
Abstract
Home-based palliative care for patients with advanced heart failure remains challenging because refractory dyspnea and hemodynamic instability often require continuous medical support. Continuous dobutamine infusion is occasionally used to facilitate discharge to home in patients with end-stage heart failure; however, symptom relief with inotropic therapy alone may become insufficient during the terminal stage of illness. Reports describing the combined use of home dobutamine infusion and opioid therapy remain limited, particularly in Japan.
We report two elderly patients with advanced heart failure who wished to spend their remaining time at home and were managed with continuous home dobutamine infusion combined with opioid therapy for symptom palliation. Case 1 involved an 84-year-old man with cardiac amyloidosis, severe mitral regurgitation (MR), and low cardiac output syndrome. Despite guideline-directed medical therapy and transcatheter edge-to-edge mitral valve repair, progressive fatigue and heart failure symptoms persisted. Continuous home dobutamine infusion was initiated, and transdermal fentanyl was subsequently added because of worsening dyspnea and discomfort. The patient remained at home and died 99 days after discharge. Case 2 involved a 91-year-old woman with advanced valvular heart disease, severe tricuspid regurgitation, pulmonary hypertension, and recurrent heart failure hospitalization. After temporary stabilization with dobutamine and symptom-oriented treatment, she was discharged home with continuous dobutamine infusion and opioid therapy. Although she died 5 days after discharge, her wish to remain at home was fulfilled.
These cases suggest that combined home-based dobutamine infusion and opioid therapy may represent a feasible symptom-oriented palliative care strategy for selected patients with advanced heart failure who strongly prefer home-based end-of-life care. Further studies are needed to clarify patient selection, symptom outcomes, and safety considerations.
Introduction
Home-based palliative care for patients with advanced heart failure remains challenging because refractory dyspnea and hemodynamic instability often require continuous medical support. Although continuous dobutamine infusion is occasionally used to facilitate discharge to home in patients with end-stage heart failure, symptom relief with inotropic therapy alone may be insufficient during the terminal stage of the illness.
In terms of safety and efficacy, dobutamine is an excellent inotropic agent for use in patients with end-stage heart failure. 1 Furthermore, it has been reported that in patients with end-stage heart failure, the use of dobutamine preparations at home not only alleviates symptoms but also reduces the rate of readmission. 2
Reports describing the combined use of home dobutamine infusion and opioid therapy remain limited, particularly in Japan. It has been reported that the use of opioids to alleviate symptoms does not affect mortality rates in patients with heart failure. 3
We report the cases of two elderly patients with advanced heart failure who wished to spend their remaining time at home and who were managed with continuous home dobutamine infusion combined with opioid therapy for symptom palliation in the same setting.
Case 1 involved an 84-year-old man with cardiac amyloidosis and severe MR complicated by low cardiac output syndrome. Despite guideline-directed therapy and transcatheter edge-to-edge mitral valve repair, progressive fatigue and heart failure symptoms persisted. Continuous home dobutamine infusion was initiated, and transdermal fentanyl was added because of worsening dyspnea and discomfort. The patient remained at home and died 99 days after discharge.
Case 2 involved a 91-year-old woman with advanced valvular heart disease, severe tricuspid regurgitation, pulmonary hypertension, and recurrent heart failure. Following stabilization with dobutamine and symptom-oriented treatment, the patient was discharged with continuous dobutamine infusion and opioid therapy. Although she died five days after discharge, her wish to remain at home was granted.
These cases highlight the feasibility of combining continuous home dobutamine infusion and opioid therapy as part of symptom-oriented palliative care in selected patients with advanced heart failure. This approach may support home-based end-of-life care for patients with refractory symptoms who strongly prefer to stay at home.
Case Description
Case 1 was an 84-year-old man with a history of catheter ablation for atrial fibrillation who developed dyspnea due to acute decompensated heart failure in 20XX. He underwent pacemaker implantation for a complete atrioventricular block in 20XX-1. After hospitalization, echocardiography revealed left ventricular hypertrophy compatible with cardiac amyloidosis and severe MR. Despite sufficient guideline-directed medical therapy and transcatheter edge-to-edge mitral valve repair, general fatigue and appetite loss due to low cardiac output syndrome persisted. Given his strong desire to return home, we decided to continue his medical care at home.
His medication list was as follows: bisoprolol fumarate (0.625 mg/day); enalapril maleate (0.625 mg/day); pimobendane (1.2 mg/day); empagliflozin (10 mg/day); tolvaptan (7.5 mg/day), torsemide (8 mg/day); bepridil hydrochloride (5 mg/day); esomeprazole magnesium hydrate (20 mg/day); rosvastatin (5 mg/day), febuxostat (10 mg/day); sodium ferrous citrate (50 mg/day); lemborexant (5 mg/day); sodium valproate (200 mg/day); and magnesium oxide (330 mg/day).
At discharge, the patient did not experience dyspnea. A physical examination revealed bilateral leg edema, and the patient’s hands and feet were cool and clammy. The pulse was 70 beats/minute, and blood pressure was 73/48 mmHg. Peripheral oxygen saturation measured by pulse oximetry was 95% on room air despite cool extremities, and the pulse waveform was adequately detected during the examination.
Blood tests revealed anemia, renal dysfunction, and elevated total bilirubin (BNP) levels (Table 1). Electrocardiography revealed a pacemaker rhythm (Fig. 1A). A plain chest radiograph revealed cardiomegaly, pleural effusion in both lungs, and congestion in the lung fields (Fig. 1B). Echocardiography showed an ejection fraction of 35% with asymmetrical hypertrophy (Fig. 1C). The patient’s hemodynamics were maintained with dobutamine (5 μg/kg/min) via a totally implantable central venous access port. However, 44 days after discharge, his appetite gradually decreased. Subsequently, progressive dyspnea and appetite loss developed.
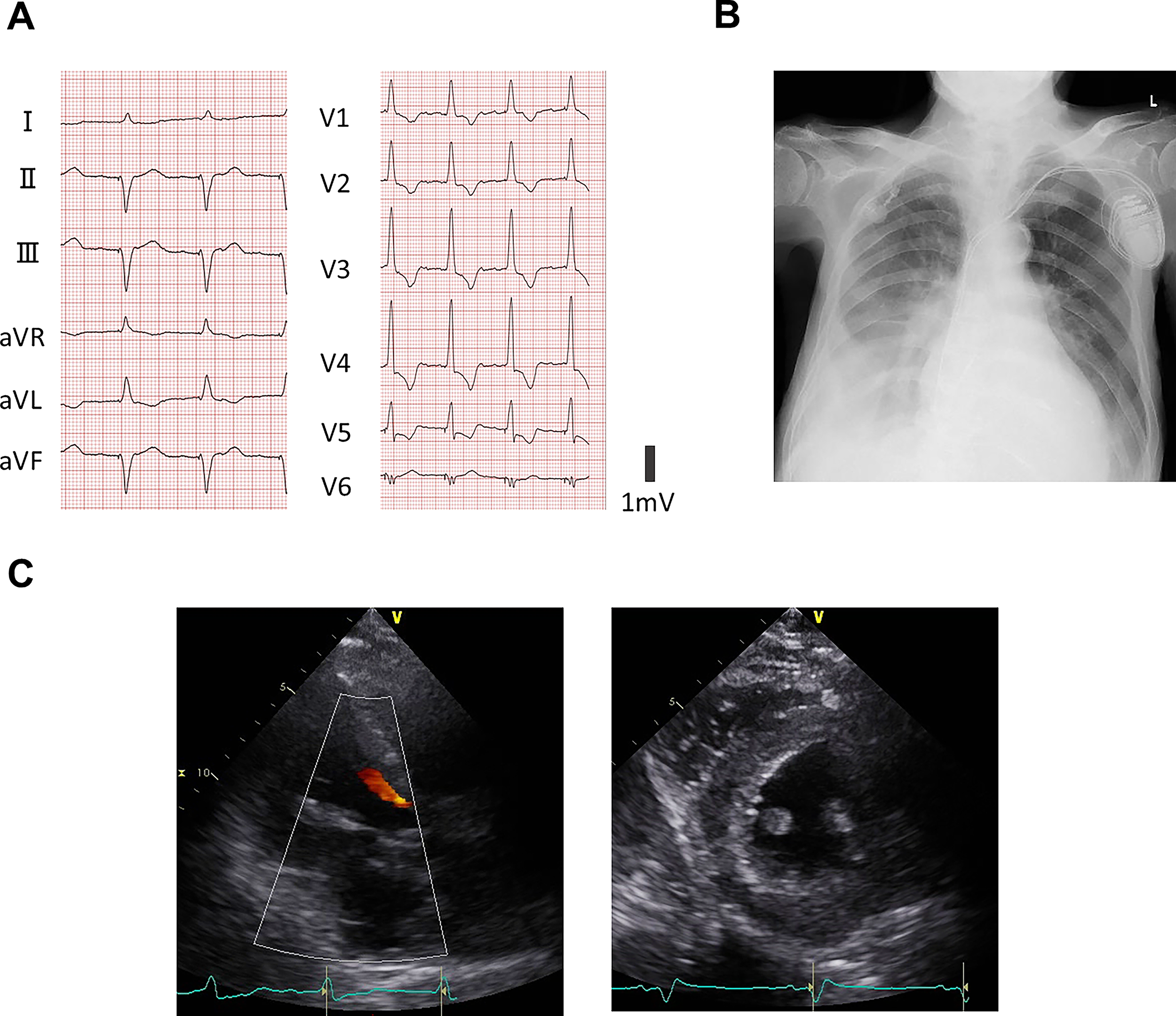
Clinical findings in Case 1.
Laboratory Findings at Discharge
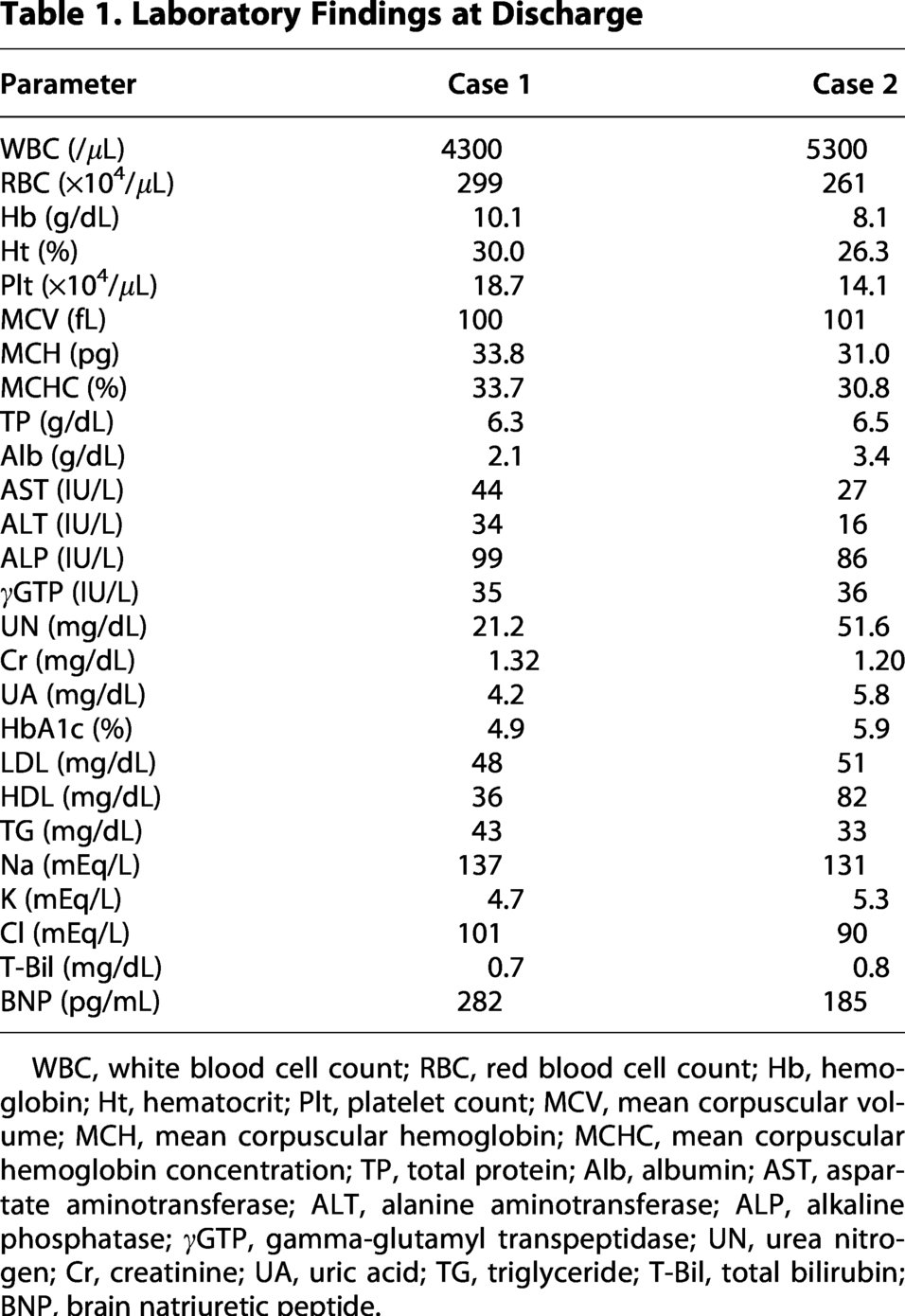
WBC, white blood cell count; RBC, red blood cell count; Hb, hemoglobin; Ht, hematocrit; Plt, platelet count; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; TP, total protein; Alb, albumin; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALP, alkaline phosphatase; γGTP, gamma-glutamyl transpeptidase; UN, urea nitrogen; Cr, creatinine; UA, uric acid; TG, triglyceride; T-Bil, total bilirubin; BNP, brain natriuretic peptide.
He was treated with a transdermal fentanyl patch (0.5 mg/day), which alleviated dyspnea, but he died on the 99th day (Fig. 2A).
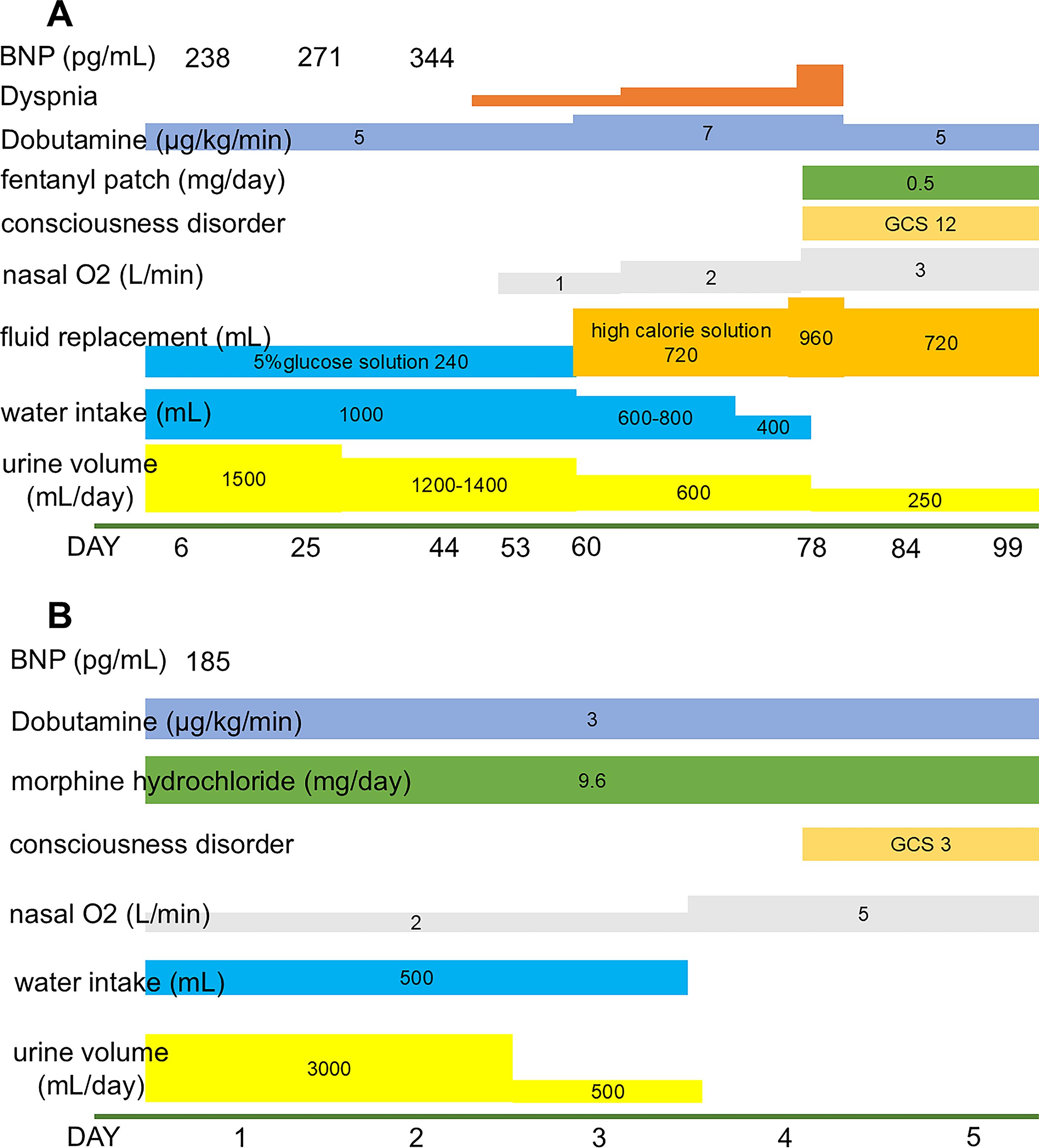
Clinical course after discharge.
Case 2 involved a 91-year-old woman with a history of hypothyroidism who developed dyspnea due to acute decompensated heart failure in 20XX. She had bilateral atrial enlargement associated with chronic atrial fibrillation, which resulted in functional MR and severe tricuspid regurgitation. Mitral valve transcatheter edge-to-edge repair was performed in 20XX, resulting in the improvement of her MR. However, one month after the surgery, she was readmitted to Y-Hospital due to an acute exacerbation of congestive heart failure. Her general fatigue improved after the administration of high-dose dobutamine, morphine hydrochloride, and oxygen therapy. As she was able to clearly express her wishes, we decided to continue her medical care at home.
Her medication list was as follows: acetaminophen (1200 mg/day), mirogabalin besilate (7.5 mg/day), digoxin (0.05 mg/day), pimobendan (5 mg/day), tolvaptan (15 mg/day), azosemide (120 mg/day), nicorandil (15 mg/day), atorvastatin calcium hydrate (20 mg/day), lansoprazole (15 mg/day), levothyroxine sodium hydrate (50 μg/day); clopidogrel sulfate (75 mg/day), zinc acetate dihydrate (50 mg/day), and febuxostat (20 mg/day).
At discharge, the patient did not experience dyspnea. A physical examination revealed bilateral leg edema, and the patient’s hands and feet were cool and clammy. Her pulse rate was 118 beats/min, and her blood pressure was 134/66 mmHg. The patient was receiving oxygen at home under nasal oxygen at 2 L/min, and her oxygen saturation was 97%.
Blood tests revealed anemia, renal dysfunction, and elevated BNP levels (Table 1). Electrocardiography revealed atrial fibrillation (Fig. 3A), and plain chest radiography revealed cardiomegaly, pleural effusion in both lungs, and congestion in the lung fields (Fig. 3B). Echocardiography showed an ejection fraction of 76% with right ventricular dysfunction and severe tricuspid valve regurgitation. The estimated pulmonary artery pressure was 81 mmHg (Fig. 3C). Hemodynamics were maintained using dobutamine at 3 μg/kg/min via a peripherally inserted central venous catheter. However, she died on the 5th day (Fig. 2B).
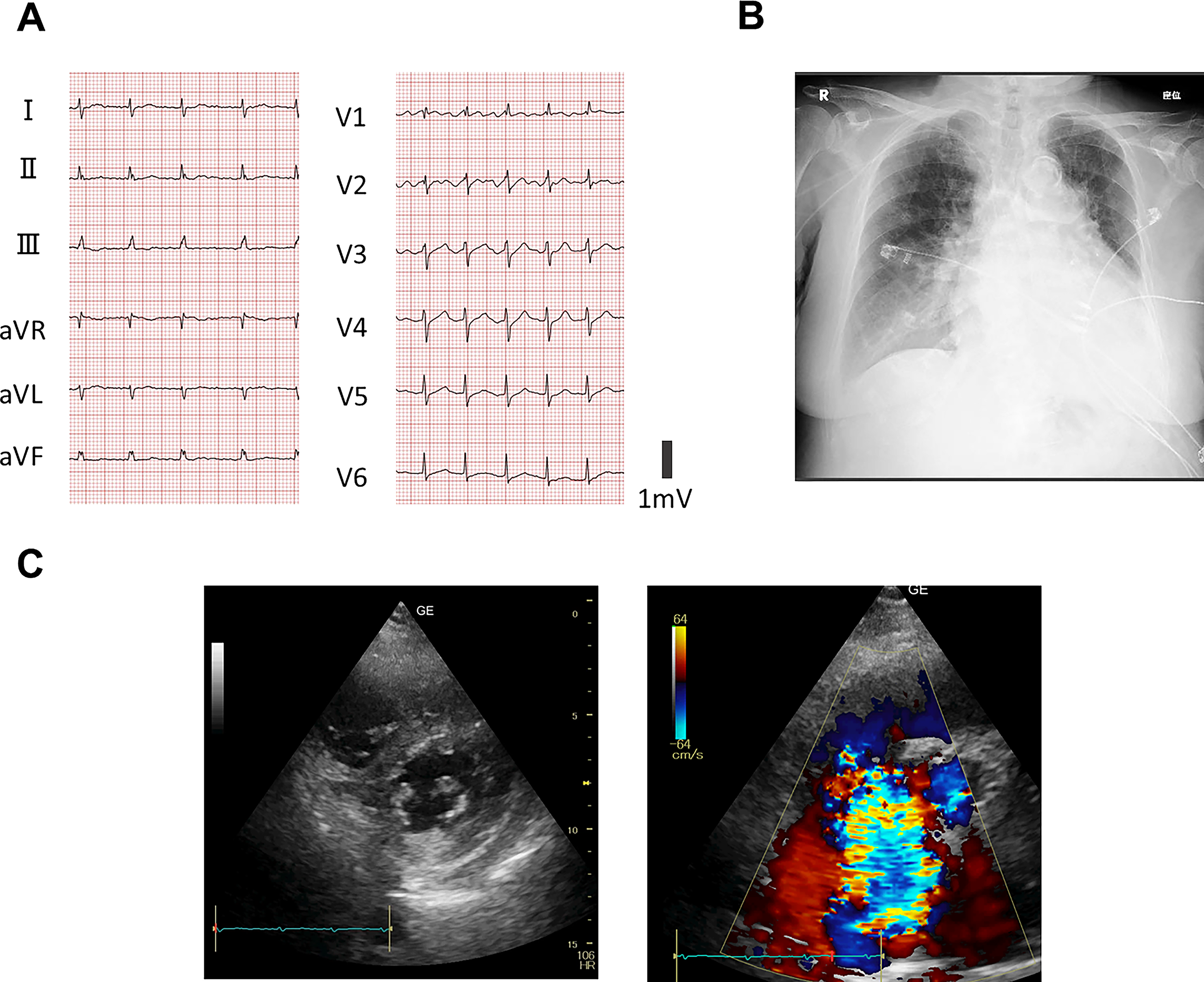
Clinical findings in case 2.
Discussion
In Japan, many patients with advanced heart failure still die in hospitals, and the transition to home-based end-of-life care can be challenging because of limited community resources and coordination systems. Continuous home dobutamine infusion is not commonly feasible in standard home care practice because it requires specialized cardiovascular management. Our home care clinic includes several board-certified cardiologists, allowing us to provide advanced heart failure management and palliative care in a home setting.
Home dobutamine intravenous infusion can contribute to effective palliative care in patients with advanced heart failure. A previous study reported on the long-term home use of dobutamine in patients with end-stage heart failure in Nigeria. 4
Refractory dyspnea is a common and distressing symptom in patients with end-stage heart failure, even when hemodynamics are temporarily maintained with inotropic support. Previous studies have also suggested that opioids may alleviate refractory dyspnea in advanced heart failure without a clear increase in mortality.3,5 In our cases, additional opioid therapy appeared to contribute to symptom relief when dobutamine alone was insufficient.
Our two cases illustrate the feasibility of home-based palliative management using continuous dobutamine infusion combined with opioid therapy in selected patients with advanced heart failure who strongly wished to remain at home during the terminal stage of their illness. Although home inotrope therapy has previously been reported to improve symptoms and reduce rehospitalization in patients with end-stage heart failure, evidence regarding concomitant opioid use in the home setting remains limited, particularly in Japan.
In recent years, palliative care for patients with advanced heart failure has received increasing attention. However, in comparison to patients with advanced malignancy, opportunities for home-based end-of-life care remain limited for patients with heart failure because of unpredictable clinical deterioration, refractory dyspnea, and the need for continuous intravenous treatment. In Japan, although morphine and codeine may be used for refractory dyspnea associated with heart failure, reports describing the combined use of continuous home dobutamine infusion and opioids are scarce. Therefore, we believe that these cases provide clinically relevant information regarding symptom-oriented home care for elderly patients with advanced heart failure.
Dobutamine is frequently used to maintain systemic perfusion and alleviate symptoms in patients with low cardiac output syndrome and advanced heart failure. Previous studies have suggested that home intravenous dobutamine therapy may improve the quality of life and reduce heart failure hospitalization in selected patients. However, symptom control with dobutamine alone may become insufficient during the terminal phase of disease progression. In our cases, opioid therapy was introduced as part of palliative symptom management when persistent discomfort or dyspnea could not be adequately controlled by hemodynamic support alone.
The clinical courses of the two patients differed substantially. Case 1 survived for 99 days after discharge, whereas Case 2 died 5 days after returning home. Several factors may explain these differences. Case 2 had severe pulmonary hypertension, severe tricuspid regurgitation, advanced right-sided heart failure, and a markedly frail clinical condition despite temporary stabilization before discharge. Therefore, although home transition was successfully achieved, her hemodynamic reserve was likely to be extremely limited. These findings emphasize that even when home discharge is feasible, the prognosis of advanced heart failure remains highly unpredictable.
Another important consideration is the selection of opioids. In case 1, transdermal fentanyl was selected because of renal dysfunction and concerns regarding adverse effects related to morphine metabolite accumulation. Although fentanyl is not formally approved in Japan for dyspnea associated with heart failure, informed consent for off-label use was obtained from the patient and family after a careful discussion about the treatment goals and symptom palliation. No clinically significant opioid-related adverse effects were observed in either patient.
This study has several limitations. First, the report describes only two heterogeneous cases, and the therapeutic efficacy of combined dobutamine-opioid therapy could not be established. Second, symptom improvement was assessed clinically, and objective dyspnea scales were not consistently used. Third, the independent contribution of opioids to symptom relief could not be definitively determined because multiple concomitant therapies were administered. In addition, long-term home infusion therapy carries important risks, including catheter-related infections and management difficulties.
The intravenous administration of dobutamine is highly effective in alleviating the symptoms of heart failure. 2 The effects of dobutamine preparations in patients with heart failure have been well studied.
Dobutamine exerts inotropic effects primarily by stimulating myocardial β1-adrenergic receptors, resulting in increased cyclic adenosine monophosphate (cAMP) production and enhanced cardiac contractility. 6 However, chronic sympathetic activation in advanced heart failure induces β-adrenergic receptor downregulation and desensitization, which may reduce responsiveness to catecholamine stimulation over time. 6 Previous experimental and clinical studies have demonstrated decreased β-adrenergic receptor density and impaired adrenergic signaling in the failing myocardium. 7 In addition, prolonged exposure to continuous inotropic therapy may contribute to tachyphylaxis and the progressive attenuation of hemodynamic responsiveness. Recent consensus statements regarding advanced heart failure have emphasized the limited evidence available for long-term continuous inotrope therapy. 8
In the present cases, continuous dobutamine infusion contributed to the temporary stabilization of the hemodynamic status and facilitated discharge to home. However, symptom progression eventually occurred despite ongoing inotropic support, suggesting that the maintenance of systemic perfusion alone may become insufficient during the terminal stage of advanced heart failure. These observations highlight the potential role of opioids as adjunctive symptom-oriented therapy when persistent dyspnea or discomfort cannot be adequately controlled by prolonged inotrope administration alone.
Further investigation is needed to better understand the relationship between prolonged catecholamine exposure, β-receptor regulation, and long-term hemodynamic responsiveness in patients receiving home-based palliative inotrope therapy.
However, because both patients received multiple concomitant medications, the independent contribution of opioids to symptom relief could not be determined. Further studies are needed to clarify the specific role of opioids in combination with dobutamine therapy at home. Nevertheless, we treated patients with end-stage heart failure using continuous dobutamine infusion combined with opioids. This treatment strategy allows patients with end-stage heart failure to spend the remainder of their lives at home with less discomfort.
In conclusion, combined home-based dobutamine infusion and opioid therapy may represent a feasible palliative treatment option for selected patients with advanced heart failure who wish to remain at home and avoid hospitalization. Further studies are needed to clarify the appropriate patient selection, symptom outcomes, and safety considerations in this clinical setting.
Footnotes
Acknowledgments
The authors thank Brian Quinn of Japan Medical Communication for his professional English language editing and support in article preparation. The authors also used ChatGPT (OpenAI) for language assistance during article preparation. All clinical interpretations and final article content were reviewed and approved by the authors.
Ethics Statement
The corresponding author is a Board-Certified Palliative Care Physician certified by the Japanese Society for Palliative Medicine and was directly involved in the management of both patients. Goals-of-care discussions were conducted by the referring cardiologists, homecare physicians, patients, and family members before discharge. The patients clearly expressed their wish to spend their remaining time at home rather than in the hospital, and home-based palliative care was initiated in accordance with their preferences. Decisions regarding the continuation of dobutamine infusion and the use of opioids for symptom relief were made through discussions among the patients, their families, treating physicians, and home-care physicians. Written informed consent for the publication of this case report and accompanying images was obtained from the patients or their families. All personal information was anonymized to protect patient privacy.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.