
Abstract
The purpose of this study was to evaluate the effect of perioperative discontinuation of antiplatelet and anticoagulation therapy (AAT) on in-hospital mortality, functional outcome, and recurrence in patients with chronic subdural hematoma (CSDH) with prior AAT use, compared to patients without AAT. We retrospectively analyzed data from patients with symptomatic CSDH who underwent surgery in our department between June 2012 and December 2023. Prior AAT was discontinued at hospital admission and reinitiated 3 weeks postoperatively if CSDH resolution was complete. Clinical and neurological status at admission and discharge were assessed using the modified Rankin Scale, with scores >3 defined as a poor outcome. Among 852 surgically treated CSDH patients (mean age 75.2 years; female-to-male ratio 1:2.1), univariate analysis revealed that prior AAT use was significantly associated with higher in-hospital mortality (p = 0.043) and poor functional outcome (p < 0.001), but not with recurrence (p = 0.434). However, multivariate analysis demonstrated that prior AAT use was not an independent predictor of mortality (p = 0.099) or poor outcome (p = 0.956). Notably, patients with prior (acetylsalicylic acid) aspirin use exhibited significantly lower recurrence rates compared to patients without AAT (p = 0.012) and to the general cohort (p = 0.003). The multivariate analysis showed that prior aspirin use was an independent predictor of reduced recurrence rates (p = 0.015, adjusted odds ratio = 0.504; 95% confidence interval 0.290–0.877). This large-scale study supports the safety of perioperative AAT discontinuation in CSDH patients, showing no significant differences in in-hospital mortality, functional outcome, or recurrence compared to patients without AAT. Intriguingly, prior aspirin therapy was associated with reduced recurrence, suggesting a potential protective role.
Introduction
Chronic subdural hematoma (CSDH) is a frequent neurosurgical condition, particularly in the elderly, characterized by blood accumulation in the subdural space. Its incidence is rising worldwide, largely due to population aging and the increasing use of antiplatelet and anticoagulation therapy (AAT) for the prevention of cardiovascular and cerebrovascular diseases.1–3 The proportion of CSDH patients receiving AAT varies across studies, ranging from 30% to 60%.4,5 Perioperative management in this group is challenging. While discontinuation of AAT is routinely undertaken to reduce the risk of postoperative bleeding, it may simultaneously elevate the risk of thromboembolic events.6,7
Evidence regarding the impact of AAT on surgical outcomes in CSDH is conflicting. Some studies associate AAT with higher rates of postoperative recurrence and mortality,8–10 whereas others report no significant influence on outcomes,11,12 leaving the safety and optimal timing of surgery in this population uncertain.
The present study aims to clarify whether surgical treatment of CSDH after perioperative AAT discontinuation is safe. Specifically, we investigate whether stopping AAT before surgery influences in-hospital mortality, functional outcome, or recurrence risk compared with patients not receiving AAT. Leveraging a large patient cohort, this study seeks to provide robust evidence to guide perioperative decision-making in CSDH, balancing the risks of hemorrhagic and thromboembolic complications.
Methods
Study population
From June 2012 to December 2023, we evaluated 938 consecutive patients aged ≥18 years with symptomatic CSDH admitted to our institution for eligibility in this study. Patients with a history of brain surgery (intracranial tumor, acute subdural hematoma, aneurysm clipping, CSDH) or ventriculoperitoneal shunt and concomitant acute lesions (intracranial hemorrhage, traumatic brain injury) were excluded. The study flowchart presents the main exclusion criteria in detail (Fig. 1). This retrospective study was performed in accordance with the ethical standards of the institutional research committee and the Code of Ethics of the World Medical Association (Declaration of Helsinki). The Institutional Review Board approved the study protocol (Medical Faculty, University of Duisburg-Essen, Registration number: 22-10763-BO). All supporting data are available within this article. Anonymized data will be shared upon request from any qualified investigator.

Study flowchart.
Routine clinical care and treatment protocol of CSDH
AAT was discontinued upon hospital admission and re-established 3 weeks after surgery in case of complete resolution of the hematoma. In all patients, hematoma evacuation was performed under general anesthesia using either a burr hole or a minicraniotomy with placement of a subdural drain whenever possible. Prior to surgery, a single dose of antibiotics was administered prophylactically. Postoperatively, patients spent 48 h in the intermediate care unit or the intensive care unit and remained on bed rest. On the second postoperative day, a cranial computer tomography scan was performed, and the subdural drain was removed. Patients were usually discharged around day 7 after surgery.
Patient data collection
The patients’ medical records were retrospectively reviewed to collect data on: age, sex, Charlson comorbidity index (CCI), American Society of Anesthesiologists Physical Status Classification System (ASA status), history of a recent trauma, as well as comorbidities such as epilepsy, dementia, arterial hypertension, diabetes mellitus, chronic kidney disease (CKD), atrial fibrillation (AF), chronic heart disease (CHD), cerebral vascular accident or transient ischemic accident (CVA/TIA), thrombophilia, AAT, seizure 24 h prior to admission, neurological condition, and functional status on admission using the Glasgow coma scale (GCS), the Markwalder grading scale, and the modified Rankin Scale (mRS), respectively. Furthermore, CSDH location (unilateral vs. bilateral), operative technique (burr hole vs. minicraniotomy) and preoperative hemoglobin level, and platelet count were analyzed. During hospitalization, neurological condition on discharge, in-hospital mortality, and postoperative complications—including postoperative bleeding, postoperative seizure, recurrence, myocardial infarction, pulmonary embolism, and postoperative stroke were thoroughly assessed. Recurrence was defined as an episode of radiological hematoma progression, with or without development of symptoms, that required reoperation. Functional status was documented at discharge, with an mRS score >3 considered indicative of a poor outcome. All data were verified by the senior author (M.C.) prior to analysis.
Definition of AAT discontinuation
AAT was discontinued prior to surgery (acetylsalicylic acid [aspirin] and clopidogrel 5–7 days, direct oral anticoagulants [DOAC] 48 h, and vitamin K antagonists until the Quick value exceeded 70%, i.e., International normalised ratio < 1.3). AAT was reinitiated 3 weeks after surgery if the hematoma had completely resolved. In cases of neurological deterioration during the discontinuation period, desmopressin or prothrombin, proconvertin, Stuart factor and antihemophilic factor B was administered to reverse the effects of aspirin and vitamin K antagonists, respectively, to normalize coagulation status.
Statistical analyses
All analyses were performed using SPSS version 29.0.2.0 (IBM, Chicago, IL). Categorical data are presented as frequencies and percentages. Normally distributed continuous variables are expressed as the mean and standard deviation. Nonnormally distributed continuous variables are expressed as the median and interquartile range. The Mann–Whitney U test was used to assess statistical associations between AAT and other continuous variables. Associations between AAT and other dichotomous variables were determined using the chi-square test and the Fisher’s exact test (when the expected cell frequency was <5). The factors in the univariate analysis, which were associated with the study endpoints (in-hospital mortality, functional outcome at discharge and recurrence) with a p value < 0.1, were implemented in the multivariate analysis. Binomial logistic regression (forward likelihood ratio method) was used to determine predictors of the study endpoints, and adjusted odds ratio (aOR) and 95% confidence intervals (95% CI) were calculated. Prediction models based on the results of the multivariate analysis were computed. p-Values < 0.05 in two-sided testing were considered statistically significant. Receiver operating characteristic (ROC) curve analyses were conducted to determine the accuracy of prediction models.
Results
Baseline characteristics
The selection process of the patients eligible for this study is presented in Figure 1. Accordingly, 852 patients (mean age: 75.2 ± 12 years, female/male: 1/2.1, CCI: 4.4 ± 2.1, ASA status: 2.8 ± 0.6) met the inclusion criteria. Of the included patients, 186 had AF (21.8%), 160 had CHD (18.8%), 84 had CKD (10.2%), and 443 received AAT (52%), which was perioperatively discontinued. Prior to admission, 134 patients (15.7%) were diagnosed with dementia, 40 patients (4.7%) with epilepsy, and 650 (76.3%) reported a recent head trauma. At admission, 393 patients (46.1%) had a GCS score < 15, and 400 individuals (46.9%) had a poor mRS score (Table 1).
Baseline Characteristics
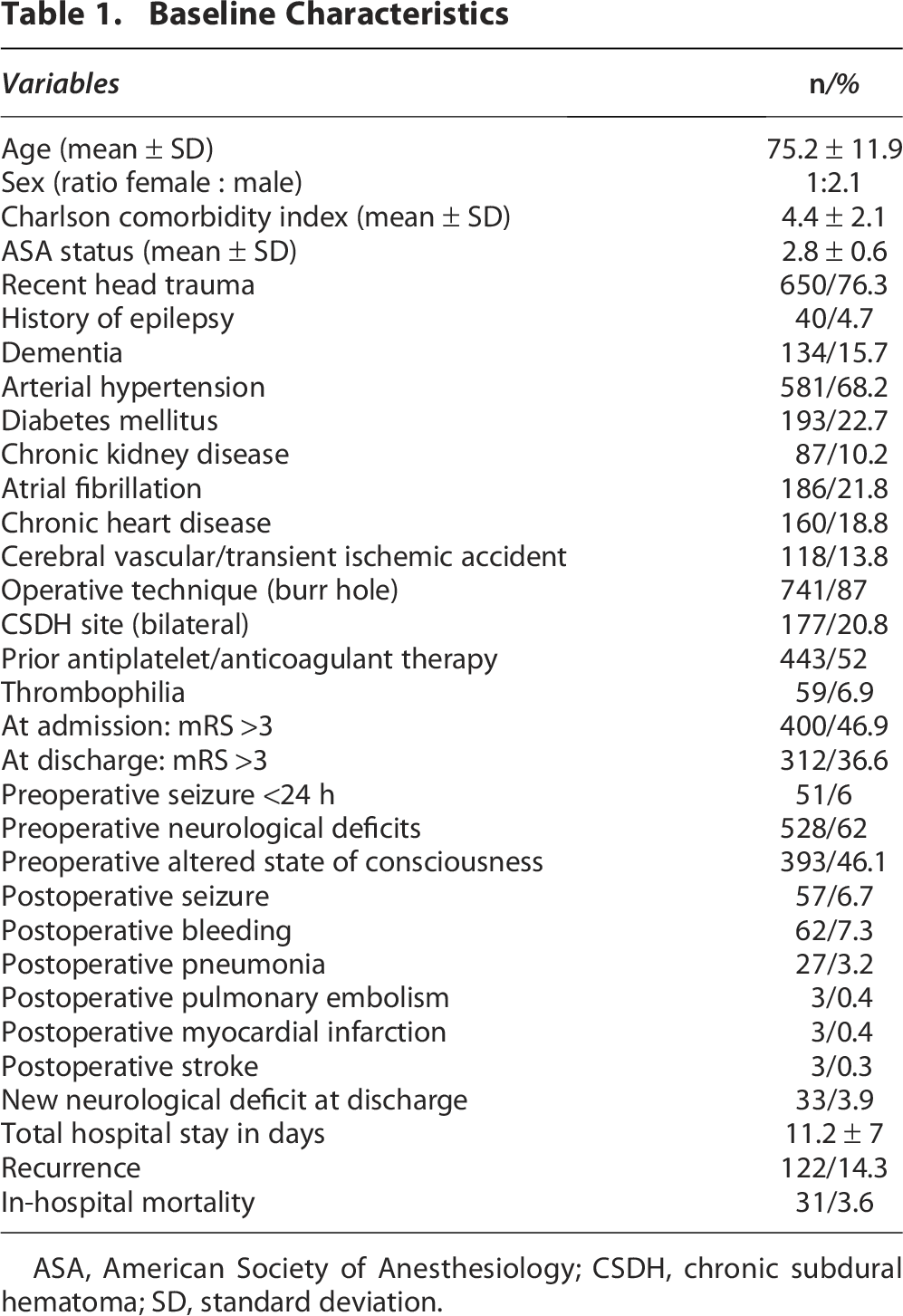
ASA, American Society of Anesthesiology; CSDH, chronic subdural hematoma; SD, standard deviation.
Characteristics and predictors of in-hospital mortality
In-hospital mortality was observed in 31 patients (3.6%). In the univariate analysis, in-hospital mortality was statistically significantly associated with prior AAT use (p = 0.043), age (p = 0.005), CCI (p < 0.001), ASA status (p = 0.001), dementia (p = 0.005), CKD (p = 0.031), thrombophilia (p = 0.016), preoperative mRS (p < 0.001), preoperative GCS score (p < 0.001), preoperative Markwalder grading (p < 0.001), preoperative platelet count (p < 0.001), preoperative hemoglobin level (p = 0.003), minicraniotomy (p = 0.013), and postoperative bleeding (p = 0.005). Furthermore, epilepsy (p = 0.052), arterial hypertension (p = 0.075), and AF (p = 0.075) showed only a non-significant statistical trend. After adjusting for all confounders, binomial logistic regression revealed that prior AAT use does not predict in-hospital mortality (p = 0.099) (Table 2 and Fig. 2A). A ROC curve analysis determined the model’s discriminative capacity and was excellent with an area under the curve (AUC) of 0.87 (95% CI 0.78–0.95) (Fig. 2B).
Independent predictors of mortality do not include prior AAT use.
Univariate and Multivariate Analysis of Predictors of in-Hospital Mortality
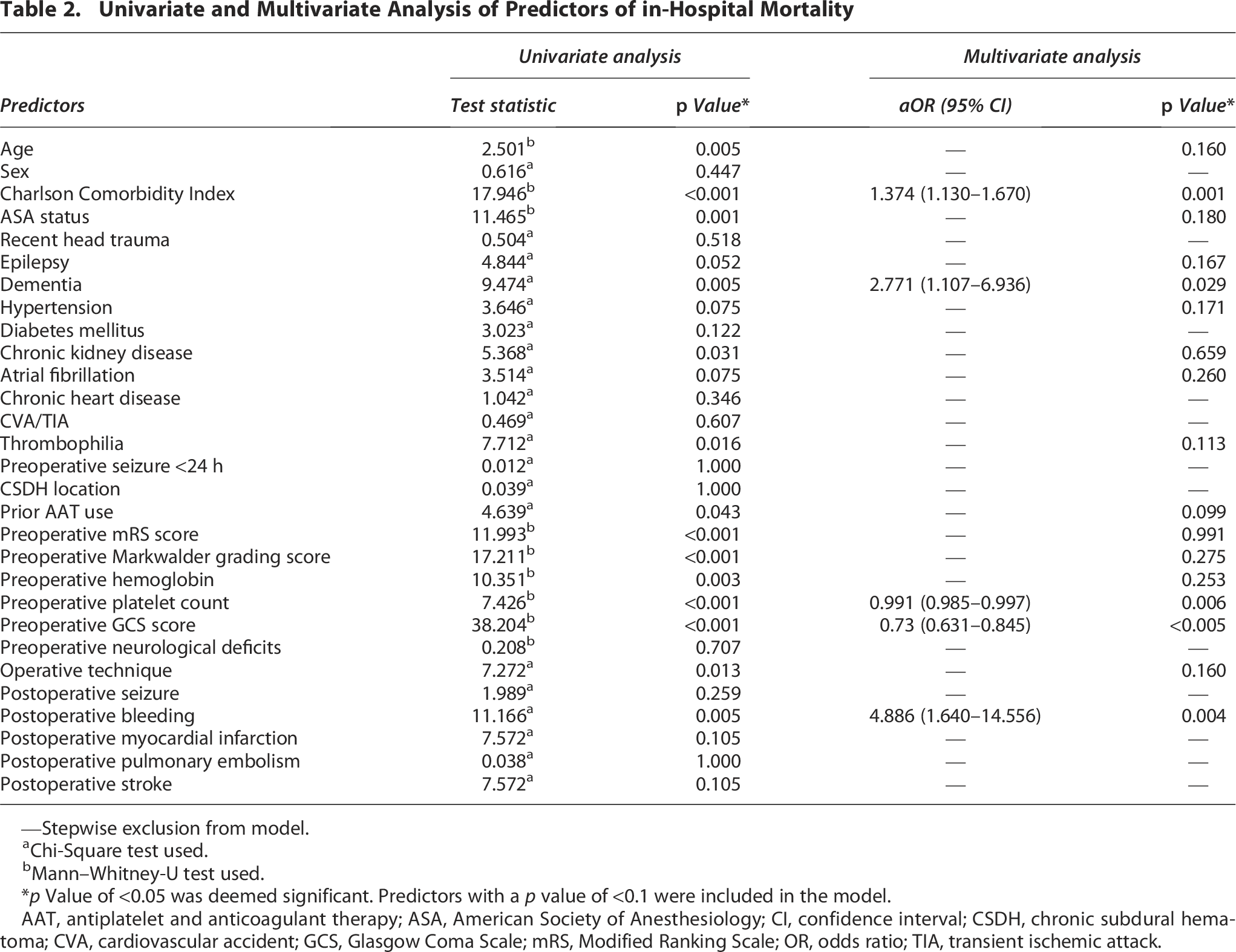
—Stepwise exclusion from model.
Chi-Square test used.
Mann–Whitney-U test used.
*p Value of <0.05 was deemed significant. Predictors with a p value of <0.1 were included in the model.
AAT, antiplatelet and anticoagulant therapy; ASA, American Society of Anesthesiology; CI, confidence interval; CSDH, chronic subdural hematoma; CVA, cardiovascular accident; GCS, Glasgow Coma Scale; mRS, Modified Ranking Scale; OR, odds ratio; TIA, transient ischemic attack.
Characteristics and predictors of functional outcome at discharge
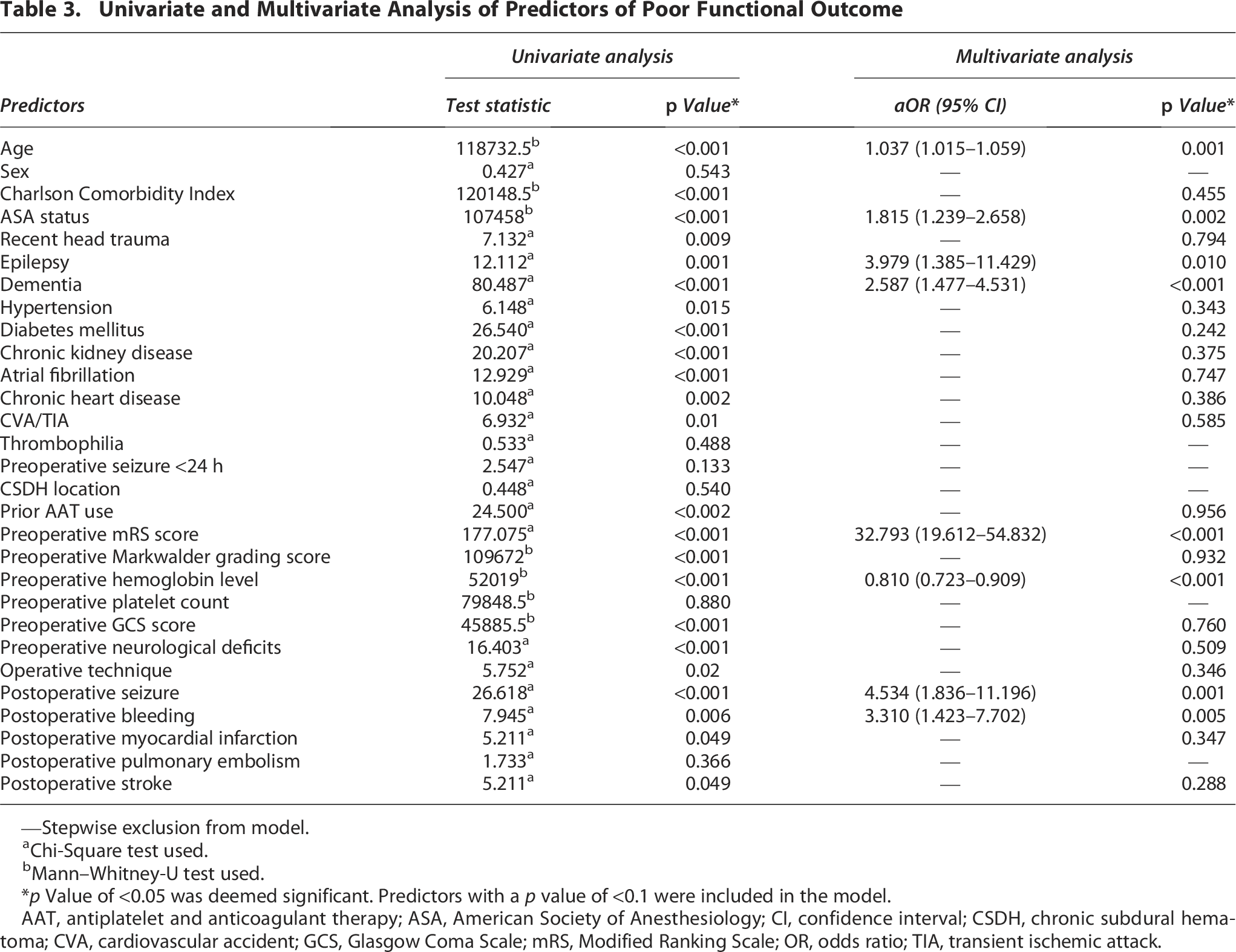
At discharge, 312 individuals (36.6%) had a poor outcome. In the univariate analysis, functional outcome at discharge was statistically significantly associated with prior AAT use (p < 0.001), age (p < 0.001), CCI (p < 0.001), ASA status (p = 0.001), recent head trauma (p = 0.009), epilepsy (p < 0.001), dementia (p < 0.001), arterial hypertension (p = 0.015), diabetes mellitus (p < 0.001), CKD (p < 0.001), AF (p < 0.001), CHD (p = 0.002), CVA/TIA (p = 0.01), preoperative neurological deficits (p < 0.001), preoperative GCS-score (p < 0.001), preoperative Markwalder grading scale (p < 0.001), preoperative mRS (p < 0.001), preoperative hemoglobin level (p < 0.001), operative technique (p = 0.02), postoperative bleeding (p = 0.006), postoperative seizure (p < 0.001), postoperative myocardial infarction (p = 0.049), and postoperative stroke (p = 0.049). After adjusting for all confounders, binomial logistic regression revealed that prior AAT use does not predict functional outcome at discharge (p = 0.956) (Table 3 and Fig. 3A). A ROC curve analysis determined the model’s discriminative capacity and was outstanding with an AUC of 0.92 (95% CI 0.90–0.94) (Fig. 3B).
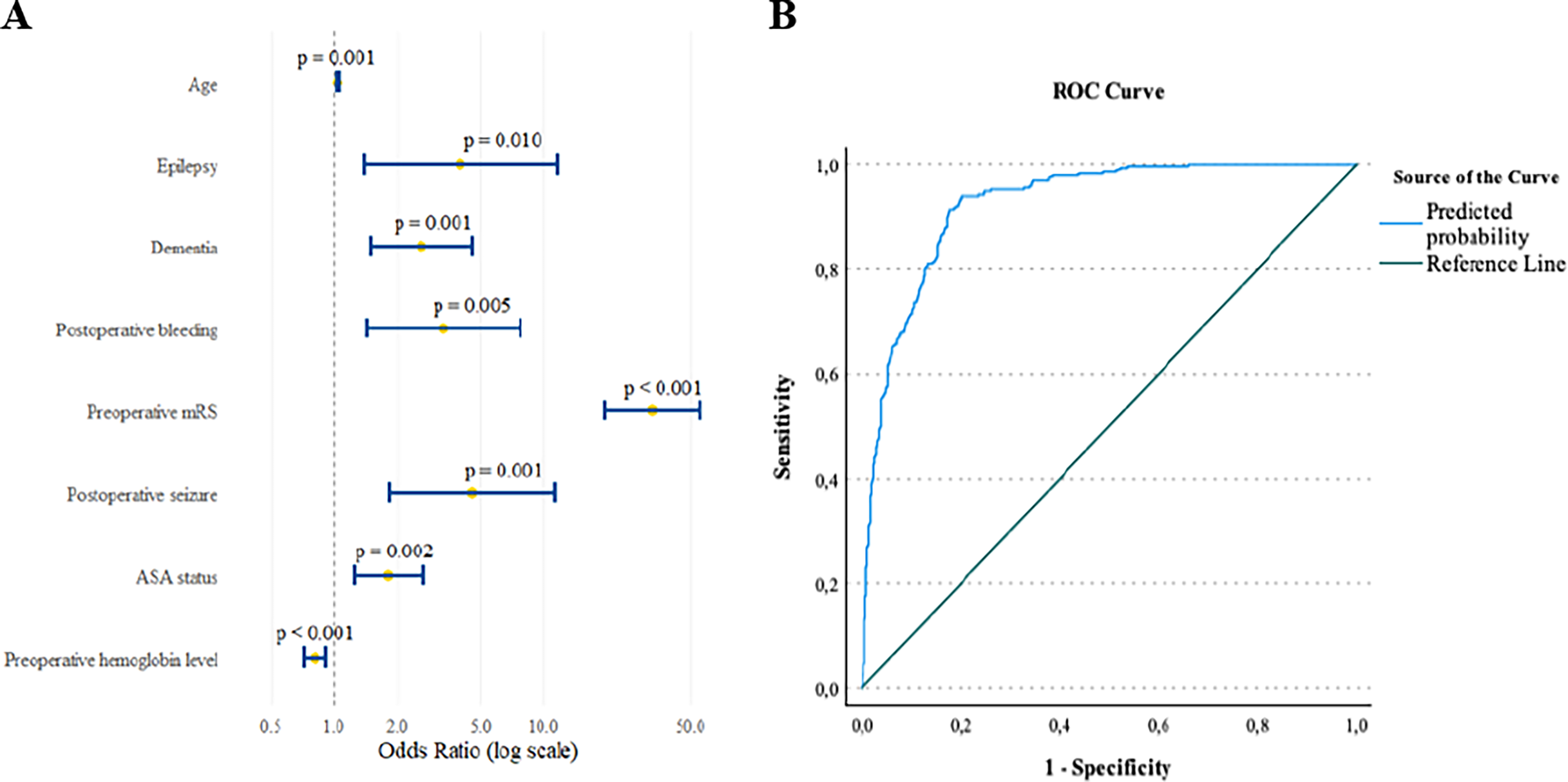
Independent predictors of poor functional outcome do not include prior AAT use.
Univariate and Multivariate Analysis of Predictors of Poor Functional Outcome
—Stepwise exclusion from model.
Chi-Square test used.
Mann–Whitney-U test used.
*p Value of <0.05 was deemed significant. Predictors with a p value of <0.1 were included in the model.
AAT, antiplatelet and anticoagulant therapy; ASA, American Society of Anesthesiology; CI, confidence interval; CSDH, chronic subdural hematoma; CVA, cardiovascular accident; GCS, Glasgow Coma Scale; mRS, Modified Ranking Scale; OR, odds ratio; TIA, transient ischemic attack.
Characteristics and predictors of recurrence
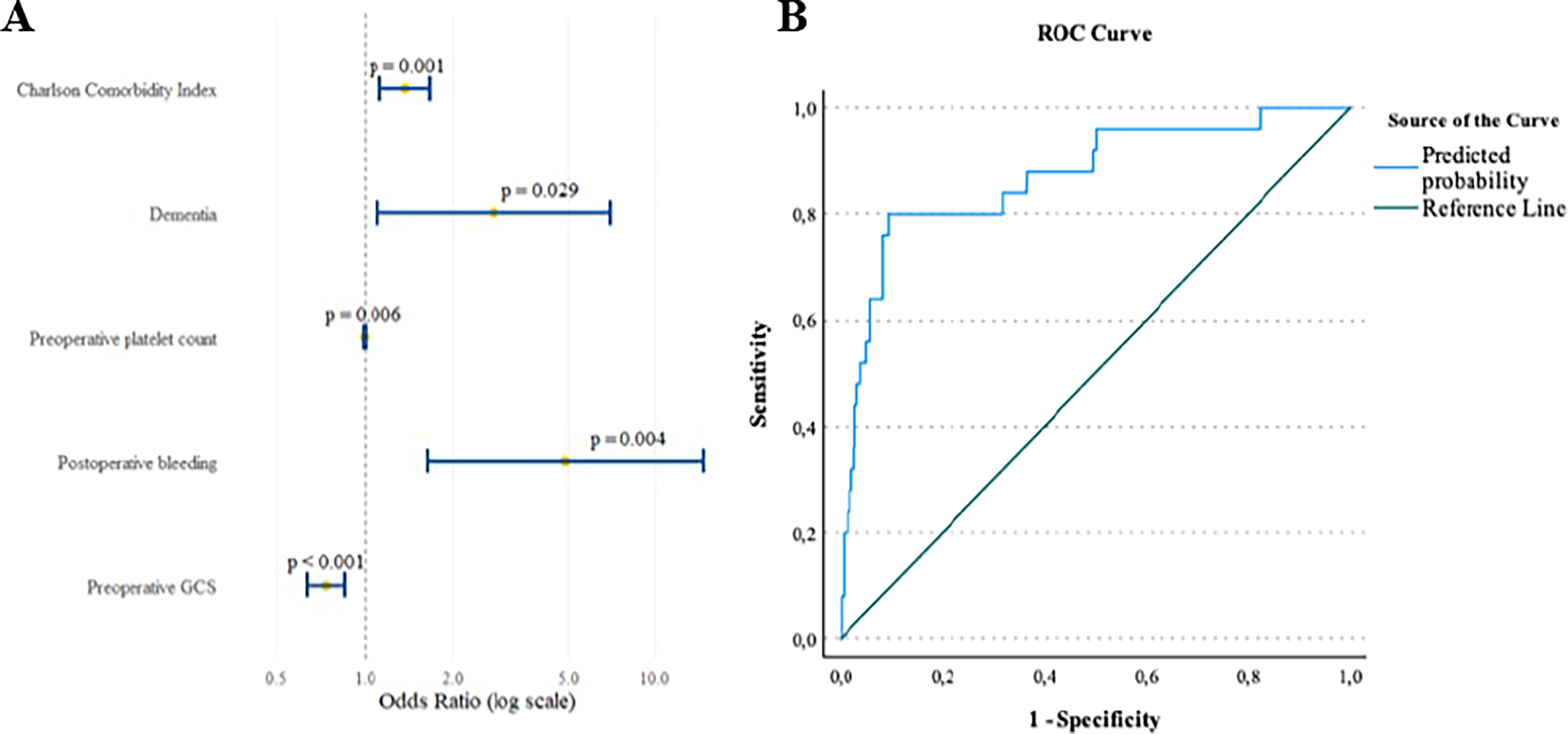
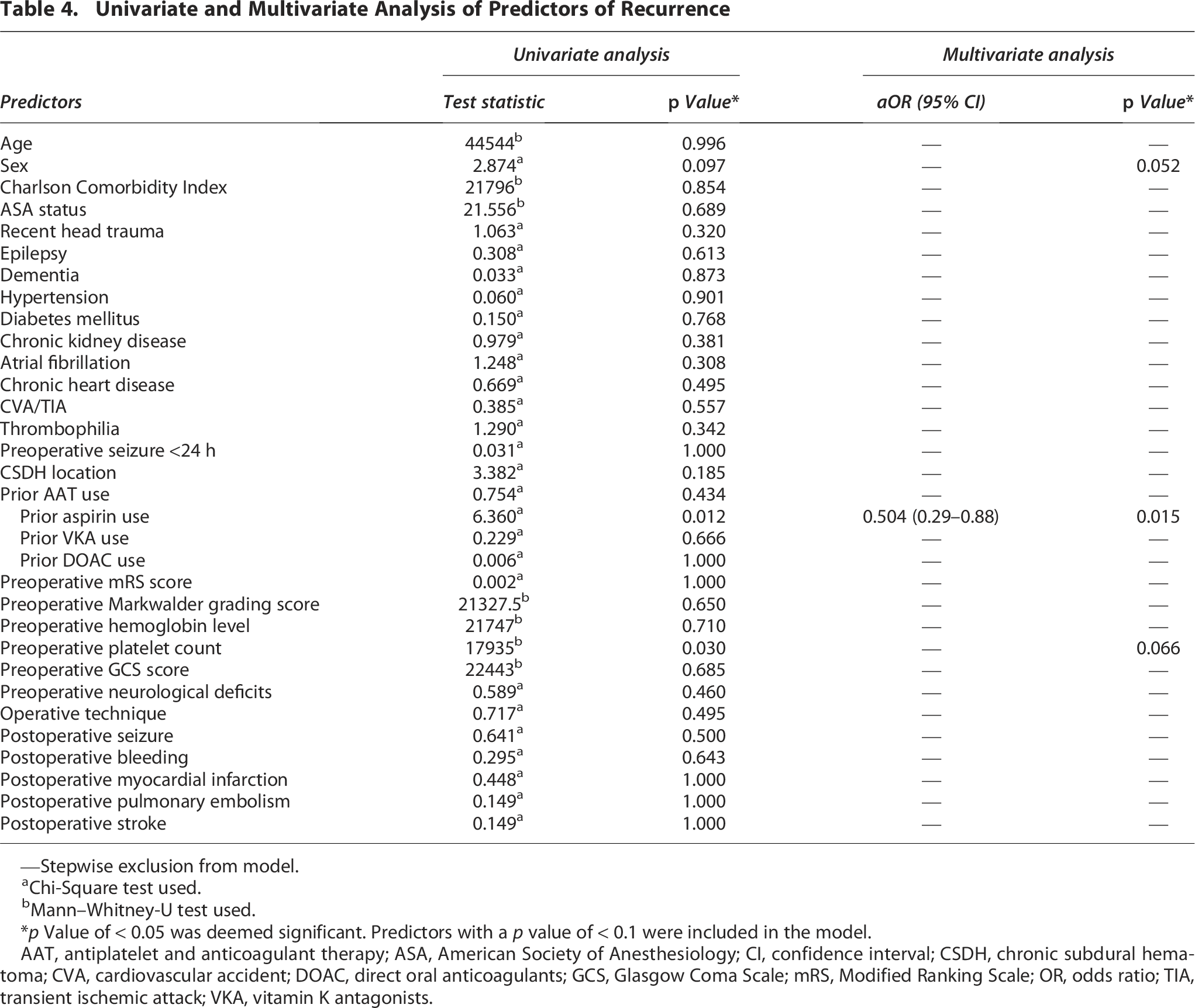
Recurrence occurred in 122 patients (14.3%). In the univariate analysis, recurrence was not statistically significantly associated with prior AAT use (p = 0.434). We then analyzed the association of recurrence between patients without AAT (n = 409) and patients with prior aspirin therapy (n = 217, p = 0.012), vitamin K antagonists (n = 116, p = 0.666), and DOAC (n = 57, p = 1.000). Interestingly, we found that patients with prior aspirin therapy had statistically significantly lower recurrence rates than patients without prior AAT use (p = 0.012). A further analysis comparing patients with prior aspirin therapy (n = 217) with all other patients (without prior AAT use and with prior AAT use other than aspirin) showed a statistically significant association of prior aspirin use with lower recurrence rates (p = 0.003). Furthermore, addressing patients with prior aspirin therapy and patients without prior AAT, recurrence was associated with preoperative platelet count (p = 0.030), whereas female sex (p = 0.097) showed a nonsignificant statistical trend. After adjusting for all confounders (sex and preoperative platelet count), binomial logistic regression revealed that patients with prior aspirin therapy had significantly lower recurrence rates (p = 0.015, aOR = 0.504; 95% CI 0.290–0.877) (Table 4). The other variables did not reach statistical significance. Nevertheless, the model’s discriminative capacity was determined by a ROC curve analysis and was poor, with an AUC of 0.57 (95% CI 0.51–0.64) (Fig. 4).
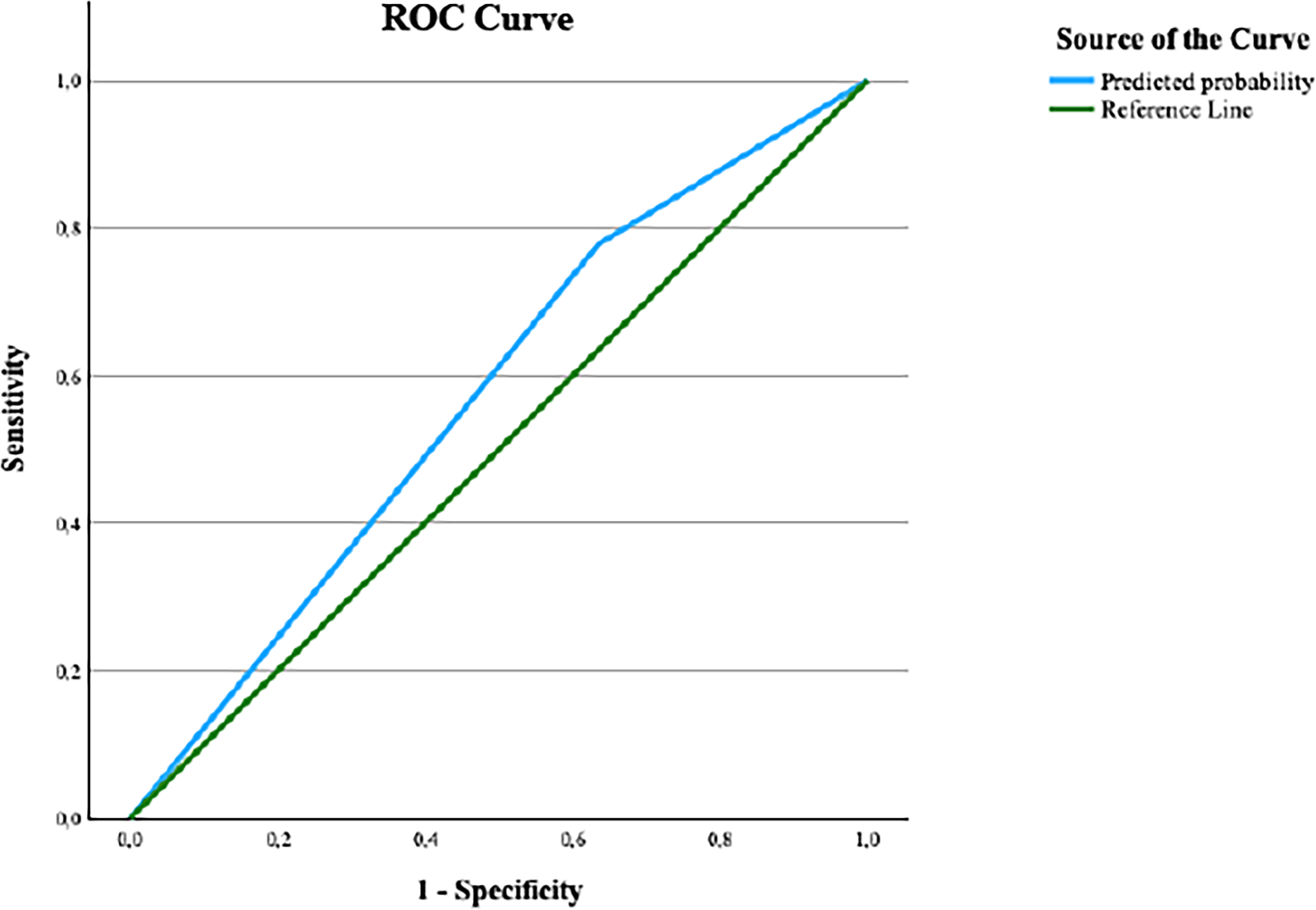
Independent predictors of recurrence. This includes only prior aspirin therapy, compared to all other variables (p = 0.015, aOR = 0.504; 95% CI 0.290–0.877). ROC curve analysis determined a discriminative capacity of the model with an AUC of 0.57 (95% CI 0.51–0.64). AAT, antiplatelet and anticoagulant therapy; ROC, receiver operating characteristic; AUC, area under the curve.
Univariate and Multivariate Analysis of Predictors of Recurrence
—Stepwise exclusion from model.
Chi-Square test used.
Mann–Whitney-U test used.
*p Value of < 0.05 was deemed significant. Predictors with a p value of < 0.1 were included in the model.
AAT, antiplatelet and anticoagulant therapy; ASA, American Society of Anesthesiology; CI, confidence interval; CSDH, chronic subdural hematoma; CVA, cardiovascular accident; DOAC, direct oral anticoagulants; GCS, Glasgow Coma Scale; mRS, Modified Ranking Scale; OR, odds ratio; TIA, transient ischemic attack; VKA, vitamin K antagonists.
Discussion
This comparative study includes a large patient cohort and offers robust, contemporary evidence on the perioperative management of CSDH patients with prior AAT use.
In our cohort, discontinuation of AAT did not independently affect in-hospital mortality, compared with patients without prior AAT use. Multivariate analysis indicated that in-hospital mortality among patients with prior AAT use was more likely related to underlying comorbidities, such as higher CCI and presence of dementia; baseline clinical and laboratory parameters, including lower GCS score and platelet count; as well as postoperative complications like postoperative bleeding. The existing literature on AAT in patients with CSDH remains inconsistent, particularly concerning perioperative risks. Earlier studies suggested that antithrombotic therapy may increase perioperative morbidity, mainly due to a higher incidence of bleeding complications.13,14 However, our findings contrast these results and align with most recent publications in multimorbid patient populations,7,10,15–19 which similarly found no association between AAT and in-hospital mortality.
Furthermore, our analyses demonstrated that discontinuation of AAT was not an independent predictor of poor functional outcome at discharge. Instead, unfavorable functional recovery was multivariately associated with higher age and ASA status, comorbidities such as epilepsy and dementia, baseline functional and hematologic indicators (higher preoperative mRS score and lower hemoglobin level), and postoperative complications including seizure and bleeding. Few studies have systematically assessed functional outcomes following AAT discontinuation. Notable investigations by Poon et al. 4 and Younsi et al., 12 consistent with our results demonstrated that although comorbid conditions and perioperative complications may contribute to poorer outcomes, AAT itself is not an independent predictor.
In contrast to in-hospital mortality and functional outcomes, our findings on recurrence revealed that, compared with patients without prior AAT use, preoperative discontinuation of aspirin in patients with prior aspirin therapy was independently associated with lower recurrence rates. Earlier studies indicated a possible association between perioperative use of antithrombotic therapy and an increased risk of CSDH recurrence.14,17,20,21 This relationship was further highlighted in a large meta-analysis by Wang et al., 10 which showed that perioperative AAT use significantly raises recurrence rates without finding any substantial difference between antiplatelet and anticoagulant therapy in the subgroup analyses. Considering these previous findings together with our results, focusing specifically on patients with prior aspirin exposure who underwent temporary perioperative discontinuation, our data suggest a potential protective effect of prior aspirin therapy. A similar trend was observed, though not explored in detail, in the study by Ridwan et al. 22 This observation accords with hypotheses derived from cerebrovascular pathology, where aspirin’s combined anti-inflammatory and antithrombotic properties have been linked to protection against growth, bleeding, and rebleeding in conditions such as intracranial cavernomas23–25 and aneurysms.26–30 Moreover, the mechanistic insights reinforce this clinical observation. CSDH recurrence and resolution are strongly influenced by angiogenesis and inflammation. Increased cyclooxygenase-2 (COX-2) activity promotes vascular endothelial growth factor production and angiogenesis; both associated with elevated prostaglandin E2 (PGE2) levels and higher recurrence rates.31–34 The observed protective effect of aspirin may stem from its inhibition of COX-2 enzyme and subsequent suppression of PGE2 synthesis, thereby attenuating inflammatory and angiogenic cascades from the onset of CSDH through diagnosis. Theoretically, this mechanism could reduce microvascular injury within the CSDH membrane during hematoma formation and expansion and help explain the lower recurrence rates observed in CSDH patients under aspirin therapy. The Surgical Evacuation of Chronic Subdural Hematoma and Aspirin randomized trial 35 further demonstrated that prior aspirin therapy—whether continued or discontinued perioperatively—did not affect recurrence rates, conveying that the proposed protective effect of aspirin on CSDH membrane occurs well before diagnosis and surgery, particularly during the development and expansion of CSDH. In particular, the extent of microvascular injury due to inflammation and rupture of fragile microvessels within the CSDH membrane appears to be an intrinsic factor that is largely irreversible once the damage has occurred, except by interrupting its vascular supply through middle meningeal artery embolization, which has proven effective in preventing recurrence.36–39 Given the possibility that recurrence risk is, to some extent, predetermined by the degree of microvascular injury within the CSDH membrane at the time of diagnosis—a concept that may represent a paradigm shift in both the understanding of recurrence and the perspective from which its treatment strategies are developed—future research should aim to identify reliable surrogate markers that can inform neurosurgeons about the degree of the CSDH membrane microvascular pathology and guide individualized recurrence risk assessment.
Limitations of the study
This study has certain limitations. First, the analysis was conducted on a single-center cohort, which may limit the generalizability of the findings to broader populations. Nevertheless, our observation of lower recurrence rates in patients with prior aspirin therapy is consistent with an early report—although this prior study did not address the key mechanistic questions explored here. Second, the predictive model assessing the effect of aspirin demonstrated limited explanatory power, as reflected by the low Nagelkerke R2 value and suboptimal AUC in the ROC analysis. This limited power may reflect heterogeneity in clotting propensity within the cohort of patients with prior aspirin therapy. These findings underscore the need for further investigations, ideally incorporating subgroup analyses based on relevant biological markers that capture individual variability in clotting propensity.
Conclusion
This large-scale retrospective study supports the safety of AAT discontinuation in patients with CSDH. Our findings indicate no significant independent association between prior AAT use and in-hospital mortality, poor functional outcomes, or recurrence. Intriguingly, prior aspirin therapy was linked to a reduced recurrence risk, suggesting a potential protective effect. Although AAT is often perceived as a factor increasing surgical risk and recurrence, our results challenge this notion, emphasizing that treatment decisions should weigh individual risk and recurrence profiles rather than default to empiric management.
Transparency, Rigor, and Reproducibility Statement
All supporting data are available within this article. Anonymized data will be shared upon request from any qualified investigator and after approval of the Institutional Review Board of University Hospital Essen.
Authors’ Contributions
S.S. acquired, analyzed and interpreted the data, drafted the initial article, and reviewed and revised the final version of the article. S.A.-R., M.A., and E.T. acquired the data, reviewed and revised the final version of the article. J.R., F.D., O.G., R.J., and P.D. analyzed and interpreted the data, reviewed and revised the final version of the article. U.S. reviewed and revised the final version of the article for important intellectual content. M.C. conceptualized and designed the study, analyzed and interpreted the data, drafted the initial article, revised the article for important intellectual content and reviewed and revised the final version of the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgments
AI-assisted copy-editing using Perplexity AI was utilized to improve the readability, grammar, and style of the article. This process involved refining human-generated text without altering the scientific content. All final text revisions were reviewed and approved by the authors to ensure accuracy and integrity.
We acknowledge support by the Open Access Publication Fund of the University of Duisburg-Essen.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.