
Abstract
Background:
Traumatic intracranial aneurysms (TICAs) secondary to penetrating traumatic brain injuries (PTBIs) including gunshot wounds and shell fragments carry a significant risk of rupture, intracerebral hematoma, neurological injury, and death. Although these lesions were previously thought to arise in a delayed fashion, TICAs have been increasingly reported immediately after PTBI. Early detection and endovascular therapies have contributed to a significant evolution in their management. Here, we review and present reported TICAs in the literature spanning both civilian and military contexts. Lesions are analyzed by morphology, location, management strategies, and outcomes.
Methods:
Case series/reports published between 1940 and 2025 were considered. Injury mechanism, arterial location, diagnostic imaging modality, time to diagnosis, treatment, and outcome data were collected. Only full texts were considered in the final analysis.
Results:
A total of 250 traumatic intracranial pseudoaneurysms in 227 patients met inclusion criteria for this study. The most common vessel distribution was the middle cerebral artery (MCA, n = 98), followed by the anterior cerebral artery (n = 68) and internal carotid artery (ICA n = 48, of which 13 were in the cavernous ICA). Historically, TICAs were detected in a delayed fashion using conventional angiography (104 patients, 113 TICAs). In recent years, early detection of TICAs has been facilitated by CT angiography (CTA; 52 patients and 64 TICAs) and digital subtraction angiography (DSA; 52 patients and 53 TICAs). Endovascular surgery and open approaches complement each other in the obliteration of TICAs, with a significant increase in the use of the former during the last three decades.
Conclusion:
TICAs are complex lesions secondary to PTBIs. Detection, management strategies, and outcomes have evolved over the last several decades. Early detection using CTA and DSA has significantly increased the incidence of these lesions in the acute phase. Vigilant monitoring and delayed follow-up imaging remain essential components of modern management given the risk of delayed aneurysm formation, growth, and recanalization.
Keywords
Introduction
Traumatic intracranial aneurysms (TICAs) are an infrequent but challenging complication of penetrating traumatic brain injury (PTBI).1–3 These lesions arise due to direct and indirect projectile injury to the vessel wall (gunshot wounds to the head [GSWH] and shell fragments), damage from bone fragments, and the high-velocity shock wave through the brain (Fig. 1).4,5 Due mainly to more sensitive imaging technologies, their incidence has steadily increased over the previous decades.6–8 Initial series reported TICAs discovered on delayed cerebral angiograms, including ruptured or enlarging aneurysms causing intra- and extracranial bleeds and mass effect.6,9–13 Evidence from Operation Iraqi Freedom indicated a higher incidence (16%, 24 TICAs) when a mixed population of closed and penetrating injuries is evaluated with digital subtraction angiography (DSA). 7
Mechanisms of injury of penetrating brain trauma. High- and low-velocity projectiles can directly damage the brain parenchyma and vasculature. Indirectly, bullets and shrapnel can drive bone fragments intracranially, producing damage to the vessels. Finally, the shock wave can reverberate through the brain tissue and weaken the arterial walls, thereby inducing TICAs. TICA, traumatic intracranial aneurysms.
With new imaging technologies, early time points have been characterized. The incidence of TICAs in the first 12 h postinjury, when lifesaving surgical decisions are made, has been as high as 20% in civilian GSWHs. 6
The shift toward earlier detection of TICAs may be attributed to the use of DSA, as well as widespread availability of CT angiography (CTA), in the hours immediately after the injury. 14
Improvements in endovascular techniques and open surgical approaches have provided new avenues for TICA obliteration. Serial imaging of TICAs has enabled monitoring for aneurysm growth and has uncovered a population of self-resolving TICAs.4–6,9–11,15–17
Considering these recent advances, the available literature was searched to review and analyze previously reported TICAs due to PTBIs. Injury mechanisms, diagnostic methods, treatment modalities, postoperative follow-up, and clinical outcomes were identified and organized. By analyzing these factors, this review aims to provide a comprehensive basis for the diagnosis and management of these complex injuries in both the acute phase and during long-term follow-up.
Methods
Inclusion/exclusion criteria
The literature was searched for full-text articles treating TICAs secondary to wartime/civilian missile PTBI. The PubMed/MEDLINE database was queried to identify full-text articles. The final search was completed on December 30, 2025. The search was confined to publications released between 1940 and 2025. All study types were considered. In order to minimize reporting bias, all the articles’ references were screened for additional publications. Discrepancies regarding the search and papers selected were resolved through discussion within the team.
PubMed searches included “traumatic intracranial pseudoaneurysm,” “traumatic intracranial aneurysm,” “penetrating brain injury,” “gunshot,” “shrapnel,” “missile.” All the papers and references identified via PubMed search were manually screened to find additional references. Abstracts were reviewed. Only full-text articles were included (Supplementary Fig. S1).
Nonpenetrating blunt traumas, reports lacking injury location and other injury characteristics, and injuries to the extracranial circulation including the carotid and vertebral arteries in the neck and external carotid artery were excluded. Duplicate patients across overlapping institutional reports were excluded (Table 1).
Wartime and Civilian TICAs Secondary to High- and Low-Velocity GSWs, as Well as Shrapnel, Are Listed
Reference, year of publication, patient age and sex, injury type, TICA location and modality of imaging used to diagnose it, time interval between injury and diagnosis, treatment modality, and outcomes are included.
ACA, anterior cerebral artery; GSW, gunshot wound; ICA, internal carotid artery; MCA, middle cerebral artery; PCA, posterior cerebral artery; TICA, traumatic intracranial aneurysm.
Case selection, data extraction, and data analysis
Collected data included TICAs secondary to civilian and military GSWs, or shrapnel. Variables collected included the publication year, patient age, sex, type of injury, TICA location, imaging modality, injury-diagnosis interval, treatment methodology, and outcome. To mitigate the studies’ heterogeneity, cases of TICA were manually classified as published before 1996 or after December 31, 1996, based on the last available angiography-based report. Treatment was described as either open or endovascular approaches or observation. Only patients with detailed data were included in each analysis, while those presenting a range were excluded. In addition, papers reporting post-PTBI TICAs that did not specify the demographic, injury, and treatment characteristics were excluded from Table 1 and final analysis.8,62,63
Statistical analysis
Chi-squared test was used for all variable comparisons including imaging modality, arterial location, time to diagnosis, and injury mechanism. p < 0.05 was considered significant. TICA occurrence in each parent artery and in the anterior and posterior circulation was analyzed. GraphPad Prism (San Diego, CA, USA) was used to conduct the analysis.
Data availability statement
All the raw data used for the analyses are presented in Table 1.
Results
A total of 227 patients presenting with 250 TICAs following PTBI were identified (Table 1). Of these, 139 suffered wartime injuries, while 88 were civilian PTBIs. The average age at presentation was 26 years (177 patients had available age), and among the reported injuries, the male:female sex distribution was 151:11. The average interval between the initial PTBI and diagnosis was 16 days (n = 184). Before 1996, the average time between PTBI and TICA discovery was 25.4 days. After 1997, the interval decreased to 10.5 days (p = 0.04). Before 1996, 113 TICAs were reported (113/250, 45%), while after 1997, 137 lesions were diagnosed (137/250, 55%).
Arterial distribution
The most common location was the middle cerebral artery (MCA; n = 98; 41.3%), followed by the anterior cerebral artery (ACA; n = 68–28%) and internal carotid artery (ICA; n = 48–20%). TICAs in the ophthalmic artery were diagnosed in four subjects, while the posterior circulation was rarely involved. Eight aneurysms were diagnosed along the posterior cerebral artery (PCA; n = 8–3%) and 12 in the basilar artery tree (5%). TICAs from 211 patients had clear mechanisms of injury. A similar distribution of TICAs along the major intracranial arteries was noted in patients who suffered civilian GSWH, wartime GSWH, and shrapnel injuries (Table 1, Fig. 2; p = 0.07, χ2 = 14.15, df = 8). Distal injuries (M2-3-4, A2-3-4, P2-3-4) appeared to be common, with 49/250 TICAs (20%), located in distal branches. This appears to be an underestimate, as most aneurysms are only assigned to a major vascular distribution.
Distribution of TICAs along the major intracranial vessels and injury etiology. TICA incidence is represented for each major intracranial arterial tree. Similar fractions of TICAs were noticed in patients who suffered civilian GSWH and shrapnel injuries, especially in the MCA distribution. A nonsignificant difference with TICAs secondary to wartime GSWH was noticed. GSWH, gunshot wound to the head; MCA, middle cerebral artery; TICA, traumatic intracranial aneurysm.
Imaging modality and timing of diagnosis
Of the 250 TICAs reported in 227 patients, 207 subjects had diagnostic imaging modality available and 204 time from injury to diagnosis available. In 104 patients, TICAs were first diagnosed with unsubtracted angiography (98 patients had interval between injury and diagnosis available); in 52 patients, 64 TICAs were first diagnosed with CTA (39 with available interval); in 49 patients, 50 TICAs were first diagnosed with DSA (25 with available interval). For 24 subjects diagnosed with DSA, only a time window was provided (Tables 1 and 2). One TICA was found on MRI. For the remaining patients, the diagnostic technique used was not specified.
Patients Diagnosed According to Imaging Modality, Time Window Between Injury and Discovery (<7 Days and ≥7 Days), and by Era (≤1996 and >1997) (χ2 = 112.1, df = 6, p < 0.0001)
Total number of patients diagnosed with the technique. Several patients did not display interval between injury and diagnosis and were not considered for this analysis. In parenthesis, the total number of aneurysms diagnosed with each modality.
CTA, CT angiography; DSA, digital subtraction angiography.
While pre-1996 reports relied on the clinical examination, medical history, and unsubtracted angiography to detect TICAs, the adoption of DSA and CTA appears to have shortened the diagnostic interval. Among injuries that occurred prior to 1996, 77/104 patients were diagnosed after the first week (74% of the total). A significant shift took place after 1997. Among patients diagnosed with CTA, 37/42 (87% of the total) harbored a TICA in the first 6 days postinjury. In the DSA cohort, 20/25 (80% of the total) were diagnosed in the same timeframe. Importantly, 58 TICAs (31% of the total) were discovered during the first 24 h after the injury.
Finally, delayed TICAs became less common >1997 across all imaging modalities, as only 8/62 patients with a precise time interval reported (13% of the total) were diagnosed ≥7 days postinjury, compared with 78/100 subjects before 1996 (78%).
Vessel imaging in the acute phase
Since the emergence of CTA, several studies have attempted to characterize its sensitivity, specificity, and positive (PPV)/negative predictive values (NPV). Bodanapally et al. retrospectively reviewed a cohort of 45 patients who suffered PTBI and compared CTA with DSA performed shortly after the injury. In this series, CTA had a sensitivity of 72.7% and a specificity of 93.5% for detection of TICA. 48 In a follow-up paper, Bodanapally et al. characterized TICA risk factors on admission CTA following PTBIs. 10 Patients with TICAs showed higher proportions of frontobasal-temporal entry, bihemispheric injuries, proximity to the circle of Willis, SAH and IVH, higher modified Hijdra score, and higher modified Graeb score. Ares et al. retrospectively compared the findings of admission CTA with DSA performed within 24 h post-PTBI. On DSA, 14/24 patients with TICAs on CTA were diagnosed with additional vascular lesions. Nine out of 32 (28%) patients with negative CTA had a TICA revealed on DSA. This resulted in a higher modified-Biffl grading in 30% of cases and a lower score in another 30% of the cohort. 62 Meyer et al. reported the findings of PTBI patients who had CTA on admission, followed by DSA within the first 2 days. They reported a 45% incidence of vascular injuries of ∼45%, with CTA having a PPV of 66.7% and NPV of 61.8%. CTA missed nine TICAs, three arterial occlusions, eight dural arteriovenous fistulas, and six carotid-cavernous fistulas to yield an overall sensitivity of 36.4% (95% confidence interval 20.4–54.9%) and a specificity of 85% for any vascular injury when assessed in a prospective fashion against DSA. 63
Treatment strategies
Open and endovascular strategies have been employed to treat TICAs. Overall, open surgery was used to treat 107 TICAs, endovascular therapies in 40 aneurysms, and observation/spontaneous resolution occurred in 34 lesions. When lesions were classified by location, open surgery was most frequently performed in the anterior circulation (102 TICAs distributed as follows: MCA n = 49 TICAs; ACA n = 24 TICAs; ICA n = 20 TICAs; ophthalmic artery n = 3; Fig. 3). Out of 107 TICAs treated with open approaches, only 5 were in the posterior circulation.
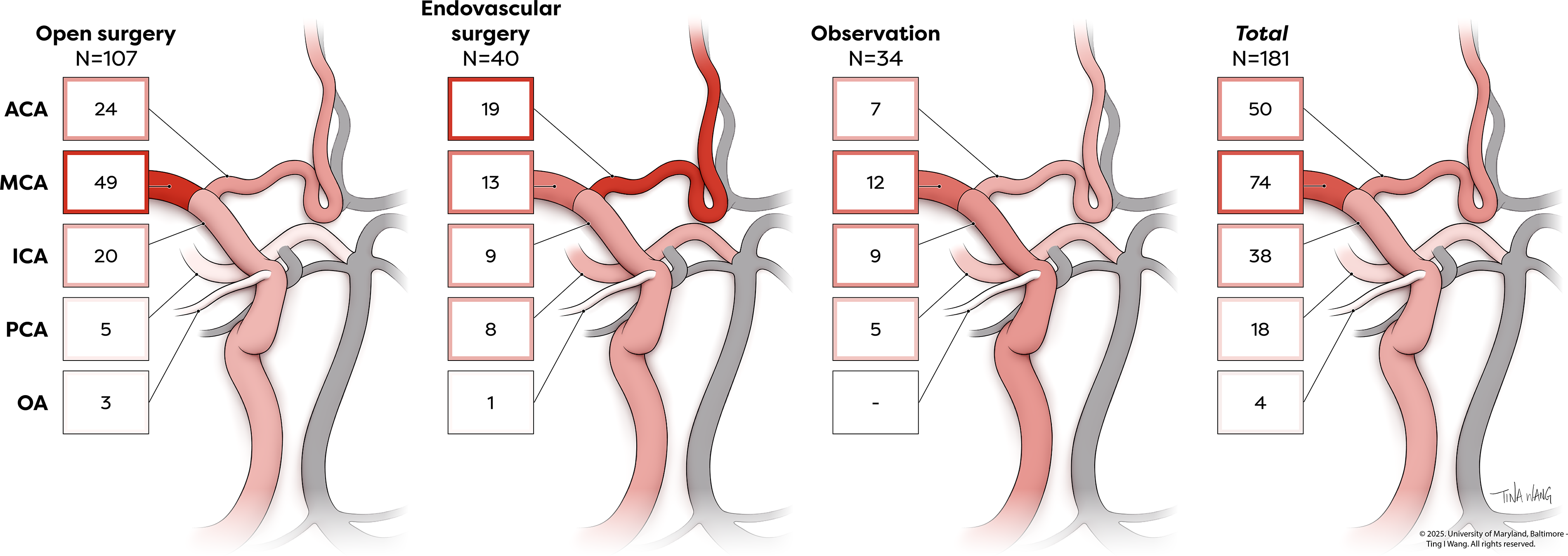
TICA treatment organized by vascular distribution. While open techniques have been used across all the major vascular intracranial distributions, endovascular approaches have been preferentially used in the anterior circulation. A significantly higher fraction of MCA TICAs was treated with open approaches, compared with endovascular surgery and observation. MCA, middle cerebral artery; TICA, traumatic intracranial aneurysm.
A higher proportion of posterior circulation TICAs was noticed in the endovascular therapy group. In the ICA distribution, 42 TICAs were treated with endovascular techniques (MCA n = 13 TICAs; ACA n = 19 TICAs; ICA n = 9 TICAs; ophthalmic artery n = 1), with 8 TICAs in the posterior circulation addressed with this approach. Observation and spontaneous resolution were reported in 28 TICAs in the anterior circulation (82% of the TICAs that underwent observation) and for 5 lesions in the posterior distribution (18% of the total observed TICAs). Chi-square test demonstrated a significant association between open treatment and aneurysmal location in the anterior circulation (p = 0.03). The difference was driven by MCA TICAs, which were predominantly treated with open surgery (80% of total MCA aneurysms, p = 0.03, χ2 = 6.44, df = 2).
For peripheral injuries occurring past the second segment of the ACA, MCA, and PCA, open treatment is predominant. Trapping/excision is the favored approach, given the small caliber of these distal vessels and easy access (13/49, 26%), followed by clipping (4/49, 8%). Endovascular treatment can, in contrast, result challenging, as microcatheters often cannot reach distal branches. Nonetheless, isolated coiling of the aneurysm or parent vessel or combined stent/coiling has been reported in 10 out of 49 peripheral TICAs (20% of the total). Several patients did not have a reported treatment strategy.
Treatment strategies by era
Up to 1996, open surgery was the predominant modality (74 cases), compared with none treated with endovascular surgery and 9 cases managed by observation (Fig. 3). Sixty patients were treated with cautery, clipping, and excision. Clamping and arterial ligation were used in 12 subjects, while 2 patients underwent bypass.
After 1997, a marked increase in endovascular surgery was reported (49 cases), while open surgery was used in 21 patients. Seventeen patients and 18 TICAs underwent clipping and/or trapping/sacrifice; 1 was treated with carotid ligation and 3 with bypass. The number of cases managed nonsurgically or that spontaneously resolved increased to 23 after 1997. Among those treated with endovascular therapy, 36 patients/TICAs were coiled, 5 were stented or stent/coiled, and 8 were occluded with onyx or embolic material (Tables 1 and 3).
Traumatic Pseudoaneurysms Treated with Each Modality or Undergoing Observation/Spontaneous Healing in Each Era (≤1996 and >1997)
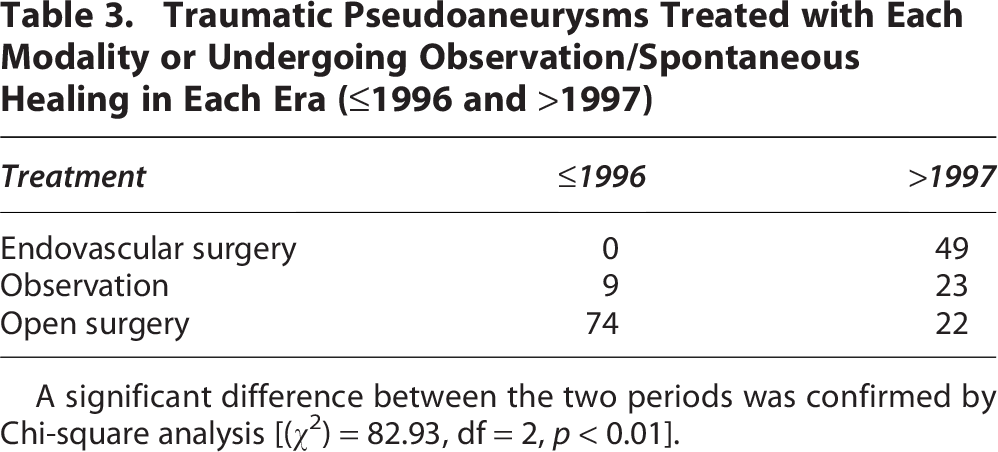
A significant difference between the two periods was confirmed by Chi-square analysis [(χ2) = 82.93, df = 2, p < 0.01].
A significant difference between the two eras (≤1996 and >1997) in the type of approach was detected by Chi-square analysis [(χ2) = 82.93, df = 2, p < 0.01].
Outcomes
Overall, 113 patients had “good outcomes.” Many of these included visual deficits ranging from ophthalmoplegia to partial or total blindness. Several reports only described aneurysmal occlusion characteristics, their stability, or need for additional treatment. Lack of precise neurological outcomes was frequent in the selected publications. Thirty-two patients died or had severe neurological deficits. Outcomes were not reported for 76 patients.
Limitations of presented evidence
Significant heterogeneity among the studies is unsurprising, in terms of surgical techniques, pre- and postsurgical management, and imaging approaches available at the time of publication. Studies were stratified by mechanism of injury (wartime vs. civilian) to control for factors such as transport from the scene to the nearest hospital, availability of CT or DSA, and delayed debridement.
Discussion
Context and mechanism of injury
PTBI causes direct damage along the missile path and indirect trauma to the brain and vessels. It is relevant to consider the energy released to decipher the impact on cerebral vasculature. 64 The force produced by PTBI can be modeled as a function of half of the projectile mass multiplied by the square of the object’s velocity or ½ mv2. As velocity dominates this equation, high-velocity projectiles have more significant destructive potential.65,66
High-velocity injuries result in distant shearing, cavitation, and the propagation of shock waves through brain tissue.64,65 The rare occurrence of TICAs with high-velocity injuries can also be explained by their lethality, which precludes patients from reaching a hospital with CTA/DSA capabilities.
Civilian gunshot wounds are characterized by lower projectile velocity. Blood vessels in the projectile’s path can develop intramural hematomas and TICAs. Bony fragments from calvarial fractures can injure blood vessels (Fig. 1).4,5,7,16,17,20 In the hyperacute phase, low-velocity PTBI can present with an incidence of TICAs up to 40%. 6
The difference between high- and low-velocity PTBI suggests that 1 a substantial number of TICAs form rapidly after low-velocity injury and resolve spontaneously, and 2 prior series underestimated the incidence due to delayed imaging or early patient death.
Prospective studies that incorporate vessel imaging at predetermined time points after the injury and during follow-up encounters might elucidate the natural behavior of these lesions.
Timing of imaging
The first reports of post-PTBI TICAs suggested a delayed pathogenesis of these lesions,4,5,7,12 a view that has been recently challenged. While TICAs still present after weeks or months post-PTBI, growing evidence supports early occurrence of TICAs.5,6
Ferry and Kempe diagnosed two TICAs among 2,187 suffering PTBIs during the Vietnam conflict. 19 During the Iran–Iraq war, Aarabi et al. reported a 2.8% incidence. 5 Among 223 patients with craniocerebral missile injuries imaged with angiography (average 16.9 days postinjury), 21 presented TICAs. Jinkins et al. reported a TICA incidence of 33% when angiograms were performed in the first 48 h postinjury. 13 This series prompted further investigation into early timepoints, as TICAs might be missed in the window when lifesaving decisions and surgeries are carried out. 13
In a recent series from the University of Maryland Shock Trauma Center, a significant proportion of hyperacute TICAs was described immediately after the injury. 14 Furthermore, an association with intracerebral hematomas, as well as interval hematoma growth and need for surgical decompression/debridement, highlighted the clinical relevance of these lesions. 6 Babichev et al. reported a similar trend from the Ukrainian conflict, where TICAs were discovered on average 10 days after the initial injury via CTA of the head, and 9 out of 18 lesions were diagnosed in the first 6 days after PTBI (50% of the total). 26
Active bleeding with intracerebral hematoma and progressive growth on serial scans are common occurrences in these early TICAs, and prompt intervention to occlude these lesions should always be considered.
Use of CTA and DSA in the acute period
As CTAs have become more accessible, their use in early TICA diagnosis has expanded. While their sensitivity is limited by metal fragments in the GSWH/shrapnel tract, CTAs still provide high-quality images for major arterial trunks, allowing for prompt identification of individuals at risk for penetrating vascular injuries who might benefit from further evaluation with DSA or immediate surgery (Fig. 4).10,48
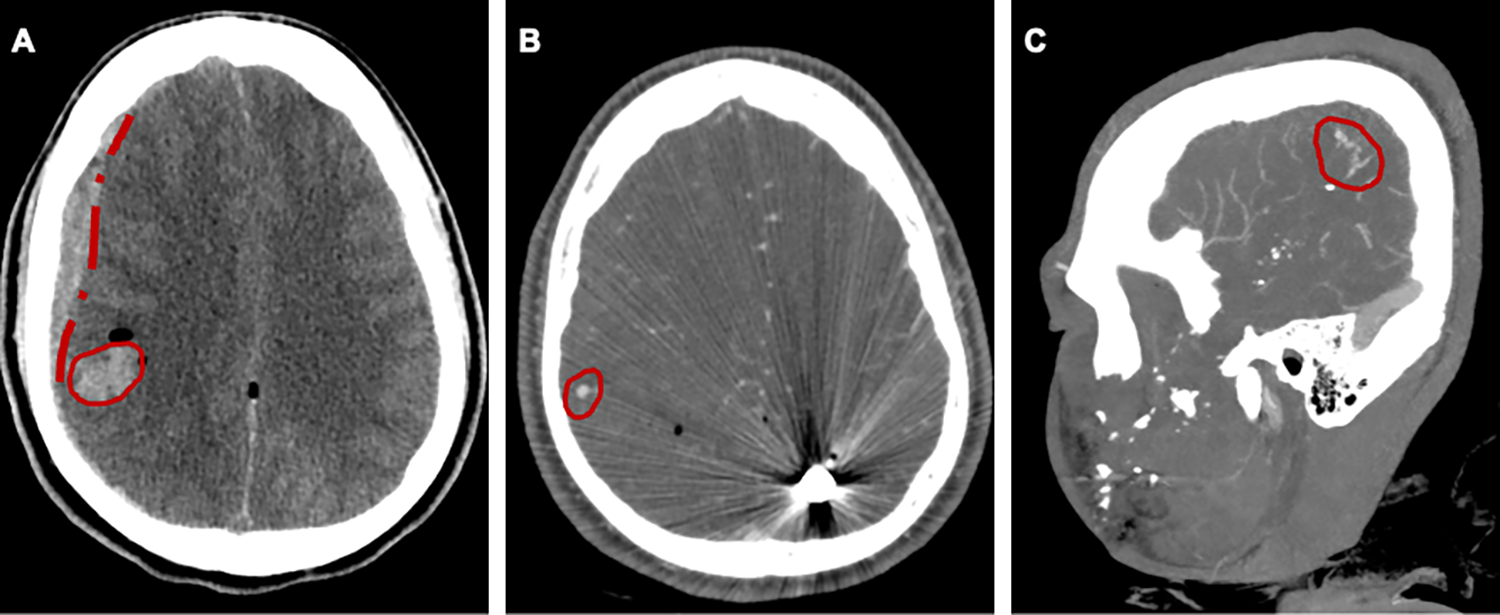
Sixteen-year-old boy 1 hour following civilian gunshot wound to the right pterional region presented with a large right non-reactive pupil and flexion-posturing on exam. CT scan revealed a small right parietal ICH (panel A), as well as an acute subdural hematoma. CT angiography showed a right MCA M4 TICA (panels B and C). The patient was taken emergently to the operating room for decompressive craniectomy and caurterization/excision of the traumatic pseudoaneurysm. The patient made a full recovery.
Recent evidence has shown that while catheter-based DSA achieves higher sensitivity and specificity than CTA, the latter retains significant value in the emergent preoperative evaluation of patients in need of cerebral decompression. DSA, with its high sensitivity and specificity, remains the gold standard for the evaluation of TICAs. Importantly, TICA treatment can also be achieved during the same session as vascular access is secured. Subjects at increased risk can undergo repeat vascular imaging in the weeks after the injury. These techniques complement each other in the acute phase following PTBI, helping the neurosurgeon in the diagnostic process and with treatment selection.
The recent proposal of a modified-Biffl scale to characterize the severity and location of intracranial vascular injuries may provide a useful addition to standardize the description and treatment of these lesions. Broader validation of this scale and its ability to predict the injury severity, patient survival, and overall neurological outcomes can be achieved with prospective multi-institutional studies.
Surgical and endovascular approaches
TICAs have been treated with open surgical clipping, vessel sacrifice, intracranial bypass, or cauterization.4–6,9–12,15,48 While aneurysm clipping is typically not performed due to lack of a neck, clip-sacrifice of the parent vessel is common. Arterial ligation was encountered, as well as Crutchfield clamping. Cauterization has mainly been employed in the MCA and ACA distribution. In contrast, bypasses have rarely been used, likely because of the distal TICA location, poor vessel availability for revascularization, and fragile parent vessel wall.
In recent years, endovascular treatment has complemented open surgery. Endovascular methods allow for easier access to distal lesions in a swollen brain. Coil-sacrifice has been employed since the mid-1990s, with or without the concomitant use of embolic materials. Importantly, a predominance of ACA lesions is noted among these patients. This is likely secondary to the interhemispheric approach that would be needed in the acute phase, considering the significant brain swelling that follows GSWHs. More recently, flow diversion and stenting allowed for the reconstruction of complex lesions. The need for dual antiplatelet therapy has nonetheless hindered more widespread implementation of these approaches, as these might increase bleeding risk. In a recent series, endovascular management was used in 43% of the TICA cohort. Approximately 14% of the patients were treated with parent vessel sacrifice and 28% with methods associated with flow preservation. 6 In the military setting, Bell and Sirko showed the significant benefits of early DSA and endovascular therapy in wartime TICAs, coupled with open surgical intervention when needed.
When taking TICA location into account, peripheral injuries are frequently treated with trapping/excision (13/49), followed by coiling/stenting (10/49) and clipping (4/49).
Conservative management and observation with scheduled imaging are typically reserved for small, distal aneurysms.12,67,68 Spontaneous resolution is more common in series that used early vessel imaging.
Conclusions
TICAs are a complex, potentially lethal complication of PTBI. Their reported incidence has risen steadily over the last decades, likely due to early detection with CTA and DSA. This allows neurosurgeons to uncover a significant proportion of lesions in the acute phase. Their early detection facilitates timely treatment with open and endovascular techniques. Parent vessel sacrifice is frequently achieved in distal arteries, while vessel reconstruction can be pursued in larger arteries with revascularization techniques and flow diversion.
In conclusion, evidence from several civilian and wartime series points toward the use of early CTAs/DSAs to diagnose, follow, and treat these lesions in the acute window. While spontaneous resolution has been reported, observation should be reserved for lesions that appear stable on repeat scans. Open and endovascular approaches are equally effective in achieving TICA occlusion. Treatment should be tailored to the patient presentation, considering the neurological status, perilesional edema, and presence of intracerebral bleeds, contusions, and other injuries. Future studies will expand our understanding of ultra-early vessel imaging and ideal timing of follow-up, as well as the integration of open and endovascular techniques.
Transparency, Rigor, and Reproducibility
To improve rigor, transparency, and reproducibility, article searches and paper selection were performed by two authors (R.S. and M.H.) blinded to the patient characteristics, clinical history, and outcomes. Statistical analyses were carried out using Prism software. All data and materials included in these studies will be freely shared with any interested party. The data that support the findings of this study are available from the authors and are included in Table 1.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
We would like to thank the SNS Neurosurgeon-Scientist Training Program for providing funding for this article.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.