants.
Similarly, age-based analyses demonstrated no significant performance variation, with the 18–30 age group achieving AUC = 0.881 (N = 14, 95% CI: 0.809–0.953) and the 31+ group achieving AUC = 0.897 (N = 161, 95% CI: 0.829–0.965, p = 0.743). Taken together, these findings suggest that the model demonstrates generalizable performance across major demographic dimensions.
Finally, model performance was evaluated separately in the prenatal group (n = 208) and postpartum group (n = 67). Both groups demonstrated strong discriminative performance, with their performance values seen in Table 5. Although there were nearly four times as many prenatal as postpartum observations, independent sample t-tests comparing prediction residuals (p = 0.841) and MAE (p = 0.866) between groups revealed no statistically significant differences, indicating consistent model performance across pregnancy stages.
Model Performance By Perinatal Period Group (N = 275)

RMSE, root mean square error; MAE, mean absolute error.
Discussion
The results demonstrate the potential to utilize acoustic-linguistic multimodal machine learning to monitor for PPD risk through the analysis of video-recorded speech. Smartphone video recording provides a convenient and accessible medium for capturing high-quality audio while preserving speech naturalness that may be lost in phone-only interactions. When the algorithm identifies elevated depression risk, health care providers are encouraged to conduct further evaluation to determine appropriate interventions. This approach represents an opportunity to provide patients with the required monitoring at standard intervals or with increased frequency based on risk stratification.
The decision to use video recording as the data collection medium, while analyzing only audio and linguistic content, provides several advantages. First, video recording via smartphone is now ubiquitous and user-friendly, reducing barriers to participation. Second, it allows users to review their recording and re-record them if desired. Finally, facial analysis represents an untapped modality that could expand as a future input and features to the models.
The model demonstrates that speech-based features can effectively predict EPDS scores, achieving strong discriminative performance (AUC = 0.89, R = 0.77). This indicates that linguistic and acoustic patterns in spontaneous speech encode substantial information relevant to the mental health dimensions captured by EPDS, enabling automated risk stratification without requiring questionnaire completion.
In traditional workflows, EPDS questionnaires serve as a first-line screening tool, identifying individuals who warrant clinical evaluation; meta-analyses have reported that the EPDS achieves 66% sensitivity when validated against diagnostic interviews. 13 The speech-based approach occupies the same position in the screening cascade of identifying individuals with elevated EPDS indicative risk who should receive follow-up assessments. The 84.4% sensitivity reflects the model’s ability to replicate EPDS-based risk categorization from speech, not its ability to detect a clinical diagnosis.
This distinction is crucial. The model makes first-tier screening more accessible and asynchronous while also capturing paralinguistic markers. However, like the EPDS itself, it flags potential risk rather than providing a diagnostic conclusion. Both approaches ultimately rely on clinical confirmation to establish actual depression diagnosis.
Standard EPDS administration faces significant real-world implementation barriers. Approximately 40% of postpartum women do not attend postpartum visits, 15 with substantially lower attendance among women facing unstable housing (odds ratio = 0.34, 95% CI: 0.18–0.67), transportation barriers, and communication difficulties. 16 Even among attendees, universal screening is inconsistently performed due to time constraints and competing clinical priorities.
Smartphone-based screening eliminates requirements for logistical concerns, which is particularly valuable for women in rural or underserved areas, those facing logistical barriers, uninsured or underinsured patients, and women experiencing stigma around mental health discussions.
The smartphone format also enables repeated assessments at multiple postpartum time points without clinic visits both during pregnancy and postnatal. This capability is critical because PPD can emerge or worsen after the traditional 6-week visit, and single-point screening, whether traditional or automated, cannot capture this dynamic disease course. Recording audio could enable longitudinal analysis to monitor changes in mental health throughout pregnancy and postpartum.
The consistent performance of the algorithm across demographic groups (Table 5) suggests that the model may be less susceptible to certain biases inherent in self-report instruments. 17 Traditional screening tools can be influenced by social desirability bias, cultural differences in expressing emotional distress, and literacy barriers. Paralinguistic features captured in spontaneous speech may provide complementary information that is less subject to these conscious or unconscious reporting biases.
Clinical Implementation
This tool functions as first-tier screening method within a stepped-care model: (1) automated speech screening for initial risk stratification, (2) clinical assessment for those meeting the EPDS threshold, and (3) treatment referral for confirmed cases. The tool’s role is to expand screening coverage and enable frequent monitoring, not to replace clinical judgment.
Limitations
The current approach incorporates both text-processing and audio-processing pipelines and focuses on end-to-end prediction accuracy. Given the architectural choices, the explainability is limited before the ElasticNet step.
When conducting comparisons across the different modalities, researchers found that the acoustic-only model severely underperformed compared with the linguistic-only model, and that the fusion of the two modalities did not improve over the linguistic baseline in our ablation experiments. However, the multimodal architecture was retained for several reasons. First, the acoustic signal captured by HuBERT in this setting reflects conversational speech elicited by an open-ended narrative prompt, which may not optimally activate the paralinguistic variance to be most predictive. Second, the present fusion strategy allows for future concatenation should advances in acoustic modeling improve the predictive utility of paralinguistic features.
Although the model was developed and validated in a diverse sample of U.S. pregnant and postpartum women, geographic restriction to a single country may limit generalizability. Cross-cultural validation is needed to ensure that the model performs equitably across different linguistic, cultural, and health care contexts, as depression presentation and help-seeking behaviors may vary across populations.
Although this study collected video recordings, the current model analyzes only acoustic and linguistic features and does not use visual information. The video recording format was maintained specifically to capture audio data and to enable future extensibility to video. Future iterations could integrate computer vision techniques to extract visual markers of depression, which may provide complementary information to speech-based multimodal modalities.
The model did not control for conception method or reproductive history, which may influence depression presentation and affect risk assessment accuracy. 18
The multimodal deep learning architecture limits interpretability because dense embeddings obscure the specific acoustic or linguistic features driving individual predictions. However, the structured ElasticNet regression layer enables feature importance analyses that can identify key predictive features. Additionally, the open-ended video format, unlike fixed multiple-choice screening, captures participants’ narratives in their own words, enabling richer qualitative insights and potential for future large language model analysis.
The sample was predominantly pregnant participants (75% vs. 25% postpartum). While additional postpartum data would improve balance, we found no statistically significant performance differences between prenatal and postpartum groups (p > 0.05), supporting the model’s validity across both populations.
Conclusion
This study demonstrates that self-administered, smartphone-recorded speech samples can reliably yield audio and linguistic data for automated EPDS prediction using multimodal machine learning. The recording format offers an accessible and scalable data collection while preserving audio quality for acoustic analysis and natural speech for linguistic analysis. Because PPD underdiagnosis is often exacerbated by insufficient screening resources and time constraints, speech-based assessment offers an alternative for women who may prefer verbal expression over written questionnaires. The underlying audio features also enable future extension to multi-condition assessment beyond depression alone. This technology has the potential to complement existing screening methods and improve the early identification of at-risk individuals for appropriate clinical evaluation.
The multimodal approach combining textual and acoustic analysis provides a comprehensive assessment that may capture subtle depression risk indicators missed by traditional screening methods. The model demonstrates robust generalization across demographic subgroups without significant performance degradation and provides accurate risk scores within the clinically expected range. This technology offers a promising solution for integrating depression screening into routine postpartum care workflows, ultimately improving maternal and child health outcomes through earlier intervention and treatment.
Ethics Statement
Data were collected during product development and market research activities, with informed consent from all participants. These activities were conducted independently of clinical care and involved no experimental intervention. The work was conducted under the exemption category described in 45 CFR 46.104(d)(4) for secondary research use of information collected for non-research purposes. The authors acknowledge that as this research is intended to inform clinical applications, future prospective studies will be submitted to a commercial or institutional IRB for formal review prior to data collection, consistent with best practices for industry-sponsored human subject research.
Footnotes
Acknowledgments
The authors conducted this research independently and have no acknowledgments to declare.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by Videra Health Inc. as part of the authors’ employment.