
Abstract
Background:
Although atherosclerotic cardiovascular disease (ASCVD) is the leading cause of death in men and women, there are sex differences in its prevalence and burden. There is limited time to address preventive counseling during in-person office visits. We propose an innovative health care delivery strategy with telehealth group counseling to improve care for women with ASCVD.
Methods:
After institutional review board approval, physicians screened our cardiology practice, and eligible patients were contacted. Women of ≥18 years of age were included, and 13 consented. Group counseling was performed via Zoom in one to five sessions over 12 weeks. Each 60-minute session discussed a secondary prevention topic. Surveys were administered before and after each session. Effectiveness was assessed using unpaired t-tests and qualitative feedback.
Results:
The average participant age was 64.5 years. 69.2% of patients were White, while 30.8% were non-White. Hypertension and hyperlipidemia were present in 53.8% and 100% of participants, respectively. 53.8% had Medicare, 7.7% had Medicaid, and 38.5% had commercial insurance. Sessions averaged 7 participants per session, with an average attendance of 2.7 sessions per person. Pre- and postintervention comparisons showed improvement in ease of receiving answers to questions, feeling rushed, and understanding of cardiac problems, though results did not reach statistical significance. Feedback noted satisfaction with format, quality of information, and accessible communication of topics.
Conclusion:
Telemedicine group health counseling enhanced patient understanding of cardiac problems. However, significance was limited by size. Telemedicine provides an opportunity to optimize preventive care, highlighting the need for larger studies and correlation with clinical outcomes.
Keywords
Introduction
Despite improved recognition of sex-specific risk factors and presentations, ischemic heart disease remains the leading cause of morbidity and mortality in women in the United States. 1 Although atherosclerotic cardiovascular disease (ASCVD) is the leading cause of death in both men and women in the United States, there are significant sex differences in the prevalence and burden of ASCVD. Notably, female patients have higher absolute numbers of deaths caused by ASCVD, including heart disease and stroke, than their male counterparts. 2 Despite the clear morbidity and mortality benefits of aspirin and statins for the secondary prevention management of ASCVD, women with ASCVD had lower use of these medications, further contributing to poorer outcomes, including more ED visits and hospitalizations per year. 3 Women are less likely to have their blood pressure at goal when compared with men, which may contribute to a higher risk of fatal and nonfatal cardiac events and death. 4 This may be in related part to prescriber practices, as well as to medication use. 4 When compared with men, women with ASCVD are more likely to experience poorer patient-provider communication, lower health care satisfaction, poorer perception of health status, and lower health-related quality-of-life scores. 3 Numerous studies have highlighted this gender disparity, and these findings have important public health consequences. We have key opportunities to design innovative approaches to reduce these disparities.
We propose an innovative health care delivery strategy with telehealth group counseling sessions to improve engagement, adherence, and, ultimately, outcomes in women. Telehealth, often used interchangeably with the term telemedicine, is a valuable option to both patients and physicians as an alternative to the standard office visit. It is a rapidly growing part of health care, due largely in part to its convenience, as well as the increased access to care it provides. 5 Due to the coronavirus disease 2019 (COVID-19) pandemic, telehealth has become even more of an accessible and acceptable form of health care delivery. Telemedicine has been shown to allow for better long-term management and patient satisfaction by enhancing follow-up care and increasing convenience for both patients and providers. 6 Metrics for telehealth quality assessment include patient experience and satisfaction, effectiveness, financial impact and cost, and access to care and information. 7
A group counseling session via telehealth would provide an opportunity for physicians to effectively counsel patients on select topics with adequate time allotted to each topic, ultimately improving patient satisfaction and intended medication use. In this study, we aim to utilize an innovative health care delivery strategy via telehealth group counseling sessions to improve engagement, adherence, and ultimately outcomes in female patients with ASCVD.
Materials and Methods
Data source and study population
After institutional review board (IRB) approval, physicians screened our cardiology practice via the electronic medical record, and eligible patients were contacted. Women of ≥18 years of age with ASCVD as defined by prior myocardial infarction (MI) (non-ST elevation myocardial infarction, ST elevation myocardial infarction, unstable angina, and acute coronary syndrome), asymptomatic (coronary atherosclerosis [CAD], coronary calcification, or microvascular disease without associated symptoms), or chest pain or angina due to underlying CAD, were included. Women with risk factors for ASCVD (e.g., hypertension [HTN], hyperlipidemia [HLD], and diabetes mellitus [DM]), but no known ASCVD, were excluded.
This study was conducted as a pilot effort, and screening was performed from a subset of patients seen by select providers within the cardiology practice, rather than from the entire practice population. Select providers were clinical cardiologists who were willing to permit the study team to approach and consent their patients for participation. In total, approximately 500 patient charts were reviewed for eligibility. Of these, an estimated 100 patients fulfilled inclusion criteria and did not meet any exclusion criteria. Recruitment was not limited by a prespecified enrollment cap, and eligible participants self-selected to participate in sessions based on interest in the topic and comfort with the technical modality provided.
Thirteen patients consented to participate. Given the pragmatic nature of the screening process, exact counts at each stage were not systematically recorded. Therefore, reported values represent approximate estimates. A Preferred Reporting Items for Systematic Reviews and Meta-Analyse flow diagram is provided to demonstrate the screening, eligibility, and enrollment process (Fig. 1). Each participant was asked to sign an IRB-approved confidentiality agreement, which included acknowledgment of the telehealth platform, prohibition of recording, and acknowledgment that patient names would be visible to other participants but that each session was confidential.
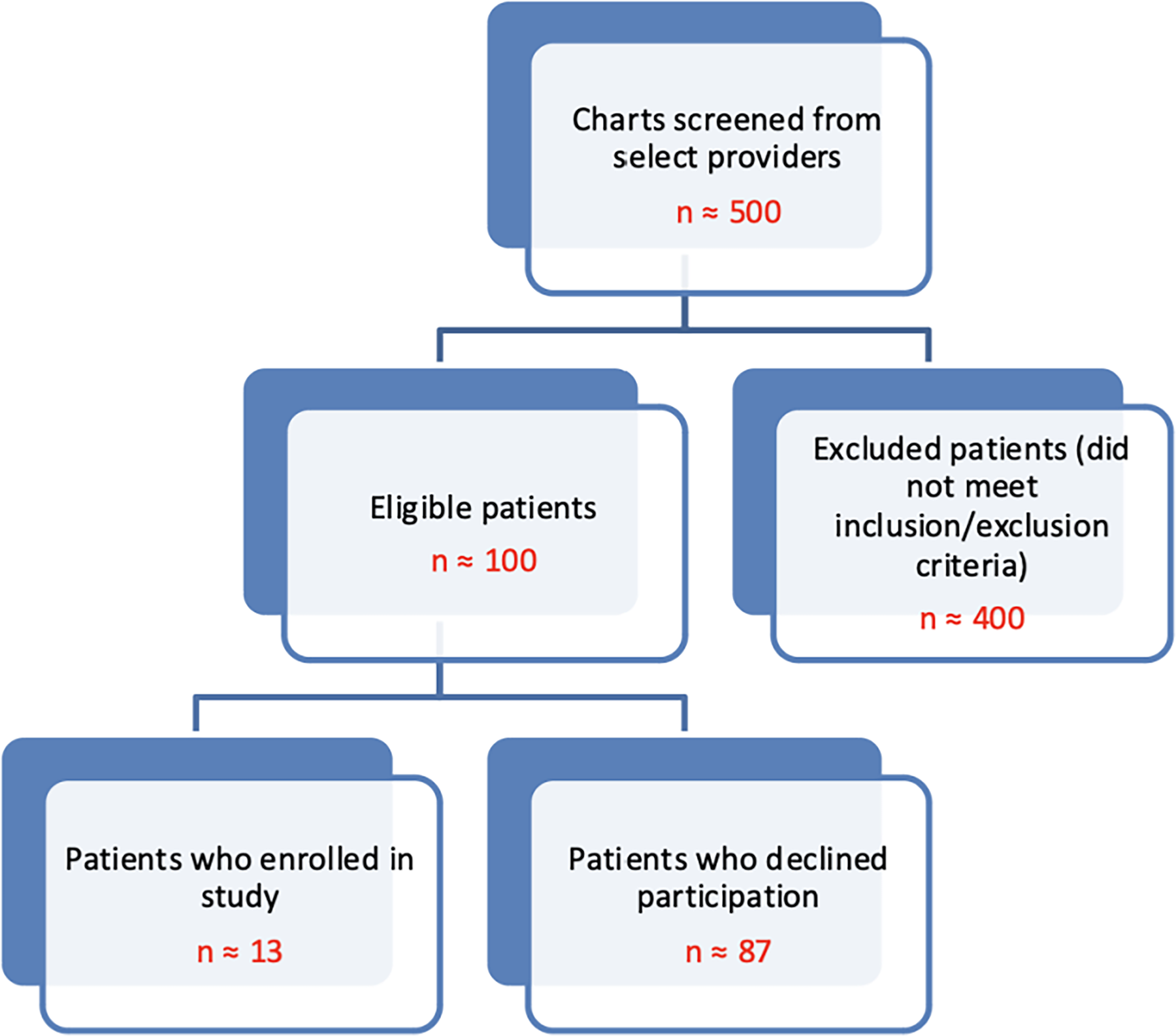
Screening process.
Study variables and endpoints
Once consent was obtained, baseline characteristics of participants were collected via chart review, including demographics such as age, race, insurance carrier, and clinician-documented diagnoses, such as ASCVD, HTN, HLD, and DM.
Group counseling was performed via Zoom and was led by a cardiologist at the practice. Participants had the option to participate in —one to five sessions over 12 weeks, depending on their preference. Each session was 60 minutes in duration and discussed a secondary prevention topic, such as an overview ASCVD, HTN, HLD, chest pain, and the effects of stress on the heart. Approximately 15 minutes were reserved at the end of each session for a question-and-answer-style discussion with the cardiologist.
Surveys were given to participants both before and after each session. The presession survey asked patients about their demographics, self-reported diagnoses, current level of satisfaction about their understanding of their diagnoses, reasons for participating in the study, and history of previous participation in telehealth group counseling. The postsession survey was aimed at assessing patient understanding, including diagnoses and medications, satisfaction with the format, satisfaction with the provider, how many sessions were attended, reasons for attending more than one session, and recommendation of this format to others. All data was de-identified prior to analysis.
Statistical analysis
Effectiveness was assessed by comparing responses pre- and postintervention with unpaired t-test analysis and through qualitative written feedback.
Results
The average participant age was 64.5 years old. 69.2% of patients were White, while 30.8% were non-White. The prevalence of hypertension, hyperlipidemia, history of prior MI, and asymptomatic coronary artery disease was 53.8%, 100%, 31%, and 69%, respectively. 53.8% had Medicare insurance, 7.7% had Medicaid insurance, and 38.5% had commercial insurance. There was an average of 7 participants per session, and each participant attended an average of 2.7 sessions (Table 1). Comparison of pre- and postintervention results showed improvement in ease of receiving answers to questions, feeling rushed, and understanding of cardiac problems. However, these results did not reach statistical significance (Fig. 2). Written feedback included satisfaction with ease of format, quality of information, and accessible communication of challenging topics.
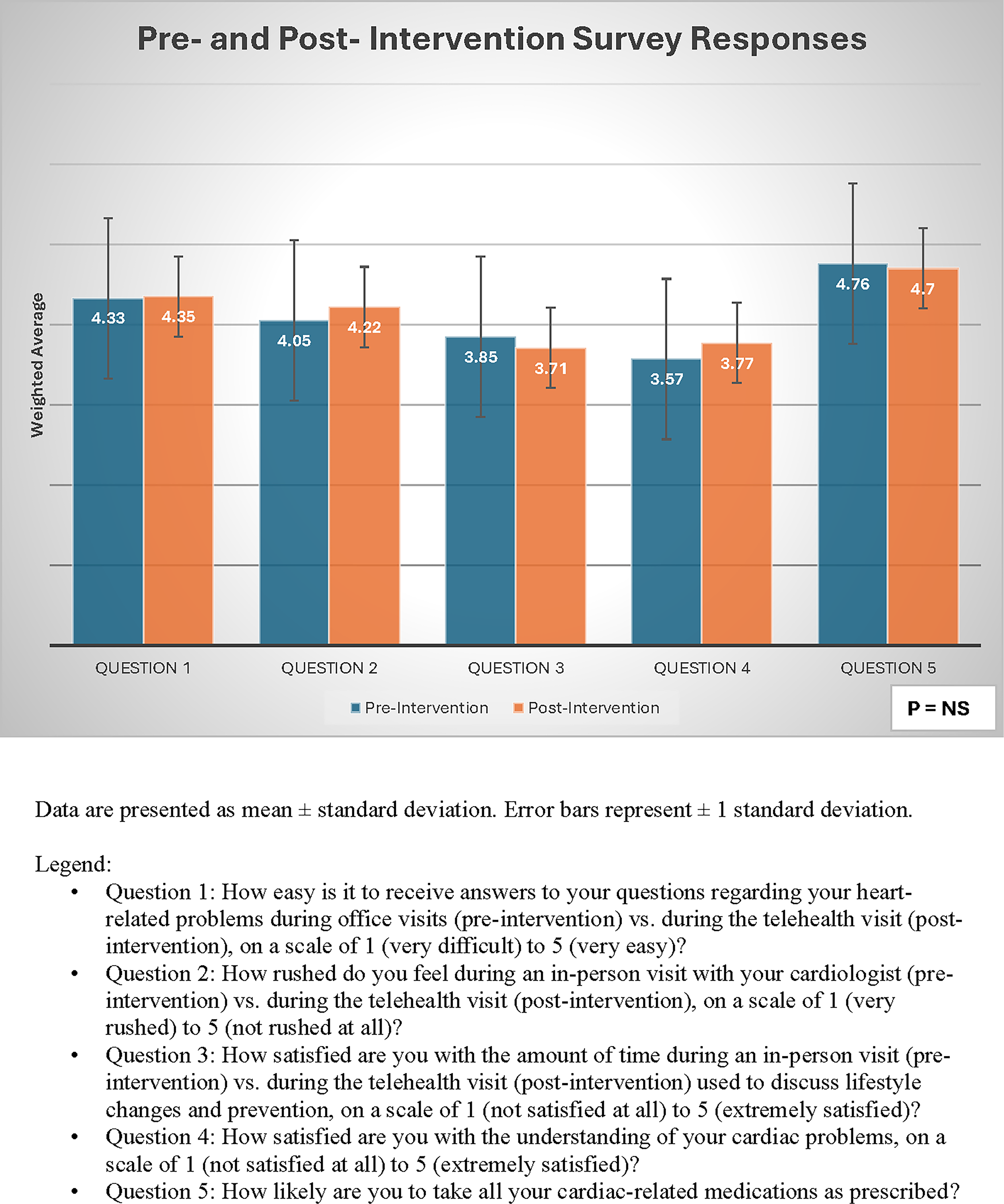
Pre- and Post- Intervention survey responses.
Demographics of Study Participants
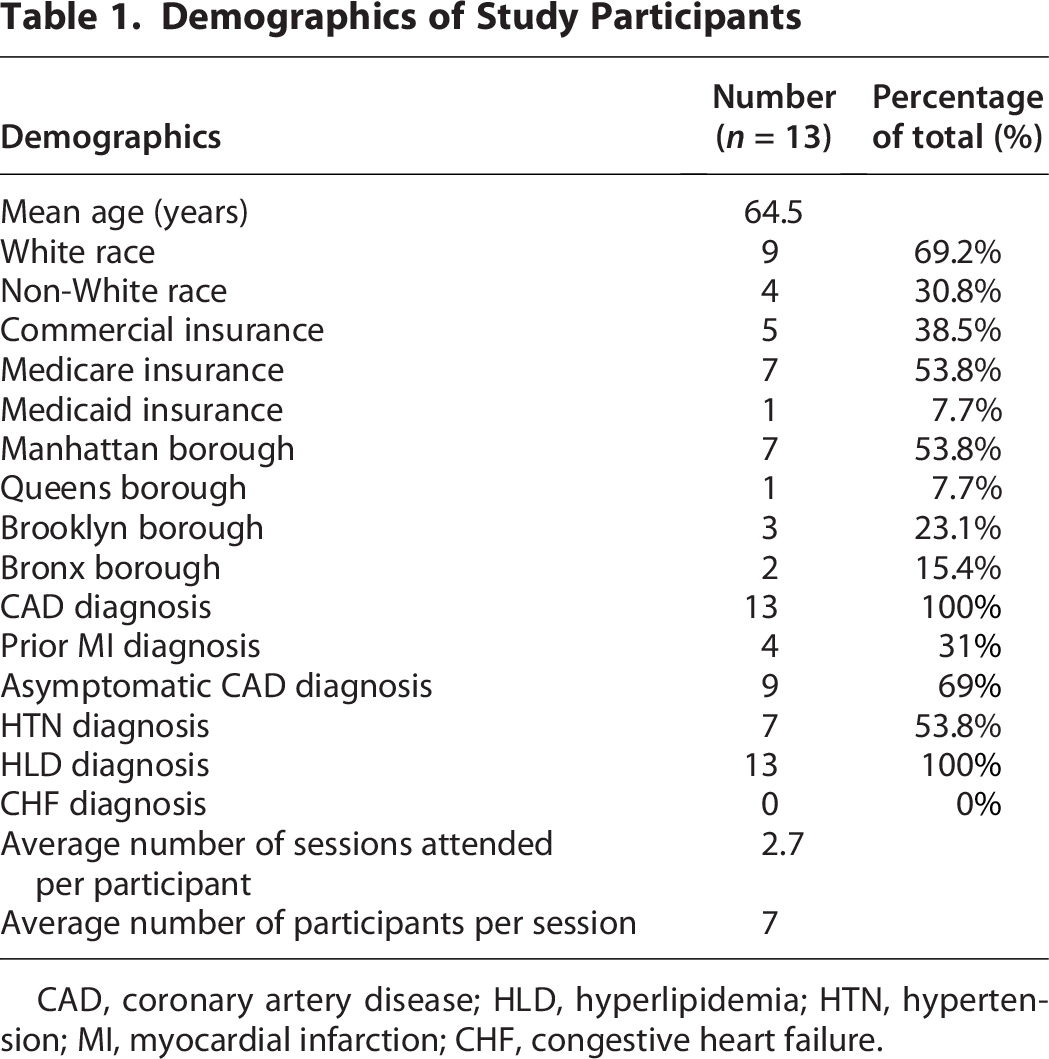
CAD, coronary artery disease; HLD, hyperlipidemia; HTN, hypertension; MI, myocardial infarction; CHF, congestive heart failure.
Figure 2 demonstrates that survey responses were generally favorable at baseline, with most preintervention weighted averages ranging between 3.5 and 4.8 on a 5-point scale. Postintervention responses showed improvements in multiple domains, including question 1, which measured participants’ perceived ease of receiving answers to heart-related questions during telehealth sessions compared with traditional visits; question 2, which measured feeling rushed during physician encounters; and question 4, which measured satisfaction with understanding of cardiac problems. This was consistent with the written feedback, highlighting the accessibility and clarity of counseling topics. The pre- and postintervention score improvements did not reach statistical significance.
Satisfaction with time spent discussing lifestyle modification and prevention (question 3) remained high in both the pre- and postintervention surveys without a significant change. Finally, participants noted a high likelihood of taking cardiac medications as prescribed in both the pre- and postintervention surveys, which indicates a strong baseline adherence and could suggest a ceiling effect that may limit measurable improvement in this cohort.
Discussion
In this pilot study, we evaluated whether a telehealth-based group counseling model could improve the process and delivery of secondary preventive care for women with established ASCVD. Although the sample size was small, several important conclusions emerged.
Women with ASCVD often face structural and interpersonal barriers to effective cardiovascular care, as previously mentioned. Studies have demonstrated that group visits may be an effective strategy to overcome these barriers and improve outcomes in patients with chronic health conditions.8,9 Group visits have been felt to be effective due to increased dedicated education time, shared learning opportunities through peer discussions, and increased time for patient questions in a supportive setting. Group visits may also lead to improvements in patient engagement and self-efficacy by fostering accountability and reinforcing healthy behavior change.
Participants in this study reported improvements in understanding of their cardiac conditions, reduced frequencies of feeling rushed, and greater ease in receiving answers to their questions after the intervention. Through this positive feedback received, it can be concluded that telehealth group sessions may serve as a practical and scalable approach to expand counseling time for women with ASCVD. The small improvements in this study across multiple patient-reported domains indicate that the group telehealth environment may reduce time constraints, provide an environment for female patients to ask questions comfortably in a group setting, and help foster a support system structure. The directionality of changes in multiple measured domains suggests that a larger sample may show meaningful differences. Furthermore, participants described the telehealth format as accessible, convenient, and effective for learning complex material. These observations are aligned with prior work showing that telemedicine enhances chronic disease management, patient satisfaction, and access to care, particularly among individuals facing barriers to traditional in-person visits.5,7
While we did not formally collect structured feedback from participating cardiologists regarding their experience with this intervention, two of the study cardiologists, who are both co-authors on this article, were directly involved throughout the study implementation. They reported the group telemedicine model to be a valuable and efficient means of delivering detailed, highly informative cardiovascular preventive counseling. The format allowed simultaneous care of multiple patients while remaining consistent with reimbursable group-based telehealth care models. This observation should be interpreted in the context of the absence of formal clinician-reported outcomes.
It is well known that the traditional in-person office visit comes with many limitations, including the lack of sufficient time to fully address all concerns of both the physician and the patient.10,11 In fact, the median office visit length is only 15.7 minutes and covers a median of six topics. About 5 minutes are typically spent on the longest topic, while the remaining topics each receive about 1.1 minutes.10,11 During this limited time, providers are expected to address both acute and chronic medical problems while also establishing rapport, coordinating care, and counseling on prevention. In the cardiovascular world, prevention counseling is essential. Many studies have shown that patients who receive planned teaching have improved knowledge, and in some instances, outcomes, when compared with those receiving routine care.12–15 The United States Preventive Services Task Force found that counseling interventions resulted in important improvements in cardiovascular outcomes, including reductions in blood pressure and cholesterol levels, as well as improvements in measures of adiposity. 16 There is undoubtedly a need for greater time allocated for preventive counseling, especially in female patients, given their higher rates of poorer patient-provider communication, in addition to their higher rates of morbidity and mortality when compared with their male counterparts. Various attempts to increase office visit lengths have been made but are limited due to current constraints in health care delivery.
An important consideration of this intervention is clinician time commitment. Each 60-minute telemedicine session included approximately seven participants, and patients attended an average of 2.7 sessions. However, because these sessions allow for simultaneous counseling of multiple patients within one 60-minute session, the effective clinician time per patient is substantially reduced compared with delivering equivalent counseling in individual clinic visits. Importantly, these group telemedicine encounters may be reimbursable under existing billing structures for telehealth services, depending on payer policies. This creates a potential advantage as opposed to extending individual clinic visit lengths, which would increase clinician time burden without proportionate reimbursement. Together, these factors suggest that group telemedicine counseling may represent a more efficient and potentially sustainable model for delivering longitudinal cardiovascular risk counseling to more individuals. Implementation will require assessment of clinic and health-system workflow processes, as well as regional and system-specific payor policies.
Importantly, our cohort included women across a range of ages, zip codes, and insurance types. The high engagement across sessions (average 2.7 sessions per participant) suggests that telehealth group counseling may be feasible and acceptable for a myriad of patient populations. This appears to be true even in older adults who are traditionally considered less familiar with virtual platforms. Barriers to care, such as caregiving responsibilities, affect women disproportionately; women have been shown to provide 2.2 times more unpaid family caregiving than men. 17 The virtual format may reduce barriers to care by eliminating the need for transportation and minimizing the impact on competing demands such as caregiving.
Although our sample size was limited, the positive feedback from patients may suggest that the telehealth model of care could eventually support improved health equity while reducing the disproportionate burden of cardiovascular morbidity and mortality of women. Prior research demonstrates that planned and dedicated teaching improves cardiovascular knowledge and can improve clinical outcomes.7–11 Structured telehealth sessions can be tailored to specific topics and questions in a given patient population, which could ultimately increase medication adherence and improve lifestyle modification and eventually reduce overall morbidity and mortality. The COVID-19 pandemic accelerated and normalized the practice of telemedicine in health care systems because of its flexible care delivery model. As telehealth continues to integrate within clinical practice beyond the pandemic, virtual group counseling may represent a sustainable approach to improving preventive cardiovascular care for women.
Strengths and limitations
This study is among the first to explore telehealth group counseling specifically for women with ASCVD. The mixed-methods design and inclusion of written qualitative feedback strengthen the interpretation of our findings.
Several limitations should be acknowledged. The sample size was small and underpowered to detect statistically significant differences. Participation varied, with patients choosing how many sessions to attend, creating heterogeneity in exposure to the intervention. Self-reported survey data are vulnerable to response bias. All participants were drawn from a single academic center, which may limit generalizability. While baseline demographics reflected some diversity within the sampled population, the cohort consisted exclusively of insured patients, which reflects the clinic’s and institution’s referral base. No patients were uninsured, and this may limit generalizability. Additionally, surveys were administered before and after each telemedicine session to assess within-session change. This repeated-measures design introduced complexity in interpretation due to incomplete survey completion across sessions and conceptual overlap between postsession surveys from earlier visits and presession surveys from subsequent visits and may have limited the ability to demonstrate any substantial changes from presession to postsession surveys. Finally, we did not assess long-term outcomes such as sustained medication adherence, blood pressure control, or hospital admission rates.
Despite these limitations, the results support the potential role of telehealth-based group counseling as an innovative strategy to reduce disparities and augment preventive cardiovascular care for women. Larger studies should evaluate the impact of this model on clinical outcomes, cost-effectiveness, optimal session structure, and long-term adherence.
Conclusions
Telemedicine group health counseling showed enhanced patient understanding of cardiac problems. However, significance was limited by study size. Telemedicine provides a unique opportunity to optimize preventive care and requires future studies with larger sample sizes.
Authors’ Contributions
All authors were major contributors in writing this article. All authors read and approved the final article.
Ethical Considerations
This study was approved by the IRB. All procedures were conducted in accordance with ethical standards and regulations.
Consent to Participate
All participants provided written informed consent prior to participation in the study.
Consent for Publication
Written informed consent for publication of any individual data was obtained from all participants. Non-essential identifying information has been omitted. The authors retain the original consent forms, which are not submitted with this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.