
Abstract
Background:
The rapid expansion of telehealth, which was accelerated by the COVID-19 pandemic, has outpaced standardized approaches to data capture, resulting in fragmented documentation and limited research infrastructure. A centralized telehealth taxonomy would be useful for improving documentation, evaluating utilization, and informing decision-making. However, no comprehensive telehealth taxonomy has been developed to date.
Methods:
A scoping literature review was conducted to identify the characteristics needed to build a comprehensive telehealth taxonomy that informs a data repository. Then, a hybrid hierarchical mind map taxonomy was built using the frameworks and concepts from the reviewed articles, along with insight and feedback from eight telehealth domain experts. The taxonomy was revised using an iterative process, and the final version was approved by the domain experts.
Results:
Ten articles were ultimately included in this scoping review. Based on the findings of those articles, the final taxonomy includes 14 core variables that span the full telehealth appointment, including previsit preparation, during-visit interactions, and postvisit follow-up. The variables are arranged across both patient and provider perspectives. The taxonomy includes four dimensions: synchronous and asynchronous modalities, user perspectives, functionality, and payment considerations. Furthermore, the taxonomy aligns with electronic health record data fields, thus promoting interoperability and structured data capture.
Discussion:
The unified framework developed herein aims to bridge gaps in telehealth research by providing a scalable, interoperable foundation for data repositories. Ultimately, this taxonomy lays the groundwork for improved telehealth data infrastructure and can enhance research, clinical care, and data-informed policy development.
Introduction
The COVID-19 pandemic led to unprecedented growth in the adoption of telehealth, revealing and amplifying existing weaknesses in health data systems. 1 Research and policy efforts related to telehealth have become fragmented due to the absence of centralized, standardized data. In addition, the lack of comparable and well-structured data limits evidence-based decision-making, innovation, and the ability to optimize health care delivery. 2 While challenges related to inconsistent documentation and heterogeneous terminology are not unique to telehealth, their impact became more visible during the pandemic. 3 These inconsistencies created barriers related to billing, insurance authorization, and reimbursement, sometimes delaying care or preventing patients from receiving timely services. 4
Existing telehealth programs often collect data using program-specific fields and terminology. However, even when data are stored in a centralized repository, the lack of standardization yields datasets that are difficult to compare or aggregate across programs.5,6 Misalignment between traditional fee-for-service models and telehealth delivery further complicates consistent documentation and assessment of utilization, cost-effectiveness, and patient outcomes. 7
Standardized data within a centralized telehealth repository are essential for improving documentation, evaluating utilization, and informing decision-making. 8 A taxonomy provides the required foundation because it is a structured classification schema that organizes concepts and defines their relationships. 9 By standardizing telehealth encounter data, a telehealth taxonomy can support accurate billing, timely patient care, cross-institutional research, and evidence-informed policy decisions; furthermore, a taxonomy can provide conceptual clarity regarding the growing set of alternatives to in-person health care.1,8 However, to our knowledge, a comprehensive telehealth taxonomy that illustrates the key data elements involved in the telehealth encounters does not exist. To lay the groundwork for a centralized data repository with standardized data, we engaged in a two-step process. First, we conducted a literature review to identify the characteristics needed to build a comprehensive telehealth taxonomy that informs the data repository. Then, we iteratively developed a telehealth taxonomy through consultation with domain experts. The result was a telehealth taxonomy ready for field testing and validation in the US context with the potential for global application after country-specific tailoring.
Methods
Team members (K.S.Y., E.M., and Suguna.K.) conducted a systematic search in the Cochrane, EBSCO, Embase, PubMed, and SCOPUS databases for all records through September 25, 2025, using the key words “telemedicine,” “taxonomy,” “virtual consult,” and “information architecture” and related terms (see Appendix A for search strategy). The search results were uploaded to Covidence, and duplicates were removed. The research team then screened the titles and abstracts of the articles for relevance; potentially relevant articles were then subjected to full-text screening based on the inclusion and exclusion criteria.
Eligibility criteria
The inclusion criteria were as follows: studies that proposed, developed, or applied a taxonomy or classification framework related to telehealth, telemedicine, or digital health; peer-reviewed journal articles, conference proceedings, or reports; and published in English. The exclusion criteria were as follows: the absence of a taxonomy; focus limited to technical infrastructure; nonrelevant study outcomes (not relevant to taxonomy development or application); nonrelevant or no study design (e.g., commentaries, editorials, opinion pieces without original data or framework development); non-health care or other nonrelevant settings (e.g., veterinary care); non-US studies (to maintain the applicability of the taxonomy to the US health care context); nonrelevant populations (e.g., pediatric-only, geriatric-only populations); non-English studies; and articles unavailable in full text. There were no restrictions on publication date.
Taxonomy development
A study team member (K.S.Y.) extracted and synthesized the concepts and variables from the included articles, evaluated them for relevance to telehealth appointments and electronic health record (EHR) data capture, and developed a preliminary hierarchical list of variables for use in the next phase. The extracted variables were further reviewed by the principal investigator. Subsequently, K.S.Y. consulted with eight domain experts in telehealth and digital health, all of whom were members of the Center for Virtual Care and Excellence (ViVE) at the authors’ institution (Table 1). These experts were not compensated for their time. The telehealth taxonomy was developed via an iterative process: it was initially presented to the experts; their feedback was solicited and incorporated; and the updated taxonomy was presented to the experts again 5 weeks later. During the former presentation, the experts provided feedback regarding which variables to include and exclude, how to ensure clinical relevance, and how to enhance the practical applicability of the taxonomy. After the experts agreed on the feedback provided by their colleagues, the suggestions were incorporated during the revision of the taxonomy, and the final version was approved by the domain experts.
Domain Experts Consulted During Telehealth Taxonomy Development
To represent the complex relationships between concepts, the variables extracted during the literature review were organized into a preliminary hybrid hierarchical mind map structure using Miro (RealtimeBoard, Inc., San Francisco, CA). The mind map supported nested subconcepts while maintaining clear organization and navigability. The final design facilitated alignment with structured data fields in EHRs to inform standardized telehealth data repositories.
Results
Literature review
A total of 1,546 records were identified through the literature search: 85 in Cochrane, 486 in EBSCO, 52 in Embase, 262 in PubMed, and 661 in SCOPUS. Twenty-three duplicate studies were removed prior to screening, and 1,475 studies were excluded during title and abstract screening due to a lack of relevance. The full texts of the remaining 48 records were screened, with 38 excluded for nonrelevant setting (n = 9), nonrelevant outcomes (n = 1), nonrelevant or no study design (n = 25), and nonrelevant patient population (n = 3). Ultimately, 10 articles were included in the review. Figure 1 shows the search strategy according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
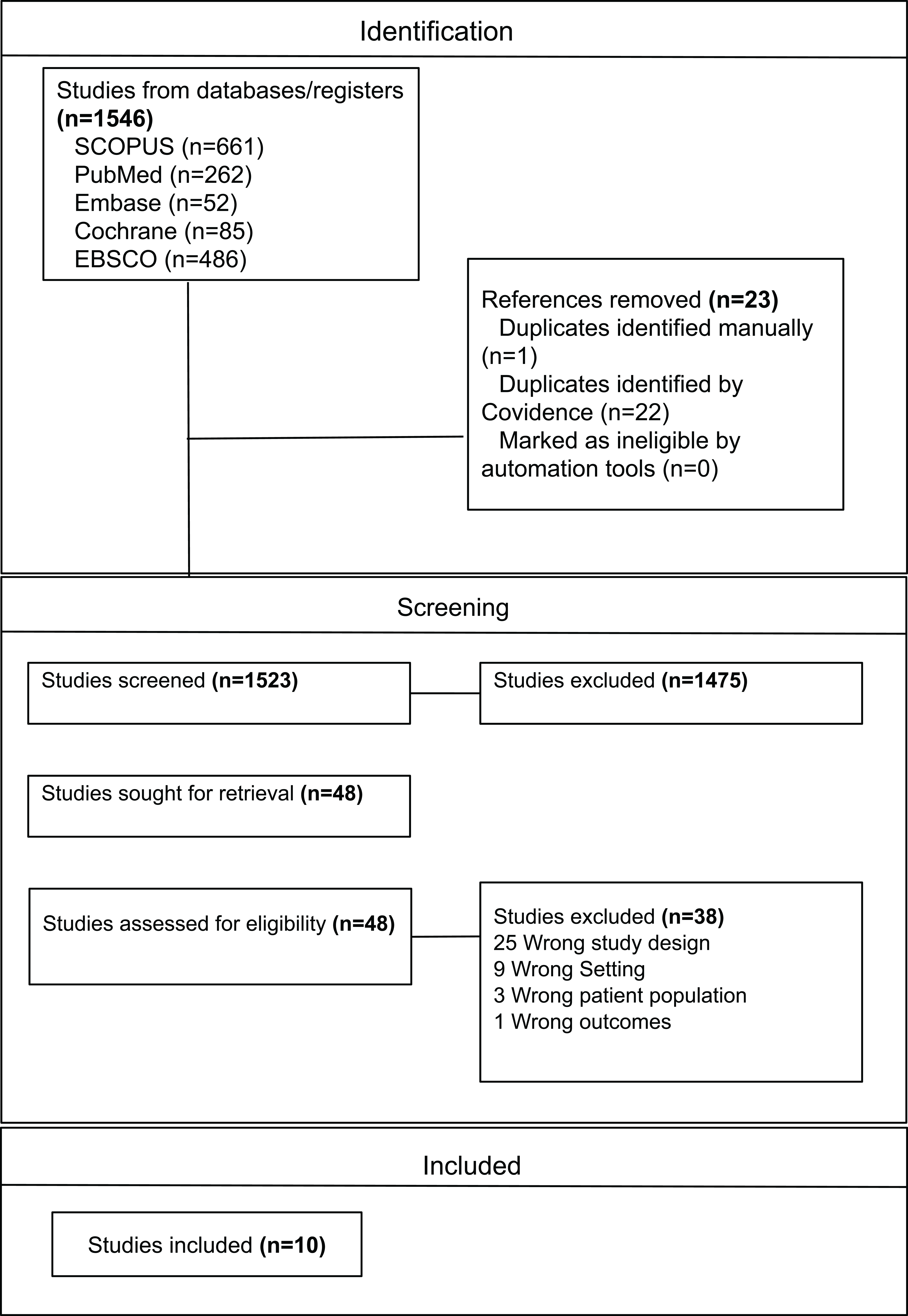
PRISMA flowchart showing the process of article selection for the systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
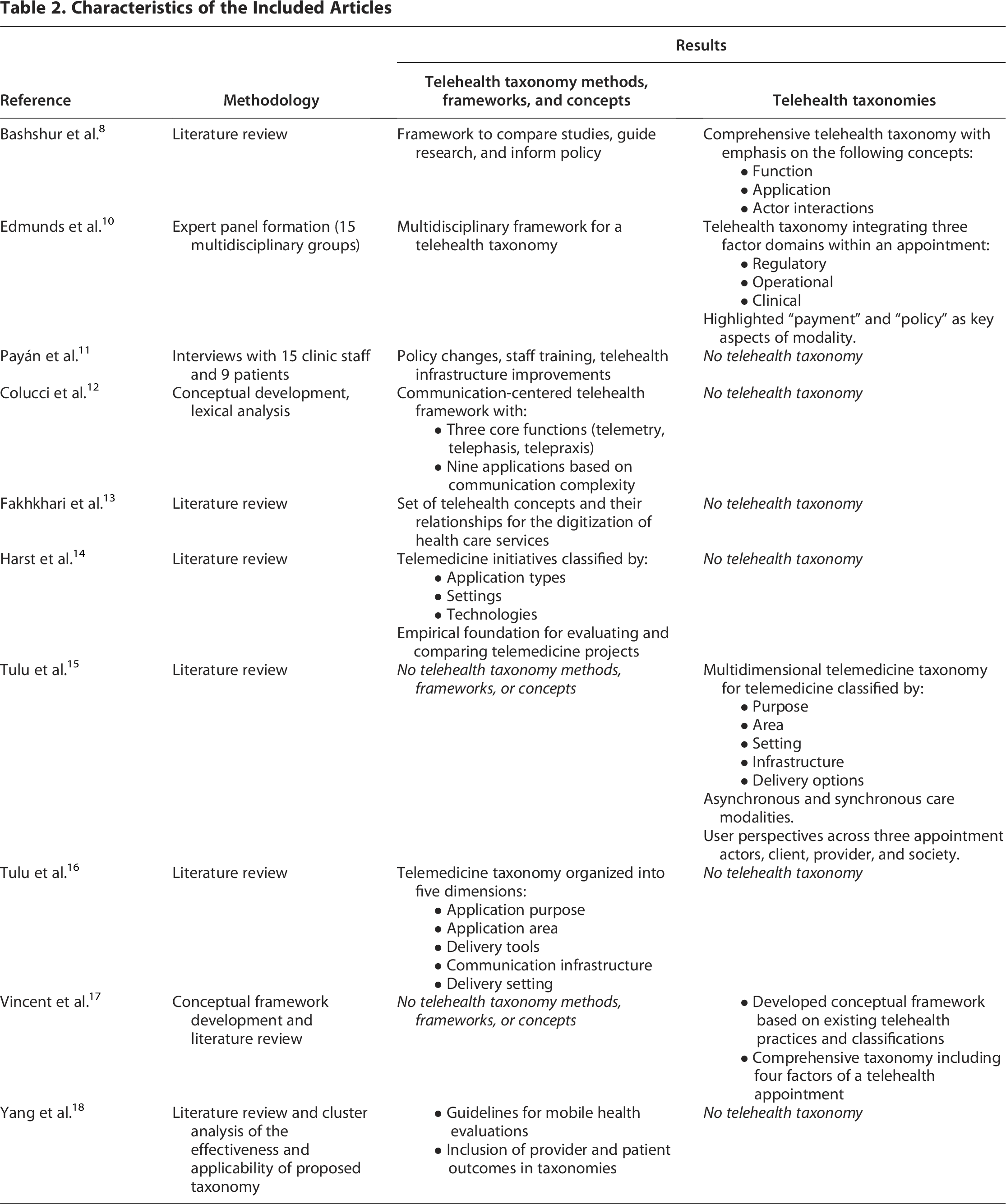
Table 2 shows the characteristics of the 10 included articles. Four of the articles provided taxonomies, while six articles provided concepts and frameworks, thus informing the development of the taxonomy.
Characteristics of the Included Articles
Key dimensions of the taxonomy
The final telehealth taxonomy consisted of 14 key parent variables and their respective subvariables (Figs. 2–4). Four key dimensions informed the organizational structure of the taxonomy: synchronous and asynchronous modalities, user perspectives, functionality, and payment considerations.
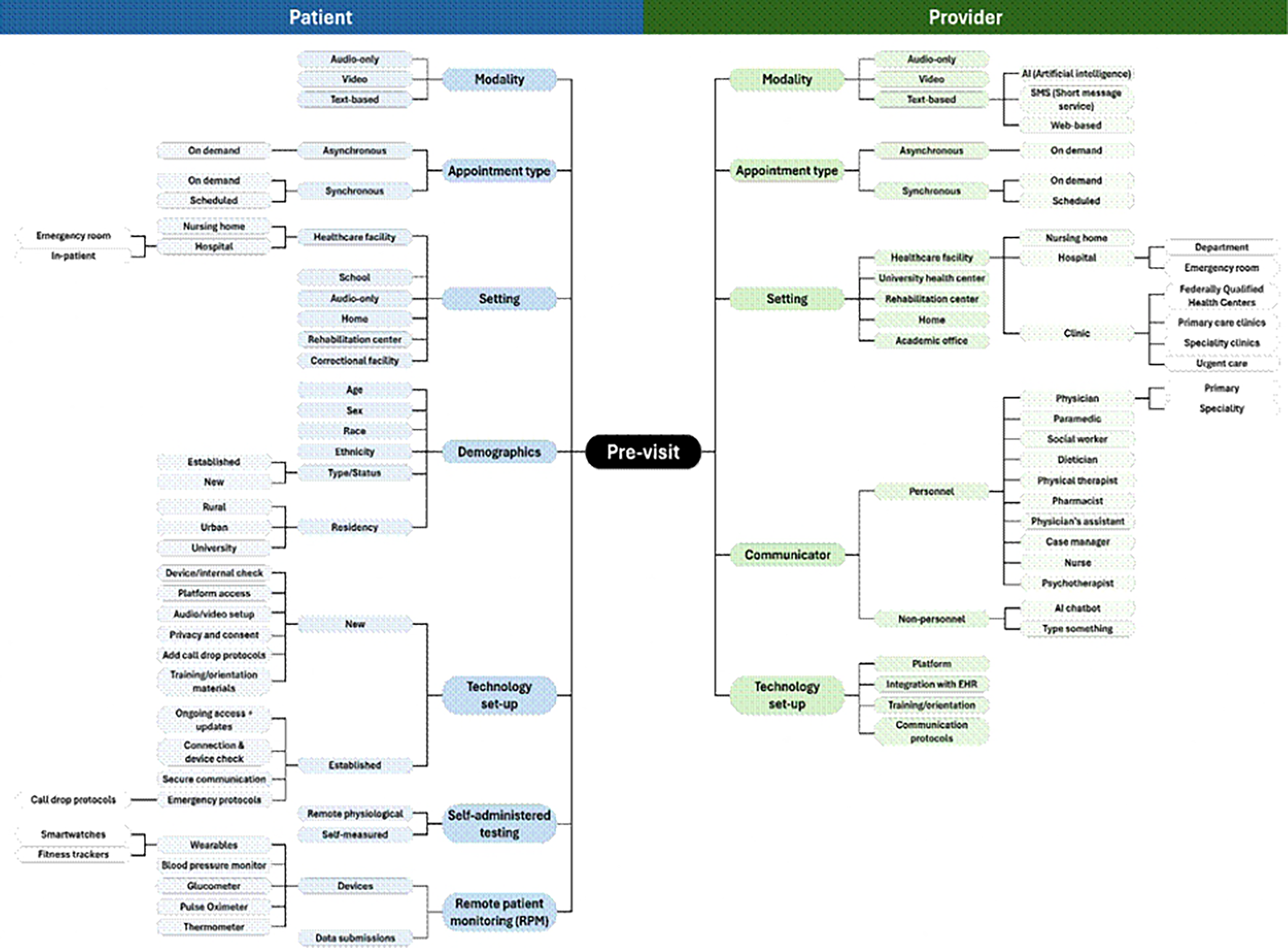
Previsit component of the taxonomy illustrating categories, subcategories of procedures and actions taken before a telehealth encounter, and the relationships between those concepts.
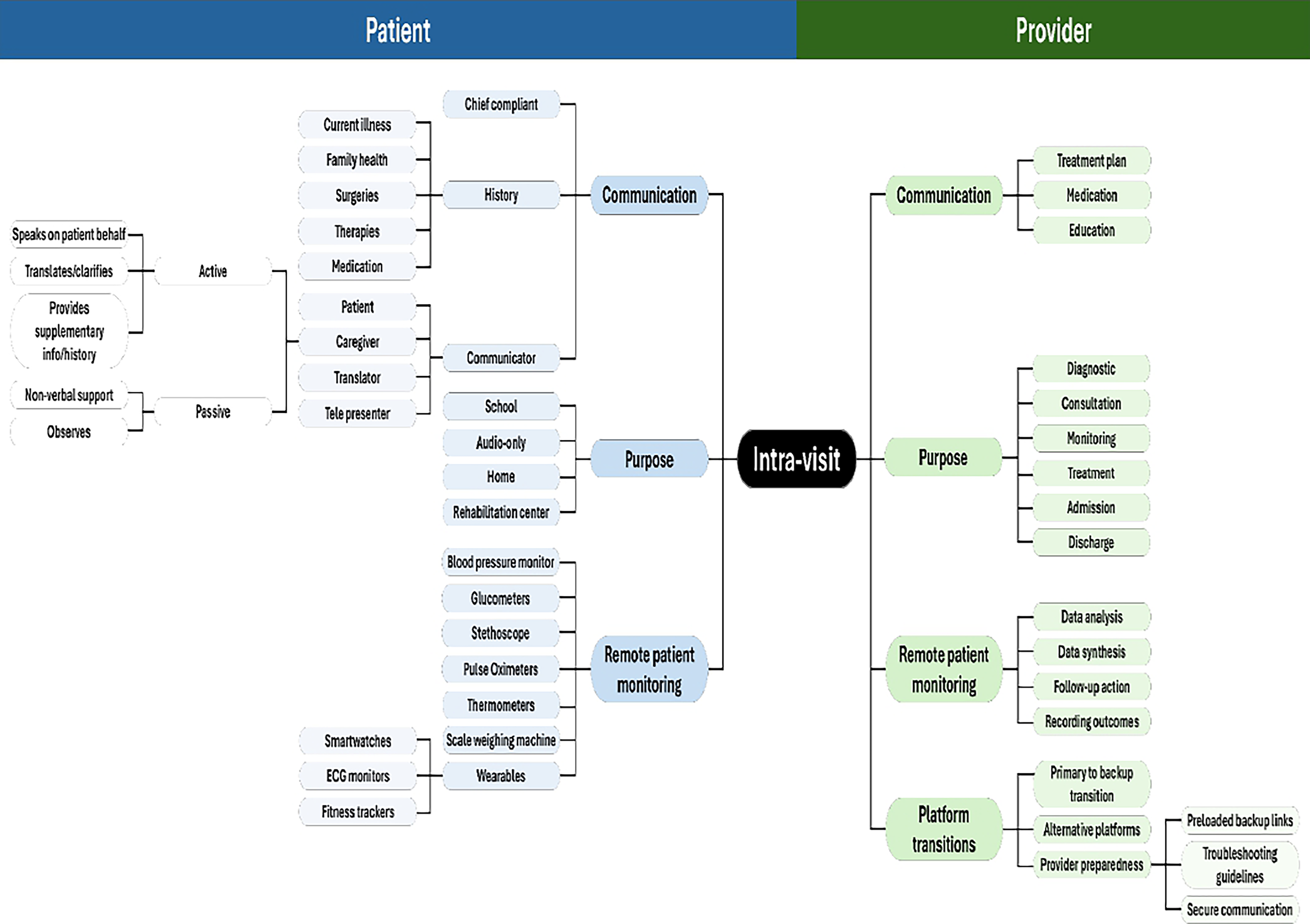
Intravisit component of the taxonomy illustrating concepts relating to patient and provider interactions and the relationships between those concepts.
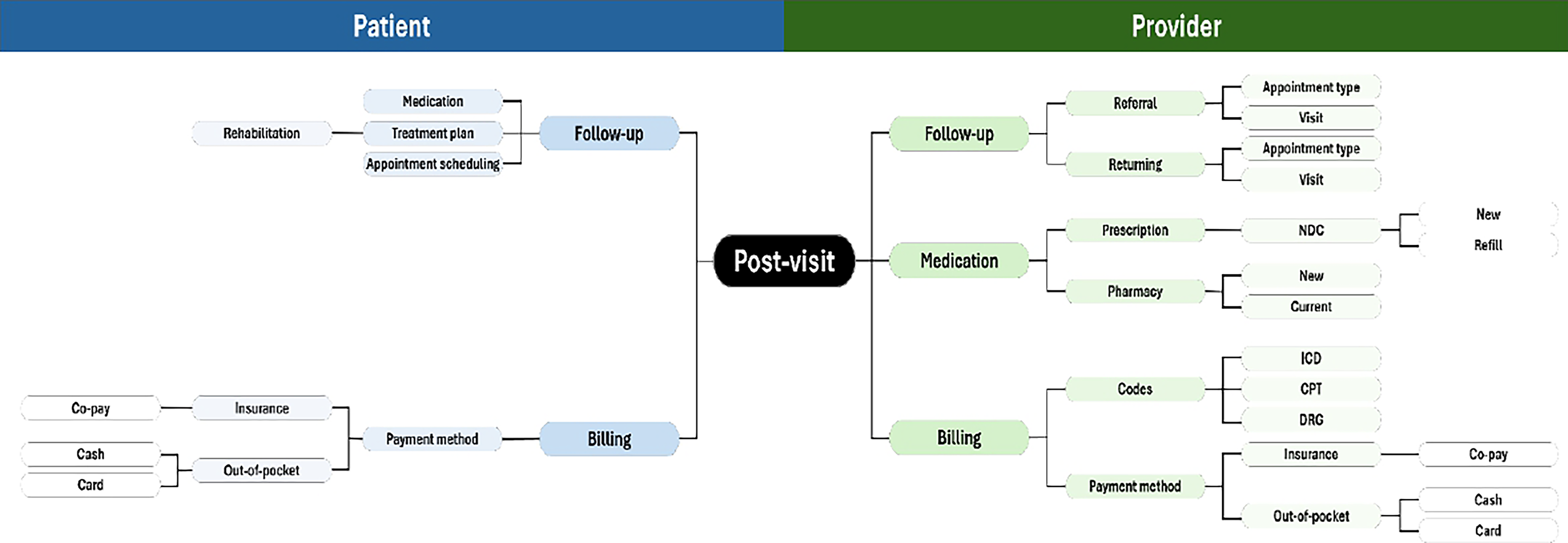
Postvisit component of the taxonomy illustrating concepts and their relationships of billing and payment options, detailing the postappointment phase of a telehealth encounter.
Synchronous and asynchronous modalities
The concepts of synchronous and asynchronous care modalities described by Tulu et al. 15 informed our temporal structuring of telehealth encounters. While synchronous and asynchronous exchanges represent foundational interaction patterns, contemporary telehealth models increasingly incorporate longitudinal modalities such as remote patient monitoring (RPM) and hybrid approaches that combine real-time and store-and-forward elements. To accommodate these evolving modalities, we organized parent variables across three temporal phases of the telehealth encounter—previsit, intravisit, and postvisit—thus enabling the taxonomy to capture both discrete encounters and continuous monitoring workflows.
User perspectives
Our delineation of primary and secondary actors within the telehealth encounter was also informed by Tulu et al. 15 The taxonomy incorporated client, provider, and societal perspectives regarding appointment-based care. This delineation was also informed by the comprehensive taxonomy developed by Vincent et al., 17 which distinguished encounters by interaction type, location of medical authority, urgency of care, and timing of communication. While patient and provider represent the primary clinical actors, our taxonomy also includes secondary and tertiary entities nested within these domains, such as caregivers and payers within the patient domain and organizational or administrative entities within the provider domain. This structure enables the framework to capture the broader socio-technical ecosystem involved in previsit authorization, documentation, and reimbursement processes.
Functionality
The “purpose” variable in our final taxonomy, which reflects the primary objective of each telehealth activity within the care process, was informed by Bashshur et al., 8 whose model emphasized “functionality” as a central organizing concept. It outlined diagnosis, consultation, monitoring, and mentoring as core telehealth functions and underscored the importance of distinguishing telehealth encounters by their intended clinical role.
Payment considerations
The fourth dimension identified in this taxonomy was payment. Edmunds et al. 10 emphasized payment as a key component of telehealth modality. In the present taxonomy, we incorporated this perspective by including “billing” in the postvisit phase, representing the administrative and reimbursement processes that influence telehealth delivery and completion.
Organizational structure of the taxonomy
The variables and subconcepts in this taxonomy were organized based on temporal phase, patient versus provider, and sequence.
Temporal phases
Dividing the taxonomy into three temporal phases provided a framework for identifying when and how particular variables were most relevant. The previsit phase captured preparatory elements occurring before a telehealth appointment begins; for example, appointment modality, provider specialty, and location were captured in the previsit phase (Fig. 2). The intravisit phase encompassed the core interactions and activities during the telehealth appointment, including purpose, communication, and RPM (Fig. 3). The postvisit phase involved follow-up steps and administrative tasks after the appointment concludes (Fig. 4), including billing and follow-up needs as important operational elements.
Patient and provider perspectives
Several variables were applicable to both the patient and provider perspective, and some were repeated from the previsit section due to their continuing relevance. For example, RPM was present in both the patient and provider sections, the latter of which referred to analyzing and interpreting patient-collected data during the encounter.
Sequential order
The variables in the taxonomy were listed according to the sequence when they occurred during each respective phase, reflecting distinct perspectives of the patient and provider. The subconcepts of the main concepts offered additional insight behind the rationale of the sequence. For example, in the intravisit patient perspective, “communication” preceded “purpose” because only after key information such as “chief complaint” and “medical history” is shared can the purpose of the appointment be established; thus, the next intravisit concept for the patient is “purpose,” with subvariables “follow-up,” “monitoring,” “treatment,” and “evaluation.” The provider side of the intravisit taxonomy also includes “communication,” which is sequenced after “purpose,” in contrast to the patient perspective. The provider must first determine the purpose of the appointment (diagnostic, consultation, monitoring, treatment, admission, or discharge) before communicating the relevant information (treatment plan, medication, and education) to the patient. Hence, “communication” follows “purpose” for the provider. In addition, while “patient” and “provider” were not treated as discrete data points, the taxonomy was structured around their respective roles, with variables explicitly divided across both perspectives. This bilateral approach acknowledges the relational dynamics of telehealth encounters and enables more nuanced data modeling.
Discussion
The scoping review in the first step of the project synthesized evidence from existing frameworks in 10 published articles, focusing on the concepts, variables, and gaps in how telehealth encounters are currently being defined, documented, and analyzed. Four articles included taxonomies, while six articles included theoretical concepts and frameworks. The articles highlighted the need to differentiate telehealth services by visit type (e.g., synchronous vs. asynchronous), clinical intent, and technology modality. The results of the review were organized into a hybrid hierarchical mind map, thus informing the iterative development of a comprehensive, structured taxonomy that captures the essential components of a telehealth appointment, reflects the evolution of digital care delivery, and supports the creation of an EHR-integrated data repository.
The taxonomy developed herein includes 14 parent-level variables that cover a telehealth encounter from both patient and provider perspectives, organized across three temporal phases: previsit, during visit, and postvisit. The key dimensions of the taxonomy include modality (synchronous/asynchronous), appointment purpose, setting, billing, and documentation method. Together, these elements provide a foundation for standardized and interoperable telehealth data capture (Fig. 5).
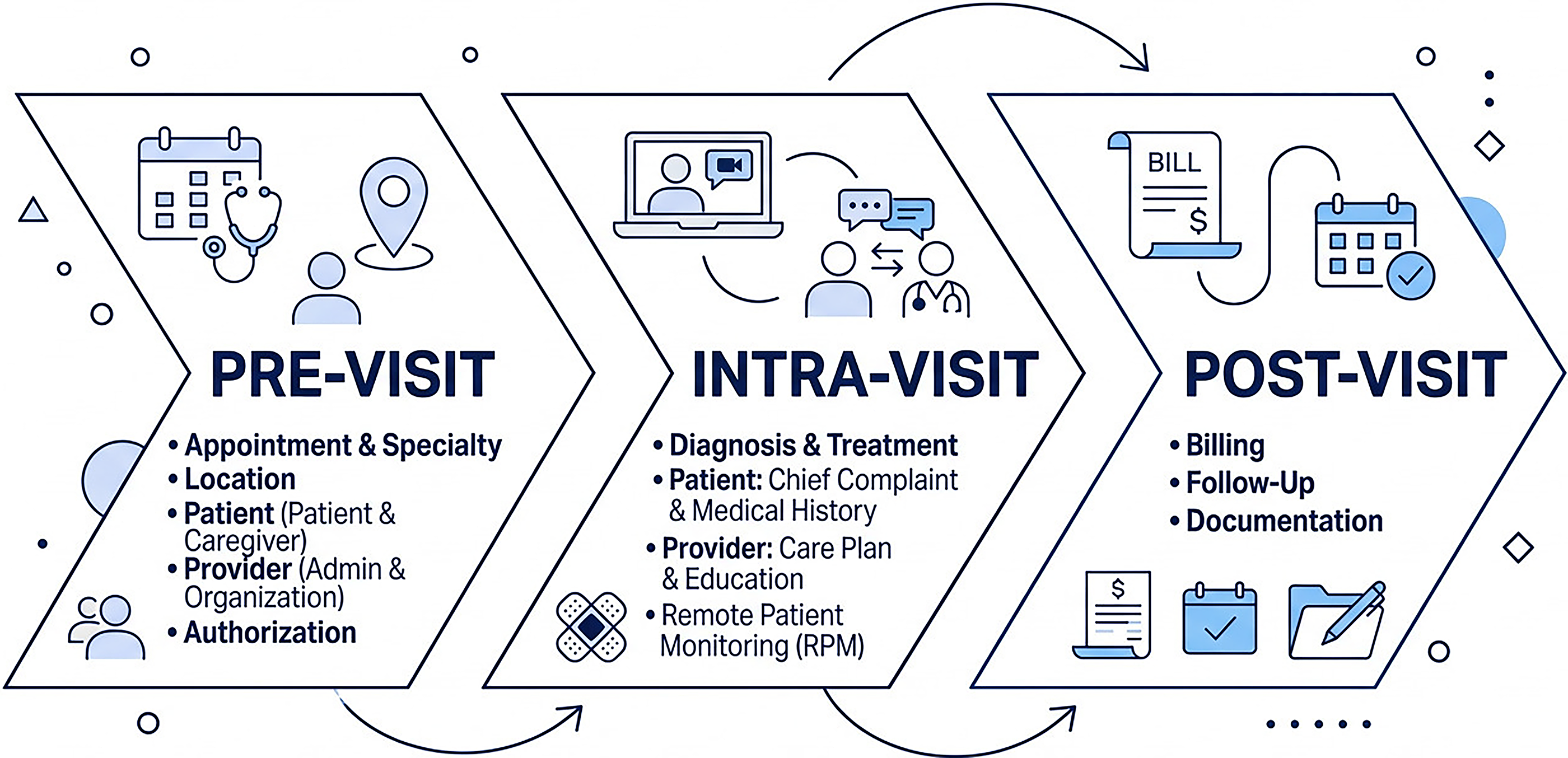
Diagram of telehealth taxonomy illustrating the high-level concepts within the three phases of the telehealth encounter.
The taxonomy advances the efforts to create a standardized telehealth data infrastructure by translating conceptual dimensions into an actionable and interoperable structure that directly maps to EHR data fields. 19 The final taxonomy is optimized for real-world implementation and future research. Its structured design supports standardized documentation, cross-platform interoperability, and integration into health data systems, enabling more consistent capture and analysis of telehealth encounters. In this way, the taxonomy consolidates and transforms existing knowledge into a practical foundation for digital health infrastructure, supporting evidence-driven care, policy, and research.
Integrating standardized telehealth terminology into health information systems carries broader implications for health systems strengthening, particularly in low- and middle-income countries. Standardized frameworks can support improvements in data consistency, documentation quality, and interoperability across diverse resource settings, including both paper-based and digitally enabled environments. 20 Reliable and structured data are essential for evaluating the feasibility, adoption, and sustainability of telemedicine interventions, thereby supporting evidence-based decision-making and equitable resource allocation. 21 Countries can adapt such a taxonomy to reflect local care models, aligning telehealth data with national priorities and facilitating cross-country comparisons. Globally, standardized telehealth data enable identification of service delivery gaps, enhancement of provider efficiency through clearer workflows, and generation of insights to inform policy and scale effective interventions. 22 Collectively, the outcomes underscore the potential of a structured telehealth taxonomy to strengthen health systems, advance equity, and improve both patient access and provider performance across diverse contexts.
Our study has several limitations. The literature search was not restricted by publication year, which resulted in the inclusion of older studies with potentially outdated outcomes; however, this decision ensured the inclusion of all relevant frameworks in the emerging field of telehealth. In addition, the exclusion of non-English and non-US-based studies may have limited generalizability to other country settings. The taxonomy has not yet been validated in clinical settings or integrated into live EHR systems, and its real-world usability remains to be established. Future research should validate the taxonomy across specialties (e.g., rehabilitation professionals) and care settings through expert review, inter-rater reliability testing, and application to real-world telehealth cases to assess construct clarity and consistency. Additional validation approaches include usability testing and pilot implementation within health information systems to examine workflow integration, interoperability, and practical impact. Furthermore, while the taxonomy was designed for synchronous encounters, it may require adaptation for asynchronous monitoring or RPM contexts. This taxonomy was developed based on telehealth literature and implementation models primarily situated within traditional health care systems. Accordingly, it assumes the presence of organizational infrastructure, established billing workflows, and payer relationships. While certain components may be adaptable to fully online or direct-to-consumer telehealth services, the framework is optimized for system-integrated telehealth delivery models. Finally, some variables, such as documentation method or follow-up planning, currently exist in unstructured EHR fields and would require the development of new templates or metadata strategies to support standardized capture.
The availability of high-quality, structured health data has far-reaching implications for health systems strengthening. Reliable data enable evidence-based decision-making, efficient resource allocation, and accountability across health services. When integrated within a structured taxonomy, telehealth data can illuminate what works—and what does not—for both patients and providers, guiding improvements in care delivery and access. By standardizing how telehealth encounters are defined and recorded, the final taxonomy provides the foundation for more equitable, efficient, and responsive digital health systems worldwide. 23
Conclusion
By offering a unified framework for consistent telehealth data capture, the taxonomy developed herein fills a crucial gap in current research infrastructure—an issue that was highlighted during the COVID-19 pandemic and remains unresolved despite widespread adoption of telehealth. Previous taxonomies offered useful conceptual elements; however, none provided a scalable, interoperable foundation with clear temporal structure and domain-level distinctions. 7 The hybrid hierarchical and mind-map design overcomes the limitations, balancing clarity with technical feasibility. Ultimately, this taxonomy lays the groundwork for a standardized telehealth data infrastructure capable of supporting robust evidence generation, improved patient care, and informed health policy in the era of digital health.
Footnotes
Acknowledgments
The authors thank Dr. Spencer Dorn, Dr. Carl Seashore, Dr. Jennifer Elston Lafata, Dr. Chris Shea, and Dr. Olga Khavjou for providing domain expertise during the taxonomy development. The authors also thank Dr. Keenan Jenkins, Natasha Mack, and Christine Weirich Paine for their contributions to the article review and their critical revisions.
Authors’ Contributions
K.S.Y. conducted the literature review, developed the taxonomy, performed analysis, and drafted and revised the article. E.M. and Suguna K. assisted with developing and executing the systematic search strategy. Z.Z. created the final taxonomy images and provided visualization and graphic design help throughout. J.C. and D.M. provided critical feedback as domain experts during the taxonomy development process. Saif K. conceptualized the study, formulated the research question, provided supervision throughout the research process, and contributed to article revisions. All authors approved the final article.
Ethics Approval and Consent to Participate
Not applicable. This study did not involve human participants.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (
Abbreviations Used
Appendix A
Search strategy:
(“Telemedicine/classification”[MeSH] OR ((“Terminology As Topic”[MAJR] OR taxonomy*[ti] OR terminology*[ti] OR “classification system*”[ti] OR nomenclature[ti] OR ontology*[ti] OR “information architecture*”[ti] OR catalog*[ti] OR category[ti] OR categories[ti] OR domain[ti] OR categorization*[ti] OR criteri*[ti]) AND (“Telemedicine”[MAJR] OR “Remote Consultation”[MAJR] OR telehealth[ti] OR telemedicine[ti] OR teleconsult*[ti] OR telenursing[ti] OR telemonitor*[ti] OR “remote visit*”[ti] OR “remote consult*”[ti] OR “remote appointment*”[ti] OR “virtual visit*”[ti] OR “virtual consult*”[ti] OR “virtual care”[ti] OR “virtual appointment*”[ti] OR “electronic visit*”[ti] OR “electronic appointment*”[ti] OR “electronic consult*”[ti] OR eConsult*[ti] OR eHealth[ti] OR “digital health”[ti]))) AND (english[Filter]).