
Abstract
Background:
Early initiation of intravenous thrombolytics for treatment of acute stroke leads to improved functional outcomes. Published guidelines aim to reduce door-to-needle (DTN) times in both prehospital and hospital settings without specific consideration of telestroke. Over the last decade, telestroke has become increasingly more common to provide emergency stroke care worldwide but published guidelines on specific practices have yet to be established. The implementation of EMS prearrival notifications, neurologic evaluation and thrombolytic administration in the CT imaging suite (CIS) are utilized as best practices by some programs.
Methods:
We utilized the Telecare by TeleSpecialistsTM database to investigate the impact of these practices on DTN times and thrombolytic treatment rates. Hospitals participating in all recommended Best Practices were considered the investigative group and those hospitals participating in all Best Practices except the variable of interest were considered the control group. Shapiro–Wilk, Mann–Whitney U, and Pearson’s chi-squared tests were used when appropriate.
Results:
Pre-notification was associated with an 8-min reduction in DTN times (p = 0.0026) and 3.7% increase in thrombolytic treatment rates (p = 0.0016). Evaluation by the neurologist in the CIS was associated with a reduction in DTN times (6-min reduction, p = 0.0192) and increase in thrombolytic administration rates (1.46% increase, p = 0.0361). Implementing administration of IV thrombolytic in the CIS was associated with similar benefits (3-min reduced DTN times, p = 0.0176; 2.87% increase in thrombolytic treatment rate, p < 0.0001).
Conclusion:
Overall, these best practices reduced DTN times and improved treatment rates supporting their integration into telestroke practices globally.
Introduction
Early initiation of intravenous thrombolytics (IVT) in cases of acute ischemic stroke (AIS) leads to improved functional outcomes, decreased IVT-related complications, and lower stroke mortality rates.1–4 Guidelines published by the American Heart Association/American Stroke Association (AHA/ASA) aim to minimize door-to-needle (DTN) times in both pre-hospital and emergency department (ED) settings, aligning with the “Get With The Guidelines—Stroke (GWTG—Stroke)” recommendations.4–6 However, these protocols are primarily tailored to institution protocols for in-person acute stroke assessment. As of 2019, ∼45% of EDs relied on telestroke services for AIS evaluation, which covers almost 90% of the U.S. population. 7 Similar findings within Europe, especially in rural areas, have shown a steady increase in the number of telestroke networks. 8 Telestroke has been proven to deliver high-quality and safe AIS care regardless of the geographic location or local infrastructure.9–11 Despite an increasing trend in IVT administration for AIS, 12 several factors still contribute to delays or failures in receiving IVT within the treatment window including delayed or absence of emergency medical services (EMS) pre-notification and prolonged door-to-CT times.13,14 Research suggests that for every ten-minute delay within the 1–3 h treatment period one fewer patient has improved disability outcome. 15 To address these challenges, early guidelines such as “Target: Stroke Key Best Practice Strategies” in 2011 recommended pre-notification by EMS and maintaining availability of IVT either in the ED or in the CT imaging suite (CIS) for prompt administration. 16 Presently, there are no established recommendations for best practices in telestroke workflow. This study aims to investigate whether compliance with the best practices: EMS pre-notification, continued neurologic assessment by the neurologist in the CIS, and IVT administration in the CIS are associated with reduced DTN times and increased IVT treatment rates.
Methods
Patient database
The Telecare by TeleSpecialistsTM database is continuously updated with data prospectively collected from encounters with TeleSpecialists, LLC neurologists in the ED as acute stroke encounters. An Institutional Review Board exemption was granted by WCGTM IRB. This comprehensive database records demographics and clinical data including clinical assessments, time-related metrics, imaging findings, and treatment decisions. TeleSpecialists, LLC, as the telestroke provider, has 15 best practices that are strongly recommended for all facilities. This database tracks which facilities have elected to participate in each of the 15 best practices.
Study design
Two separate retrospectively reviewed cohorts were identified to investigate the impact of three distinct best practices from the 15 best practices recommended by the quality program of the telestroke physicians (Fig. 1). The control group consists of facilities that participate in all best practices. The experimental groups were identified based on the participation of facilities in all best practices except the best practice being evaluated. Study “A” investigated the impact of EMS pre-notification while maintaining compliance with the other 14 Best Practices. Whereas Study “B” investigated the impact of continued neurologic evaluation and thrombolytic administration in the CIS (two separately defined Best Practices) while maintaining compliance with the other 13 best practices.
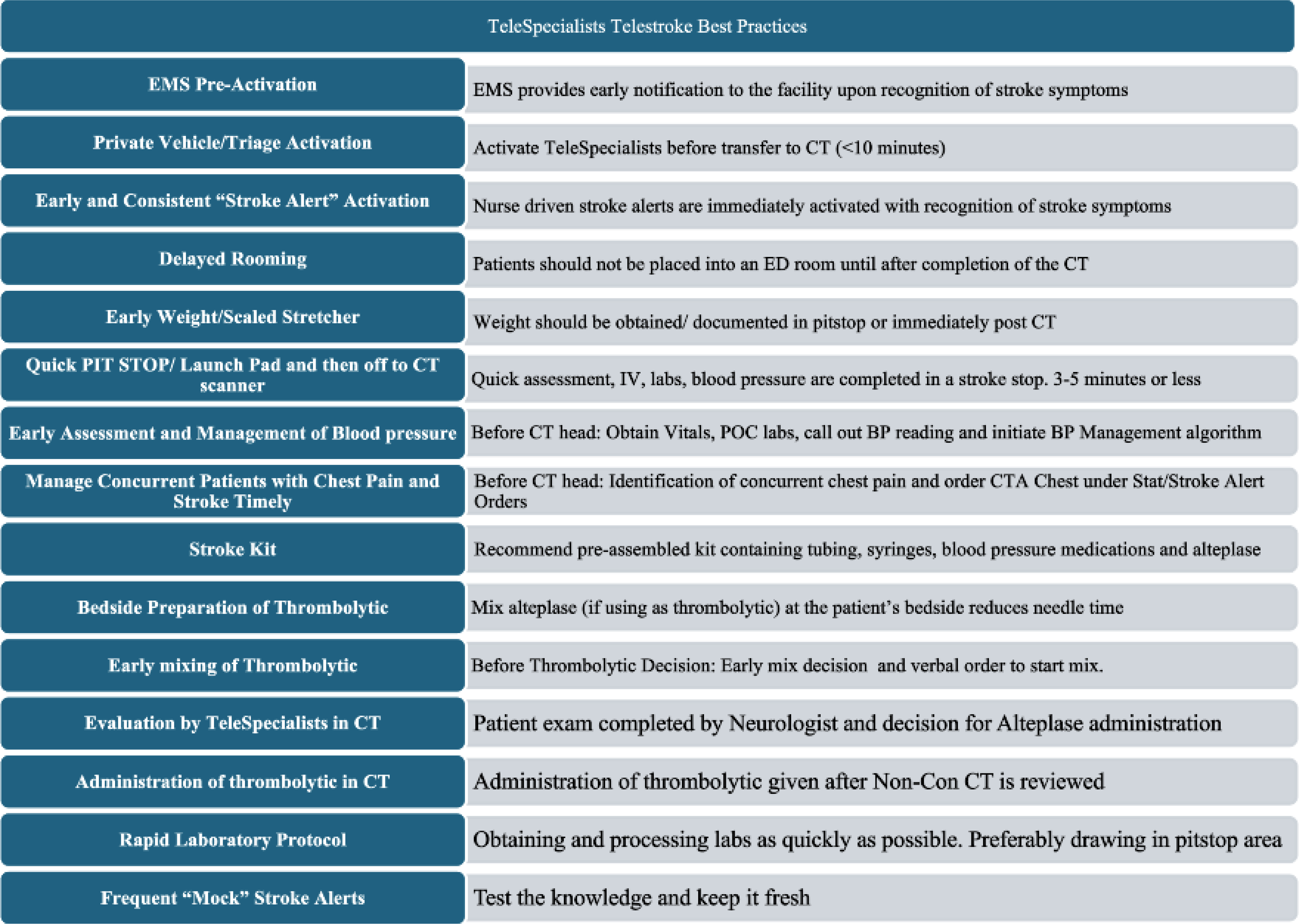
TeleSpecialists 15 best practices in telestroke.
Study populations
Study “A” included all acute stroke evaluations by teleneurologists affiliated with TeleSpecialists, LLC between July 1, 2021, and December 31, 2021. Inclusion criteria were patients 18 years or older who met the criteria for IVT (per AHA/ASA guidelines) and were treated with IVT. We excluded patients evaluated at hospital systems that did not adhere to the other 14 best practices.
Study “B” included all acute stroke evaluations conducted by teleneurologists affiliated with TeleSpecialists, LLC between July 1, 2021, and December 31, 2021. Inclusion criteria were patients 18 years or older with a last-known-normal time within 24 h. We excluded patients evaluated at hospital systems that did not adhere to the other 13 best practices. The cohort was then divided into two groups: those transferred to CIS with the neurology telecart and those who were not accompanied by the telecart (teleneurologist). Within the cart-to-CIS cohort, there was further subdivision based on whether Tissue plasminogen activator administration occurred in the CIS or upon return to the patient’s room in the ED.
Baseline characteristics and outcomes
Baseline characteristics included age, gender, National Institutes of Health Stroke Scale (NIHSS), and arrival-to-notification time (ATN). ATN is defined as the difference in minutes between patient arrival to the ED and the time of teleneurologist notification. The primary outcome measure was median DTN time. DTN time was calculated utilizing the documented arrival time and the IVT bolus time in minutes. The secondary outcome measure was thrombolytic treatment rates.
Statistical analysis
In this study, descriptive statistics were used to summarize patient characteristics and treatment outcomes. Continuous variables such as DTN times were expressed as medians with interquartile ranges (IQR) due to the non-normal distribution of the data as confirmed by Shapiro–Wilk test at a significance level of 0.05, while categorical variables were presented as counts and percentages. The Mann–Whitney U test, a nonparametric statistical method, was employed to compare differences in medians of time intervals between facilities with and without EMS pre-notification process, as well as between groups treated with and without a cart to Computed Tomography (CT) and thrombolytic treatment in CT. Pearson’s chi-squared test was utilized to assess the significance of differences in categorical outcomes, such as the proportion of patients achieving DTN times < 60 min and IVT treatment rates, across different facility types. Results with a p-value < 0.05 were considered statistically significant, and specific comparisons where significance was achieved are reported in the results. All data analysis was conducted using R version 4.3.1.
Results
Study A
A total of 9,290 patients were screened for inclusion of the study, with 8,529 excluded due to not receiving IVT. This includes patients from a total of 79 hospitals across 14 different states. 761 patients underwent treatment with IVT per protocol of which 730 were treated at facilities with an established pre-notification system and 31 patients were treated at a facility with no pre-notification system. Of the 730 patients treated at a facility with an established EMS prenotification system, EMS pre-notification occurred in 394 (54.0%) cases.
Among those treated at facilities with an established pre-notification system, median DTN times were shorter (35.0 min [26.0, 46.0] vs. 43.0 [32.5, 65.0] min; p = 0.013) and there were higher IVT treatment rates (8.5% vs. 4.8%, p = 0.0016). Those facilities with a prenotification process carried a higher rate of DTN times in < 60 min (88% vs. 67.7%, p = 0.0026). There was a trend toward higher rates of DTN in < 30 min (36% vs. 22.6%) but did not meet statistical significance (p = 0.1799). The NIHSS score was higher, among those treated at a facility with an established pre-notification system (8 [4.0, 14.0]) than those treated at other facilities (4 [3.0, 7.0]; p = 0.0023), but there was no difference between age, gender, or arrival to notification time (Table 1).
Study Population A: Pre-Notification Policy
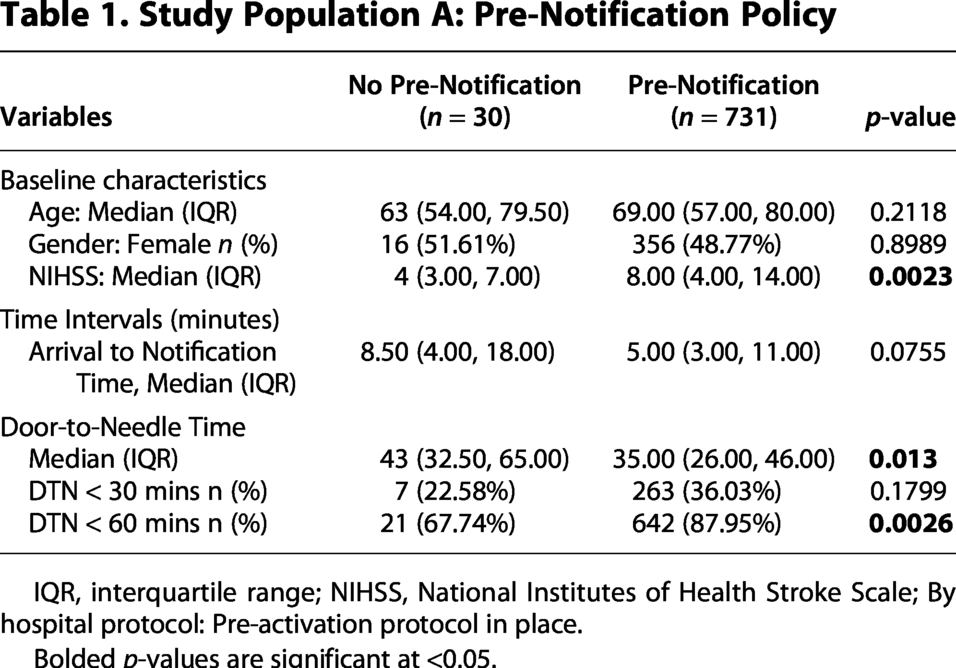
IQR, interquartile range; NIHSS, National Institutes of Health Stroke Scale; By hospital protocol: Pre-activation protocol in place.
Bolded p-values are significant at <0.05.
Acute stroke activations that were initiated by EMS pre-notification experienced shorter median DTN times (29 [23.0, 39.0] min vs. 41.0 [32.8, 54.0] min, p < 0.0001). (Table 2). These cases where pre-notification was initiated experienced higher rates of DTN times < 60 min (93.4% vs. 81.5%, p < 0.0001) and DTN times < 30 min (50.3% vs. 19.35%, p < 0.0001).
Study Population A: Pre-Notification Occurred at Facilities with Policy
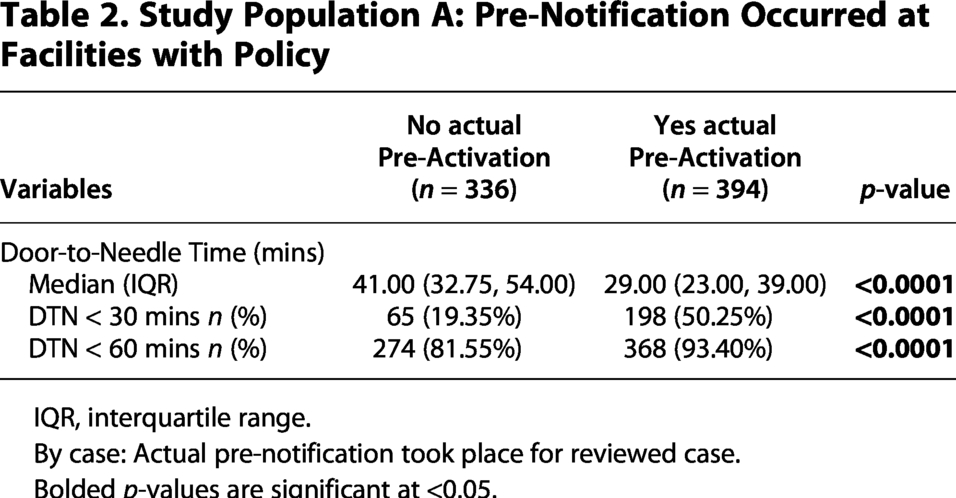
IQR, interquartile range.
By case: Actual pre-notification took place for reviewed case.
Bolded p-values are significant at <0.05.
Study B
A total of 15,118 patients were assessed with 90% (13,626) accompanied by a teleneurologist to the CIS and 10% (1,492) not accompanied by a teleneurologist to the CIS. Across all patients included in the study, 68 hospitals across 14 different states were included in the cart to CIS and 11 hospitals in the no cart to CIS cohorts (Table 3).
Study Population B: Tele-Cart to the CT Imaging Suite
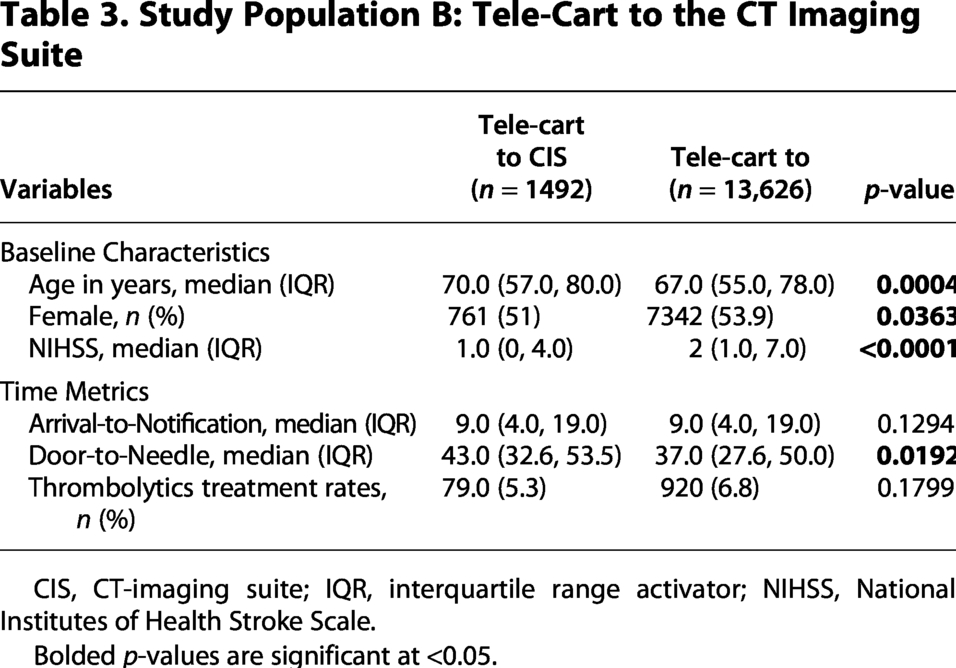
CIS, CT-imaging suite; IQR, interquartile range activator; NIHSS, National Institutes of Health Stroke Scale.
Bolded p-values are significant at <0.05.
Evaluation by a teleneurologist in the CIS resulted in a 6-min reduction in DTN time (37.00 [27.59, 50.00]) over patients that were not accompanied to the CIS (43.00 [32.59, 53.50], p = 0.0192). In addition to faster administration of IVT, evaluation of treatment eligibility in the CIS also resulted in a 1.46% increase in IVT treatment over those not evaluated in the CIS (6.75% vs. 5.29%, p = 0.0361). There was not a statistically or clinically significant difference between cohorts in the arrival-to-stroke alert notification time (both cohorts reported 9.00 [4.00, 19.00], p = 0.1294) and therefore did not require adjustment.
The patients treated in the CIS also experienced reduced DTN times [36.13 (27.00, 49.51)] over those treated at hospitals without a protocol for IVT treatment in the CIS [39.48 (29.58, 51.74), p = 0.0176]. Additionally, those eligible to receive IVT in the CIS were treated more frequently (7.77% vs. 4.83%, p < 0.0001) (Table 4).
Study Population B: Treatment in the CT-Imaging Suite
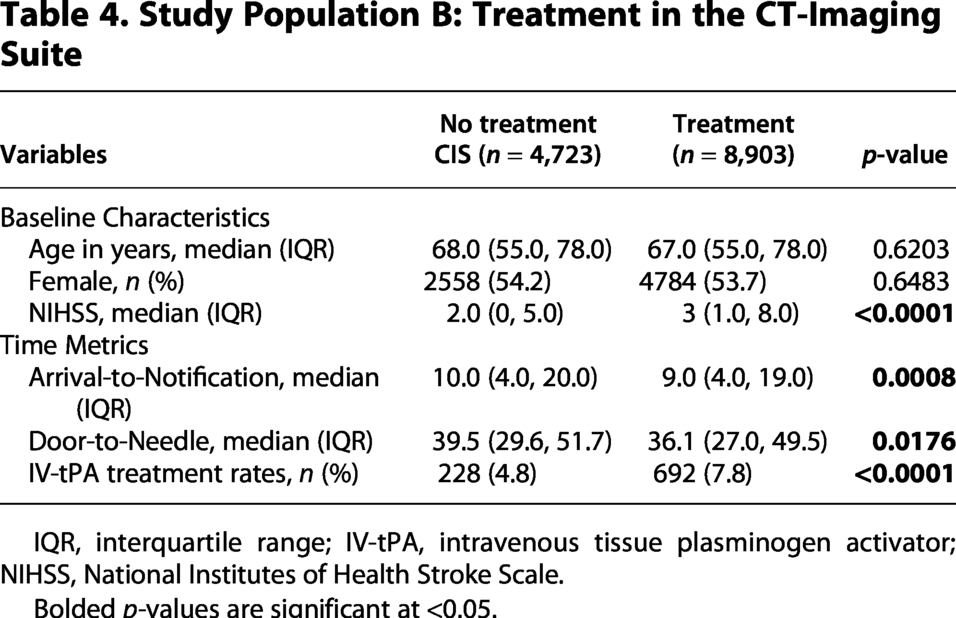
IQR, interquartile range; IV-tPA, intravenous tissue plasminogen activator; NIHSS, National Institutes of Health Stroke Scale.
Bolded p-values are significant at <0.05.
Discussion
Acute stroke care protocols are continuously being modified with the primary goal of reducing DTN times. A prior study investigated the impact of GWTG implementation on DTN times and revealed a 1.3-min decrease in DTN times for every guideline integrated into stroke evaluation protocols. 17 This underscores the ongoing interest among designated stroke centers in refining and implementing best practices for acute stroke evaluation and management. These guidelines and protocols have traditionally focused on in-person stroke evaluation and have not been validated for integration with telestroke programs. Therefore, the goal of this study was to characterize the impact of EMS pre-notification, continued neurologic evaluation in the CIS, and treatment in the CIS on acute Telestroke assessments across our nationwide, multi-hospital telestroke network. We found that integration of these best practices was associated with reduced DTN times and increased treatment rates. Our findings are consistent with other in-person stroke evaluation protocol studies that demonstrated reduced DTN times and increased treatment rates when pre-notification takes place and continued assessment and treatment occur in the CIS.18,19 While the conventional practice of gathering essential information to rule out IVT contraindications remains unchanged, we acknowledge the added benefit of obtaining this information concurrently to expedite time-sensitive care.
Among those who were brought to the ED by EMS with pre-notification, we observed a higher IVT treatment rate than those without pre-notification (8.5% vs. 4.8%, p = 0.0016). We hypothesize this difference in treatment rate may be due to multiple reasons including but not limited to severity of symptoms, availability of resources, and bias. We believe that patients who are brought in by EMS with pre-notification are more likely to have symptoms consistent with “classic stroke syndromes” that score higher on pre-hospital stroke triage scales. The hospitals with an established pre-notification system are more likely to be larger hospitals with more resources (Fig. 2). Lastly, acute stroke cases presenting with pre-notification carry the potential for confirmation bias, therefore, increasing the rate of acute stroke diagnoses and IVT treatment.
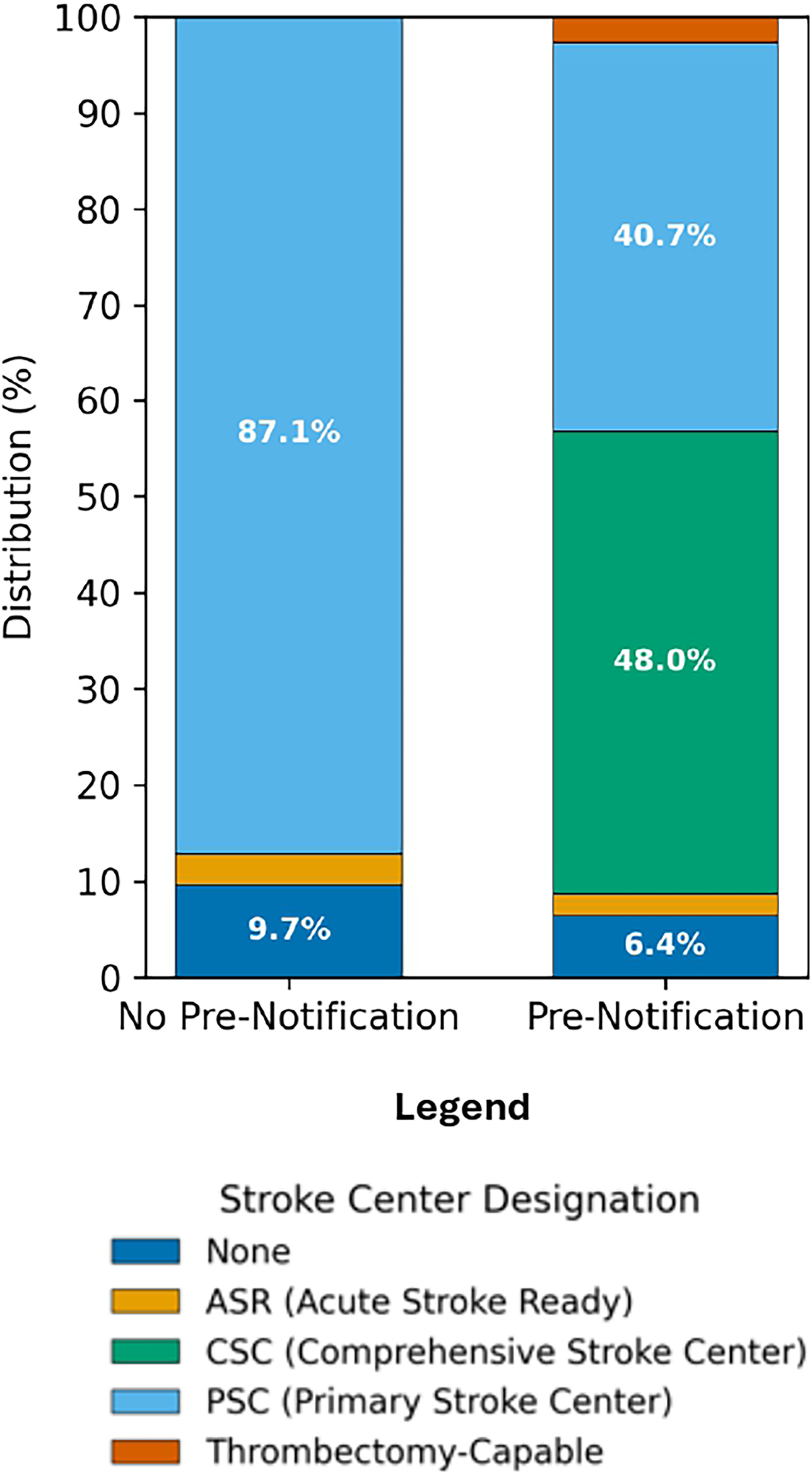
Distribution of hospital Joint Commission stroke center designations by EMS pre-notification policy.
Our study is limited by its retrospective design. Patient allocation to a specific cohort was determined by site-specific stroke protocols rather than randomization. Additionally, the study lacks comprehensive demographic data, imaging findings, and other documented delays in standard acute stroke evaluations, which may be considered as outliers in terms of decision and treatment delays. While we are able to report on the impact of our telestroke practices on standard acute stroke time metrics, standard long-term outcomes like 90-day functional outcomes (i.e., modified Rankin Scale) are unavailable.
To our knowledge, this study is the first to explore the impact of these best practices in a real-time, multihospital, geographically diverse, telestroke setting. Based on our findings, we advocate for incorporating EMS pre-notification of the teleneurologist, prompt teleneurologist evaluation and assessment in the CIS, and IVT administration in the CIS into telestroke networks worldwide. Our results demonstrate the feasibility across multiple hospital systems in geographically diverse locations and the efficacy of implementing these protocols to deliver optimal patient care in the telestroke setting.
Conclusion
EMS pre-notification, neurologic assessment in the CIS, and IVT treatment in the CIS are associated with a significant reduction in DTN times and increased treatment rates. These findings support integrating these best practices into telestroke care nationwide and standard recommendations globally.
Authors’ Contributions
All authors met authorship criteria and contributed substantially to conceptualization (T.S.), data curation (M.F., Y.V., and T.S.), analysis and interpretation of data (J.S., M.M., T.S., O.C., and L.G.), drafted (J.S.) or revised (all authors) and gave final approval of the version to be published (all authors).
Footnotes
Acknowledgments
All the physicians and quality team members who helped to gather and verify the data in the TeleCare by TeleSpecialistsTM database.
Data Availability Statement
The dataset is available on request. The raw data supporting the conclusions of this article will be made available by the authors, with undue reservation.
Author Disclosure Statement
T.S. has fractional shares in Moderna stock. All other authors have no disclosures. J.S., M.M., L.M., Y.V., M.F., and T.S. were employed by the company TeleSpecialists, LLC. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
There was no funding received for this project.