
Abstract
Background:
This study examined the associations between specific adverse childhood experiences (ACEs) and hysterectomy among adult women and assesses the dose–response relationship with cumulative ACE exposure. It extends prior work by evaluating individual ACE categories while adjusting for gynecological cancers, diabetes, obesity, and selected health-risk behaviors.
Methods:
Data were drawn from the 2020, 2021, 2022, and 2024 Behavioral Risk Factor Surveillance System (BRFSS), including 119,165 women across 26 U.S. areas with available data on ACEs and hysterectomy. Multivariable logistic regression estimated associations between ACEs and hysterectomy, adjusting for covariates.
Results:
Approximately 24.2% of participants reported a history of hysterectomy, and 65.8% reported at least one ACE. All but one of the 11 ACE items were independently associated with higher odds of hysterectomy after adjustment for age, race/ethnicity, marital status, education, annual income, survey year, area, gynecological cancers, diabetes, obesity, physical activity, smoking, and alcohol consumption. The strongest associations were observed for childhood sexual abuse, including unwanted sexual touching and forced sexual intercourse. The ACE distribution was 34.2% for 0 ACEs, 33.5% for 1–2 ACEs, 15.5% for 3–4 ACEs, and 16.9% for ≥5 ACEs. The odds of hysterectomy increased in a dose–response manner with higher ACE exposure, becoming statistically significant at ≥3 ACEs after adjustment. The association between ACE count and hysterectomy did not differ significantly by age (p = 0.2464).
Conclusions:
ACEs, particularly childhood sexual abuse, were associated with higher odds of hysterectomy. These associations persisted after adjustment for demographic, clinical, and behavioral factors, suggesting long-term gynecological consequences of early-life adversity.
Introduction
Excluding obstetric procedures, hysterectomy is the most common major surgical operation among women, affecting approximately 15% of U.S. adult women, with prevalence increasing substantially with age (2.8% among ages 18–44 and 42% among those aged ≥75). 1 Hysterectomy is typically performed for a range of medical indications, including refractory abnormal uterine bleeding, severe uterine prolapse, advanced endometriosis, large fibroids, gynecologic cancers (ovarian, cervical, and uterine), chronic pelvic pain and other uterine disorders. 2 As such, hysterectomy should be reserved for clearly defined clinical indications.
Adverse childhood experiences (ACEs) have been linked to an increased risk of gynecologic conditions, including endometriosis, uterine fibroids, chronic pelvic pain, and more severe menopausal symptoms.3–11 Chronic stress resulting from ACEs may dysregulate the hypothalamic–pituitary–adrenal axis and sympathetic nervous system, leading to systemic inflammation and hormonal disruption that increase susceptibility to these conditions. 12 Accordingly, higher ACE exposure has been associated with an increased likelihood of hysterectomy.5,13–15
Prior studies have attempted to explain this relationship by adjusting for potential confounders. A retrospective cohort study of 2,648 women aged ≥55 years in England reported that ACEs were associated with an increased risk of hysterectomy and bilateral oophorectomy and that this association persisted after adjustment for socioeconomic position, smoking, marital status, obesity, reproductive history, and related health behaviors. 13 However, although this study examined cumulative ACE exposure, it did not assess associations with individual ACE types and was limited to older women.
A smaller population-based cohort study of 128 women undergoing bilateral oophorectomy found that exposure to childhood abuse before age 19 was associated with an increased risk of surgery before menopause, even after adjustment for socioeconomic, behavioral, and mental health factors. 14 However, the limited sample size and focus on oophorectomy rather than hysterectomy restrict the generalizability of these findings.
In contrast, a study of 1,004 premenopausal female veterans found that childhood sexual assault involving vaginal penetration and posttraumatic stress disorder were associated with earlier hysterectomy, potentially mediated by higher rates of gynecological disease. 15 Although this study had a larger sample, its findings were limited to veterans and specific trauma exposures.
Unlike prior research, the present study examines the associations between specific ACE types and hysterectomy in a nationally representative sample of U.S. women, including both premenopausal and postmenopausal individuals. In addition, we extend prior work by adjusting for a broader range of clinical and behavioral covariates, including gynecological cancers, diabetes, obesity, and health-risk behaviors.
Methods
Data
Analyses were based on data from the 2020, 2021, 2022, and 2024 Behavioral Risk Factor Surveillance System (BRFSS). The BRFSS is a nationally representative, health-related telephone survey that collects information from residents of U.S. states, the District of Columbia, and participating territories regarding health behaviors, chronic health conditions, and the use of preventive health services. 16 The survey is anonymous, cross-sectional, and administered annually using random probability sampling of the noninstitutionalized adult population aged 18 years and older. Each year, the BRFSS obtains more than 400,000 standardized interviews, making it the largest continuously conducted health survey system in the world. The BRFSS includes three components: (1) core questions administered annually to all participants, (2) rotating core questions, and (3) optional modules administered at the discretion of participating areas. The median response rates across participating areas were 44.8% in 2020, 43.4% in 2021, 45.1% in 2022, and 45.6% in 2024.17–20
All BRFSS participants provided informed consent before completing the interview. Detailed information regarding the survey design, questionnaire content, sampling procedures, and data collection methods has been published elsewhere. 21 The present study was deemed exempt from institutional review board approval because it used publicly available, deidentified BRFSS data and did not involve human subjects research.
Analyses were restricted to areas that administered both the ACEs module and the hysterectomy question. Eligible areas included 22 areas in 2020 (Alabama, Arizona, District of Columbia, Florida, Georgia, Hawaii, Idaho, Iowa, Kentucky, Mississippi, Missouri, Montana, Nevada, North Dakota, Rhode Island, South Carolina, South Dakota, Texas, Utah, Virginia, Wisconsin, and Wyoming), 1 area in 2021 (Mississippi), 8 areas in 2022 (Arkansas, Florida, Iowa, Nevada, New Hampshire, Oregon, South Dakota, and Virginia), no areas in 2023, and 8 areas in 2024 (Florida, Georgia, Hawaii, Nevada, North Dakota, Virginia, Puerto Rico, and the U.S. Virgin Islands). Across the 26 unique areas, 119,787 women provided information on ACEs and hysterectomy status. Participants who reported being unsure whether they had undergone a hysterectomy (n = 268; 0.27%) or who refused to answer the question (n = 354; 0.30%) were excluded, yielding a final analytic sample of 119,165 women.
The large and geographically diverse BRFSS sample, together with the availability of data on both ACEs and hysterectomy, provided a unique opportunity to examine their association among adult women in the United States.
Measures
Outcome variable
The outcome variable was hysterectomy (defined as an operation to remove the uterus [womb]).
Explanatory variable
The primary explanatory variable was ACEs. The 11 ACE items are shown in Table 3. For the first five items, “Yes” responses were coded as 1, and “No” or “Unknown” responses were coded as 0 for analytic purposes. The item assessing parental marital status was coded as 1 for parents not married. For the remaining six items, “Once” or “More than once” were coded as 1, whereas “Never” and “Unknown” responses were coded as 0. An ACE index was created by summing all 11 items and was categorized as 0, 1–2, 3–4, and ≥5 ACEs.
Covariates
Several covariates previously shown to be associated with hysterectomy were included in the analysis. 22 Demographic variables included age, race/ethnicity, marital status, education, annual household income, survey year, and area (Table 1).
Hysterectomy and Adverse Childhood Experiences (ACEs) According to Selected Demographic Characteristics Among U.S. Women
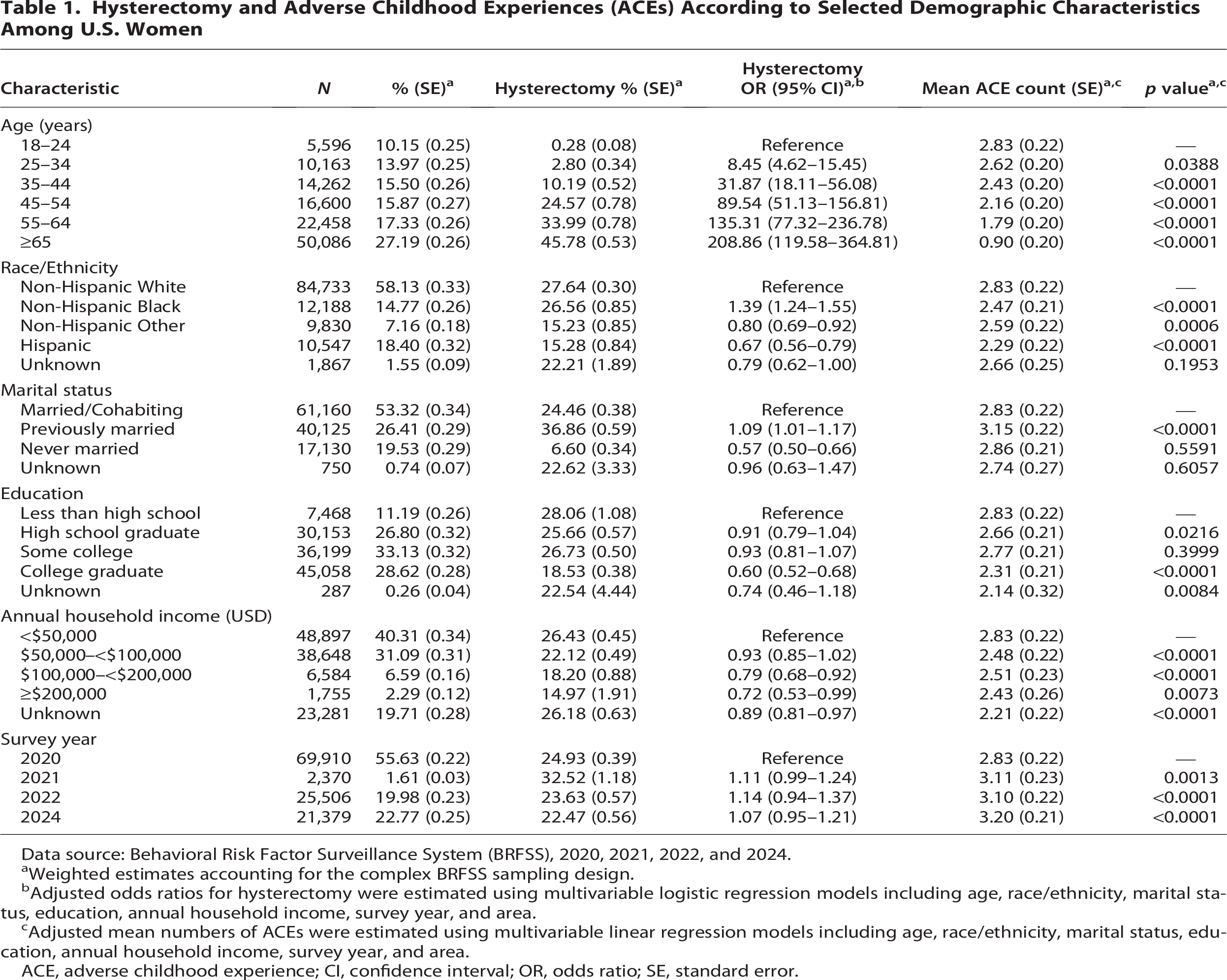
Data source: Behavioral Risk Factor Surveillance System (BRFSS), 2020, 2021, 2022, and 2024.
Weighted estimates accounting for the complex BRFSS sampling design.
Adjusted odds ratios for hysterectomy were estimated using multivariable logistic regression models including age, race/ethnicity, marital status, education, annual household income, survey year, and area.
Adjusted mean numbers of ACEs were estimated using multivariable linear regression models including age, race/ethnicity, marital status, education, annual household income, survey year, and area.
ACE, adverse childhood experience; CI, confidence interval; OR, odds ratio; SE, standard error.
Health-related covariates included self-reported history of cervical, ovarian, or uterine cancer, as well as diabetes status. Participants were asked whether they had ever been told by a health professional that they had diabetes, with response options including “Yes,” “Yes, but only during pregnancy,” “No,” “Pre-diabetes or borderline diabetes,” and “Don’t know/Not sure.”
Body mass index (BMI) was used to classify weight status as underweight (BMI < 18.5), normal weight (18.5 ≤ BMI < 25), overweight (25 ≤ BMI < 30), and obese (BMI ≥ 30).
Behavioral covariates included physical activity, smoking status, and alcohol consumption. Physical activity was assessed by self-reported participation in any exercise or physical activity during the past 30 days, excluding regular job-related activity. Smoking status was categorized as current smoker (every day or some days), former smoker, or never smoker. Current smokers included both daily and occasional smokers. Heavy drinking was defined as >7 drinks per week among women, whereas binge drinking was defined as consuming four or more drinks on a single occasion for women.
Statistical analysis
The data were summarized using frequencies, weighted percentages, and standard errors. All analyses accounted for the complex survey design by incorporating strata, primary sampling units, and sampling weights.
Weighted descriptive statistics were generated for all study variables. Multivariable logistic regression models were used to estimate adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for the association between hysterectomy and demographic characteristics, gynecological cancers, diabetes, BMI, and health behaviors (physical activity, smoking, binge drinking, and heavy alcohol consumption), controlling for age, race/ethnicity, marital status, education, annual household income, survey year, and area.
Linear regression models were used to estimate adjusted mean differences in the number of ACEs across demographic and clinical characteristics. Separate multivariable logistic regression models examined associations between hysterectomy and (1) individual ACE items and (2) cumulative ACE exposure, adjusting for demographic, clinical, and behavioral covariates.
Model significance was assessed using type III tests of effects. Statistical significance was determined using two-sided tests with a threshold of p < 0.05, and 95% CIs that excluded 1 were considered statistically significant. All analyses were conducted using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
The distribution of participants across demographic characteristics is shown in Table 1. Most were aged ≥45 years, non-Hispanic White, married or cohabiting, had some college education or a college degree, and reported an annual household income of <$100,000 (USD). ACE and hysterectomy items were most frequently available in areas participating in the 2020 BRFSS. All analyses were adjusted for age, race/ethnicity, marital status, education, annual household income, survey year, and area.
Approximately 24.2% of participants had undergone a hysterectomy, and 65.8% had experienced at least one ACE. The adjusted odds of hysterectomy significantly increased with older age and were significantly more common in non-Hispanic Black women (vs. non-Hispanic White women), in previously married (vs. married/cohabiting), and those with lower levels of education and income. The adjusted mean number of ACEs significantly decreased with older age and was significantly greater among non-Hispanic White women, in those with lower education and income, and in later years. In the hysterectomy model, type III analysis of effects indicated significant associations for age (F = 322, p < 0.0001), race/ethnicity (F = 18, p < 0.0001), marital status (F = 27, p < 0.0001), education (F = 38, p < 0.0001), income (F = 3, p = 0.0169), and area (F = 20, p < 0.0001), whereas survey year was not significant (F = 1, p = 0.3386). In the ACE model, all covariates were statistically significant, including age (F = 376, p < 0.0001), race/ethnicity (F = 26, p < 0.0001), marital status (F = 23, p < 0.0001), education (F = 44, p < 0.0001), income (F = 47, p < 0.0001), area (F = 15, p < 0.0001), and survey year (F = 18, p < 0.0001).
The distribution of gynecological cancers, diabetes, obesity, and health-risk behaviors is presented in Table 2. Gynecological cancers were relatively rare, whereas diabetes, obesity, and health-risk behaviors were more prevalent. Adjusted odds of hysterectomy were highest among participants with gynecological cancers, particularly uterine cancer. Higher adjusted odds were also observed among individuals with diabetes, obesity, no physical activity, and former smoking. In contrast, binge drinking and heavy alcohol consumption were associated with lower adjusted odds of hysterectomy.
Hysterectomy and Adverse Childhood Experiences (ACEs) According to Selected Health Conditions and Health-Risk Behaviors Among U.S. Women
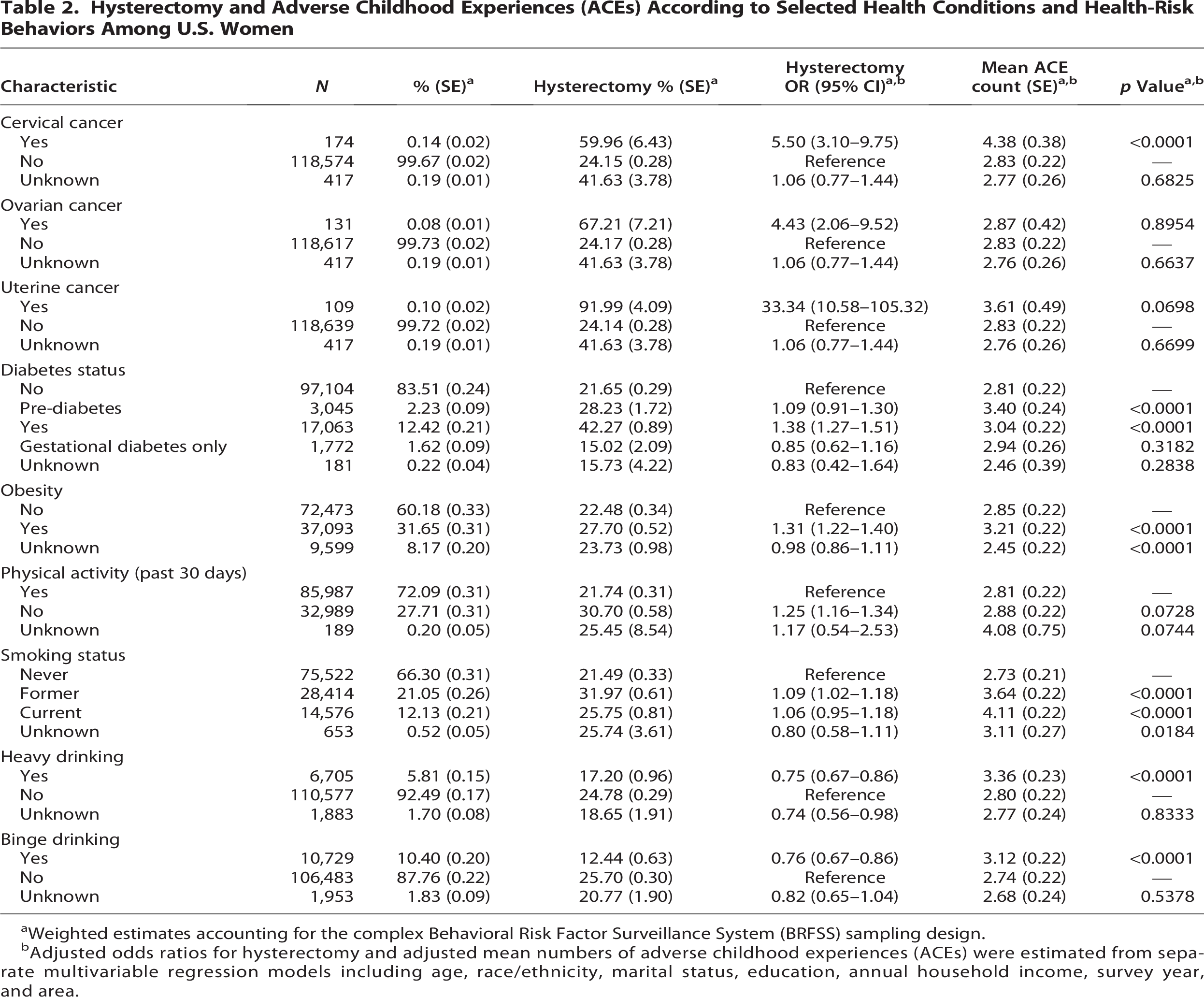
Weighted estimates accounting for the complex Behavioral Risk Factor Surveillance System (BRFSS) sampling design.
Adjusted odds ratios for hysterectomy and adjusted mean numbers of adverse childhood experiences (ACEs) were estimated from separate multivariable regression models including age, race/ethnicity, marital status, education, annual household income, survey year, and area.
The adjusted mean number of ACEs was significantly higher among participants with cervical cancer, diabetes or prediabetes, obesity, current or former smoking, and both binge drinking and heavy alcohol consumption.
The distribution of participants across each ACE is shown in Table 3, and prevalence estimates are presented in Figure 1. The most common ACEs were verbal abuse by a household adult (being sworn at, insulted, or put down) and parental separation or divorce (including parents not married), whereas the least common were household incarceration and forced sexual intercourse by an adult or someone at least 5 years older.
Individual Adverse Childhood Experience (ACE) Items and Hysterectomy Among U.S. Women
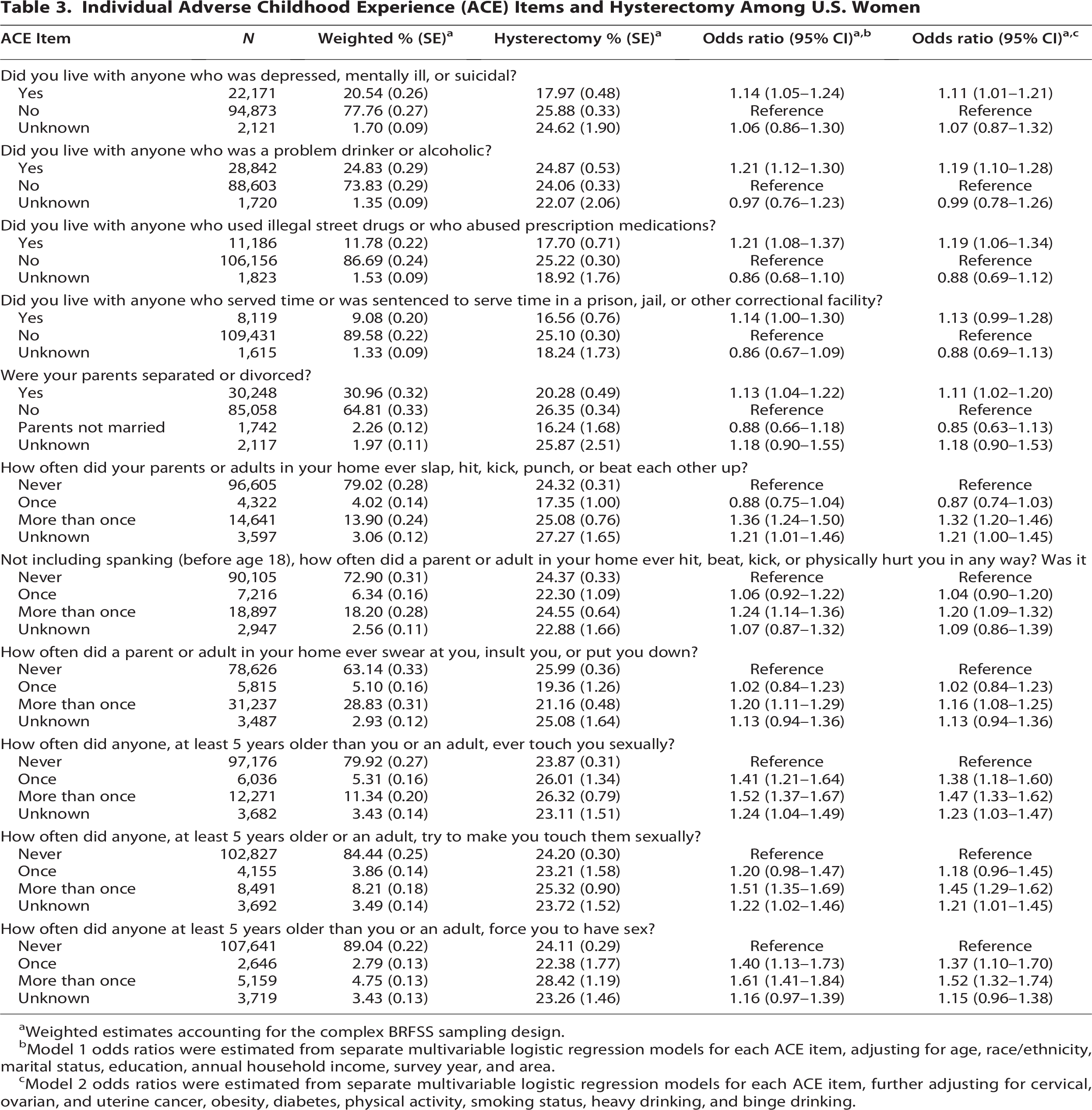
Weighted estimates accounting for the complex BRFSS sampling design.
Model 1 odds ratios were estimated from separate multivariable logistic regression models for each ACE item, adjusting for age, race/ethnicity, marital status, education, annual household income, survey year, and area.
Model 2 odds ratios were estimated from separate multivariable logistic regression models for each ACE item, further adjusting for cervical, ovarian, and uterine cancer, obesity, diabetes, physical activity, smoking status, heavy drinking, and binge drinking.
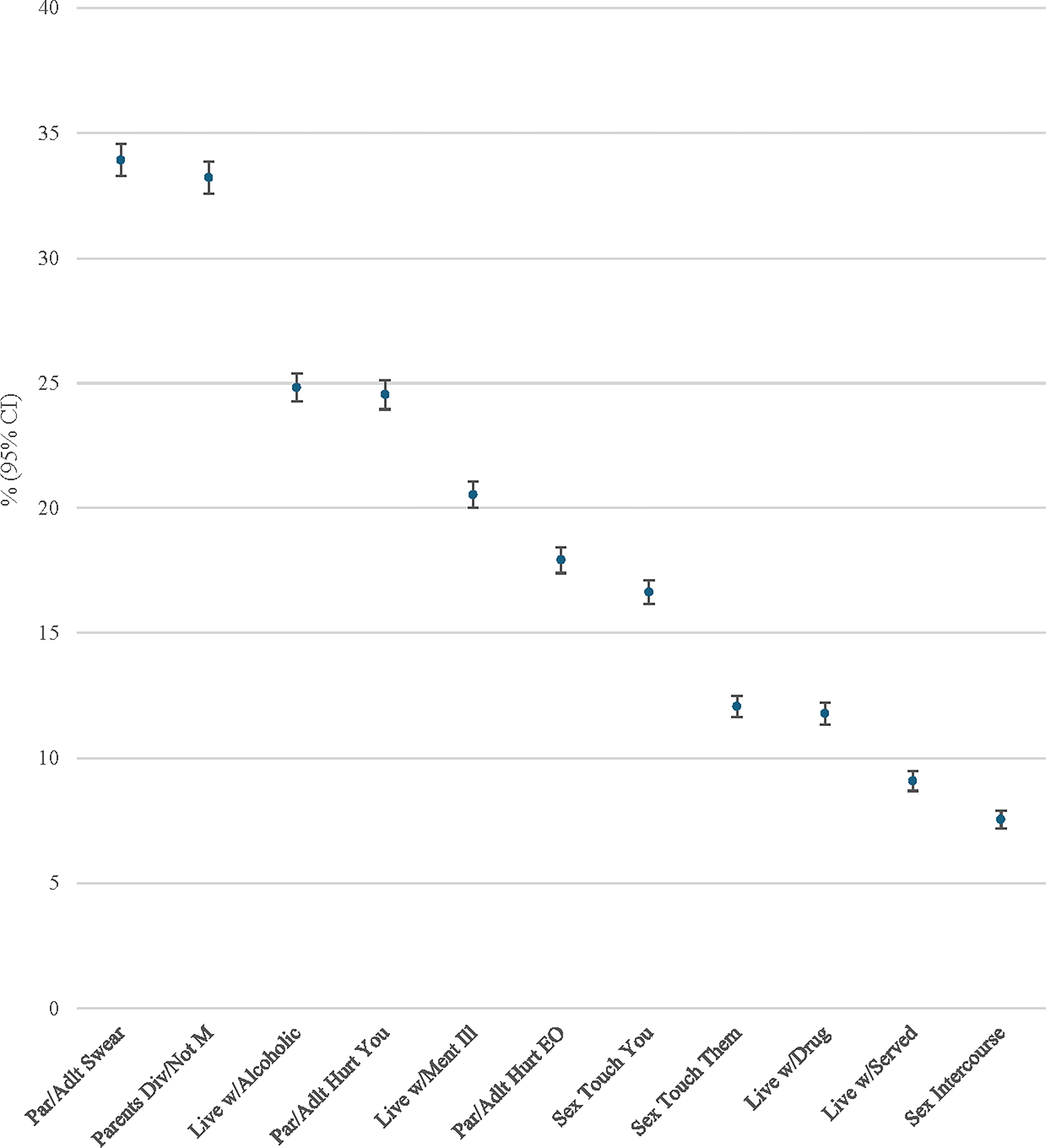
Prevalence of specific adverse childhood experiences (ACEs) among U.S. women. Data source: Behavioral Risk Factor Surveillance System (BRFSS), 2020, 2021, 2022, and 2024. CI, confidence interval. Weighted estimates based on the complex sampling design.
Two multivariable logistic regression models were used to examine the associations between each ACE and hysterectomy. Model 1 adjusted for age, race/ethnicity, marital status, education, annual household income, survey year, and area. Model 2 further adjusted for gynecological cancers (cervical, ovarian, and uterine), obesity, diabetes, physical activity, smoking status, heavy drinking, and binge drinking. Across ACE items, most exposures were associated with higher odds of hysterectomy compared with no exposure, with the strongest and most consistent associations observed for sexual abuse-related ACEs, including unwanted sexual touching, attempted sexual coercion, and forced sexual intercourse. Additional adjustments for gynecological cancers, diabetes, obesity, and health-risk behaviors had little impact on effect estimates (Table 3; Fig. 2).
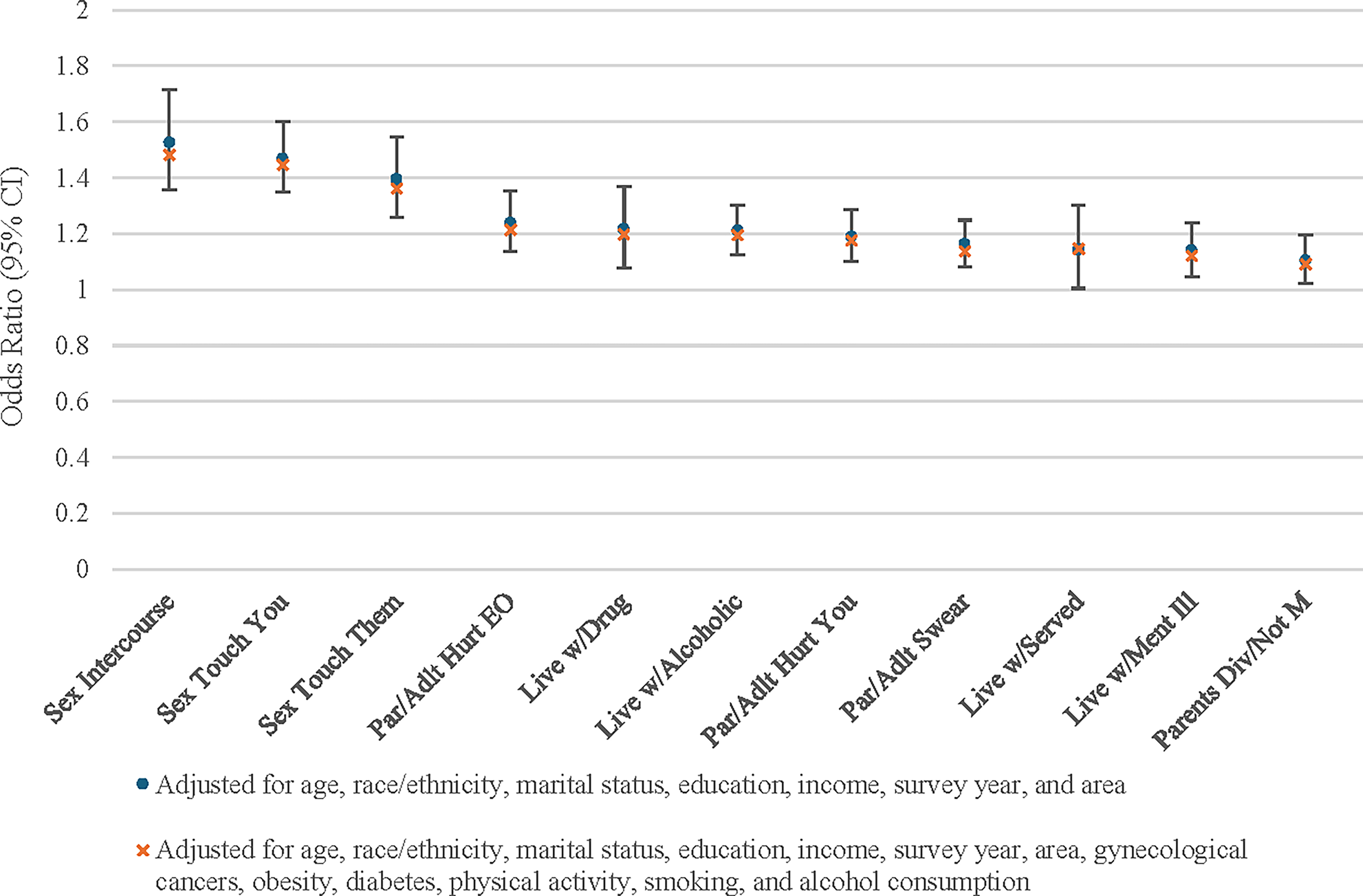
Odds of hysterectomy according to specific ACEs and level of adjustment. Data source: Behavioral Risk Factor Surveillance System (BRFSS), 2020, 2021, 2022, and 2024. CI, confidence interval. Weighted estimates based on the complex sampling design.
Among participants, 34.2% reported 0 ACEs, 33.5% reported 1–2 ACEs, 15.5% reported 3–4 ACEs, and 16.9% reported ≥5 ACEs. Odds ratios for hysterectomy by ACE category are presented in Figure 3. The odds of hysterectomy increased in a dose–response manner with higher ACE exposure after adjustment for demographic covariates. Significantly elevated odds were observed beginning at ≥3 ACEs compared with no ACEs. Additional adjustment for selected diseases, obesity, and health-risk behaviors had minimal impact on effect estimates. The association between cumulative ACE exposure and hysterectomy did not vary significantly by age (p = 0.2464).
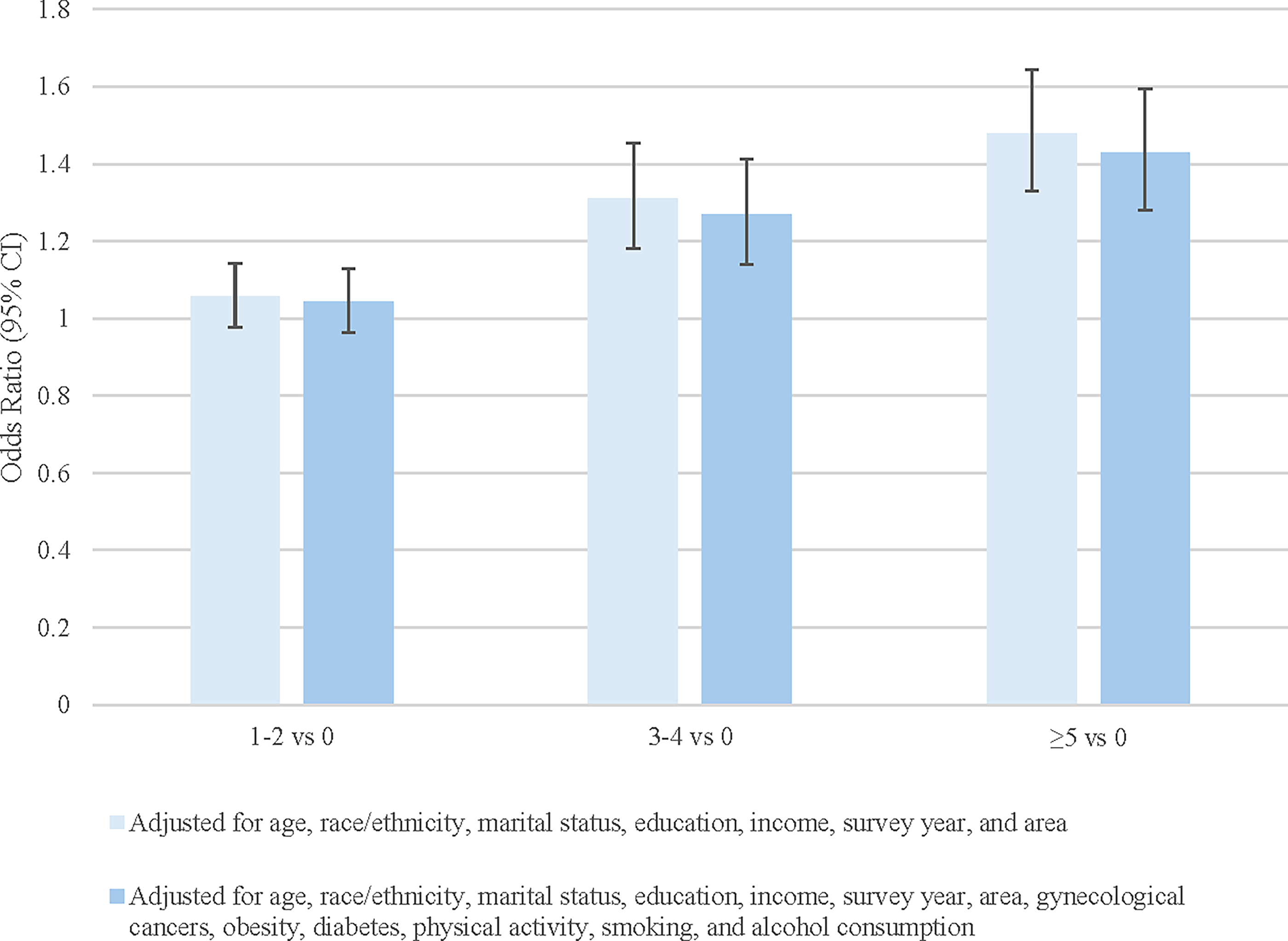
Odds of hysterectomy by number of ACEs. Data source: Behavioral Risk Factor Surveillance System (BRFSS), 2020, 2021, 2022, and 2024. CI, confidence interval. Weighted estimates based on the complex sampling design.
Type III analysis of effects was used to assess the relative contribution of predictors to the final model. Age was the strongest predictor of hysterectomy (F = 284, p < 0.0001), followed by cervical cancer (F = 39, p < 0.0001), uterine cancer (F = 34, p < 0.0001), marital status (F = 29, p < 0.0001), education (F = 26, p < 0.0001), area (F = 18, p < 0.0001), number of ACEs (F = 17, p < 0.0001), race/ethnicity (F = 17, p < 0.0001), ovarian cancer (F = 16, p < 0.0001), obesity (F = 13, p < 0.0001), physical activity (F = 9, p < 0.0001), diabetes (F = 8, p < 0.0001), and binge drinking (F = 5, p = 0.0085). Heavy drinking (F = 3, p = 0.0573), survey year (F = 2, p = 0.0716), income (F = 1, p = 0.4277), and smoking status (F = 1, p = 0.3996) were not statistically significant in the final model. Figure 3 shows a similar ordering of predictor importance. Interaction terms between ACE count and age and between ACE count and race/ethnicity were not statistically significant; therefore, stratified analyses were not conducted.
Discussion
This nationally representative study of U.S. women found that ACEs are consistently associated with higher odds of hysterectomy in adulthood, even after adjustment for a wide range of covariates. Both individual ACE domains and cumulative ACE exposure demonstrated significant associations, with the strongest effects observed for childhood sexual abuse-related experiences. A clear dose–response relationship was also observed, with increasing ACE burden corresponding to progressively higher odds of hysterectomy. These associations persisted after adjustment for age, race/ethnicity, marital status, education, annual household income, survey year, and geographic area, as well as clinical and behavioral factors including cervical, ovarian, and uterine cancers, diabetes, obesity, physical activity, smoking status, heavy alcohol consumption, and binge drinking. These findings extend prior research by evaluating specific ACE categories in a large, multi-year U.S. sample spanning both younger and older women while incorporating a broader set of gynecological and metabolic covariates than have been included in earlier studies.
Adjustment for these covariates did not attenuate the associations between individual ACE items and hysterectomy or the graded relationship with cumulative ACE exposure. Similarly, prior studies have reported that the dose–response association between ACEs and hysterectomy persists after adjustment for socioeconomic, reproductive, and behavioral factors, including childhood and adult socioeconomic status, birth cohort, age at menarche, marital status, smoking history, and parity. 13 Comparable findings have also been reported for oophorectomy, with associations remaining significant after multivariable adjustment. 14 The present study extends this literature by demonstrating that the association between cumulative ACE exposure and hysterectomy does not significantly differ by age or race/ethnicity among U.S. women.
The current study found significant associations between all but one of the ACE items and hysterectomy after adjustment for covariates. A prior study of premenopausal women reported a positive association between childhood sexual assault involving vaginal penetration and adult hysterectomy; however, that study did not examine other categories of adverse childhood experiences. 15 In the present study, the strongest associations were observed for sexual abuse-related ACEs, including unwanted sexual touching and forced sexual intercourse, whereas the weakest associations were observed for household disruption and psychosocial stressors, such as living with a parent who was mentally ill or suicidal, parental separation or divorce, and parental unmarried status.
Hysterectomy may be performed for various clinical reasons. Although adjustment for demographic, clinical, and behavioral covariates did not attenuate the association between ACEs and hysterectomy, unmeasured factors may contribute to this relationship. In particular, uterine fibroids and endometriosis—both of which have been associated with ACE exposure—are common indications for hysterectomy and may partially explain the observed associations.9,10,13,23 However, some researchers have suggested that the association between childhood abuse and fibroid development may be influenced by detection bias, as women with abuse histories may be more likely to undergo diagnostic imaging, such as ultrasound; alternatively, stress-related pathways have been proposed as a more direct etiologic mechanism.24,25 Despite this, a recent systematic review reported that both childhood sexual and physical abuse are associated with an increased risk of fibroids and endometriosis. 3 One proposed biological mechanism is that chronic stress resulting from abuse may dysregulate immune function and increase systemic inflammation, thereby elevating the risk for gynecological disease.9,10,26
Prior work has also suggested that ACE-related epigenetic changes, chronic low-grade inflammation, obesity, and health-risk behaviors may contribute to these associations. 13 However, in the present study, adjustment for obesity and behavioral factors did not materially alter the observed relationships, suggesting that these pathways do not fully explain the association. ACE-related chronic stress and subsequent neuroendocrine and immune dysregulation remain plausible mechanisms warranting further investigation. 13 An inverse association between hysterectomy and both binge drinking and heavy alcohol consumption was also observed; however, this finding is unlikely to reflect a protective effect and may instead be explained by reverse causation, residual confounding (including age and comorbid conditions), or changes in health behaviors following the diagnosis or treatment of gynecological conditions.
A related study of oophorectomy proposed a dual-pathway explanation involving both stress-related biological mechanisms and psychodynamic or behavioral factors. 14 In that study, 20.3% of women undergoing surgery were reported to have no identifiable ovarian or uterine pathology but reported clinically significant symptoms that warranted evaluation. Although few participants explicitly linked their symptoms to past trauma, the authors suggested that the perception that removal of reproductive organs could alleviate distress may influence surgical decision-making in some cases. 14 Further research is needed to better understand patient perceptions and decision-making processes regarding hysterectomy, particularly in relation to histories of childhood adversity.
Limitations
This study used BRFSS data, which are cross-sectional and involve individuals aged ≥18 years. Recalling information about adverse experiences from their childhood may introduce some bias due to the long time elapsed since childhood, particularly among older participants. Some individuals may suppress, and others may exaggerate, reports of ACEs. We cannot determine the accuracy of the responses, but the anonymous nature of the survey is assumed to minimize bias. Furthermore, we were unable to assess mediating effects because of the cross-sectional nature or the data. In addition, not all U.S. states, the District of Columbia, and territories provided information on ACEs and hysterectomy. However, by combining 4 years of BRFSS data which do collect this information, a large representation of U.S. areas was included in the study. While the area’s decision to ask questions about ACEs or hysterectomy may influence the results, area is adjusted for in the analyses. Finally, it is possible that the prevalence of hysterectomy may have been affected by the COVID-19 pandemic. However, the estimated prevalence of hysterectomy did not significantly vary across the study years.
Conclusion
This study found significant positive associations between several individual ACE items and hysterectomy, as well as between the number of ACEs and the prevalence of hysterectomy, after adjustment for demographic, disease, obesity, and health-risk behaviors. Sexual abuse-related ACEs, particularly forces sexual intercourse, demonstrated the strongest associatons with hyterectomy. This study expanded prior studies by analyzing a larger and more recent set of data and by considering more disease and health-risk behavior covariates. However, as in previous research, these covariates failed to explain the association between ACEs and hysterectomy. In addition, the association between the number of ACEs and hysterectomy does not depend on age or race/ethnicity. Because childhood sexual abuse showed the strongest observed associations with hysterectomy, further research is warranted to understand potential causal pathways and long-term gynecological consequences.
Authors’ Contributions
R.M.M.: Conceptualization, data curation, formal analysis; investigation, methodology, software, validation, visualization, writing—original draft, and writing—review and editing; K.C.C.: Conceptualization, visualization, writing—original draft, and writing—review and editing.
Footnotes
Acknowledgments
The authors wish to thank Dr. Eric Huish, DO, FACOG, for his valuable suggestions on the article.
Ethical Considerations
This study was deemed exempt from human subjects review by the authors’ institutional review board (IRB) because the Behavioral Risk Factor Surveillance System (BRFSS) data are publicly available and deidentified. The research was conducted in accordance with the ethical principles of the Declaration of Helsinki, as established by the World Medical Association for medical research involving human participants.
Consent to Participate
Participation in BRFSS is voluntary, and verbally informed consent is obtained at the time of survey administration.
Data Availability
The datasets analyzed during the current study are publicly available from the Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System (BRFSS) website.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.