
Abstract
Background:
We sought to analyze the effect of a palliative care intervention on quality of life (QoL) in patients with fibrotic interstitial lung disease (fILD).
Design:
This was a prospective observational study including 14 patients with fILD treated with a bundle of care provided by multidisciplinary specialists in pain and palliative care, a psychologist, physical therapists, and a nutritionist, with all patients initiating 10 mg of morphine sulfate. Measurements at baseline, 30 days, and 90 days included cough, dyspnea, pain, tiredness, nausea, depression, anxiety, sleepiness, appetite, and difficulty sleeping. QoL was recorded using the modified St. George’s Respiratory Questionnaire (SGRQ-1). Change over time in each endpoint was analyzed.
Results:
Baseline assessment reflected an impaired QoL (median SGRQ-1, 91 points). All symptom scores improved at 90 days, with a statistically significant and clinically meaningful 20-point decrease in the SGRQ-1 (p = 0.001).
Conclusion:
Palliative care intervention improves symptom and QoL in fILD.
Background
Fibrotic interstitial lung disease (fILD) is frequently progressive and unpredictable.1–3 The main features of fILD are declining pulmonary function, worsening symptoms (cough, severe dyspnea, anxiety, panic, and depression) and health-related quality of life (HRQoL), and early mortality.4–6 Patients with fILD may have the same symptom burden and need of medical care as terminal cancer patients. 7 There are several palliative interventions that can mitigate the impact of end-stage lung disease to improve symptoms and quality of life (QoL), with mortality benefit also observed in some populations such as terminal cancer. 8 However, evidence supporting the pharmacological and nonpharmacological interventions provided by the palliative care team is limited, with inconsistent results particularly for patients with fibrotic ILD. 9 The aim of this study was therefore to analyze the impact of a palliative bundle of care in patients with fILD. We hypothetized that the interventions suggested by the palliative care team would improve symptoms and HRQoL in patients with fILD.
Methods
Selection and description of participants
This was a prospective observational study of patients with fibrotic ILD referred to the Clinica del Dolor y Cuidados Paliativos (Pain and Palliative Care Clinic) from the Hospital Regional de Alta Especialidad de la Península de Yucatán IMSS–Bienestar between March 2019 and February 2020. The research and ethics committees from the Hospital Regional de Alta Especialidad de la Península de Yucatán IMSS–Bienestar approved the protocol (number 2019-018). All patients provided informed consent.
Interventions
The interventions of the Pain and Palliative Care Clinic team consisted of a bundle of care provided by multidisciplinary specialists in pain and palliative care, a psychologist with a Master’s in thanatology, a physical therapist, and a nutritionist. The pharmacological options included opioids and neuromodulators gamma-aminobutyric acid analogs, with doses of morphine sulfate from 5 mg to 30 mg orally per day, pregabalin 75 mg to 150 mg, and gabapentin 300 mg per day. The most responsible physician for each patient provided the final treatment recommendation.
Measurements
Patients were evaluated at baseline and two follow-up appointments at 30 and 90 days. Baseline demographic variables included age, sex, anthropometric measurements, education, comorbidities, and functional capacity (mobility, cardiac, and pulmonary, and Karnofsky index). Severity was recorded at all timepoints for cough, dyspnea, pain, tiredness, nausea, sleepiness, appetite, and difficulty sleeping using the Edmonton Symptom Assessment System (ESAS), Visual Analogue Scale (VAS), and modified Medical Research Council (mMRC) scale. QoL was measured using the EuroQol-5D and modified Saint George’s Respiratory Questionnaire (SGRQ-1).10–12
Statistical analysis
A Kolmogorov-Smirnov test confirmed a nonparametric distribution. Categorical variables are shown as frequencies with percentages, whereas the continuous variables are shown as medians with an interquartile range (IQR). Given the unknown trajectory over time, differences across the three timepoints were evaluated using Kruskal-Wallis test with a post hoc Chi-square adjustment. In all analyses, a two-sided p value <0.05 was considered statistically significant. Data were analyzed using STATA Version 18 software (StataCorp, College Station, Tx. the USA).
Results
Sample demographic and clinical characteristics
We included 14 patients during the study period, with all patients being followed up at 30 and 90 days (Table 1). Median age was 63 years (54–71), and 85% were female. The most frequent etiology associated with fILD was connective tissue disease (64%), with 44% of these having rheumatoid arthritis. Only 14% of patients had a diagnosis of IPF. The median Karnofsky index was 65 (50–70), reflecting the requirement of occasional assistance but with the ability to self-manage most personal needs. Lung function was severely reduced with the median FVC of 44%, (33–47) and a 6-minute walk distance of 328 meters (283–360). All patients reported cough, dyspnea, and fatigue at baseline.
General Characteristics of the Population under Study (n = 14)
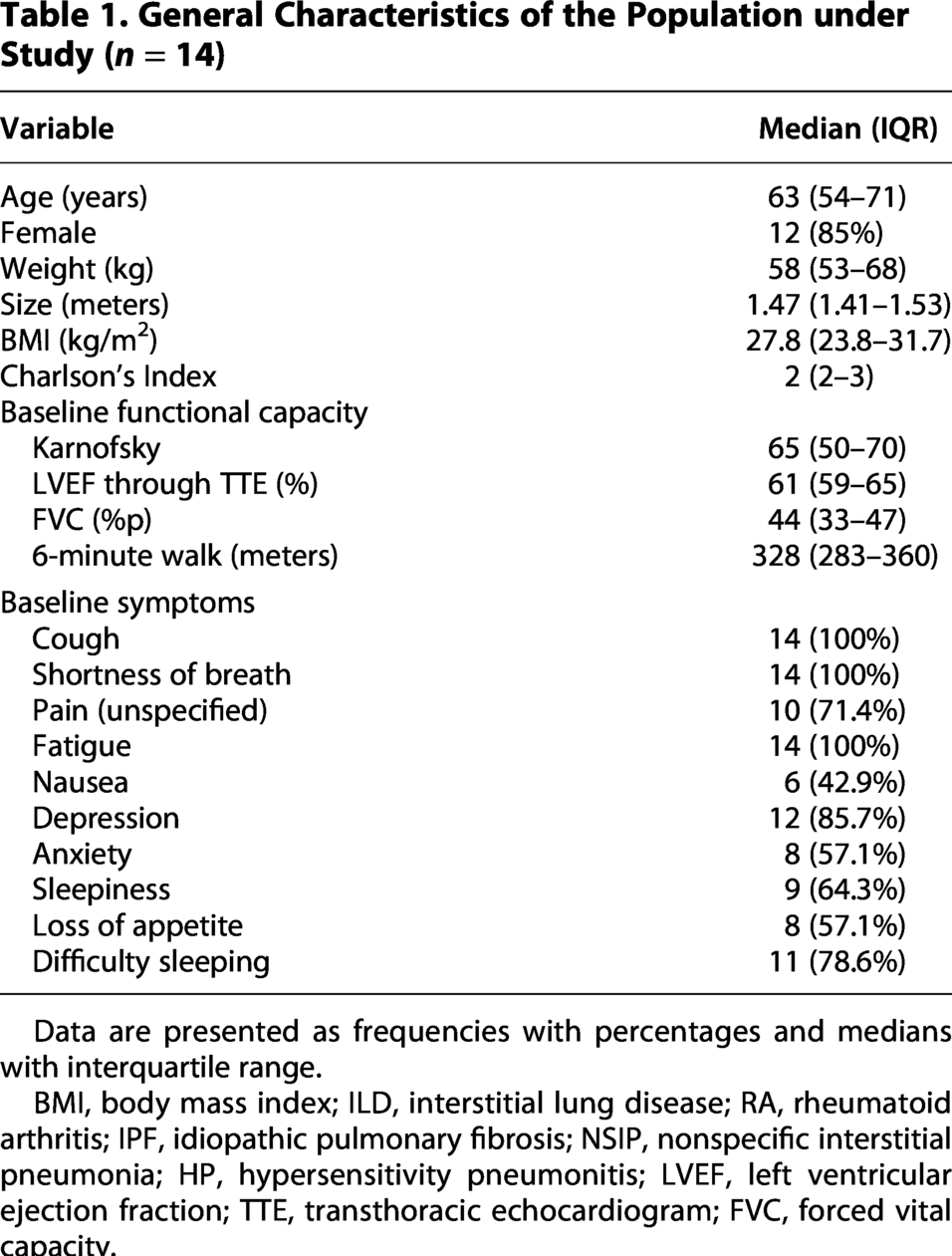
Data are presented as frequencies with percentages and medians with interquartile range.
BMI, body mass index; ILD, interstitial lung disease; RA, rheumatoid arthritis; IPF, idiopathic pulmonary fibrosis; NSIP, nonspecific interstitial pneumonia; HP, hypersensitivity pneumonitis; LVEF, left ventricular ejection fraction; TTE, transthoracic echocardiogram; FVC, forced vital capacity.
Interventions
All patients received morphine sulfate 10 mg (10–10) after baseline evaluation, which was titrated up according to the therapeutic response and presence of drug-associated effects. At the 30-day visit, there was a slightly increase in morphine doses to 12.5 mg (10–15) and neuromodulators were prescribed in 7 patients due to the presence of neuropathic pain and/or persistence of nocturnal cough, including 4 patients receiving gabapentin 300 mg daily and 3 patients receiving pregabalin 75 mg daily. The median morphine dose at 90 days was 10 mg (10–20).
Change in symptoms and quality of life
There was statistically significant improvement in all symptoms at days 30 and 90 (Table 2). The improvements were seen over time in dyspnea (mMRC scale, p < 0.001) and cough (p < 0.001). The ESAS questionnaire also showed improvement in tiredness/fatigue (p = 0.002), appetite (p < 0.001), difficulty sleeping (p = 0.015), and sleepiness (p = 0.041) (Fig. 1). There was improvement in QoL and well-being at 30 and 90 days, particularly in the SGRQ-1 (p = 0.001), which improved by 20 points from baseline to 90-day follow-up (91.2 points, IQR 84.3–96 vs. 71.3 points, IQR 55.9–75.6, p = 0.006) (Fig. 2).
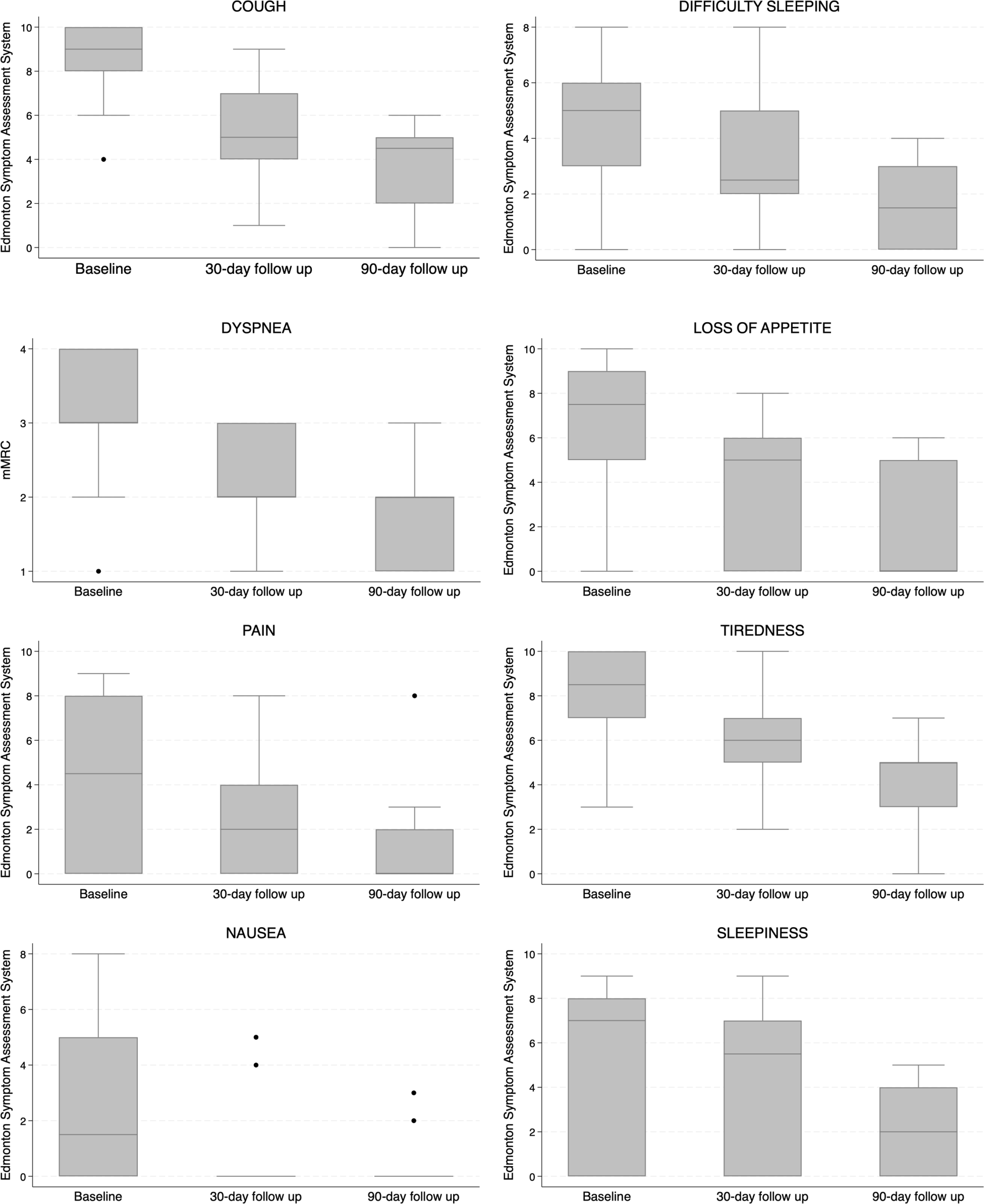
Changes in symptom perception at follow-up with palliative care intervention.
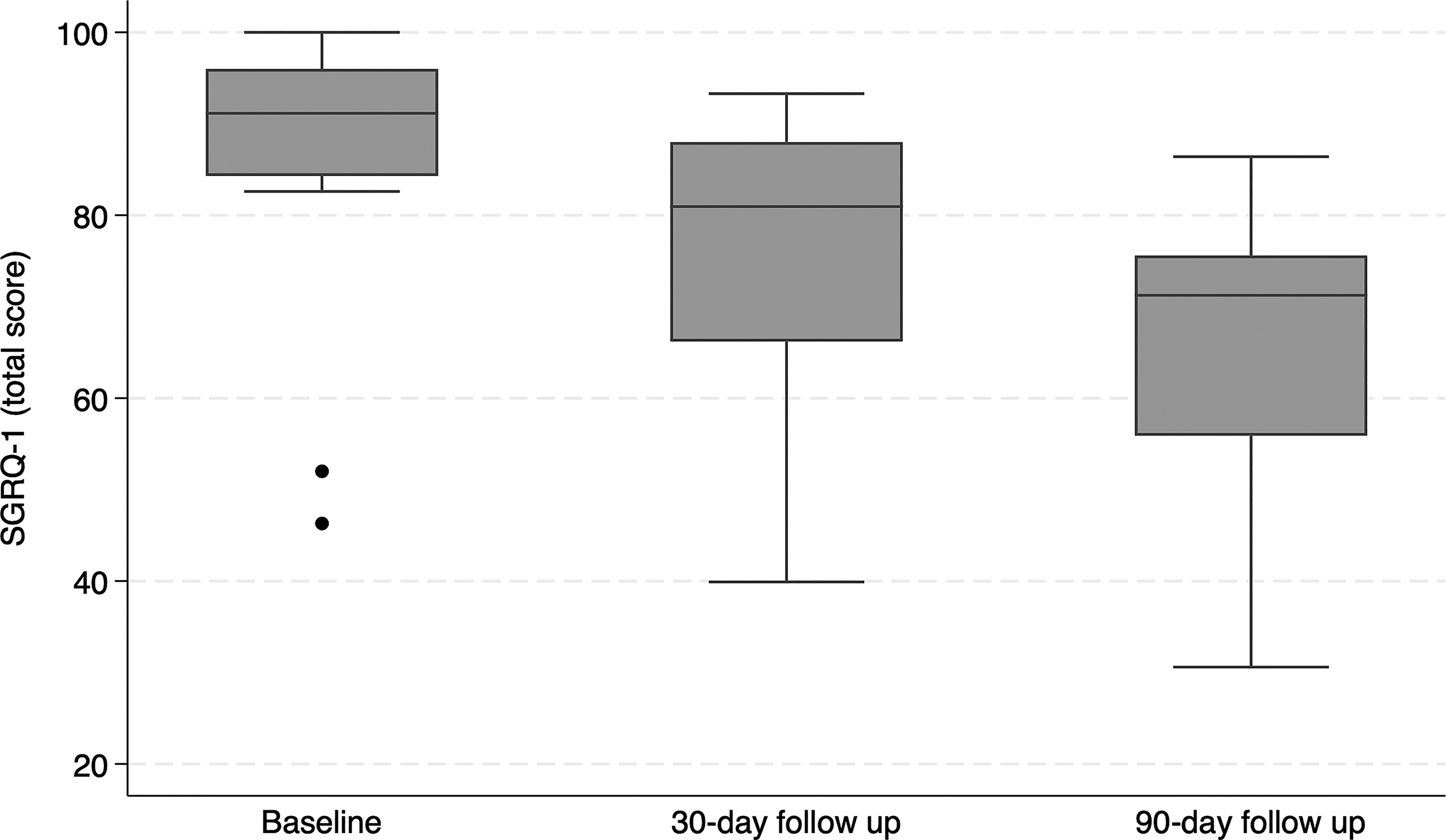
Quality of life evaluation, perceived by the patients through the SGRQ-1 (Saint-George Respiratory Questionnaire-1).
Change in Symptoms and Quality of Life over Time
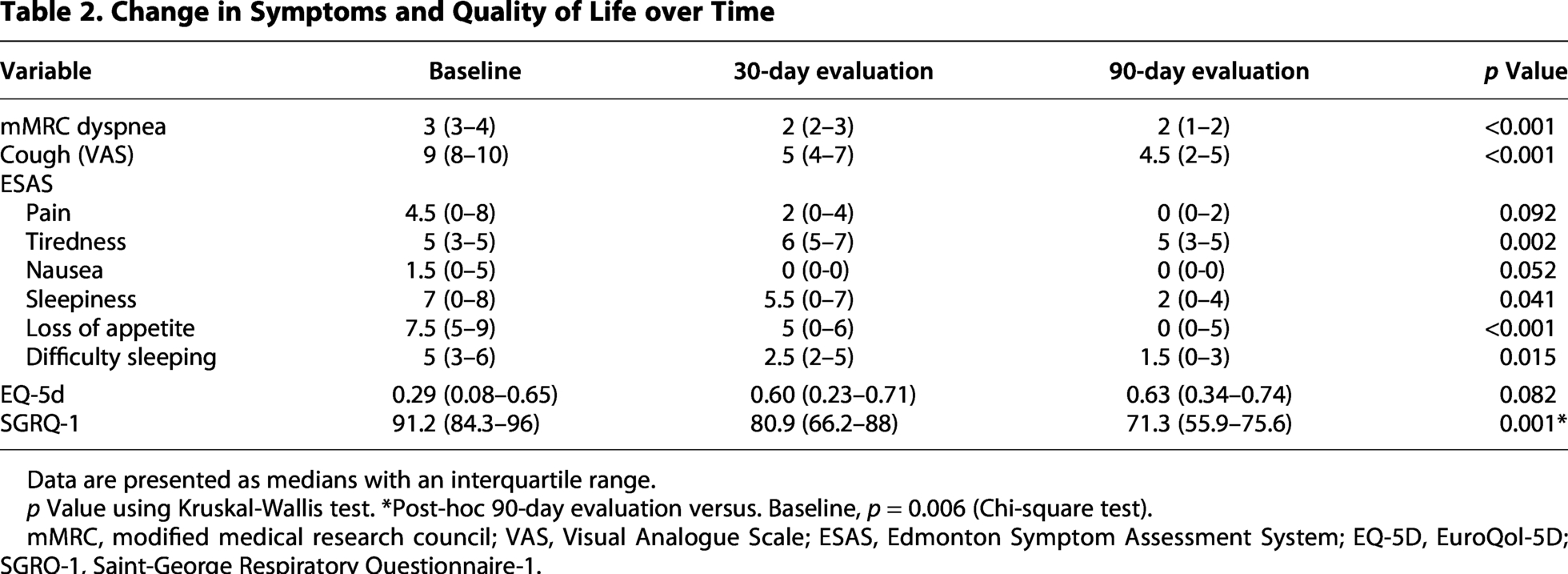
Data are presented as medians with an interquartile range.
p Value using Kruskal-Wallis test. *Post-hoc 90-day evaluation versus. Baseline, p = 0.006 (Chi-square test).
mMRC, modified medical research council; VAS, Visual Analogue Scale; ESAS, Edmonton Symptom Assessment System; EQ-5D, EuroQol-5D; SGRQ-1, Saint-George Respiratory Questionnaire-1.
Discussion
Fibrotic ILD has a substantial impact on symptoms, QoL, and survival.3,4,6 Palliative care has potential to mitigate the consequences of severe fILD; however, this intervention is rarely implemented in patients with fILD, in part due to limited and inconsistent results in the previous literature. In this study, we show a consistent and clinically meaningful benefit of common palliative care interventions on symptoms and QoL in patients with fILD.
Early comprehensive palliative support and management of refractory dyspnea significantly improved the perception of symptoms in a previous study of 105 patients, including 19 with ILD. Similar to our study, this previous study employed a multidisciplinary team approach that included multiple potential interventions directed by experts in respiratory physiotherapy, occupational therapy, and palliative care. This multidisciplinary team evaluated and treated the physical, emotional or psychological, and spiritual aspects in what was essentially a bundle of care. Like the present study, it is unclear what components of care were most helpful. 8 In contrast, another study of 36 patients with fILD did not find a benefit of morphine on dyspnea; however, this endpoint was assessed only after seven days of treatment. 13
We demonstrated that implementing palliative care and particularly considering the addition of morphine is associated with improved dyspnea and HRQoL in patients with fILD. 14 This benefit was sustained at 30- and 90-day follow-ups. There did not appear to be implications in the respiratory function of the patients, which is a frequent concern that often limits prescription of opioids in clinical practice. Our findings are also consistent with previous evidence showing that opioids improve the severity of cough, dyspnea, and anxiety without increasing the risk of respiratory impairment in patients with advanced respiratory disease.15–17 Beyond the improvement in dyspnea, we also observed improvements in sleep quality and anxiety, which is similar to previous studies.16,18
The optimal timing of referral to PC is unclear; however, the sustained benefits we observed at 30 and 90 days of follow-up suggest early referral has limited downside. Early referral to PC would also support better establishment of a trustful relationship and better ability for patients and caregivers to participate in critical decision-making. 19 Early referral also provides greater potential for benefit given the need to titrate some potential medications to effect. Despite the likely benefit, before dying, only 13.7% of the patients with a non-cancer disease have received palliative care, and rarely being offered to patients with fILD. Unfortunately, the lack of palliative care support remains as high as 70% even in the 30 days before death. 20
This analysis is limited by the small sample size; however, this is countered by the statistically significant benefits suggesting adequate power, including the sustained benefit of the intervention over three months of follow-up. We did not repeat pulmonary function measurements to understand whether symptom improvement was independent of any potential increase in pulmonary function; however, the progressive nature of fILD makes this an unlikely possibility. The absence of a placebo group is similarly mitigated by the large and persistent benefits in the context of what is almost universally a progressive disease. Finally, the doses and types of drugs were adjusted based on patient needs as assessed by the treating physicians without a standardized protocol, resulting in some lack of certainty as to what components of care are most beneficial.
In conclusion, implementing a bundle of palliative care in patients with fILD was associated with a decrease in symptoms and improvement in HRQoL. The sustained benefits over 90 days of follow-up suggest early intervention may be appropriate to yield the greatest patient benefit. Additional studies with a larger sample size and greater standardization of interventions are necessary to confirm and expand upon the benefit observed in the present study.
Authors’ Contributions
The author(s) meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE).
Ethical Approval and Informed Consent Statements
The research and ethics committees from the hospital approved the protocol (number 2019-018). All the patients provided informed consent.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Disclaimers
The authors declare that the views expressed in the present article are their own without any representations for an official position of an institution or funder.
Footnotes
Author Disclosure Statement
The authors declare they do not have any conflict of interest regarding the present article.
Funding Information
The authors declare that they did not receive any type of support to carry out this research. Also, the authors did not receive payment related to the development of this Investigation.