
Abstract
Females of reproductive age with concussion often report greater symptom severity and duration than age-matched males; the mechanisms underlying female symptomology remain unclear. This study investigated the association between hormone profiles and time to return to learn/work (RTL/W) following concussion. A secondary aim was to explore differences in symptom severity and salivary miR-27a-5p/miR-30a-3p expression between hormone profile groups. Based on an a priori power calculation, 36 females aged 28.8 ± 7.5 (17–44 years) presenting to an emergency department within 72 h of a confirmed concussion were recruited. Participants were classified into three hormone profile groups: n = 20 natural menstrual cycle (NMC); n = 8 progestin-only hormonal contraception (PROG); and n = 8 oral contraception (Oral Contraceptive Pill; OCP). Saliva samples were collected for measurement of miR-27a-5p/miR-30a-3p, and participants completed weekly online surveys reporting symptom scores until achieving RTL/W. The mean initial symptom score was 47.0 ± 23.7 (8–100), and mean time to RTL/W was 27.3 ± 33.1 (2–179 days). Cox hazard regression revealed a statistically significant association of hormone profile with time to RTL/W. PROG (hazard ratio [HR]: 2.5, 95% confidence interval [CI]: 1.0–6.1, p = 0.048) and OCP (HR: 2.7, 95% CI: 1.1–6.4, p = 0.027) were significantly associated with increased likelihood of RTL/W compared with NMC. Initial symptom score was not significantly associated with time to RTL/W (p = 0.628). Exploratory analysis showed no statistically significant mean differences between groups for initial symptom score [F(2, 33) = 1.755, p = 0.189]. Fourteen saliva samples provided complete miR-27a-5p/miR-30a-3p data; mean miR-27a-5p/miR-30a-3p was 0.84 ± 0.06 (0.75–0.92). No statistically significant mean differences in miR-27/miR-30 expression were observed between hormone profile groups (F 2, 11 = 0.519, p = 0.609). Females using PROG or OCP were between 1.0 and 6.7 times more likely to achieve RTL/W than NMC at any given time. Hormone profile, but not initial symptom score, was predictive of time to RTL/W. Salivary miR-27a-5p/miR-30a-3p may be a useful biomarker in females with concussion and warrants further research.
Introduction
Concussion is a brain injury induced by direct or indirect biomechanical force being transmitted to the head via a blow to the head or the body. Disturbance in brain cellular homeostasis initiates complex biochemical and neurometabolic changes 1 resulting in a transient “energy crisis” in the brain. Concussion is a functional rather than structural injury and presents as a variable cluster of physical, cognitive, emotional, and sleep-related symptoms. Sex differences are evident in concussion; females often having more severe symptoms that are longer in duration when compared with males. 2 Underlying mechanisms for these observed sex differences are not yet well understood. Limited data show that the female hormone profile may be associated with recovery outcomes.3,4 The primary female sex hormones, estrogen and progesterone, have a modulatory effect on multiple body systems, including temperature regulation,5,6 macronutrient metabolism,5,7,8 central nervous system fatigue, 5 and brain bioenergetics.5,7,8 During the reproductive years, estrogen and progesterone fluctuate across the menstrual cycle, which typically lasts 21–35 days. 9
Diagnosis of concussion may not always be clear; assessment includes use of neurocognitive and physical tests and subjective symptom report. Immediate and early postinjury symptoms are reported as best predictors of recovery. 1 However, athletes or those who are subject to domestic violence may hide their injury and symptoms. Research investigating potential biomarkers of concussion has identified salivary miRNAs that can accurately discriminate between clinical diagnosis and absence of concussion,10–12 more specifically the ratio of two miRNAs has shown greater accuracy 10 and is advantageous because it does not require baseline measurement. These miRNAs could provide a useful objective adjunct as a sideline test and in the clinical environment to aid concussion diagnosis. However, these studies have focused on male athletic populations. Given that the miRNA expression in other central nervous system diseases is sex dependent 13 and there is a potential modulatory effect of sex hormones on concussion outcomes, findings of studies in male athletes cannot be extrapolated to female populations without further investigation.
This article presents findings from the Female RNA in Concussion (FeRNAC study) 14 ; the primary aim was to determine if time to return to learn/work (RTL/W) (in days) differs among females categorized by their hormone profiles at the point of concussion injury. The secondary aims were to explore (1) whether the salivary miRNA ratio differs across females categorized by their hormone profiles at the point of concussion injury; and (2) whether the initial self-reported symptom score differs among females categorized by their hormone profiles at the point of concussion injury.
Methods
The study was performed in accordance with the ethical standards of the Declaration of Helsinki, given that the ethical approval was obtained from the Health and Disability Ethics Committee (HDEC #2021 EXP 11655), Auckland University of Technology Ethics Committee (AUTEC #22/110), and locality consent through the Hutt Valley hospital research office on November 24, 2021. Written informed consent was obtained from all participants.
Study design
The prospective cohort study recruited female participants from an emergency department (ED) in Lower Hutt, New Zealand. This study used a previously published protocol 14 and included an a priori sample size calculation that estimated 30 participants were needed to have adequate power to examine the primary study aim and detect a hazard ratio (HR) of 1.5 (log HR coefficient = 0.4055), with 80% power, and type I error rate of 0.05. This was calculated assuming a covariate standard deviation (SD) of 1.5, multiple regression R2 (variable of interest regressed on covariates) of 0.2, and expected event (RTL/W) rate of 0.9 within the 6-month follow-up.4,15 To allow for 20% dropout rate during follow-up, 38 participants were recruited.
Participants
Thirty-eight females of reproductive age (16–42 years) presenting to the ED within 3 days of injury and receiving a confirmed concussion diagnosis were recruited by ED health care practitioners. Diagnostic criteria for concussion were those outlined in the most recent international consensus statement from the concussion in sport group. 1 Exclusion criteria were as follows: three or more previously diagnosed concussions, current concussion was more than 3 days prior, postmenopausal, started taking medication that would alter reproductive hormone concentrations (corticosteroids, e.g., prednisone, antidepressant or antipsychotic medication) within the last 3 months, current clinical diagnosis of an eating disorder, prediagnosed psychiatric disorder or neurological condition, polycystic ovarian syndrome, oligomenorrheic (irregular periods), amenorrheic (loss of periods for 3 months or longer), GCS* score less than 15 at 4 h after the initial assessment. These patients may be referred for a CT scan and are not eligible for the study. The routine concussion assessment and study flow are detailed in Figure 1.
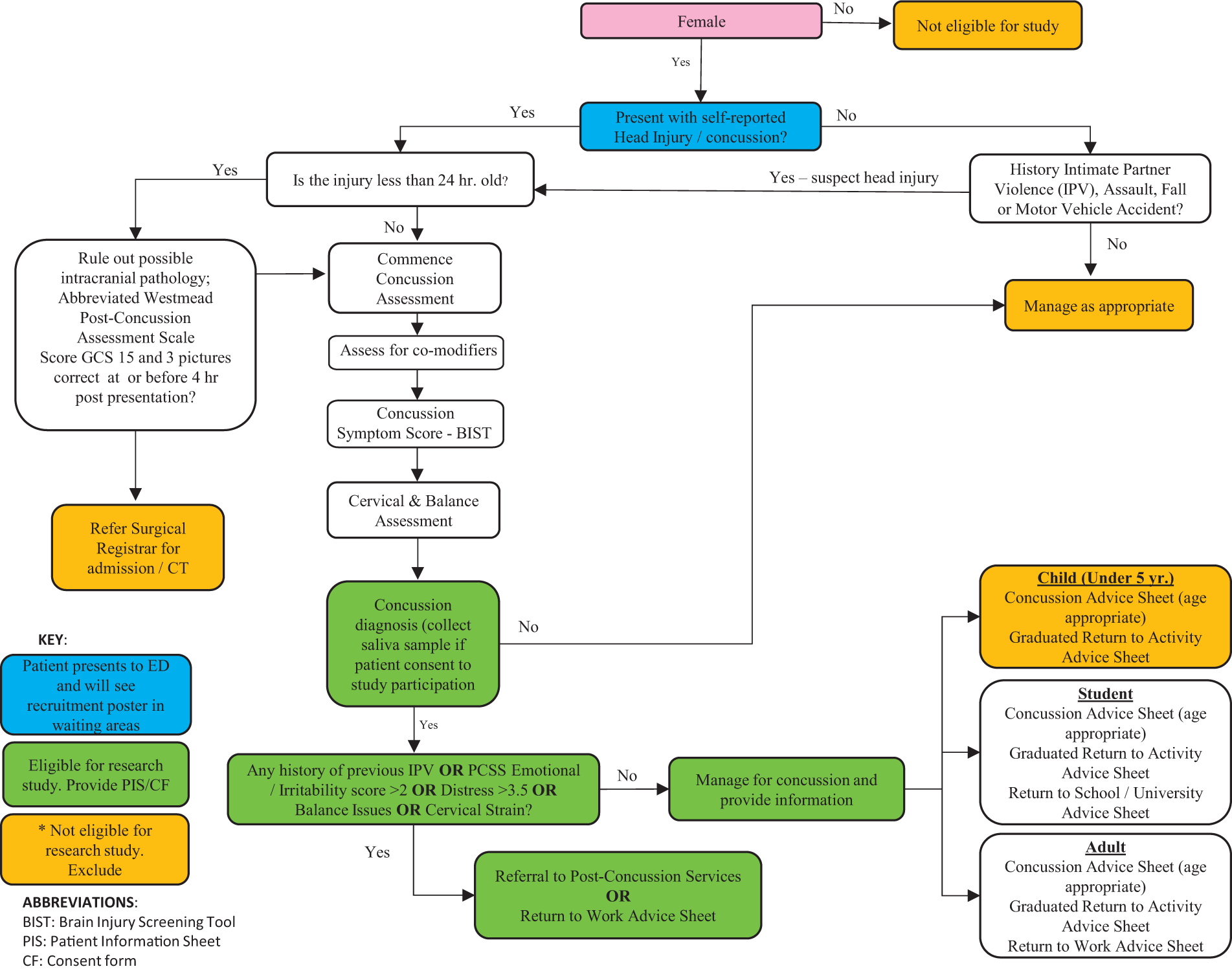
Routine clinical assessment and study flow.
Given that interpersonal violence disproportionately affects females, to ensure safeguarding of any participants in this study who may have been vulnerable, the Ministry of Health Family Violence Assessment and Intervention Guideline was utilized. 16
Procedures and measures
Due to logistics, adopting best practice research methodologies, and refinement of the technique for evaluation of miRNA, it was necessary to make modifications to the published protocol, including storage of saliva samples, recategorization of hormone profile, and the endogenous control gene used in miRNA analyses.
Data provided by participants included a 2 mL saliva sample to measure miRNAs collected in Thermo Fisher Scientific (TFS) SpeciMAX tubes prefilled with 1 mL of virus-inactivating and nucleic stabilization solution to protect against RNA degradation, and two different follow-up surveys administered online weekly until the participant reported full RTL/W. The surveys were (1) the Low Energy in Females Questionnaire (LEAF_Q) to monitor Low Energy Availability (LEA) and reproductive status; and (2) the Brain Injury Screening Tool to monitor symptoms. 17 A LEAF_Q total score of ≥8 (in combination with an injury score ≥2 and/or menstruation dysfunction score ≥4) was used to identify those having symptoms of LEA. 18 Saliva samples were stored in the ED freezer at −20°C and then transferred to the −80°C freezer within 3 months of initial collection and were stored until the point of processing and analyses.
Hormone profile
The hormone profile groups examined were (1) natural menstrual cycle (NMC); (2) progestin-only contraception (PROG), which included the Jadelle implant and the Depo-Provera injection; and (3) oral contraceptive pill (OCP). The PROG and OCP groups were examined separately (rather than as one contraceptive group) due to the different delivery modes and pharmacokinetic properties of each method. The NMC group was examined as one hormone profile group rather than the three separate phases outlined in the original protocol due to the lack of certainty of phase estimation when applying the backward calculation method particularly when estimating midcycle. For example, a participant with a date of injury 13.11, completed the LEAF_Q 17.11 and reported her last period as 2 weeks ago. Therefore, she could have been anywhere from day 4 to 10 of her cycle on the day of injury.
MicroRNA expression analysis
For consistency with the previous study12,19 utilizing the miR-27a-5p/miR-30a-3p ratio for differentiating concussed from nonconcussed individuals, miR-16-5p was used as the reference gene. As miR-16-5p only amplified in 34% of samples, a second suitable reference gene, 19 miR-25-3p, was used and amplified in 69% of samples. In samples where both reference genes were amplified, the ratio values for miR-27a-5p/miR-16-5p/miR-30a-5p/miR-16-5p and miR-27a-5p/miR-25-5p/miR-30a-5p/miR-25-5p were identical. Therefore, miR-25-3p was used as the endogenous control for all samples included in final analyses. Details of information collected each week are included in Table 1.
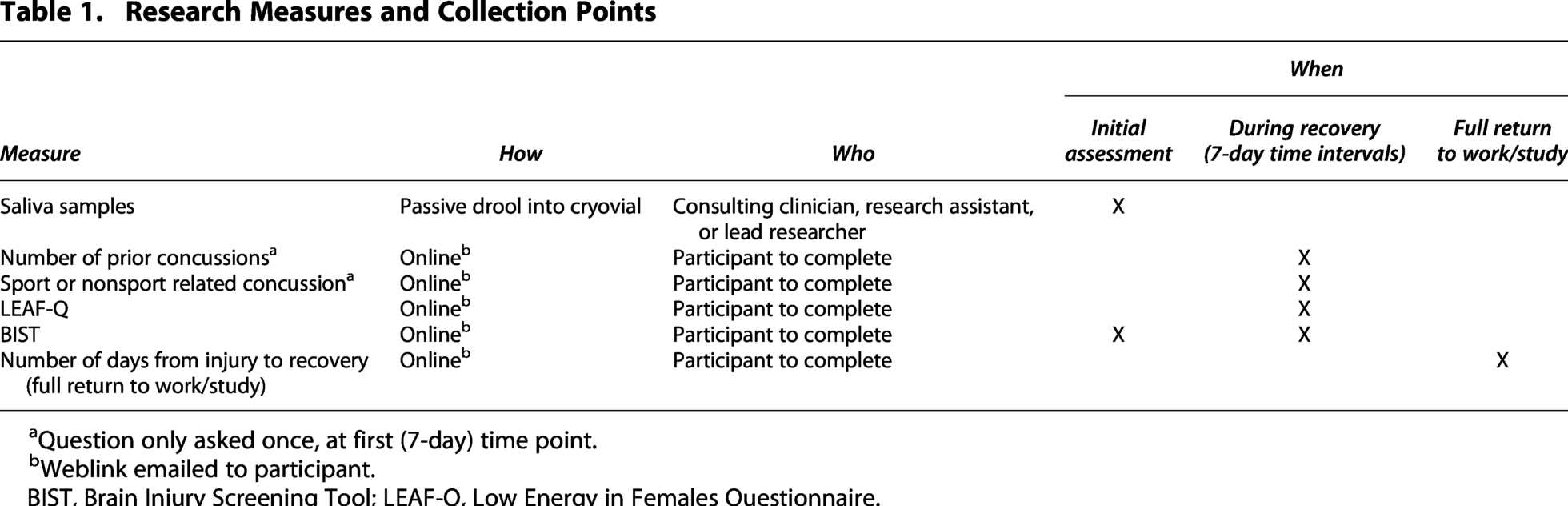
Question only asked once, at first (7-day) time point.
Weblink emailed to participant.
BIST, Brain Injury Screening Tool; LEAF-Q, Low Energy in Females Questionnaire.
Statistical analyses
All data were captured, cleaned, and coded for analysis in Microsoft Excel 2024 (version 16.0.18324.20092). Data were imported into JASP (Version 0.19.3; JASP Team, 2020) statistical software for analysis. To examine the associations between hormone profile or initial symptom score and time to RTL/W, a Cox proportional hazards regression was conducted. The model assumed that the HRs were constant over time (proportional hazards assumption). The time-to-event variable was defined as the duration from point of injury to RTL/W in days. The proportional hazards assumptions were found to be met when tested using Scaled Schoenfeld residuals. Model adequacy was verified through log-minus-log plots and concordance statistics. HRs with 95% confidence intervals (CIs) were reported. Levene’s test was nonsignificant for miRNA (p = 0.223) and symptom data (p = 0.732), indicating that the assumption of homogeneity was not violated. No deviations were noted in normality checked, utilizing a Q-Q plot that graphically compared the distribution of the two data. Two separate one-way ANOVAs were used to determine whether there were significant mean differences between hormone profile groups for initial symptom score and miR ratio. The statistical significance level was set at p < 0.05 for all analyses.
Results
Of the 38 participants recruited, one was excluded due to using the hormonal contraceptive coil and one had one set of data excluded due to having already participated in the study with a prior concussion. Table 2 outlines the demographic information of the remaining 36 participants. The mean LEAF_Q score was 4.8 ± 2.6 (2–10). Based on these scores, no participants were considered at risk of LEA. Twenty-seven percent of participants reported history of amenorrhea. One participant was a full-time mum; therefore, her RTL/W was taken as the number of days until her symptoms no longer impacted on her ability to achieve all daily tasks and in doing so there was no provocation of her symptoms.
Demographic Information
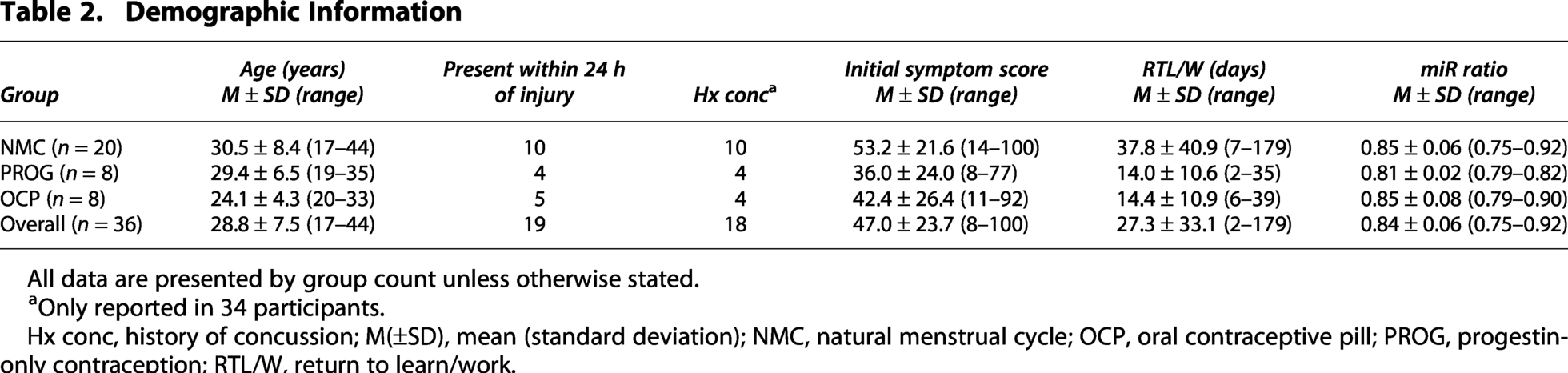
All data are presented by group count unless otherwise stated.
Only reported in 34 participants.
Hx conc, history of concussion; M(±SD), mean (standard deviation); NMC, natural menstrual cycle; OCP, oral contraceptive pill; PROG, progestin-only contraception; RTL/W, return to learn/work.
Hormone profile and time to RTL/W
Analysis of 36 participants showed that RTL/W was achieved within a mean follow-up of 27.3 ± 33.1 (2 to 179) days. There was a statistically significant association of hormone profile with time to RTL/W. Both PROG (HR = 2.5; 95% CI: 1.0–6.1, p = 0.048) and OCP (HR = 2.7; 95% CI: 1.1–6.4, p = 0.027) were significantly associated with increased likelihood of RTL/W. Initial symptom score was not significantly associated with time to RTL/W (p = 0.628) (Fig. 2).
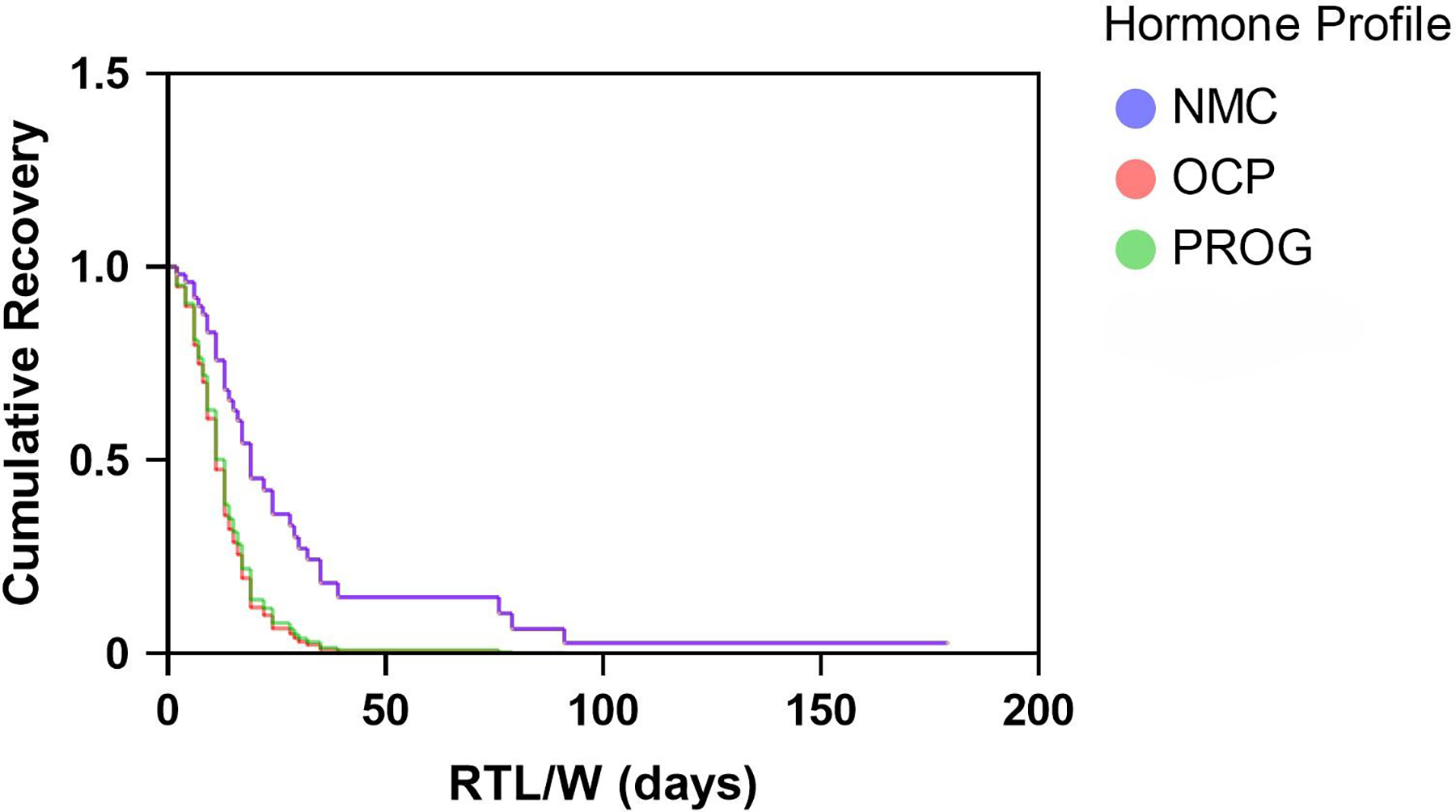
Recovery probability by hormone profile. NMC, natural menstrual cycle; OCP, oral contraceptive pill; PROG, progestin-only contraception; RTL/W, return to learn/work.
Expression of miRNA ratio
Of the 36 samples collected, 29 (81%) amplified miR-27a-5p and 14 (39%) amplified miR-30a-3p, and therefore, only 14 samples that amplified both miRNAs and could provide a ratio were included in data analyses. There was no statistically significant difference between groups for expression of miR-27/miR-30 [F(2, 11) = 0.519, p = 0.609].
Symptoms
There was no statistically significant difference between groups for the initial symptom score [F(2, 33) = 1.755, p = 0.189].
Discussion
How hormonal contraceptives downregulate endogenous hormones
Hormonal contraceptives downregulate endogenous hormones through inhibition of the hypothalamic–pituitary–ovarian axis. 20 The implant is a long-acting reversible contraceptive administered subcutaneously that delivers low-dose, steady-state concentration of progestin. The contraceptive injection is administered intramuscularly, works in the same way as the implant, and is effective between 8 and 13 weeks. 21 Both methods are parenteral 21 and therefore enter the bloodstream directly and do not undergo first-pass metabolism in the liver. 22 The OCP is ingested, undergoes first-pass metabolism before being released into systemic circulation, and needs to be administered daily to maintain serum concentrations of exogenous hormones at levels sufficient to provide contraceptive efficacy. 22 The OCP primarily interrupts the feedback loops between the hypothalamus, pituitary, and the ovaries due to the synthetic hormones in the bloodstream, whereas the progestins in the implant/injection can also bind to progesterone receptors in the hypothalamus. In addition, contraceptive progestins appear to alter the serotonergic system and modulate inhibitory GABA-ergic signaling in the brain. 23 Importantly, brain interaction and effect on mood and cognition may be different between the two contraceptive methods and still not fully understood. 24
Associations of hormone profile and symptom severity with time taken to RTL/W
Females in this study using either form of contraception (OCP or PROG) were 1.0–6.4 times more likely to have achieved RTL/W than those in the NMC group at any given time. There was no statistically significant association between initial symptom score and RTL/W, indicating that hormone profile and not initial symptom score was a predictor of time to RTL/W. Given the wide CI and that the lower value is 1.0, there is uncertainty about the magnitude of the effect. There was a nonsignificant trend toward a higher early postconcussion symptom score in those participants in the NMC group. These findings were somewhat consistent with other studies3,4,25 investigating whether HCs or menstrual cycle phase at the point of injury affects postconcussion outcomes, all of which reported that females using HC or in the follicular (low hormone) phase (FP) of the menstrual cycle had better QoL scores, 4 lower symptom scores,3,4,25 and a trend toward shorter length of recovery.3,25 This may not necessarily reflect that HC offers a neuroprotective effect or that females using HC physiologically recover faster, rather that HC may modulate symptoms that these females experience. It is also possible that hormone-related symptoms are misattributed to concussion during recovery from the injury.
Given that some females use hormonal contraception to reduce premenstrual symptoms, 21 that females respond differently to various forms of hormonal contraception available, and some experience side-effects and others do not, it is plausible that females in this in study self-selected the form of hormonal contraception that was optimal for them, with minimal side-effects and general reduction in symptoms. This participant bias would have been reflected in these study results. In addition, two different studies4,25 reported that females in the menstrual cycle FP at point of injury also had better outcomes when compared with those in the luteal phase and that there were no differences between FP and HC. 4 Collectively, these studies suggested that the low endogenous hormone state may be associated with lower symptom severity and shorter length of recovery. However, given that the length of recovery is typically measured by RTL/W or return to sport and that this is informed by the subjective symptom report, it remains unclear whether this reflects a true physiological recovery or only lessening of symptoms. Early postinjury symptoms are cited as the best predictor of recovery1,26 and that females are at greater risk for having symptoms that persist for more than 1 month. 26 Yet, 80% of data informing consensus statements are still based on males 27 and a seemingly overlooked data point from one study with 90 participants 3 showed that symptom severity was a strong predictor of recovery time in males (r = 0.051, p < 0.01) but not in females (r = −0.003, p > 0.05). The current study builds on this finding showing that symptoms were not a significant predictor of time to RTL/W, but that the hormone profile was; in those females using contraception, time to RTL/W was shorter.
Salivary miR ratio
Sex differences in postconcussion symptoms have been hypothesized to stem, in part, from reporting bias from females. A different perspective is that both males and females report their concussion experiences, which differ in nature and response. Both may be equally susceptible to deliberate non-disclosure or hiding of symptoms. Being focused on symptoms as a predictor or marker of recovery is probably insufficient and the ambiguity around symptom reporting, and experience, highlights the need for more objective measures of concussion and recovery. A novel aspect of the current study was inclusion of sampling and measurement of the ratio of concussion-specific salivary miRNA (miR-27a-5p/miR-30a-3p) in a female cohort presenting to the ED. Of the 36 samples collected, only 14 (39%) amplified both miRNAs (miR-27a-5p and miR-30a-3p) of interest and the endogenous control gene. In those 14 samples, all miR-27a-5p/miR-30a-3p ratios were less than 1, consistent with the findings of Hicks 12 for being indicative of concussion in the acute phase of the injury. Comparing mean ratio values across hormone profile groups revealed no meaningful differences; this suggested that the miR ratio could be a useful objective measure of concussion in females and that it was not affected by circulating exogenous hormones. Further research examining different menstrual cycle phases would be needed to confirm whether fluctuating endogenous hormones affect this measure. In addition, given that 76% of samples amplified miR-27a-5p but not miR-30a-3p, it may be there are other factors that can affect the regulation and abundance of miR-30a-3p and whether it is amplified or not. Differences in experimental design affect miRNA expression. From the technical or methodological perspectives, saliva collection method and storage, miRNA extraction and isolation, and miRNA expression profiling and aligner technique (in next-generation sequencing) must be considered. Use of an RNA stabilizer and the saliva collection method are two technical factors that account for most variance. 19 In the current study, the RNA stabilizer was used, however, the method of sample collection was passive drool, which may have affected the variance in whether the target miRNA was expressed and could be amplified. In addition, miRNA expression may be dependent on participant factors, including age, sex, prandial status, exercise, and BMI, 19 and there is also evidence of diurnal variation in salivary miRNAs. 28 Further research is needed to achieve consistency in the methodological approach to salivary miRNA measurement, the exclusion of miRNAs confounded by numerous biological factors, and to identify appropriate miRNA controls.
Limitations of the study
This study considered whether hormone profile (menstrual cycle, contraceptive use) affected time to RTL/W and salivary miRNA expression following concussion and contributed to addressing gaps in understanding female-specific responses to concussion. However, there were some study limitations that must be considered when interpreting the results. RTL/W was a proxy for recovery from concussion and did not necessarily reflect full physiological healing of the brain. In addition, RTL/W can also relate to other factors that are independent of symptoms, for example, financial considerations and social expectations. Information regarding treatment interventions and follow-up appointments for each participant was not collected, and therefore, it was unknown if or how ongoing management may have affected overall outcome. Similarly, reporting of information regarding the mechanism of injury (e.g., sport vs. nonsport related) was inconsistent and therefore not factored into the analyses. Hormone profile categorization was based on self-report responses to the LEAF_Q and did not include verification with any objective measurement. Data from those participants with NMCs were analyzed as one group and did not examine whether a specific menstrual cycle phase affected any outcome variables. The hormonal contraceptions included in analyses were the OCP and the progestin-only implant or injection, which means the findings may not apply to females using IUD, IUS, or the vaginal ring. Those using OCP were analyzed as one group and therefore the different types of OCP were not examined. Despite the use of self-report information in this study, the LEAF_Q is a valid questionnaire that provides a degree of standardization to the answers and although there is no quantification of hormone concentrations, what is known is that the circulating levels of endogenous hormones would be lower and more stable in both the contraceptive groups when compared with the NMC group. Only 14% of saliva samples amplified all miRNAs, and therefore, the findings from the data analysis of these 14 samples were limited due to the reduced sample size. Although the study sample size was based on an a priori power calculation, 14 this was to address the primary aim of the study, and only allowed for one covariate (symptoms) to be included in the analyses. Future larger studies should also consider other potential confounders, including age and mechanism of injury.
Conclusion and recommendations
This study combined with earlier research is indicative that hormone profile may be associated with concussion recovery in females. Collecting reliable, objective hormone data is a key component missing from this study and from earlier work and needs to be included in future female-specific concussion research. This can be difficult when conducting research in clinical environments, particularly a busy ED. The current study also demonstrated that saliva sampling is a feasible noninvasive biomarker sampling method that can be used by clinicians in an ED environment. However, further work needs to be done to validate the technique and use of the miRNA ratio as a concussion biomarker and to continue to understand how that correlates with hormone profile and symptom severity. This would be valuable to improve diagnostic accuracy and confirmation of recovery.
Authors’ Contributions
N.H.: Conceptualization and methodology, resources, investigation, formal analysis and data curation, writing—original draft, and writing—review and editing. P.A.H.: Conceptualization and methodology, formal analysis and data curation, and writing—review and editing. S.S., D.K., and I.B.: Conceptualization and methodology, and writing—review and editing. All authors have read and approved the final version of the article and agree with the order of presentation of the authors. The opinions expressed are solely those of the authors and do not necessarily reflect those of the
Footnotes
Acknowledgments
The authors thank Tom Stewart for his advice in developing the statistical analysis plan and Professor Alice Theadom and Drs Ken Quarrie, Stevphen Kolose, and Trevor Clark for providing scientific peer review and Māori and Pasifika peer review. The authors also acknowledge the technical support from the Awanui Group in the analysis of the salivary miRNAs.
Ethical Considerations
The study was performed in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Health and Disability Ethics Committee (HDEC #2021 EXP 11655), Auckland University of Technology Ethics Committee (AUTEC #22/110), and locality consent through Hutt Valley hospital research office on November 24, 2021. Written informed consent was obtained from all participants.
Data Availability
Data are available from the corresponding author (N.H.) upon reasonable request.
Transparency,Rigor,and Reproducibility Summary
The study was preregistered at the Australian New Zealand Clinical Trials Registry (ANZCTR); registration number ACTRN12623001129673. The analysis plan was published in a protocol article after starting data collection but before data analysis in BMC Neurology (![]() ). Allowing for 20% dropout during follow-up, a sample size of 38 was planned based on a Cox proportional hazards regression model to allow the detection of a HR of 1.5 (log HR coefficient = 0.4055), with 80% power, and a type I error rate of 0.05. This was calculated assuming a covariate SD of 1.5, a multiple regression R2 (variable of interest regressed on covariates) of 0.2, and an expected event (RTL/W) rate of 0.9 within the follow-up period. Forty-four potential participants were screened, 38 participated, and complete data were obtained from 36. Participants were aware of the outcome of their clinical assessments as they received a diagnosis of concussion, and were aware of their symptom and LEAF-Q scores throughout the study as they were self-report. Participants were told the results of their miR ratio at the end of the study through a study summary report. Initial data collection was performed by ED staff carrying out routine clinical assessment and were therefore aware of relevant participant characteristics. Data analyses were performed by investigators who were aware of relevant characteristics of the participants. Data were labeled using codes linked to participant-identifying information. Data were acquired between January 2023 and May 2025 at different times of the day based on patient presentation to ED. Salivary miRNA data were collected using SpeciMAX Stabilized Saliva Collection Kits (TFS SpeciMAX Stabilized Saliva Collection Kit A50697, Life technologies Corp, Austin, Texas USA), which were prefilled with 1 mL of virus-inactivating and nucleic stabilization solution. Saliva samples were analyzed in three separate groups, with samples assigned to batches in the order they were acquired.
). Allowing for 20% dropout during follow-up, a sample size of 38 was planned based on a Cox proportional hazards regression model to allow the detection of a HR of 1.5 (log HR coefficient = 0.4055), with 80% power, and a type I error rate of 0.05. This was calculated assuming a covariate SD of 1.5, a multiple regression R2 (variable of interest regressed on covariates) of 0.2, and an expected event (RTL/W) rate of 0.9 within the follow-up period. Forty-four potential participants were screened, 38 participated, and complete data were obtained from 36. Participants were aware of the outcome of their clinical assessments as they received a diagnosis of concussion, and were aware of their symptom and LEAF-Q scores throughout the study as they were self-report. Participants were told the results of their miR ratio at the end of the study through a study summary report. Initial data collection was performed by ED staff carrying out routine clinical assessment and were therefore aware of relevant participant characteristics. Data analyses were performed by investigators who were aware of relevant characteristics of the participants. Data were labeled using codes linked to participant-identifying information. Data were acquired between January 2023 and May 2025 at different times of the day based on patient presentation to ED. Salivary miRNA data were collected using SpeciMAX Stabilized Saliva Collection Kits (TFS SpeciMAX Stabilized Saliva Collection Kit A50697, Life technologies Corp, Austin, Texas USA), which were prefilled with 1 mL of virus-inactivating and nucleic stabilization solution. Saliva samples were analyzed in three separate groups, with samples assigned to batches in the order they were acquired.
All surveys and questionnaires used are available from the authors. The key inclusion criteria are established standards in clinical practice. Key inclusion criteria were assessed by investigators with professional qualifications in emergency medicine and expertise in the field of concussion. Replication by the study group is planned. Deidentified data from this study are not available in a public archive. Deidentified data from this study will be made available (as allowable according to institutional IRB standards) by emailing the corresponding author as of October 15, 2025. The authors agree to provide the full content of the article on request by contacting
Author Disclosure Statement
This research is part of the lead author’s (N.H.) PhD. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The New Zealand