
Abstract
Background:
Delirium is associated with high mortality and substantial patient distress; therefore, early identification and management are crucial. Among patients with cancer receiving palliative care, delirium is highly prevalent yet often underrecognized by attending physicians. Recently, palliative care for patients with noncancer conditions has gained attention. Nonetheless, the prevalence of delirium and the extent of physician awareness in this population remain unclear. This study aimed to clarify these aspects in noncancer patient populations to raise awareness among physicians and provide insights to improve palliative care delivery.
Methods:
We retrospectively reviewed 1540 inpatients receiving palliative care at a university hospital in Japan between January 2018 and December 2023. Psychiatric diagnoses, referral reasons, physical diagnoses, and demographic information were analyzed.
Results:
In the noncancer group, the number of annual referrals to palliative care increased during the study period (from 7 to 66). Both the cancer and noncancer groups were commonly referred for pain, dyspnea, anxiety, insomnia, and delirium. Compared with the cancer group, the noncancer group was more likely to receive a psychiatric diagnosis (45.7% vs. 57.6%) and had a higher prevalence of delirium (12.9% vs. 21.5%). In the noncancer group, the proportion of referrals citing psychiatric symptoms was higher (38.5% vs. 54.2%), whereas the frequency of delirium underrecognition was comparable to that in the cancer group (59.6% vs. 71.0%).
Conclusion:
Underrecognition of delirium in palliative care settings is a common issue in both cancer and noncancer patient populations. Enhancing physician awareness may improve palliative care quality in these populations.
Background
Delirium is an acute neuropsychiatric syndrome characterized by disturbances in consciousness, attention, and cognition, typically exhibiting diurnal variation. 1 It increases mortality, hospital stay, and patient distress.2–4
In palliative care, patients with cancer have a high incidence of delirium (27.6%–46.9%),5–8 often precipitated by multiple factors, including old age, low Palliative Performance Scale score, brain metastasis, infection, and electrolyte imbalance. 5 Despite its high prevalence, delirium in this population is frequently underrecognized by attending physicians (55.1%–76.1%)5–8 due to limited knowledge and awareness, as well as inadequate screening.9–12 Educational interventions and implementation of screening tools have been recommended for early detection and intervention,5–8 which can reduce mortality and the need for palliative sedation.3,13
Recently, there has been growing attention on palliative care for patients with noncancer conditions. The World Health Organization (WHO) clarifies that palliative care is not only for patients with cancer. 14 In Japan, reimbursement for palliative care services now includes end-stage heart failure, 15 and clinical guidelines for patients with noncancer conditions have been published. 16 However, the prevalence and recognition of delirium in this population remain unclear. Heart failure is a notable example of noncancer condition, with cardiologists reporting barriers to end-of-life psychiatric care, 17 rarely screening for psychiatric symptoms, 18 and often overlooking delirium. 19 Thus, we hypothesized that patients with noncancer conditions receiving palliative care may also have a high prevalence of delirium, which may be underrecognized by attending physicians.
Objective
To compare the prevalence and recognition of delirium between cancer and noncancer patient populations to highlight the current gap in physician awareness and emphasize its importance in effective palliative care delivery.
Methods
Design
A retrospective cohort study design was adopted.
Setting/Subjects
This study was conducted at a university hospital in Japan, in which the palliative care team—comprising palliative care physicians, psychiatrists, nurses, pharmacists, nutritionists, psychologists, and acupuncturists—provides care to patients referred by attending physicians. A survey of 1540 inpatients who received palliative care between January 1, 2018, and December 31, 2023, was conducted. All patients who received palliative care during this period were included. If the same patient was referred to palliative care multiple times during this period, each instance was counted separately, resulting in the total number of referrals analyzed. As this study aimed to comprehensively capture all palliative care cases, no specific exclusion criteria were applied.
The cancer group was defined as those whose primary reason for hospitalization and palliative care during the study period was a malignant disease, regardless of any prior history of noncancer conditions. In contrast, the noncancer group was defined as those whose primary reason for hospitalization and palliative care was a nonmalignant condition, even if they had a prior history of malignancy.
Measurements
At the study site, all patients referred to the palliative care team underwent comprehensive psychiatric assessments considering the possibility of delirium by two or more psychiatrists. Diagnoses were made based on the International Classification of Diseases, 10th Revision (ICD-10), which provides international diagnostic criteria. This means that delirium was diagnosed based on concurrent disturbances of consciousness and attention, perception, thinking, memory, psychomotor behavior, emotion, and the sleep-wake schedule. Multiple sources of information were utilized, including clinical findings at evaluation, information obtained either through direct interviews with attending physicians and nurses or from their documentation in medical records during hospitalization (including Richmond Agitation–Sedation Scale [RASS] scores 20 ), and information gathered from family members regarding the patient’s condition before admission. Final diagnoses were determined by consensus during daily conferences held by a team typically comprising five psychiatrists on working days and were clearly documented in the medical records. This team included a board-certified specialist accredited by the Japanese Society of Psychiatry and Neurology. Assessments were performed at the time of the referral and continued throughout hospitalization. Cases categorized as “Psychiatric Diagnosis Absent” included patients who could not be fully evaluated due to discharge or death shortly after the referral.
Data were collected from electronic medical records and palliative care referral forms. The referral forms included both checkboxes and free-text fields indicating the reasons for the referral. The checkboxes included items, such as “pain,” “anxiety,” and “delirium.” All personally identifiable information, such as names, addresses, and telephone numbers, was removed before analysis to ensure anonymity. Anonymized data were securely stored on a password-protected server accessible only to authorized personnel. A comprehensive database was constructed using the collected data, including psychiatric diagnoses; referral reasons provided by attending physicians; physical diagnoses; and demographic characteristics, including age, sex, disposition status, and referral department.
The primary outcome was the rate of delirium unrecognized by referring physicians; this outcome was compared between the cancer and noncancer patient cohorts. Delirium recognition was defined as cases in which the referring physician, for patients diagnosed with delirium by psychiatrists, had either (1) checked the “delirium” box or explicitly mentioned delirium in the referral form, (2) requested a psychiatric consultation for delirium alongside the palliative care referral, or (3) documented “delirium” in the medical records between admission and the diagnosis by the psychiatrists. Conversely, cases that did not meet these criteria were considered unrecognized. The rate of unrecognized delirium was calculated as the number of unrecognized cases divided by the total number of cases diagnosed with delirium.
Secondary outcomes included the prevalence of delirium in both groups, annual trends in referral numbers, demographic characteristics, reasons for referral, and distributions of psychiatric diagnoses.
Direct comparison between cancer and noncancer patient populations was limited to data from 2021 to 2023 because earlier records often lacked sufficient detail for extraction. This timeframe aligns with the increased attention toward noncancer palliative care following recent reimbursement changes and guideline publications in Japan, which is consistent with the objectives of this study. Univariate analyses were performed to compare the cancer and noncancer patient populations. Student’s t-test was used for continuous variables, while chi-square or Fisher’s exact tests were used for categorical variables, as appropriate. Categorical variables included sex, disposition status, referral department, reasons for referral, psychiatric diagnosis, rate of unrecognized delirium, and reasons for referral of unrecognized cases. When exact calculation was not feasible due to the size of the contingency table, p values were estimated using a Monte Carlo simulation with 10,000 replicates. Following a significant chi-square test outcome, residual analysis was conducted to identify the categories that accounted for the observed associations. To investigate the independent associations between cancer status and both the prevalence and recognition of delirium, multivariable logistic regression analyses were performed using psychiatric diagnosis (coded as 0 = without delirium, 1 = with delirium) and recognition of delirium by the attending physician (coded as 0 = unrecognized, 1 = recognized) as dependent variables. Independent variables included cancer status (coded as 0 = noncancer, 1 = cancer), age, and sex (coded as 0 = women, 1 = men).
To assess temporal trends in the number of palliative care referrals, the Mann–Kendall trend test was applied. Statistical significance was set at p < 0.05. All analyses were performed using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Trends in referral numbers
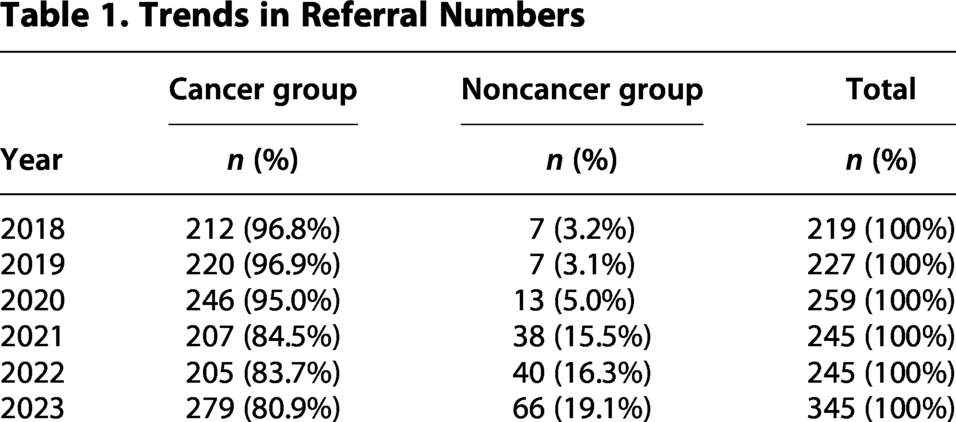
Figure 1 and Table 1 illustrate the annual referral trends from 2018 to 2023. Cancer referrals increased from a mean of 218 (2018–2022) to 279 (2023), although this trend was not statistically significant (Mann–Kendall trend test, p = 1.000). In contrast, noncancer referrals increased significantly (p = 0.013) from 7 (2018) to 66 (2023). Notably, noncancer referrals, which accounted for only 3.2% of all referrals in 2018, had increased to 19.1% by 2023.
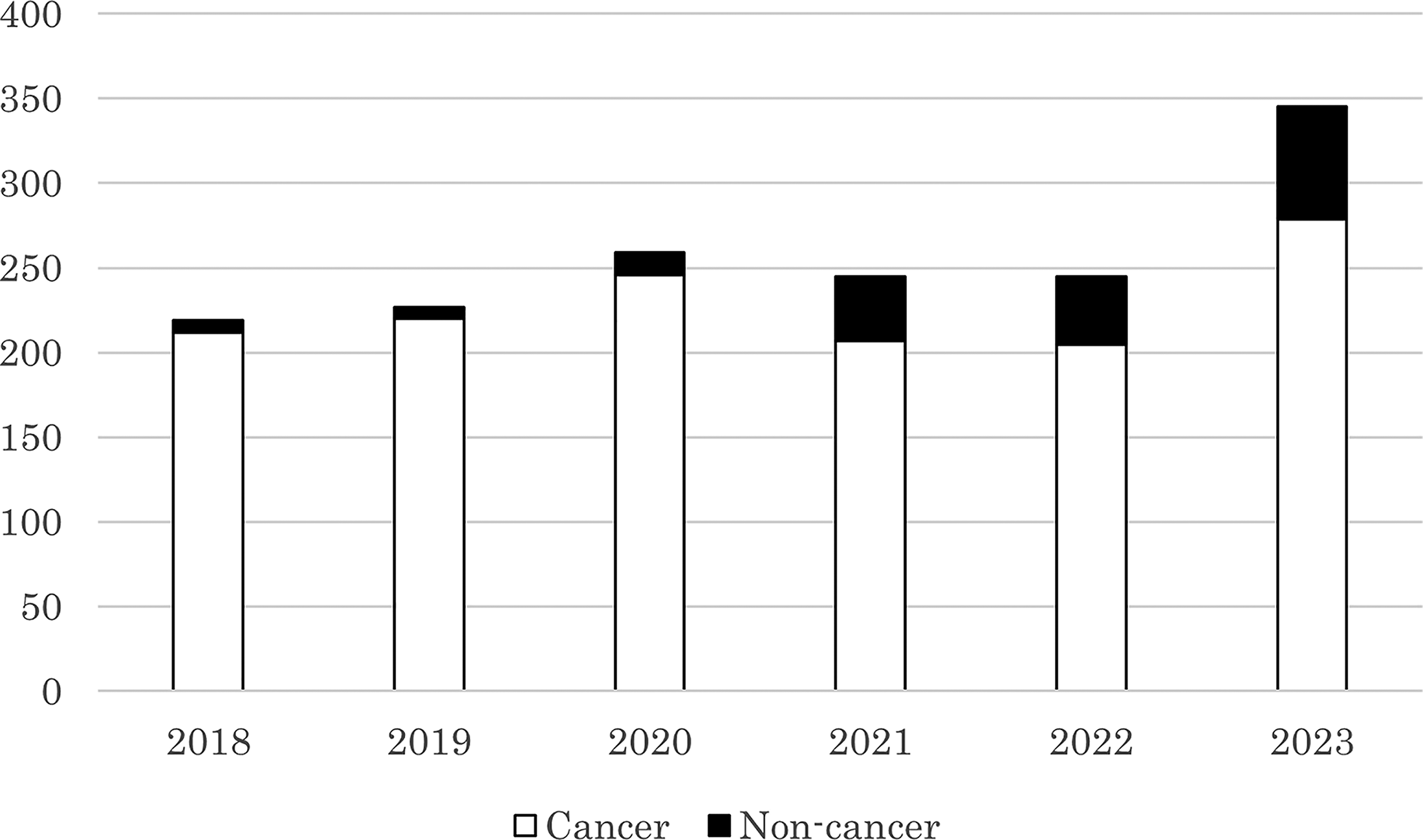
Trends in referral numbers. The stacked bars represent the annual number of referrals to the palliative care team from 2018 to 2023. The white and black segments indicate the cancer group and the noncancer group, respectively.
Trends in Referral Numbers
Clinical characteristics of referred patients (2021–2023)
The following analyses focused on patients referred between 2021 and 2023. The clinical characteristics of the cancer and noncancer groups referred during this period are summarized in Table 2.
Clinical Characteristics of Referred Patients (2021–2023)
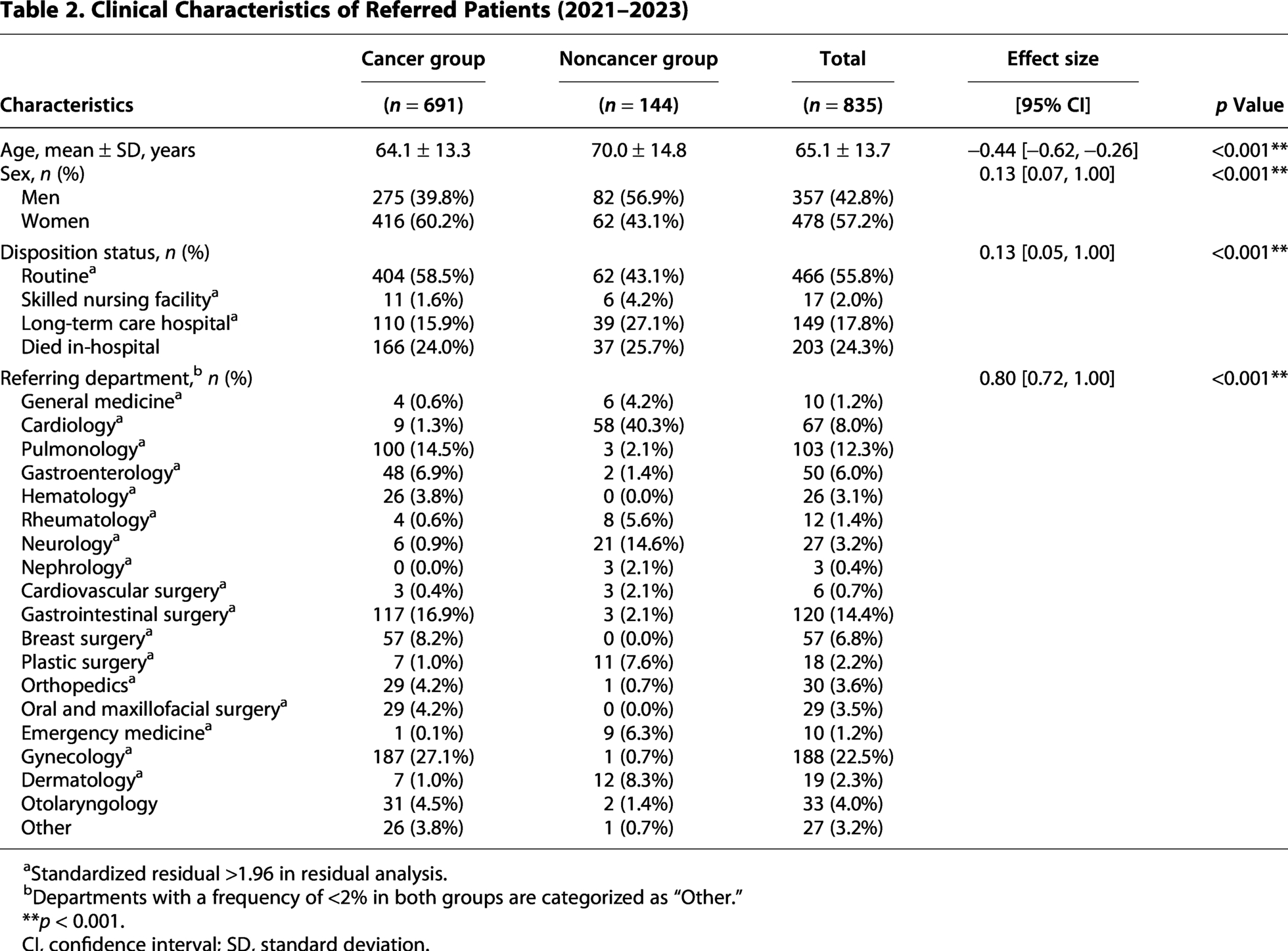
Standardized residual >1.96 in residual analysis.
Departments with a frequency of <2% in both groups are categorized as “Other.”
**p < 0.001.
CI, confidence interval; SD, standard deviation.
Compared to the cancer group, the noncancer group was significantly older (mean age: 64.1 ± 13.3 vs. 70.0 ± 14.8 years) and comprised a higher proportion of men (39.8% vs. 56.9%). Regarding disposition status, compared to the cancer group, the noncancer group was more likely to be transferred to long-term care hospitals (15.9% vs. 27.1%) or skilled nursing facilities (1.6% vs. 4.2%) and less likely to return home (58.5% vs. 43.1%). Referrals for the noncancer group came primarily from the cardiology (40.3%) and neurology (14.6%) departments.
Referral reasons and psychiatric diagnoses (2021–2023)
Table 3 provides an overview of the referral reasons and psychiatric diagnoses (2021–2023). Compared with the cancer group, the noncancer group was more often referred for reasons including psychiatric symptoms (38.5% vs. 54.2%). The five most common reasons for referral were comparable between the groups: pain (69.5% vs. 59.7%) and dyspnea (13.9% vs. 16.7%) as physical symptoms, and anxiety (22.3% vs. 22.9%), insomnia (10.6% vs. 16.0%), and delirium (5.1% vs. 8.3%) as psychiatric symptoms.
Referral Reasons and Psychiatric Diagnoses (2021–2023)
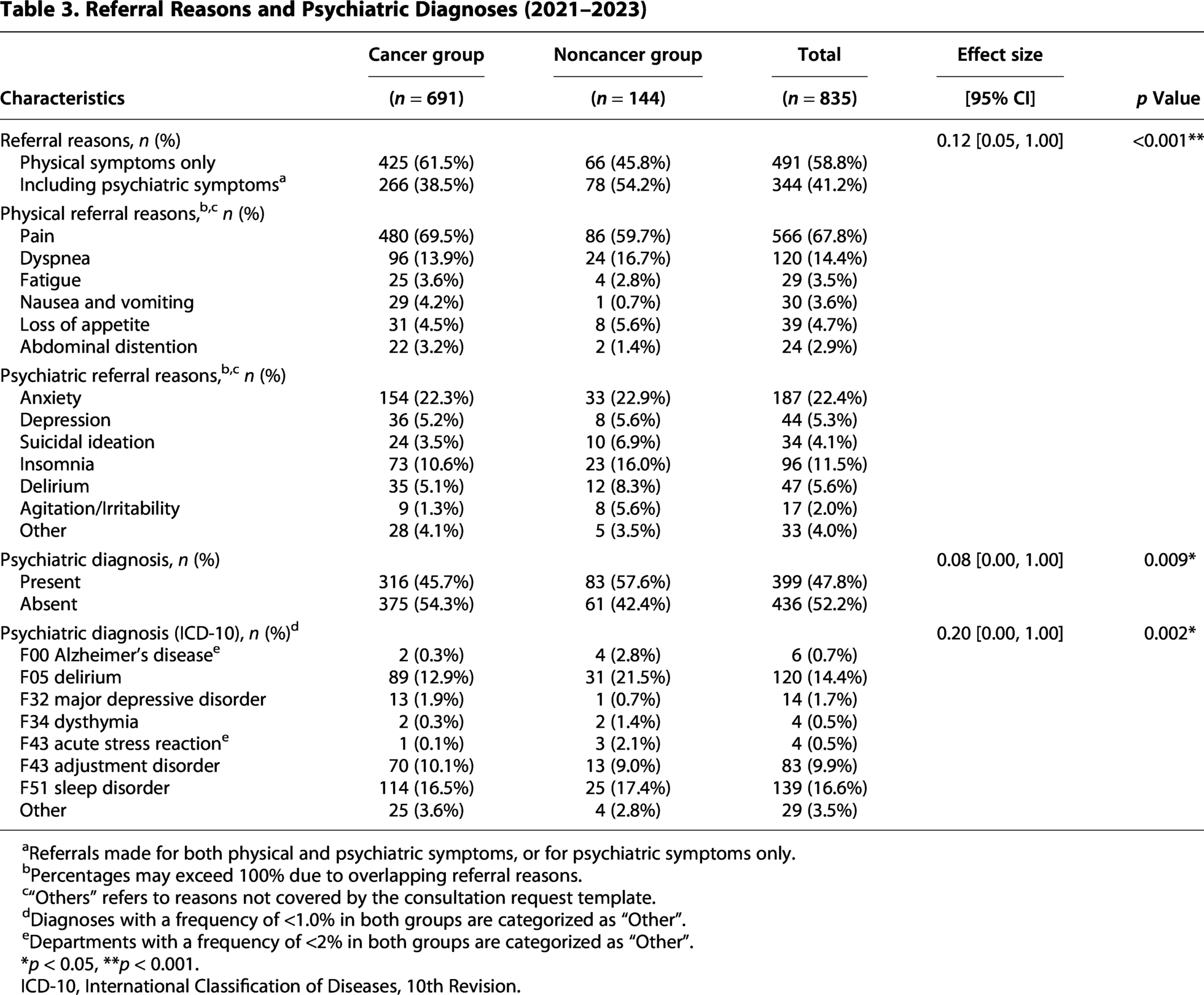
Referrals made for both physical and psychiatric symptoms, or for psychiatric symptoms only.
Percentages may exceed 100% due to overlapping referral reasons.
“Others” refers to reasons not covered by the consultation request template.
Diagnoses with a frequency of <1.0% in both groups are categorized as “Other”.
Departments with a frequency of <2% in both groups are categorized as “Other”.
*p < 0.05, **p < 0.001.
ICD-10, International Classification of Diseases, 10th Revision.
Compared with the cancer group, the noncancer group had a higher rate of psychiatric diagnoses (45.7% vs. 57.6%). Analysis of the eight diagnostic categories using the Monte Carlo method revealed a significant intergroup difference. Although residual analysis showed that delirium did not substantially contribute to this overall difference, a 2 × 2 chi-square test focusing solely on delirium identified a significant difference (12.9% vs. 21.5%, p = 0.007).
Referring physicians’ recognition and mortality of delirium (2021–2023)
The counts for each category are presented in Table 4. Among the patients diagnosed with delirium, the referring physicians did not recognize delirium in 59.6% of the cancer group and 71.0% of the noncancer group. The underrecognition rate of delirium did not significantly differ between the groups.
Referring Physicians Recognition and Mortality of Delirium (2021–2023)
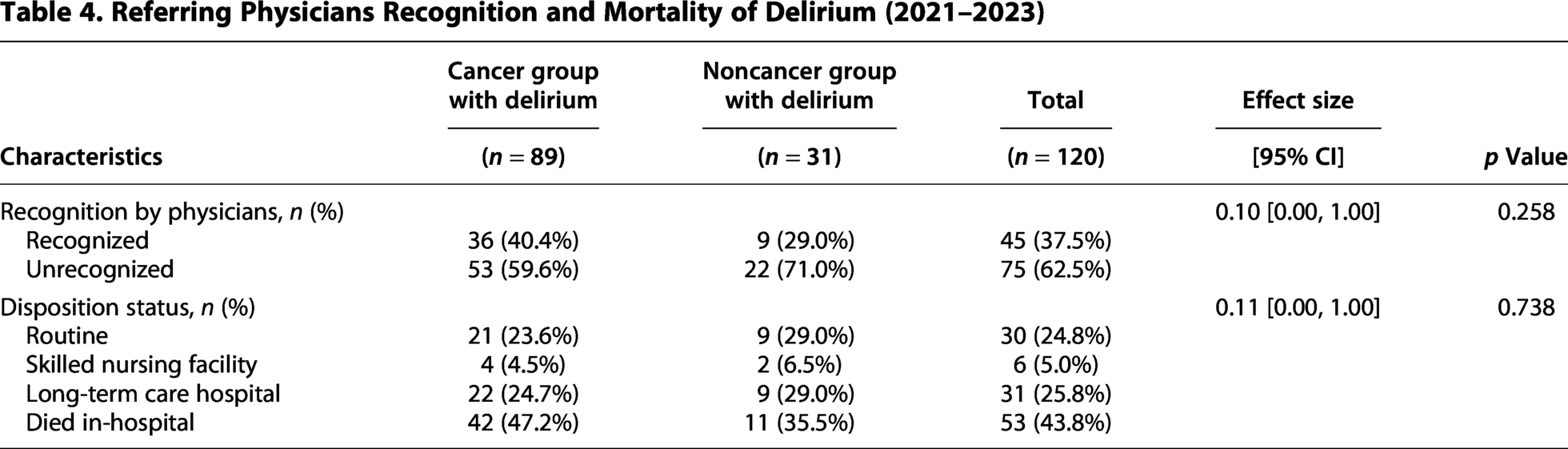
In the cancer group, patients with delirium had a higher mortality rate than those without delirium (47.2% vs. 20.6%, p < 0.001). On the other hand, there was no significant difference in mortality between patients with and without delirium in the noncancer group (35.5% vs. 23.0%, p = 0.159).
Adjusted odds ratios for delirium prevalence and recognition (2021–2023)
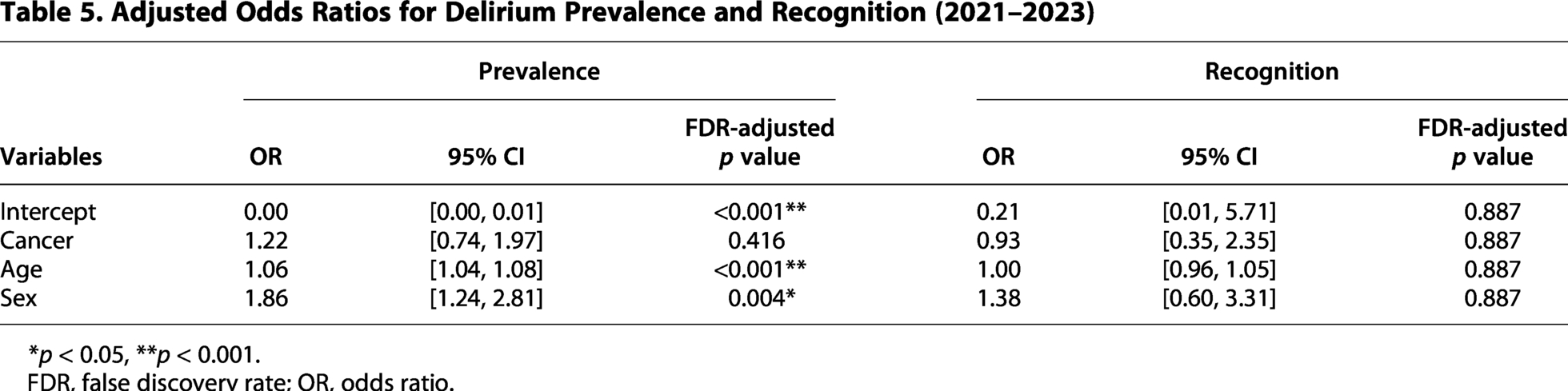
After adjusting for age and sex, cancer status showed no independent association with either the prevalence of delirium or its recognition by the attending physician (Table 5).
Adjusted Odds Ratios for Delirium Prevalence and Recognition (2021–2023)
p < 0.05, **p < 0.001.
FDR, false discovery rate; OR, odds ratio.
Referral reasons in unrecognized delirium cases (2021–2023)
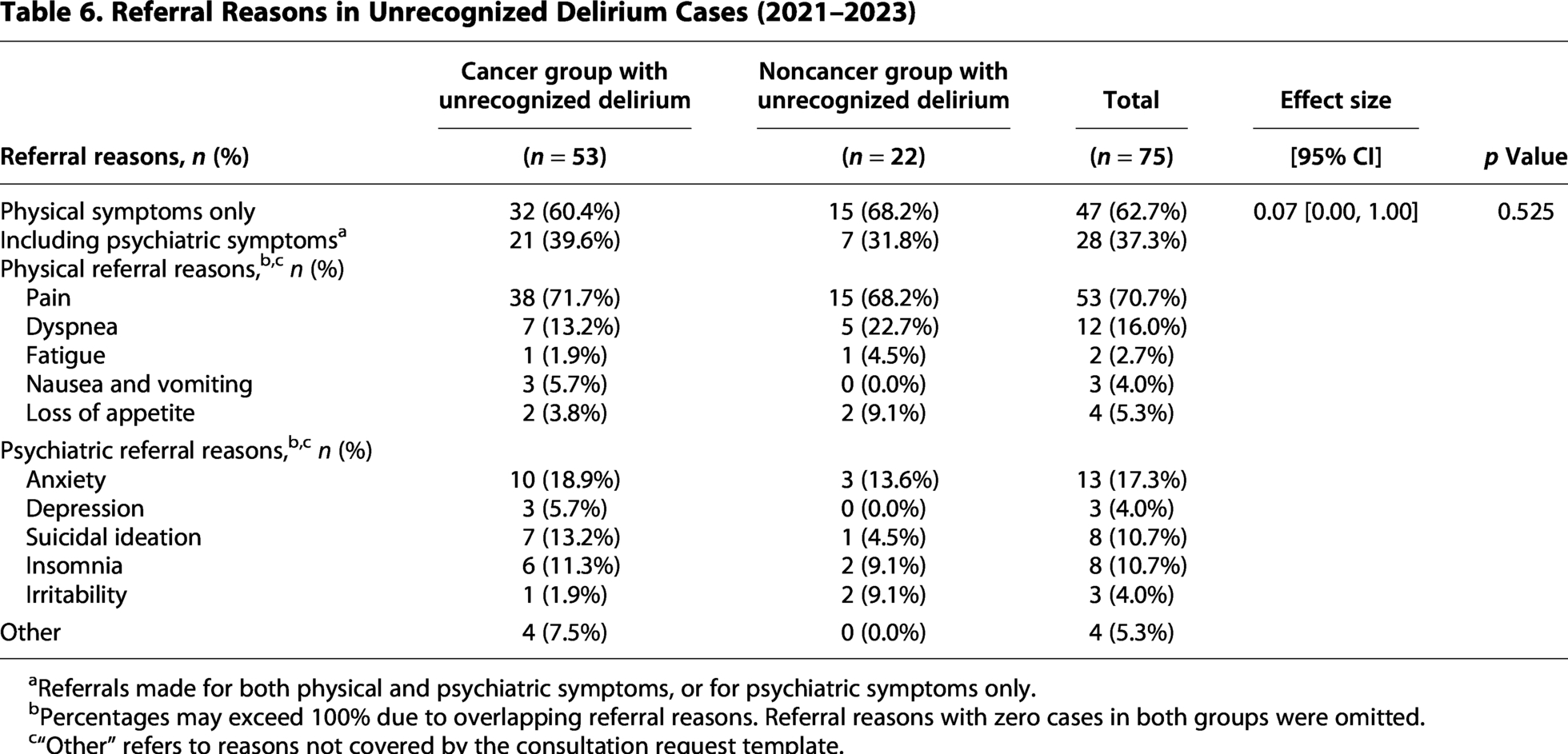
The referral reasons for patients with unrecognized delirium are presented in Table 6. In both groups, the most common reason for referral was pain (71.7% vs. 68.2%).
Referral Reasons in Unrecognized Delirium Cases (2021–2023)
Referrals made for both physical and psychiatric symptoms, or for psychiatric symptoms only.
Percentages may exceed 100% due to overlapping referral reasons. Referral reasons with zero cases in both groups were omitted.
“Other” refers to reasons not covered by the consultation request template.
Discussion
Between 2018 and 2023, palliative care referrals for the noncancer group increased almost tenfold, with a high frequency of referrals from the cardiology and neurology departments. This shift reflects a growing awareness of the importance of palliative care for patients with noncancer conditions, as well as institutional changes, such as revisions to the reimbursement system and the publication of new clinical guidelines.
Against this backdrop of increasing noncancer referrals, our study revealed the characteristics of patients with noncancer conditions receiving palliative care. These patients had a higher proportion of referral reasons citing psychiatric symptoms and a higher prevalence of delirium compared to patients with cancer; nonetheless, referring physicians often overlooked delirium. Pain was cited as a referral reason in approximately 70% of cases of unrecognized delirium.
The prevalence of delirium in patients with cancer receiving palliative care reportedly ranges from 27.6% to 46.9%.5–8 In our study, the prevalence of delirium among the cancer group was lower than that reported in previous studies. This discrepancy may be attributed to differences in care settings, such as cancer centers or hospices, where differences in cancer progression stages may play a role.
Regarding noncancer conditions, studies outside palliative care reported a delirium prevalence of 49.1% in heart failure, 19 31.5% in chronic limb-threatening ischemia, 21 33.4% in chronic obstructive pulmonary disease, 22 and 69.2% in end-stage kidney disease. 23 In the current study, the prevalence was comparatively lower, which may be attributable to differences in patient characteristics or underlying medical conditions. The univariate analysis results reflect the actual clinical situation: delirium is significantly more prevalent in patients with noncancer conditions than in those with cancer. However, it should be noted that our multivariable analysis suggests that this situation is primarily shaped by patient background characteristics, such as older age and a higher proportion of men, rather than cancer status itself.
Previous studies have reported that 55.1% to 76.1% of patients with both cancer and delirium receiving palliative care are unrecognized by attending physicians.5–7 In the present study, 59.8% of patients with cancer who had delirium were not recognized by referring physicians; this is consistent with prior findings. Notably, our results indicated that delirium was unrecognized in a similar proportion of patients with noncancer conditions. These findings highlight that the issue of delirium underrecognition is not limited to patients with cancer but extends to patients with noncancer conditions, despite physicians’ greater focus on their psychiatric symptoms.
Delirium is categorized into three types: “hyperactive,” “hypoactive,” and “mixed.” 24 Hyperactive delirium—characterized by agitation and confusion—is relatively easy to recognize; in contrast, hypoactive delirium—characterized by reduced attention, speech, and activity—is often mistaken for depression, fatigue, or somnolence. 7 In a palliative care setting, a previous report revealed that only 20.5% of patients with the hypoactive subtype were detected by the palliative care team, whereas 95.7% of those with the hyperactive subtype were recognized. 6 The high rate of unrecognized delirium in the current study may partly reflect the diagnostic challenges associated with the hypoactive presentation. Since hypoactive delirium is associated with a poorer prognosis than hyperactive or mixed delirium, 25 early detection and intervention are important.
Delirium is more likely to be overlooked when referrals are primarily for pain management, 7 as symptoms may be misinterpreted as pain responses. 26 Supporting this observation, pain was included as a referral reason for approximately 70% of patients with unrecognized delirium in the current study. It should be emphasized that this tendency was also observed in patients with noncancer conditions.
Our results showed that delirium significantly increased mortality in the cancer group but not in the noncancer group. In palliative settings, opportunities are generally provided to decide the location of end-of-life care, and patients may transition to home care or move to a hospice during their course of care. Given that delirium is widely known to increase mortality, 27 our findings in the noncancer group might have been affected by censoring of observations due to these transitions. Delirium is a treatable condition, and early diagnosis enables prompt intervention to reduce the need for palliative sedation and lower mortality.3,13 However, our results suggest that referring physicians often overlook delirium in both cancer and noncancer patient populations, supporting the notion that enhancing attending physicians’ awareness of delirium could improve the quality of palliative care.
Several effective delirium screening tools have been developed and validated. 28 However, screening rates remain low owing to challenges in applying these tools, the lack of standardized guidelines, and communication barriers. 9 In palliative care, a single screening tool is unlikely to meet the needs of the entire patient population across all care settings. 28 A previous study showed that combining training sessions with the Confusion Assessment Method improved diagnostic accuracy. 29 Thus, in palliative care, it is considered effective to not only integrate standardized screening tools into electronic medical records and incorporate routine screening by attending physicians into the clinical workflow but also to implement systematic educational interventions for early detection of delirium. With regard to educational interventions, it is recommended that clinicians develop materials and systems to regularly update attending physicians on the clinical benefits of early delirium detection, typical symptoms (including those associated with the hypoactive type), the use of screening tools, and initial management protocols when delirium is suspected. The primary treatment for delirium involves nonpharmacological multicomponent approaches. It is effective to include the identification and management of causes, appropriate pain management, reorientation and environmental adjustment, introducing cognitively stimulating activities, and promoting good sleep patterns.30,31 It should be noted that delirium tends to reoccur, 32 and its recurrence is dose-responsively associated with a higher risk of adverse outcomes. 33
Strength and Limitations
A key strength of this study was the systematic evaluation of all palliative care cases referred by psychiatrists at the study site. This process likely contributed to the accurate identification of psychiatric conditions, including delirium, which are frequently underrecognized in general clinical practice. To the best of our knowledge, this is the first study to directly compare the recognition of delirium in patients with cancer and those with noncancer conditions receiving palliative care.
Nonetheless, this study had certain limitations. First, the imbalance in sample sizes between groups and the relatively small number of delirium cases may have affected the validity and statistical power of the comparisons made. Second, several factors may have influenced the prevalence and recognition of delirium, including the marked disparity in referring departments between groups, the combination of risk factors in individual patients, and the heterogeneity of underlying diseases within the noncancer group. Differences in referring departments may have led to variations not only in diseases and treatments but also in the routine practice of delirium prevention and neuropsychiatric assessment. Nevertheless, this study is valuable as it captures the actual clinical situation, reflecting diverse patient backgrounds. Third, early transfer or death after referral and variations in diagnosis among the psychiatrists may have affected the accuracy of the psychiatric diagnoses. However, the accuracy was ensured by the consensus within a team, including a board-certified psychiatrist, based on the ICD-10 criteria. Fourth, unrecognized delirium might have been overestimated, as some attending physicians might have identified delirium but not explicitly stated it in the referral. Fifth, this was a single-center retrospective analysis, potentially limiting the generalizability of the findings.
Despite these limitations, our findings highlight the need for the appropriate use of screening tools and the systematic implementation of educational interventions to improve the early identification of delirium and other psychiatric conditions in palliative care settings. Future prospective studies focusing on risk factors and subtypes of delirium, using multivariable analysis, will help identify independent factors associated with delirium prevalence and recognition, leading to more effective screening and education.
Conclusions
Although patients with noncancer conditions receiving palliative care have a notably higher prevalence of delirium than those with cancer, the condition is frequently underrecognized by attending physicians. These findings underscore the need for delirium education for physicians to ensure the timely and appropriate management of delirium in palliative care settings.
Ethical Approval and Informed Consent Statements
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of Tokai University School of Medicine (approval number: 23R240) on May 17, 2024. The need for written informed consent was waived owing to the use of retrospective, anonymized data.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.
Authors’ Contributions
Y.S.: Conceptualization (lead), investigation (lead), data curation (equal), formal analysis (equal), writing—original draft (lead), and writing—review and editing (equal). Y.T.: Supervision (lead), conceptualization (supporting), and writing—review and editing (equal). T.N.: Investigation (supporting), data curation (equal), and writing—review and editing (supporting). S.S.: Investigation (supporting), data curation (equal), and writing—review and editing (supporting). K.F.: Formal analysis (lead), validation (equal), and writing—review and editing (supporting). K.M.: Methodology (equal), formal analysis (supporting), and writing—review and editing (supporting). M.T.: Supervision (supporting), resources (equal), and writing—review and editing (supporting). K.Y.: Supervision (lead), conceptualization (supporting), resources (equal), and writing—review and editing (equal).
Footnotes
Acknowledgments
The authors would like to thank Editage for its English editing and proofreading services.
Author Disclosure Statement
K.Y. reports grants and personal fees from Eisai Co., Ltd., Otsuka Pharmaceutical Co., Ltd., and Shionogi & Co., Ltd.; personal fees from Meiji Seika Pharma Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Merck Sharp & Dohme, Viatris Inc., Takeda Pharmaceutical Co., Ltd., Janssen Pharmaceutical K.K., Lundbeck Japan K.K., Daiichi Sankyo Co., Ltd., and OCTAWELL Co., Ltd.; and grant support from JSPS KAKENHI (grant number: 22K07588), all outside the submitted work.K.M. has received a Grant-in-Aid for Scientific Research (C) (Number 22K07624) and financial support from Shionogi & Co., Ltd.; honoraria from Shionogi & Co., Ltd., Sumitomo Pharma Co., Ltd., and Takeda Pharmaceutical Co., Ltd.; travel and accommodation expenses from Otsuka Pharmaceutical Co., Ltd.; and consulting fees from Shionogi & Co., Ltd., EA Pharma Co., Ltd., Sumitomo Pharma Co., Ltd., and Otsuka Pharmaceutical Co., Ltd.Y.T. reports grant from Shionogi & Co., Ltd.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.