
Abstract
This is an original follow-up study on predictors of social participation outcomes after traumatic brain injury (TBI) in a prospective longitudinal cohort followed within a universally accessible specialized rehabilitation pathway. The analytic sample comprised 98 individuals with complete clinical data that participated in inpatient and/or outpatient rehabilitation programs at three health centers and completed the outcome measures at a minimum of one year after discharge. The study sample included 26 participants with mild TBI, 23 with complex-mild TBI, 36 with moderate TBI, and 13 with severe TBI. Two outcome measures were administered, the Mayo-Portland Adaptability Inventory-4 (MPAI-4) and the Quality of Life after Brain Injury (QOLIBRI) questionnaire, to investigate social participation and health-related quality of life outcomes in patients with TBI at least one-year post-rehabilitation. Hierarchical regression models assessed the significance of various pre-, peri-, and post-TBI potential predictors in relation to the two outcome measures. Results showed that significant predictors of social participation (MPAI-4 Participation scale) at least one year after rehabilitation included the MPAI-4 Abilities subscale score at intake (p = 0.032) and the delay to rehabilitation intake (p = 0.012). The 8-predictor multivariate model accounted for 33.5% of the variance in social participation. For quality of life as measured by the QOLIBRI, significant predictors were the MPAI-4 Adjustment scale at intake (p = 0.031), employment status post-discharge (p = 0.024), and sports-related cause of injury (p = 0.000). The 10-predictor multivariate model accounted for 45.8% of the variance in quality of life. Our study highlights the importance of following up on individuals with TBI and studying predictors of social participation and quality of life in the years following rehabilitation since they can vary in time. This could help to target appropriate services to develop and offer once rehabilitation has ended, to support favorable long-term outcomes following a brain injury.
Introduction
The impact of traumatic brain injury (TBI) significantly challenges individuals’ ability to return to their social lives, in some cases, long after the TBI incident.1–3 In general, most adults with severe TBI and many with moderate TBI experience significant difficulties in social and occupational reintegration. In the case of people with mild TBI, evolution is positive in most cases, but several studies show that between 15% and 20% are at risk of presenting persistent symptoms impacting several areas of their lives.4–6
In the literature looking at TBI outcomes, especially social participation (e.g., return to work or other productive activities, community integration), there is a great deal of inconsistency about the significance of predictors as shown in the findings of several reviews conducted on predictors of social participation after TBI.7–9 This is because such outcomes depend on the interplay between injury-related impairments and environmental factors, such as sociocultural context, social support, government policies, and accessibility to health care services.10–12
This study is a follow-up to that conducted by Guerrette and McKerral (2023) within a universally accessible and organized trauma continuum of care. Their study investigated pre-injury, injury-related, and post-injury predictor variables of social participation following TBI as measured by the Mayo-Portland Adaptability Inventory—version 4 (MPAI-4) Participation scale at the end of rehabilitation.13,14 The authors found that for individuals who underwent inpatient and outpatient rehabilitation, three variables significantly predicted their social participation outcome: years of education and scores for MPAI-4 Ability and Adjustment scales at rehabilitation intake. These variables accounted for 49% of the variance in social participation. For individuals who only received outpatient rehabilitation, five variables significantly predicted social participation outcome: premorbid hypertension and mental health diagnosis, total indirect rehabilitation hours received, and MPAI-4 Abilities and Adjustment scores at rehabilitation intake. These variables accounted for 47% of the variance in social participation. 13
Their study captured social participation levels at the beginning and end of rehabilitation, and while it enabled measurement of improvements in social participation levels during rehabilitation and identification of its predictors at discharge, it did not permit evaluation of whether these improvements were sustained post-discharge from outpatient rehabilitation and if the predictors of social participation remained the same or evolved. In addition, the MPAI-4 measures functional impairment and extent of disruption in various domains of social participation; it does not address a person’s perceived well-being and quality of life, which are known to be often altered after a TBI.15,16 Research has consistently shown that TBI can have a profound negative impact on both overall and health-related quality of life.17–19 This underscores the need to also investigate the predictors of quality of life, particularly within rehabilitation settings and post-discharge. Studying these predictors can inform targeted interventions and improve outcomes for individuals recovering from TBI.
Therefore, our study objectives were to identify variables that could contribute to predicting social participation measured by the MPAI-4 Participation scale as well as quality of life measured by the Quality of Life after Brain Injury (QOLIBRI) scale at least one year following rehabilitation discharge. The QOLIBRI scale is validated and commonly used for assessing health-related quality of life in individuals with TBI.20–22 This study is novel in that it reports on the one-year follow-up of individuals who received inpatient and/or outpatient rehabilitation in a public and universally accessible health setting and for whom social participation had been previously measured during rehabilitation.
Methods
Experimental design
This study was part of a prospective longitudinal cohort study, from which a subset of the initial cohort was followed up at one year post-rehabilitation. This study was registered at ClinicalTrials.gov (Identifier: NCT05022940) and is reported according to the STROBE statement for cohort studies. 23
Participants
Participants were recruited from a database of adults who spoke French or English and who had received TBI rehabilitation between April 2016 and June 2020 at two Integrated University Health and Social Services Centers and one Integrated Health and Social Services Center in the Greater area of Montreal, QC, Canada. All participants had been diagnosed with TBI and referred to rehabilitation by a health care professional. Ethical approval for the study was obtained from the Research Ethics Board of the Center for Interdisciplinary Research in Rehabilitation of Greater Montreal (project #CRIR-1219-0317).
Procedure and data collection
The French-Canadian version of the MPAI-4 had been previously systematically administered to all participants in the database by consensus of the clinical team upon intake to inpatient or outpatient rehabilitation according to a standardized clinical protocol previously implemented within the rehabilitation programs. 24 For the inpatients, this occurred within two weeks of admission, and for the outpatients, within four weeks. The MPAI-4 was also administered at the conclusion of outpatient rehabilitation, within one week of discharge.
Patients with TBI identified in the database were contacted by telephone at least one year after the end of their rehabilitation to ask them to complete the MPAI-4 and the QOLIBRI through a phone interview. A person identified at each rehabilitation site (e.g., research coordination staff, not related to the study research team) made initial contact with potential participants to obtain their consent to be contacted by our research team. The consenting participants were then contacted by the research team to solicit their participation in the study. Two members of the research team completed sociodemographic, MPAI-4, and QOLIBRI questionnaires with all the participants by phone using a detailed verbatim, relying on the participants’ self-reporting. All questionnaires were completed by the participants themselves with no proxies. There were 348 adults (≥16 y at time of TBI) who were contacted by the rehabilitation sites at least one year after their discharge, of which 106 (30.5%) were unreachable. Of the remaining 242 participants, 171 (70.7%) consented to the follow-up assessment (post-rehabilitation M = 19.1 months, SD = 7.2 months) and 71 (29.3%) declined.
Only data from participants who had a complete set of clinical information were included in the analyses (N = 98). A member of the research team had extracted additional sociodemographic and clinical data for each of these participants from the rehabilitation database during visits to the participating sites. Following a comprehensive review of the literature and available information, data were recorded to create both dichotomous and continuous independent variables for the analyses. Participants with complete clinical information (N = 98) and those without (N = 73) did not differ significantly on age, sex, TBI severity, delay to rehabilitation, or MPAI-4 subscale scores at intake or follow-up (all p > 0.05). We also compared the respondents and the nonrespondents (i.e., those who were unreachable or declined to participate) based on age, biological sex, severity, and education. In the respondent group (N = 171), there were 81 (47.4%) females, and the average age was 57.6. In the nonrespondent group (N = 177), there were 74 (41.8%) females, and the average age was 61.9. There were no significant differences between the two groups on these variables (all p > 0.05).
Independent variables
We considered sociodemographic and clinical variables to build our prediction models. These variables were grouped into three categories: pre-injury, injury-related, and post-injury. 13 The MPAI-4 Participation and Total scores at discharge were not included in both prediction models and employment status post-discharge was not included in the social participation model due to multicollinearity issues. For the social participation model, variable selection was grounded in the findings of Guerrette and McKerral (2023), who predicted the same outcome in a similar population. Variables significant in their multivariate models were retained alongside our study variables passing a p < 0.05 bivariate Pearson correlation screen with outcome. For the quality of life model, no prior study has predicted QOLIBRI outcomes in a comparable TBI rehabilitation sample. Variable selection therefore relied on bivariate correlations (p < 0.05) between our study variables and outcome.
Outcome variables
The MPAI-4 Participation scale score, obtained at least one year after discharge from outpatient rehabilitation, was used as the measure of social participation. Participants who had only MPAI-4 data collected at intake at least one year before but not at end of rehabilitation (e.g., because they continued rehabilitation at a different site) were also included. The psychometric properties of the French-Canadian version of the MPAI-4 are described elsewhere. 24
The QOLIBRI was used as a measure of health-related quality of life. It assesses the cognitive, affective, functional, relational, emotional, and physical domains of quality of life. 17 It has been adapted and validated in 10 languages.18,19,25
Statistical analysis
We used linear hierarchical regression to evaluate our prediction models, ensuring adherence to statistical assumptions. Consistent with Guerrette and McKerral (2023), predictors were organized into three sequential blocks representing pre-injury, injury-related, and post-injury characteristics. A fourth block was added, comprising MPAI-4 Abilities and Adjustment subscale scores at rehabilitation intake. These variables were placed in a separate final block because they represent a standardized clinical assessment of TBI-related functional status at the start of rehabilitation, which is a conceptually distinct category from the sociodemographic, injury, and post-injury variables in the earlier blocks—and entering them last allowed us to evaluate how much additional predictive value functional status at intake provided beyond all other predictors.
The dataset contained no significant outliers and minimal missing data. Any variable with a small number of cases (n < 10) was excluded from the analysis because of their potential to limit the stability and the generalizability of the estimated effects. While most variables met assumptions of normality, a few exhibited skewness and kurtosis values slightly exceeding the recommended thresholds. However, following Field’s (2013) recommendation, this deviation was deemed acceptable given the use of bootstrapped confidence intervals. 26
Multicollinearity was assessed using variance inflation factors (VIF) and tolerance statistics, which were all within acceptable limits. The independence of errors was tested with the Durbin–Watson statistic, yielding satisfactory results. All statistical analyses were conducted with a significance level of 0.05 and 95% confidence intervals. Python was used for all analysis.
Results
Descriptive statistics
Table 1 presents the descriptive statistics for the study participants, detailing key sociodemographic and pre-injury variables, as well as other variables of interest.
Descriptive Statistics and Participant Characteristics (N = 98)
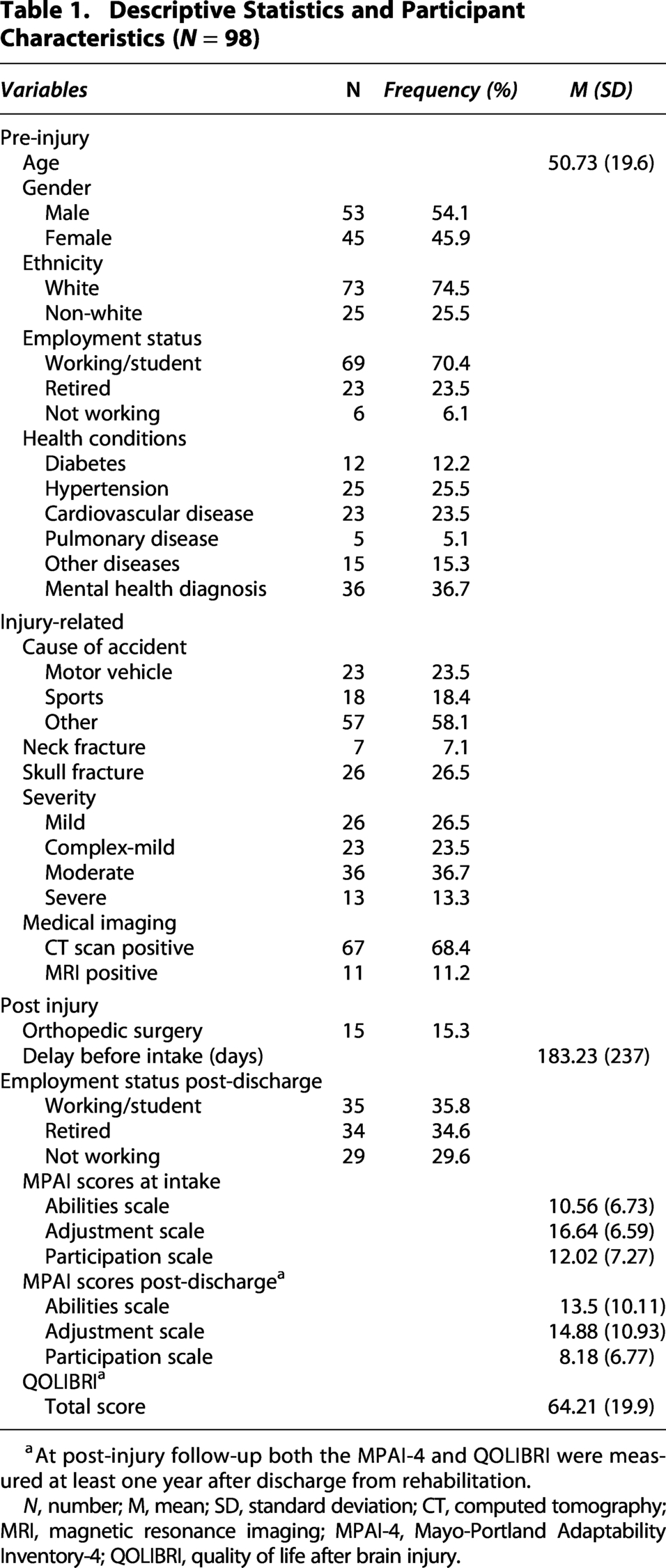
At post-injury follow-up both the MPAI-4 and QOLIBRI were measured at least one year after discharge from rehabilitation.
N, number; M, mean; SD, standard deviation; CT, computed tomography; MRI, magnetic resonance imaging; MPAI-4, Mayo-Portland Adaptability Inventory-4; QOLIBRI, quality of life after brain injury.
Social participation
Table 2 shows the bivariate correlations between social participation outcome and significant predictors from Guerrette and McKerral (2023), as well as the significant bivariate correlations between remaining study variables and outcome. The initial variable pool for the social participation model included education, premorbid hypertension, premorbid mental health diagnosis, delay between TBI and start of rehabilitation, MPAI-4 Abilities at intake, and MPAI-4 Adjustment at intake. We also included the following significant variables from our bivariate screen (p < 0.05): age at TBI and cause of injury—sports versus all other causes. In post hoc analysis, we verified and confirmed that motor vehicle and other causes of injury did not contribute any independent variance to the model.
Variables Correlated with Social Participation at Least One Year After Discharge from Rehabilitation
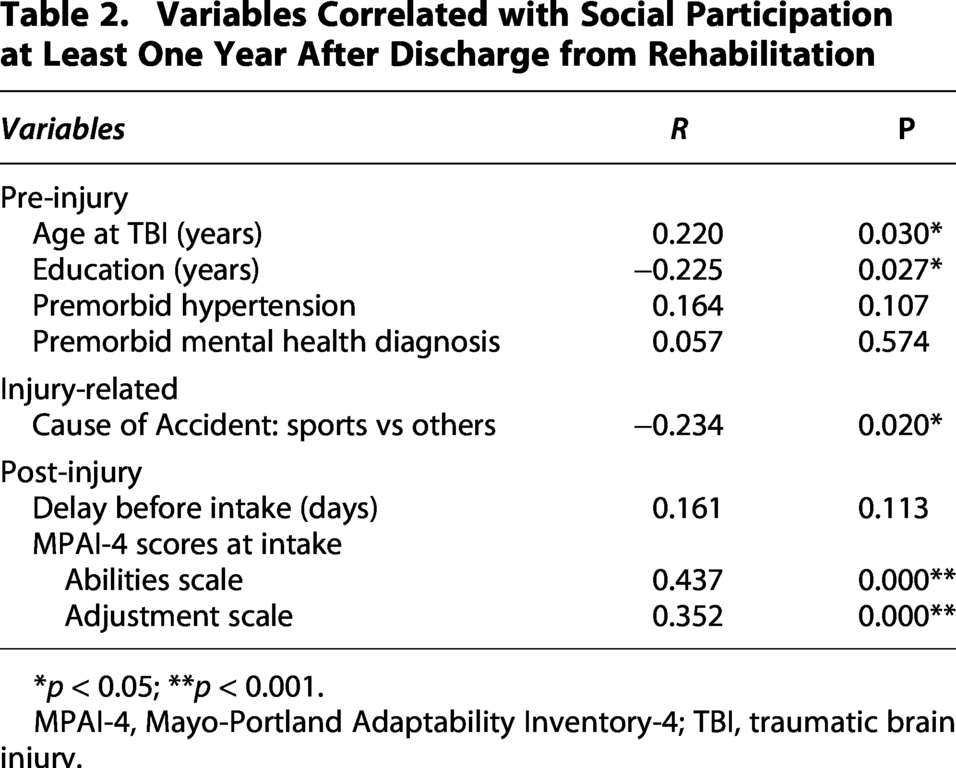
*p < 0.05; **p < 0.001.
MPAI-4, Mayo-Portland Adaptability Inventory-4; TBI, traumatic brain injury.
Rehabilitation hours received, a significant predictor in Guerrette and McKerral (2023), could not be included because it was collected at rehabilitation discharge from clinical records and was not available in the present follow-up dataset.
Table 3 presents the results of the hierarchical regression model predicting social participation at least one year after rehabilitation discharge. The final social participation model comprised eight predictors in four hierarchical blocks. The model was statistically significant, accounting for 33.5% of the variance. The optimism-corrected R2, estimated via bootstrap resampling (1,000 samples), indicated minimal overfitting.
Hierarchical Regression Predicting Social Participation (MPAI-4) at ≥1-Year Follow Up

95% CIs based on 1,000 bootstrap samples (percentile method). Age × Hypertension r = .547 (VIF age = 7.76; hypertension = 1.93). MPAI-4 Abilities × Adjustment r = .633 (VIF = 7.16 and 12.00); block-level ΔR² is primary inference for Block 4. The events-per-variable ratio (EPV) was 11.75.
†p < 0.10; *p < 0.05; **p < 0.001.
B, unstandardized coefficient; SE, standard error; β, standardized coefficient.
In the model, two variables were significant independent predictors. Delay between TBI and start of rehabilitation was a significant positive predictor, indicating longer delays were associated with worse participation. MPAI-4 Abilities at intake was a significant positive predictor, indicating higher functional impairment at the start of rehabilitation predicted worse participation one year later. Age and education showed trend-level associations in the expected directions. The two MPAI-4 subscales were correlated; the block-level ΔR2 provided the most reliable estimate of their combined contribution.
Quality of life
Table 4 shows the significant bivariate correlations between study variables and quality of life outcome. The final quality of life model comprised 10 predictors in four hierarchical blocks: sex, premorbid mental health diagnosis, TBI severity (complex mild), skull fracture, cause of injury (sports), delay between TBI and start of rehabilitation, employment status post-discharge (working, retired), MPAI-4 Abilities at intake, and MPAI-4 Adjustment at intake.
Variables Correlated with Quality of Life at Least One Year After Rehabilitation

*p < 0.05; **p < 0.01; ***p < 0.001.
MPAI-4, Mayo-Portland Adaptability Inventory-4; QoL, quality of life; SP, social participation.
Table 5 presents the results of the hierarchical regression model predicting quality of life at least one year after rehabilitation discharge. The model was statistically significant, accounting for 45.8% of the variance in quality of life. The optimism-corrected R2, estimated via bootstrap resampling (1,000 samples), indicated minimal overfitting. All four blocks contributed significantly to the model.
Hierarchical Regression Predicting Quality of Life (QOLIBRI) at ≥1-Year Follow-Up

95% CIs based on 1,000 bootstrap samples (percentile method). The events-per-variable ratio (EPV) was 9.5.
†p < 0.10; *p < 0.05; **p < 0.001.
B, unstandardized coefficient; SE, standard error; β, standardized coefficient.
Three variables emerged as significant independent predictors of quality of life at follow-up. The cause of injury—sport versus all other causes—was the strongest predictor, indicating that participants who sustained a sport-related TBI reported substantially better quality of life one year after rehabilitation discharge compared with those whose injury resulted from other causes. Employment status post-discharge was another significant predictor when employment status was compared with the nonworking group as the reference category: participants who were employed following discharge reported significantly better quality of life than those who were not working, corresponding to approximately 10 points on the QOLIBRI scale. MPAI-4 Adjustment subscale score at rehabilitation intake was also a significant negative predictor, indicating that more adjustment difficulties at the start of rehabilitation were associated with lower quality of life at follow-up of one year after rehabilitation discharge.
Discussion
Our study aimed to identify significant predictors of social participation (Participation scale of the MPAI-4) and quality of life (QOLIBRI) for individuals with TBI at least one year after the end of their rehabilitation. Longer delays to rehabilitation access and higher functional impairment at intake predicted lower social participation. Sports-related injury and being employed post-discharge predicted better quality of life, while lower adjustment at intake predicted lower quality of life.
Our findings about delay to access rehabilitation and functional impairment as predictors of social participation are consistent with previous research. Studies have shown that deficits in various elements of the MPAI-4 Abilities subscale affect social participation in individuals with TBI, including return to work, return to driving, and other variables.27–33 While these studies did not use the MPAI-4 Abilities subscale directly, they addressed many of its components. For example, a systematic review 34 noted that cognitive and behavioral sequelae often hinder successful professional outcomes, even many years post-injury. Likewise, it has been found that individuals who reported greater cognitive challenges and reduced mobility one year after injury experienced more employment instability. 35
For the other significant predictor of social participation in our study, which was the delay before intake into rehabilitation, research suggests that such delays can negatively impact recovery a year or more after completing a rehabilitation program.36–38 High Jr and colleagues 39 found that the greatest improvements on variables such as community integration were observed in patients who were admitted to post-acute rehabilitation within six months of their injury. These improvements continued even after discharge. Rehabilitation may exert its benefits not only by facilitating improvements in physical functions but also by preventing further declines in community functioning. 40
The second outcome studied was quality of life. The prediction model relied on bivariate screening applied to the variables of interest, as no prior study had examined predictors of quality of life in a comparable TBI rehabilitation cohort. Guerrette and McKerral’s (2023) findings pertaining to social participation could not be assumed to generalize to a different construct. The significance of the MPAI-4 Adjustment scale score at intake in our model may be explained by the cognitive and psychological impairments associated with TBI, which can continue to impact quality of life in the years after the injury. 41 Research literature has extensively explored various sub-elements that are captured by the scale, including mood outcomes related to anxiety and depression, irritability and anger, pain and fatigue, altered self-awareness, and, crucially, social support.42–46 The emphasis across studies is on the importance of accurate and timely assessment of these factors at the time of injury and the need for immediate, consistent intervention, beyond the rehabilitation phase, to ensure better and more sustainable psychosocial and behavioral adjustment outcomes.
Cause of injury was a significant predictor of quality of life, where TBI participants who had been injured through sports-related incidents had a better quality of life one year or more after discharge compared with those injured through other non-sports-related causes. Occupational reintegration appeared to be one of the associated mechanisms: 50% of sport-injured participants were employed post-rehabilitation discharge compared with 32.5% of those with other causes of injury. Previous research reached various conclusions in understanding this advantage47–51 and suggested that some characteristics of sport-injured individuals may account for this advantage, such as showing better recovery of mental health and post-concussion symptoms than those injured in another context, which may be associated with quicker return to regular exercise and more resilience to some post-TBI effects.
Our results also showed that participants who were employed post-discharge reported significantly better quality of life than those who were not. This finding is consistent with a considerable body of literature documenting the central role of return to work in health-related quality of life following TBI.52,53 More so, retired participants in our study did not differ significantly from nonworking participants, suggesting that the quality of life advantage of the employed group could reflect active occupational reintegration after TBI, rather than a general age-related effect or a pre-injury life course trajectory. These results underscore the importance of vocational and return-to-work objectives as integral components of TBI rehabilitation, since they clearly contribute to post-rehabilitation quality of life.
The social participation model in this study was developed as an extension of Guerrette and McKerral’ (2023) models, which predicted social participation in the same population using the same instrument. In both studies, functional abilities and delay before rehabilitation intake were significant predictors. This supports the conclusion that MPAI-4 functional status at the start of rehabilitation represents a durable prognostic marker whose predictive value persists well beyond the end of formal care. Likewise, no injury-related variable was a significant multivariate predictor of social participation, indicating that post-TBI impacts can vary across individuals with similar injury severity indicators. Compared with Guerrette and McKerral’s models that explained between 47% and 49% of variance in social participation, the present model explained 33.5%. A substantial part of this gap may be attributable to the rehabilitation hours variable, a significant predictor in their models, which could not be included in the present study as it was not available in the present follow-up dataset. It is also likely that different prognostic indicators of social participation that we did not capture are at play one year after rehabilitation versus at end of rehabilitation. It is noteworthy to underscore that the present study built on this previous work by adding a quality of life outcome at one year post-rehabilitation. The fact that the two outcomes studied have distinct predictor profiles reinforces that they measure different constructs and that both deserve attention in TBI rehabilitation and research.
Finally, it is worth noting that some participants in our study wished to emphasize after completing our questionnaires that they would have benefited from immediate counseling and guidance at the time of their TBI incident. They believed that early intervention could have helped them prevent rumination on their symptoms and their negative impacts. Future research should explore how access to early interventions and delay to rehabilitation intake affect such post-TBI difficulties. Many participants also stressed the wish to have benefited from regular follow-ups following rehabilitation. The availability and effects of such services should be appropriately studied since they could have a positive influence on TBI patients’ social participation and quality of life in the years after completing rehabilitation.
Study limitations
Several limitations must be considered in interpreting the findings of this study. First, the sample composition was relatively homogenous, possibly limiting the generalizability of findings to more diverse cultural backgrounds. Another issue lies in the inability to access some participants’ clinical information, which lowered sample size and may have reduced the robustness of the analysis. Also, there could be potential influence of unknown or unmeasured socio-environmental factors. For instance, participants who moved to a different city, experienced changes in access to professional resources, or faced the loss of family members might have experienced variations in their social participation and quality of life that are not captured in the study. Furthermore, a shift in the measurement modality represents a limitation of our study, as different rating methods were used at intake (clinician consensus rating approach) compared with the one-year follow-up (participant self-report via telephone interviews). These differing measurement modalities need to be taken into consideration when interpreting and generalizing the results. The reliance on self-reported measures to assess both social participation and quality of life can introduce bias. These responses may be influenced by individual perceptions, mood, or social desirability biases. Factors such as memory loss, impaired self-awareness, attention deficits, and fatigue could also affect participants’ responses on both the MPAI-4 and QOLIBRI instruments. These limitations should be addressed in future research to enhance the generalizability and validity of the findings.
Conclusions
Our study highlights the importance of studying specific predictors of social participation and quality of life outcomes of individuals with TBI in the years after completing rehabilitation. We conclude that employing the MPAI-4 and QOLIBRI measures are useful tools for evaluating patients’ self-perceived social participation and quality of life in the post-rehabilitation phase, respectively. This study demonstrated that participants with higher functional impairment and who showed a longer delay before accessing rehabilitation were at higher risk of experiencing sustained reductions in social participation. Participants with more adjustment difficulties had lower quality of life, and those whose TBI was sport-related and who were employed post-discharge reported higher quality of life. As these findings remain preliminary, future studies should focus on developing a more complete understanding of the variables that impact and predict social participation and quality of life in the years following rehabilitation. This should lead to the development of sustainable and cost-effective interventions that address the specific needs of patients with TBI and their support system after the end of formal rehabilitation services.
Transparency, Rigor, and Reproducibility Statement
This study was registered at ClinicalTrials.gov (Identifier: NCT05022940) and is reported in accordance with the STROBE statement for cohort studies. It is a longitudinal follow-up to Predictors of social participation outcome after traumatic brain injury differ according to rehabilitation pathways, conducted within an accessible and organized trauma continuum of care (Guerrette and McKerral, 2023). The sample size was determined by the number of participants meeting eligibility criteria (≥16 years at the time of TBI, with no premorbid neurodegenerative disease) and available for follow-up at least one year after discharge from rehabilitation. There were initially 348 adults (≥16 y at time of TBI) who were contacted by the rehabilitation sites at least one year after their discharge, of which 106 (30.5%) were unreachable. Of the remaining 242 participants, 171 (70.7%) consented to the follow-up assessment and 71 (29.3%) declined. Only data from participants who had a complete set of clinical information were included in the analyses (N = 98). Multiple linear regression analyses were conducted to evaluate the predictive models. The dataset contained no influential outliers and minimal missing data. Most variables met assumptions of normality; a small number exhibited skewness and kurtosis values slightly exceeding recommended thresholds. These deviations were considered acceptable given the use of bootstrapped confidence intervals, following Field (2013). Multicollinearity was assessed using VIF and tolerance statistics, and independence of errors was evaluated using the Durbin–Watson statistic. Dichotomous or categorical variables with fewer than 10 cases in any category were excluded to ensure robustness of the statistical models. All statistical analyses were conducted using a two-tailed significance level of 0.05 with 95% confidence intervals. Python was used for all analyses. The primary clinical outcome measures are established standards in the field. Validation of the MPAI-4 has been previously reported (Guerrette and McKerral, 2022), and validation of the QOLIBRI has been documented in prior studies (Giustini et al., 2014). The dataset generated and analyzed during the current study is not publicly available due to absence of prior authorization from participants to share their information with a third party, even if deidentified (Quebec Bill 25). Requests to share data can be addressed to the corresponding author; they will be considered on a case-by-case basis by the institutional review board and may require a data use agreement.
Authors’ Contributions
Z.A.: Data collection and management (lead), writing—original draft (equal), writing—review and editing (supporting), project administration (equal), visualization (lead), and validation (supporting). F.B.: Data collection (supporting), formal analysis (lead), writing—original draft (equal), writing—review and editing (supporting), methodology (equal), project administration (equal), and supervision (supporting). M.M.: Conceptualization (lead), funding acquisition (lead), methodology (equal), supervision (lead), validation (lead), and writing—review and editing (lead).
Footnotes
Acknowledgments
The authors wish to thank the clinicians and program managers from the TBI rehabilitation programs at the two Integrated University Health and Social Services Centres (CIUSSS) and the Integrated Health and Social Services Centre (CISSS) that participated in the study: the CIUSSS du Centre-Sud-de-l’Île-de-Montréal, the CIUSSS du Centre-Ouest-de-l’Île-de-Montréal, and the CISSS de Laval.
Author Disclosure Statement
The authors report no competing financial interests or other conflicts of interest.
Funding Information
This research was supported by a research grant from the Fonds de recherche du Québec—Santé (FRQS) to Michelle McKerral [grant number 254599].