
Abstract
Background:
Opioid-induced constipation (OIC) is a common adverse effect of opioid therapy in cancer patients, often persisting despite laxatives and peripherally acting μ-opioid receptor antagonists. Moxibustion, a traditional thermal therapy applied to acupuncture points, has been proposed as a supportive option, but clinical evidence for OIC remains scarce. This study evaluated the clinical outcomes and feasibility of moxibustion for OIC in advanced cancer patients.
Methods:
We conducted a prospective case series at Kagawa University Hospital (April 2023–July 2025). Ten patients with advanced cancer and clinically diagnosed OIC were included. Eligibility required Eastern Cooperative Oncology Group performance status 0–2 and no prior chronic constipation. Moxibustion was delivered twice weekly for three weeks (six sessions) to standardized abdominal, hand, and foot acupoints using a ceramic warming device. Constipation severity was assessed with the Constipation Assessment Scale (CAS). Secondary outcomes included laxative use, stool form, and Edmonton Symptom Assessment System-Revised.
Results:
Eight patients improved in CAS scores (mean change −2.8, SD: 3.0; p = 0.012) and sustained it at four-week follow-up (−2.5, SD: 2.7; p = 0.022). All patients reduced laxative use, and several achieved normalization of stool form. No treatment-related adverse events occurred.
Conclusions:
This case series indicates moxibustion is a feasible and safe complementary therapy for OIC in advanced cancer, with the potential to reduce symptom burden and medication use. While limited by small sample size and lack of control, the findings support further trials to confirm its role in integrative palliative care.
Introduction
Opioid analgesics such as morphine, fentanyl, oxycodone, methadone, tapentadol, and hydromorphone are indispensable for cancer pain management. However, their use is often accompanied by tolerance and adverse effects. Among these, constipation is the most frequent, occurring in more than half of patients receiving opioids.1,2 Unlike nausea or drowsiness, constipation does not improve spontaneously over time, and therefore continuous management is required during opioid therapy. The mechanisms of opioid-induced constipation (OIC) include inhibition of small intestinal motility, reduction in digestive secretions, increased stool viscosity, impaired colonic propulsion, and enhanced anal sphincter tone. 2
In clinical practice, dietary modification and lifestyle management alone are often insufficient. Pharmacological approaches such as laxatives and, more recently, peripherally acting μ-opioid receptor antagonists (PAMORAs), such as naldemedine and methylnaltrexone, are essential.3,4 Nonetheless, patients frequently continue to experience difficult-to-manage constipation, alternating with diarrhea, and in severe cases require invasive interventions such as manual disimpaction or enemas. These situations increase physical and psychological distress for patients, as well as the burden on caregivers and health care providers.
Current Japanese guidelines mention nonpharmacological strategies such as abdominal massage and acupoint stimulation but conclude that the evidence supporting acupuncture for constipation remains insufficient.3–7 On the contrary, international guidelines highlight integrative approaches. The American Society of Clinical Oncology (ASCO) and the Society for Integrative Oncology (SIO) recommend nonpharmacological interventions, including acupuncture, as a part of integrative care for cancer survivors.8,9 The Oncology Nursing Society (ONS) guidelines also suggest acupuncture and electroacupuncture for constipation within the context of clinical trials. 10 This discrepancy underscores the need for additional real-world clinical evidence, particularly in Asian populations.
Recent studies have begun to provide evidence for the role of acupuncture in OIC. Olson et al. reported symptomatic improvement in a patient with OIC when acupuncture was used in addition to pharmacotherapy. 11 Yildirim et al. demonstrated in a randomized controlled trial (RCT) that acupressure significantly improved stool frequency, stool consistency, and quality of life (QOL) in cancer patients with OIC. 12 Wang et al. reported in a multicenter RCT that electroacupuncture improved OIC symptoms and QOL. 13 Furthermore, systematic reviews and meta-analyses support the efficacy and safety of acupuncture and moxibustion for constipation, gastrointestinal dysfunction, and chemotherapy-related side effects.14–16 Yang et al. also summarized recent progress in integrative oncology, including the potential role of acupuncture and moxibustion in cancer care. 17 Moxibustion is a traditional thermal therapy widely practiced in East Asia, particularly in Japan, China, and Korea. Although it is less commonly incorporated into mainstream oncology and palliative care outside Asia, it is available in some countries through integrative medicine, acupuncture, or complementary therapy services. These findings suggest that acupuncture and moxibustion may be promising supportive options for OIC, warranting further clinical research. Given the limited availability of clinical data on moxibustion for OIC, case series may provide important preliminary evidence to inform future trials. Therefore, we conducted a case series to describe the clinical outcomes of moxibustion as a supportive therapy for OIC in patients with advanced cancer.
Materials and Methods
Patients
Between April 2023 and July 2025, this prospective case series enrolled ten patients with advanced cancer who were diagnosed with OIC by a physician at the Department of Palliative Care, Kagawa University Hospital. OIC was diagnosed according to the Rome IV criteria, defined as the presence or worsening of constipation symptoms following opioid initiation or dose escalation, including straining, hard or lumpy stools, a sensation of incomplete evacuation, a sensation of anorectal obstruction, or the need for manual maneuvers in more than 25% of defecations, accompanied by fewer than three spontaneous bowel movements (SBMs) per week. 18 Eligible patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2 and did not have preexisting chronic constipation, which was defined as having at least three spontaneous bowel movements during the seven days prior to enrollment. All patients developed constipation symptoms such as hard stool, incomplete evacuation, or abdominal bloating after the initiation of opioid analgesics for cancer pain. Although all patients were receiving concomitant laxatives, they continued to experience alternating constipation and diarrhea, which prompted the initiation of moxibustion therapy as a supportive intervention.
Intervention
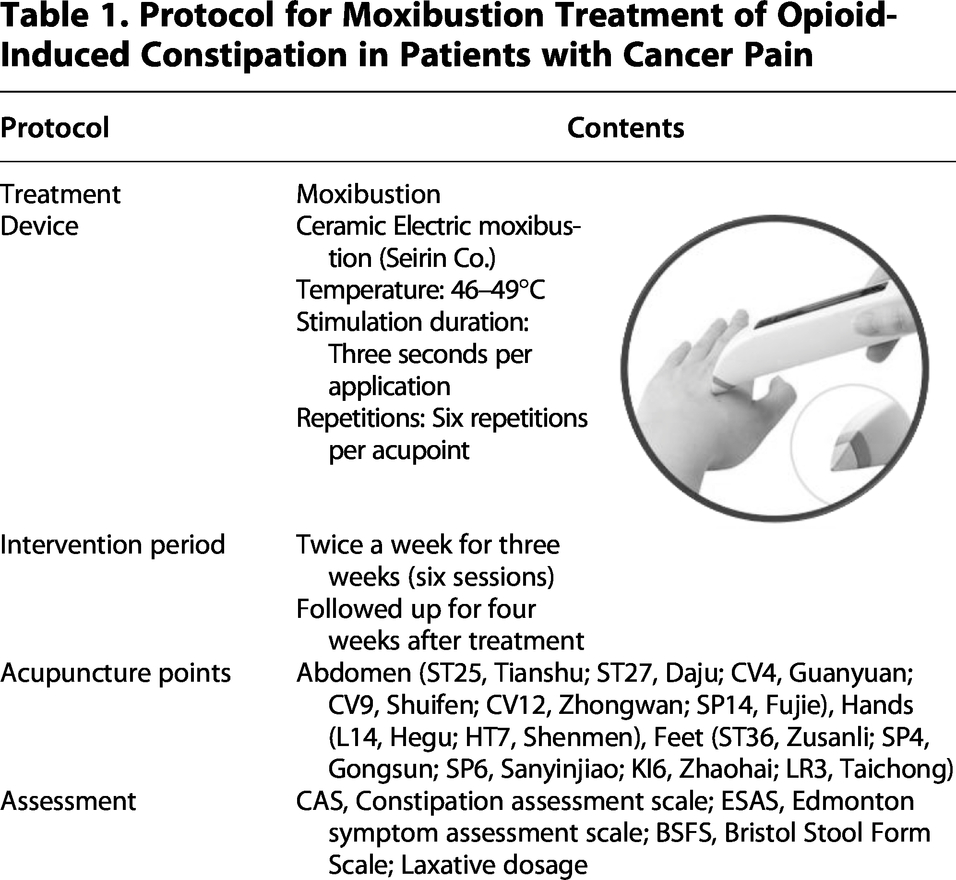
Moxibustion was administered twice weekly for three weeks (six sessions in total) according to a standardized protocol (Table 1). A ceramic electric warming device (Seirin Corporation, Japan) was applied to deliver thermal stimulation to the following acupuncture points: abdominal points (ST25, Tianshu; ST27, Daju; CV4, Guanyuan; CV9, Shuifen; CV12, Zhongwan; SP14, Fujie), hand points (LI4, Hegu; HT7, Shenmen), and foot points (ST36, Zusanli; SP4, Gongsun; SP6, Sanyinjiao; KI6, Zhaohai; LR3, Taichong).
Protocol for Moxibustion Treatment of Opioid-Induced Constipation in Patients with Cancer Pain
Outcome measures
The primary outcome was the change in constipation symptoms assessed using the Japanese version of the Constipation Assessment Scale (CAS; 8 items on a 3-point scale, range 0–16, with higher scores indicating more severe constipation).19,20 Secondary outcomes included the following: (1) laxative dose, (2) stool form assessed by the Bristol Stool Form Scale (BSFS), and (3) symptom burden assessed by the Japanese version of the Edmonton Symptom Assessment System-Revised (ESAS-r). Patients were followed for four weeks after completion of the intervention.
Statistical analysis
Changes in outcome measures at baseline, posttreatment, and 4-week follow-up were analyzed using repeated-measures ANOVA. Given the small sample size, results were primarily descriptive and supported by Wilcoxon signed-rank tests. A p value <0.05 was considered statistically significant. Analyses were performed with JMP Pro 18 (SAS Institute, Cary, NC, USA).
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee of the Kagawa University School of Medicine (approval no.: 2021-119; approval date: November 8, 2021). The benefits and risks of the study were explained to the participants using an explanatory document. After ensuring that the participants fully understood this explanation, their free and voluntary informed consent to participate in this study was obtained in writing.
Case presentations
A total of 10 patients with advanced cancer who developed OIC were included.
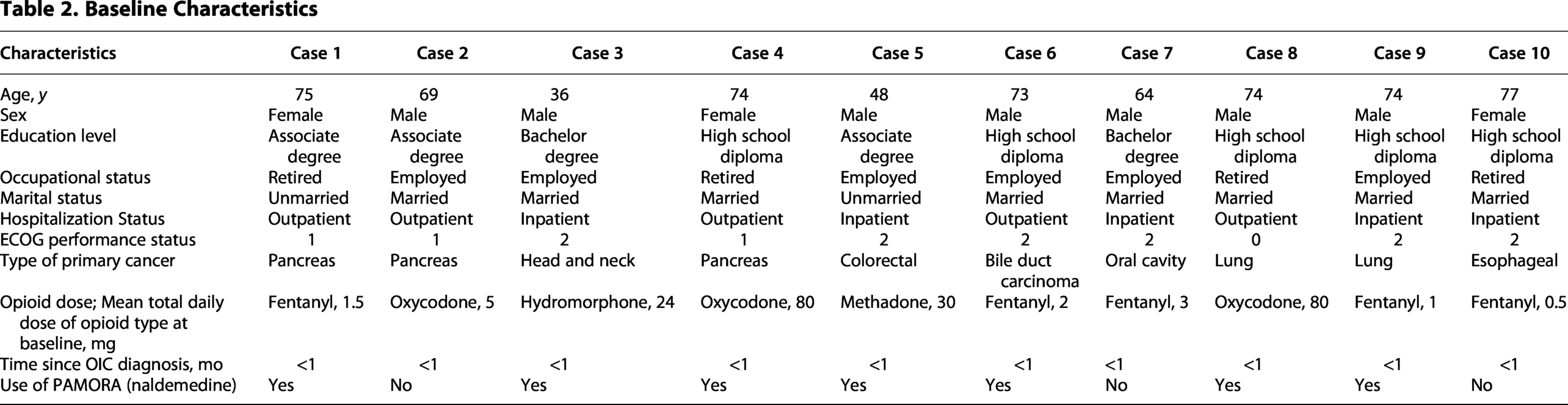
Brief summaries of individual cases are provided to illustrate the clinical context and heterogeneity of presentation. A 75-year-old woman with pancreatic cancer receiving fentanyl (1.5 mg/day) developed hard stools and incomplete evacuation. A 69-year-old man with pancreatic cancer on oxycodone (5 mg/day) reported new-onset constipation unresponsive to laxatives. A 36-year-old man with head and neck cancer on hydromorphone (24 mg/day) developed abdominal bloating and decreased stool frequency. A 74-year-old woman with pancreatic cancer on oxycodone (80 mg/day) experienced alternating constipation and diarrhea. A 48-year-old man with colorectal cancer on methadone (30 mg/day) presented with straining and hard stools. A 73-year-old man with bile duct carcinoma receiving fentanyl (2 mg/day) reported incomplete evacuation and small-volume stools. A 64-year-old man with oral cavity cancer on fentanyl (3 mg/day) experienced progressive constipation despite laxatives. A 74-year-old man with lung cancer on oxycodone (80 mg/day) had reduced bowel movements and abdominal discomfort. A 74-year-old man with lung cancer receiving fentanyl (1 mg/day) developed new-onset constipation shortly after opioid initiation. A 77-year-old woman with esophageal cancer on fentanyl (0.5 mg/day) reported abdominal bloating and stool hardness.
All patients met the eligibility criteria and subsequently completed the standardized 6-session moxibustion protocol.
Results
The baseline characteristics and concomitant medications of the 10 patients are summarized in Table 2. All patients completed the treatment protocol and follow-up, and no adverse events such as skin reactions, worsening of pain, or fatigue requiring discontinuation were observed. At baseline, all patients were receiving pharmacologic bowel regimens, including stimulant laxatives, osmotic agents, and/or stool softeners. Seven of ten patients (70%) were receiving naldemedine (Symproic®), a PAMORA.
Baseline Characteristics
Eight of ten patients showed improvement in constipation symptoms. The mean CAS score decreased by −2.8 points (SD: 3.0; p = 0.012) after six sessions of moxibustion, with the benefit sustained at 4-week follow-up (−2.5, SD: 2.7; p = 0.022) (Table 3). Spontaneous bowel function improved during the treatment period. The mean time to first spontaneous bowel movement after initiation of moxibustion was 0.9 days. The mean number of spontaneous bowel movements per week increased significantly from 1.6 at baseline to 4.4 posttreatment (mean change + 2.8, SD: 1.9; p = 0.003), with the effect partially maintained at follow-up (3.9; mean change + 2.3, SD: 1.8; p = 0.027). In parallel with these improvements, all patients reduced their laxative use during the treatment period. Stool consistency also improved, with the proportion of patients achieving normal stool form (BSFS types 3–4) increasing from 20.0% at baseline to 60.0% posttreatment, although this decreased to 30.0% at follow-up (Table 3). Several patients achieved normalization of stool consistency, although some continued to report loose or small-volume stools (types 6–7).
Primary and Secondary Outcomes
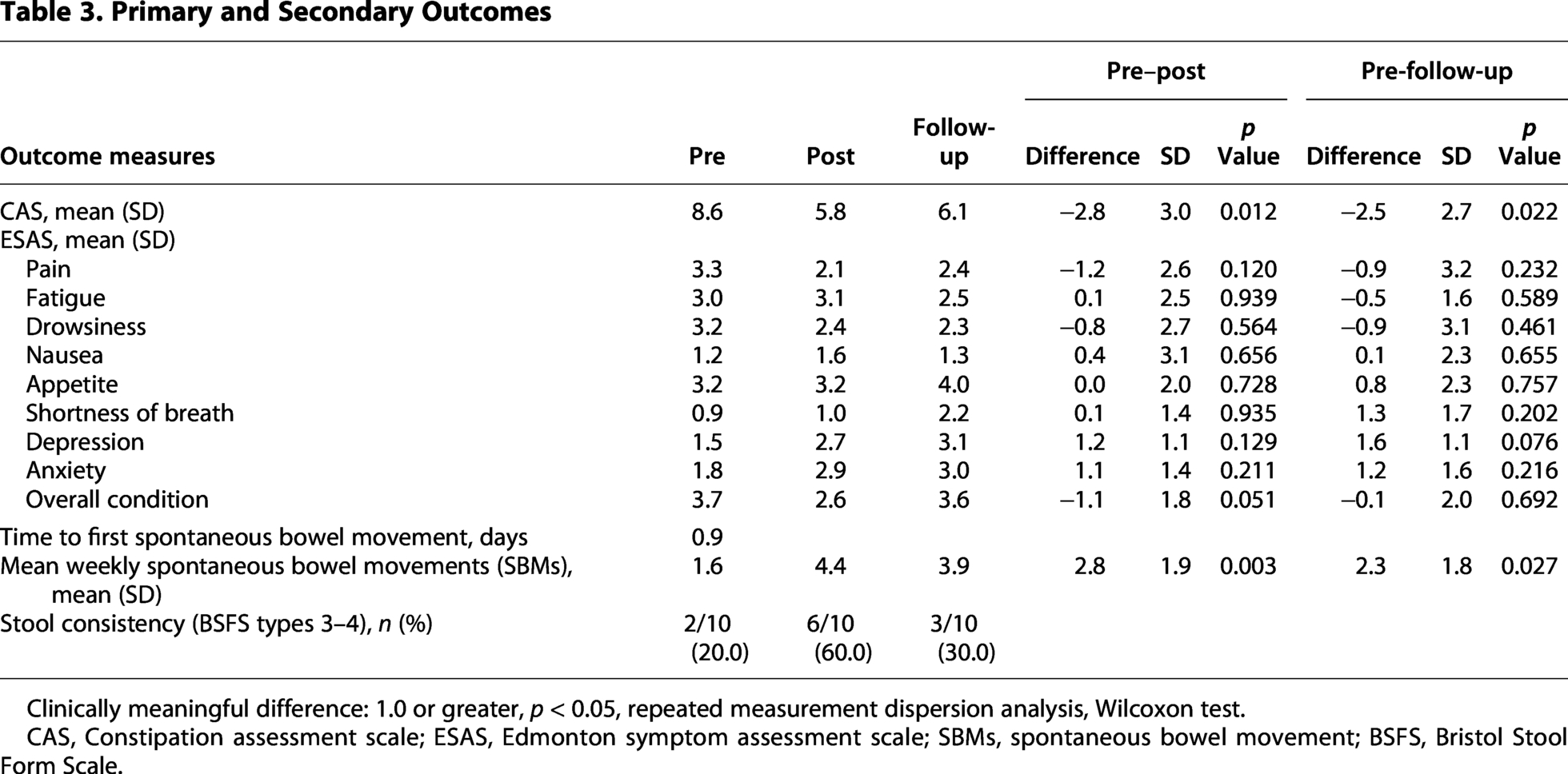
Clinically meaningful difference: 1.0 or greater, p < 0.05, repeated measurement dispersion analysis, Wilcoxon test.
CAS, Constipation assessment scale; ESAS, Edmonton symptom assessment scale; SBMs, spontaneous bowel movement; BSFS, Bristol Stool Form Scale.
During the short follow-up period, constipation symptoms did not uniformly recur, although longer-term outcomes could not be assessed.
Regarding general symptoms, ESAS-r-J indicated a mean improvement of −1.2 (SD: 2.6) in pain after treatment. Other physical symptoms showed minimal changes (mean change <1.0). Psychological distress scores showed a small increase (+1.2, SD: 1.1), indicating that emotional burden persisted despite stable pain control.
Discussion
This case series suggests that moxibustion may contribute to alleviation of OIC symptoms in patients with advanced cancer. In addition to improvements in constipation symptoms and reduced laxative use, the absence of treatment-related adverse events highlights its feasibility and safety in routine clinical care.
The potential mechanisms of action of moxibustion include stimulation of intestinal peristalsis, enhancement of local blood flow, and modulation of the autonomic nervous system through thermal stimulation at acupoints. 21 The clinical improvements observed in this study are consistent with these proposed mechanisms. Notably, spontaneous bowel movements occurred early after initiation of moxibustion, with a mean time to first bowel movement of less than one day. This finding suggests a rapid onset of effect, which may be clinically meaningful for patients experiencing distressing constipation. Nevertheless, stool quality remained a challenge: while some patients achieved normalization, others experienced loose or small-volume stools, likely reflecting the complexity of OIC and possible overflow constipation.³ This may also explain the observed alternation between constipation and diarrhea, resulting from intermittent leakage of liquid stool around impacted feces. The decline in normalization rates at follow-up may suggest that the effects of moxibustion are time-limited, and repeated or maintenance sessions may be required to sustain these benefits, which should be explored in future studies.
The integration of complementary therapies with pharmacological interventions plays an important role in OIC management. Acupuncture and moxibustion have long been used for pain and functional constipation, and recent attention has focused on their role in OIC. Evidence from randomized trials and meta-analyses suggests that these interventions improve stool frequency, abdominal symptoms, and QOL.11–16 Our findings extend this evidence by demonstrating that a standardized moxibustion protocol can be safely implemented in a real-world palliative care setting. In addition, all patients were able to reduce their laxative use during the treatment period, suggesting that moxibustion may help decrease reliance on pharmacologic interventions. This is particularly relevant in palliative care, where minimizing medication burden is an important clinical goal.
Regarding general symptoms, the ESAS-r-J showed a modest improvement in pain scores, while other physical symptoms demonstrated minimal changes. Psychological distress scores showed a small increase, indicating that emotional burden persisted despite stable pain control. This finding likely reflects the multifactorial nature of psychological distress in advanced cancer, including disease progression, prognostic awareness, and psychosocial stressors that may not improve in parallel with physical symptom control.
When introducing nonpharmacological interventions, it is essential to consider patients’ needs, treatment preferences, and the balance with existing therapies. Deng emphasized that although integrative therapies can improve QOL, their application requires careful consideration of evidence quality, potential risks, and financial burden. 22 These perspectives are crucial for integrating acupuncture and moxibustion into palliative care. Although moxibustion was readily available and feasible within our hospital setting in Japan, its availability and insurance coverage vary across countries and health care systems. Therefore, issues related to access, cost, and equity should be considered when interpreting the generalizability of these findings to other settings.
This study has limitations, including its small sample size, lack of a control group, and reliance on subjective measures. However, its strengths include prospective design, standardized intervention protocol, and detailed safety monitoring. These features support the reliability of our observations.
In summary, moxibustion appears to be a feasible, safe, and potentially useful complementary intervention for OIC in advanced cancer. While larger controlled trials are needed, the present findings suggest that clinicians may consider moxibustion as a supportive option when conventional treatments are insufficient.
Conclusion
This prospective case series suggests that moxibustion may be a complementary option for managing OIC in patients with advanced cancer. Further controlled studies are warranted to confirm efficacy and to define the optimal treatment protocol.
Authors’ Contributions
K.K. and A.M. conceived the study. K.K. collected and analyzed the data and drafted the article. A.M. supervised the clinical management, contributed to patient recruitment and data acquisition. N.R.N. contributed to study design and interpretation and assisted in article editing. T.H. provided academic supervision and contributed to the interpretation of results. A.H. provided guidance on research design and critically reviewed the article. All authors critically revised and approved the final version of the article.
Ethics Approval and Consent to Participate
The study was conducted according to the Declaration of Helsinki and approved by the Ethics Committee of Kagawa University School of Medicine (approval no.: 2021–119; approval date: November 8, 2021). Written informed consent was obtained from all participants. All patient information was fully anonymized prior to analysis and reporting.
Consent for Publication
Written informed consent for publication of anonymized clinical data was obtained from all participants. All patient information was fully anonymized prior to analysis and reporting.
Use of Artificial Intelligence
No generative artificial intelligence tools were used to create, analyze, or interpret the data in this study.
AI-based tools were used only for language editing after the scientific content was finalized, and all authors reviewed and approved the final article.
Footnotes
Acknowledgments
The authors thank the staff of the Department of Palliative Care, Kagawa University Hospital, for their dedicated support of inpatient care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a Grant-in-Aid for Young Scientists from the Japan Society for the Promotion of Science (JSPS KAKENHI, grant number