
Abstract
The hypoplastic mandible results in facial convergence and pseudo-prognathism. We present a patient with significant maxillary hypoplasia in both the vertical and sagittal dimensions resulting in a reverse occlusal plane. Given the significant maxillary movements required, particularly clockwise rotation, more traditional mandibular osteotomies resulted in an unsatisfactory result. A modified version to the classic “C” osteotomy with the use of surgical planning and cutting guides was performed. A review of the literature on this rarely discussed ramus osteotomy is also presented.
Introduction
Maxillary hypoplasia with relative mandibular excess is one of the classic abnormal facial growth patterns of the maxillofacial complex. Terminology such as deep bite, convergent facial profile, or pseudo-prognathism have been used to describe this classic facial pattern.1-3 The convergent, concave facial profile of this Angle’s class III deformity contributes to a sunken-appearing midface and a perceived prominent chin. This characteristic subtype of the “Habsburg Jaw” can lead to many functional impairments including speech disarticulations, dysphagia, chronic nasal airway obstruction, and temporomandibular disorders.3-5
One common treatment option has been maxillary advancement with a clockwise rotation. Reorienting the pitch of the maxilla in such fashion has a profound effect on the midface. 6 Mandibular osteotomies are often necessitated to facilitate optimal occlusion and enhance the overall aesthetics. While sagittal split osteotomies have become the preferred technique, we present a case report in which C-osteotomies to the rami of the mandible was the preferred method. Literature on this modified vertical ramus osteotomy was also reviewed.
Case Report
A 17 year old female presented with skeletal and dental class III malocclusions with 7 mm of reverse overjet with a concave facial profile (Figures 1 and 2). Maxillary hypoplasia with transverse deficiency existed with paranasal deficiency and limited midface projection. Vertical maxillary deficiency resulted in absent incisor exposure with full animation as the smile buried behind the drape of the upper lip. Functional challenges included complaints of difficulty with mastication, leading to episodic dysphagia. Patients also exhibited speech impediment particularly with “s” and “sh” sounds secondary to incisor malpositioning. Decision was made to proceed with bimaxillary surgery with the aid of virtual surgical planning and patient specific cutting guides. This included a 3-piece segmental Lefort I advancement of 4 mm, disimpaction of 6.5 mm with clockwise rotation with a mandibular C-osteotomy to adjust the occlusal plane from negative to positive.

Preoperative clinical photo displaying maxillary hypoplasia.

Preoperative radiograph showing convergent.
Surgical Procedure
The patient was induced with general anesthesia and underwent nasotracheal intubation. Following standard prepping and draping, the preoperative measurement from nasion to the surgical arch wire between brackets #8 and #9 was found to be 36 mm (as opposed to the average ranging from 60 to 80 mm), indicating how profoundly maxillary deficient the patient was. As mandible first surgery has become the standard for the practice in that it eliminates the potential uncertainty of centric relation, the focus was turned toward the mandible. A standard BSSO incision was made and dissection carried along the lateral and medial aspects of the mandibular ramus. Partially impacted teeth #17 and 32 were sectioned and removed. Next, a combination of Bauer and toe up retractors were used to expose the surgical site. The cutting guide was then applied to the lateral aspect of the ramus, engaging the posterior border as well as the sigmoid notch to ensure proper seating. A coronoidectomy was then completed bilaterally to avoid any interference along the zygomatic arch as the distal segment (which otherwise includes the coronoid process for this specific osteotomy) would be rotated superiorly in a clockwise direction. An oscillating saw was used along the cutting guide to create 5, separate, small osteotomies in order to recreate the curvilinear “C” shape (Figure 3). Upon completion of the osteotomies bilaterally, the distal mandible was found to be freely moveable. A prefabricated intermediate splint was then applied along with maxillomandibular fixation, essentially ratcheting the complex in a clockwise direction. All interferences noted on the pre-operative plan were then relieved and the proximal and distal segments were found to lay passively in great approximation with each other. These were then fixated using 2 “L” shaped plates facing one another. A trocar system was used to apply the screws to the plates. The plates were placed through the intraoral incision and held in place with a combination of the assistant surgeon using a Woodson elevator and the primary surgeon using a drill guide through the transbuccal trocar.
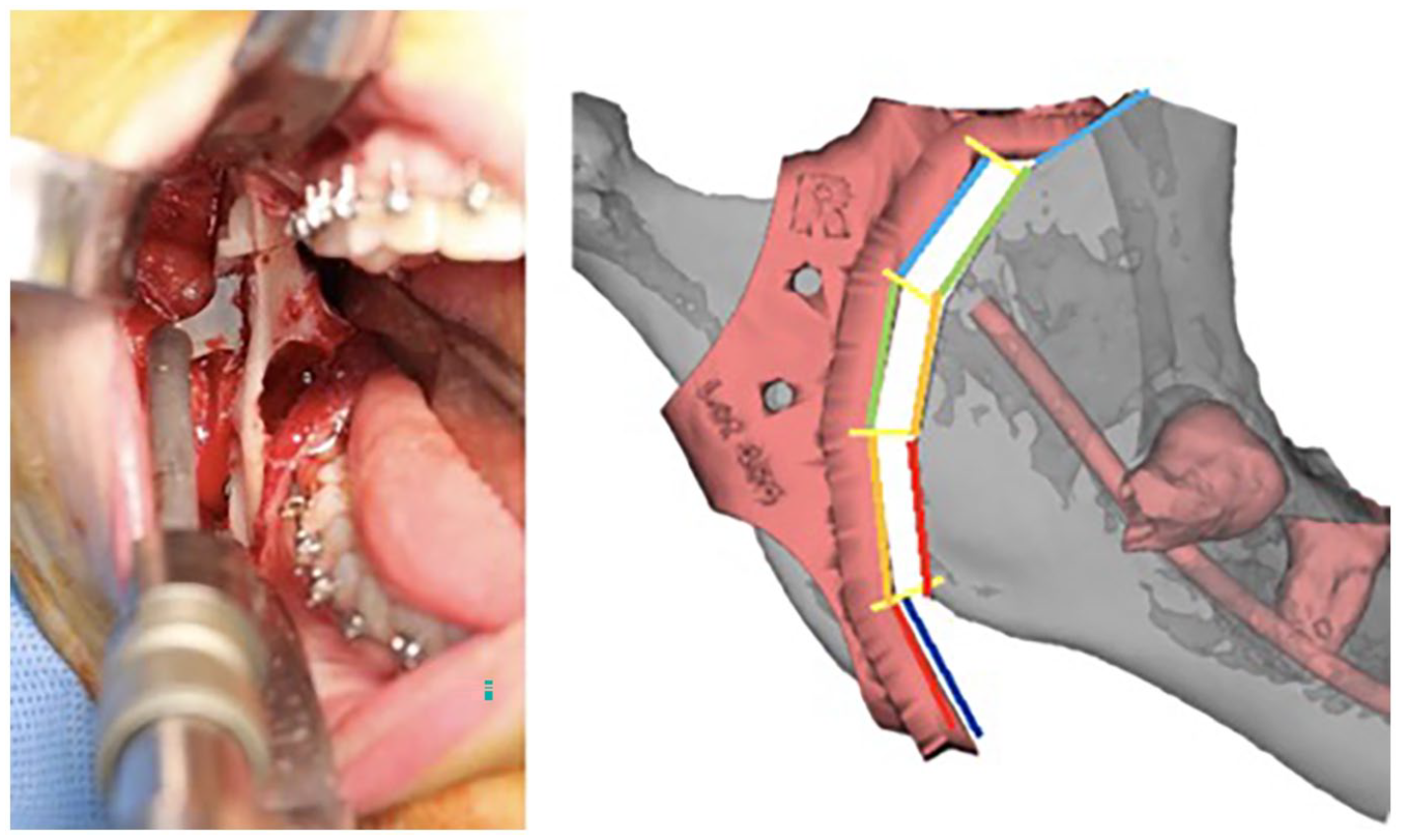
Intraoperative photo with splint in place. Notice the cogwheel design to provide stability and accommodate the conventional oscillating saw.
Following the release of the maxillomandibular fixation, the patient was found to reproducibly bite into the intermediate splint reproducibly and accurately. Thurs surgery then proceeded onto the maxilla where a 3-piece Lefort advancement with down-grafting was completed (Figure 4). The grafting was completed using freeze-dried corticocancellous block that was appropriately trimmed to fit in the anterior osteotomy gaps and secured with 10 mm screws in order to prevent relapse. The parasagittal and interdental gaps were grafted with autogenous bone harvested from the nasal crest of the maxilla as well as bilateral coronoids. Four “L” shaped plates were placed with 2 in the pyriform region and 2 at the zygomaticomaxillary buttress. Her final splint was then removed. Her distance from nasion to the surgical arch wire between brackets #8 and 9 was then found to be 55 mm at the completion of the case with a change in occlusal plane of 18° and excellent bony contact in the ramus without interference. While this corrected the occlusal plane to 0°, it is still shy of the normal value of 1.5° to 14°. The patient was then placed in guiding elastics bilaterally to aid in training her muscles of mastication to her new occlusion. There was no maxillomandibular fixation applied.
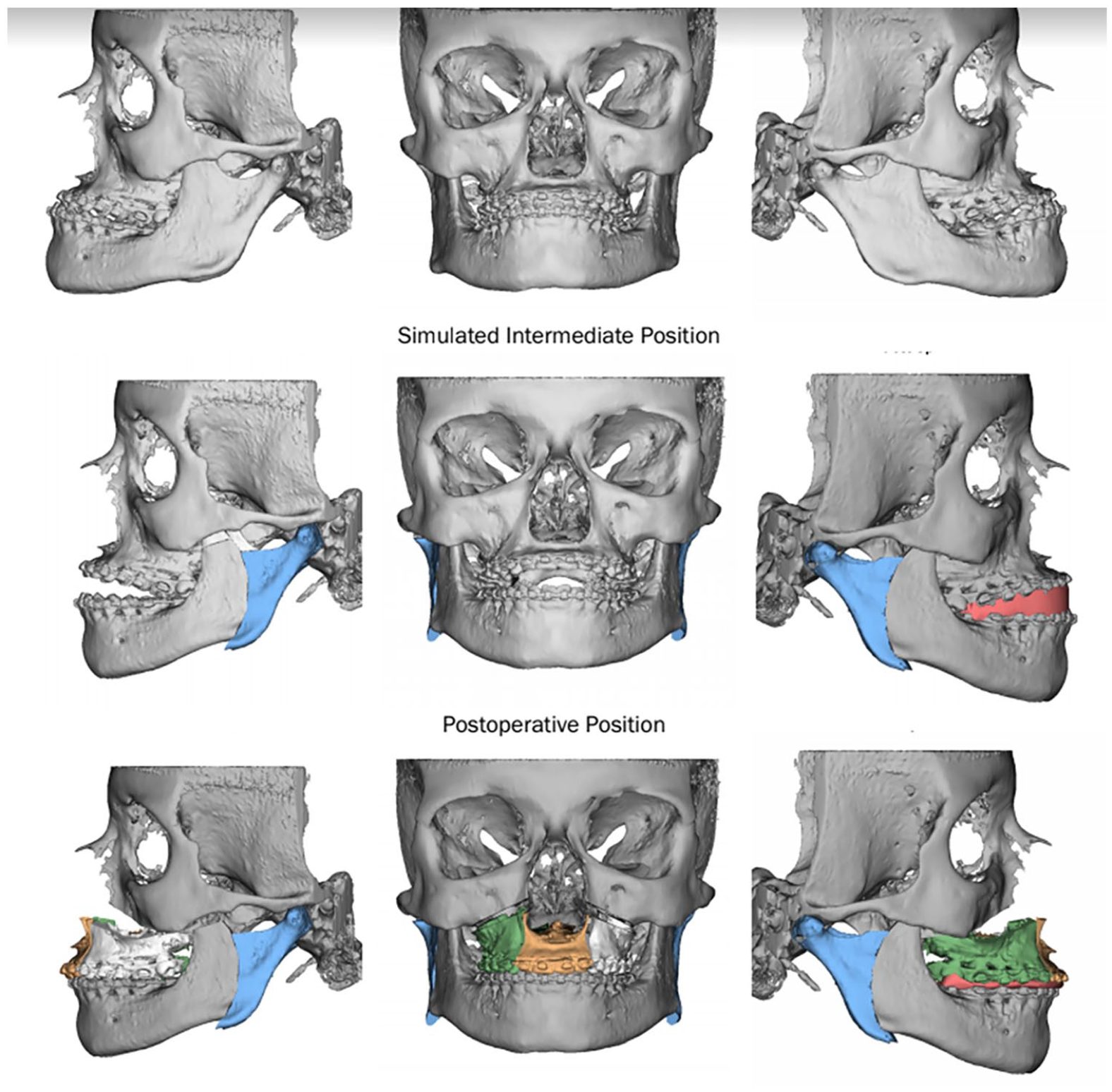
Proposed radiographic representation of orthognathic movements including modified C-osteotomy.
The patient remained in the hospital for a single night and was then seen in the office the next day for post operative imaging and regular hygiene. She was then seen back at 1, 3, and 6 weeks. There were no complications during the surgery. The patient was most recently seen for follow-up 22 months after her surgery and is continuing to do well subjectively and clinically without any complications or signs of relapse (Figures 5 to 8).

Twenty-two-month postoperative frontal photograph.

Twenty-two-month postoperative lateral photograph.

Postoperative panoramic radiograph.
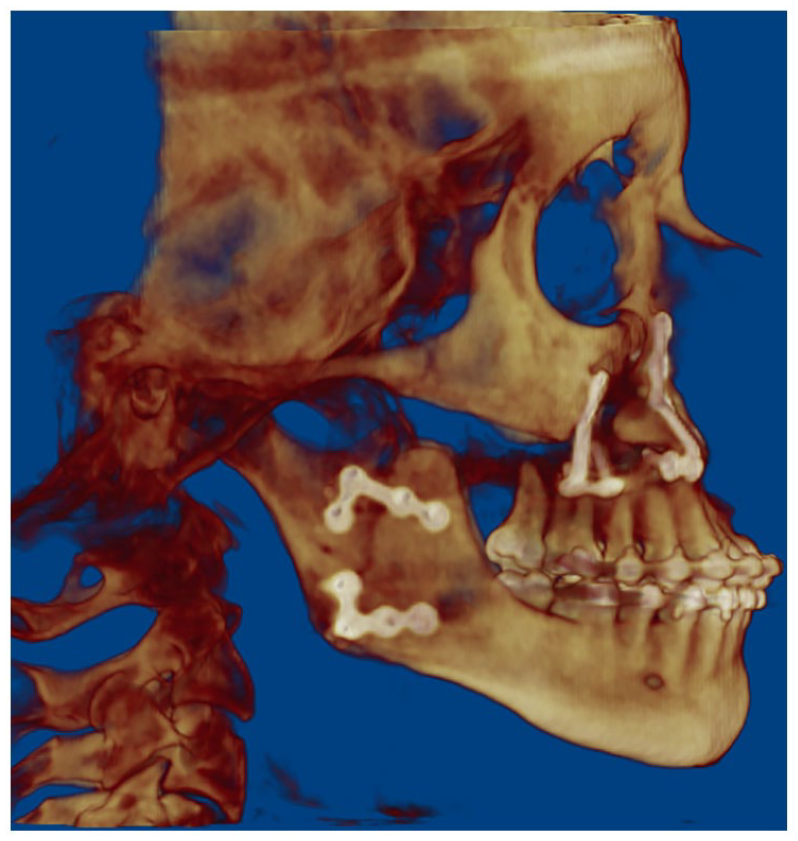
Postoperative lateral ceph (reformatted).
Discussion
Variable “phenotypic heterogeneity” exists amongst Class III malocclusion, comprising as many as 5 subclassifications.2,7 Our above mentioned patient represents one such subclassification: a vertically deficient maxilla with a prominent pogonion. 1 Often, they exhibit a rather flat occlusal plane with deep overbite along with malar flattening. This skeletal architecture often lends itself to undesirable soft tissue draping: scleral show, shallow labiomental folds, minimal to no maxillary tooth to upper lip relationship, and lip incompetence. 8
While maxillary advancement alone can correct the skeletal abnormality, clockwise rotation of the maxilla can provide superior results. Such alterations to the pitch drastically improves the soft tissue stigmata. Correction of the negative vector relationship between the ocular globe and lower eyelid enhances the periorbital soft tissue and corrects scleral show.3,9 Moreover, clockwise rotation to the entire maxillomandibular complex as it uniquely addresses the A-point to B-point relationship. 10 In essence, the mandibular incisors remain unchanged in the sagittal plane while allowing the posterior movement of the pogonion. The concurrent mandibular surgery has been shown to slenderize and soften the square appearance of the lower facial thirds while augmenting the midface.9,10
Caldwell et al. 11 introduced his C-shaped modification to the inverted L osteotomy. The new “technic” addressed 2 main issues that were encountered with the recently developed Obwegeser/Dal Pont’s sagittal split osteotomy (SSO): perceived inadequate bony apposition at site of osteotomy and injury to the inferior alveolar nerve. 12 Other authors cited additional advantages over SSO including conservation of gonial angle, adequate fixation due to increased bone contact, and relative technical ease.13,14 More importantly, the associated minimal masticatory muscle repositioning, particularly the minimal dissection of medial pterygoid and masseter muscles, was shown to significantly maintain mandibular viability after orthognathic osteotomies in animal models. 15
As with novel techniques, they eventually become heavily scrutinized with reports of increased complications such as alveolar segmental necrosis when combined with additional mandibular osteotomies.16,17 Furthermore, mandibular advancements required “mortised” iliac bone grafts. 11 Additionally, refinements to the SSO technique by Hunsuck 18 and Epker 19 along with the development of plate and screw fixation by Luhr, 20 ultimately led to SSO becoming the preferred technique.
With its decline in popularity, literature on C-osteotomy has become almost nonexistent since the 1980s (Supplemental Table 1). Meanwhile, intraoral vertical ramus osteotomies (IVRO) gained traction and has become the standard vertical osteotomy.13,21 Our literature review revealed only 1 recent study evaluating complications associated with a modified C-osteotomy. 22 In their cohort of C-shaped osteotomies, Kawase-Koga et al found 2 incidences of condylar luxation out of 37 rami (5.4%). They concluded the results and complications to be comparable to other IVRO designs (vertical and oblique).
We describe a case report of modified C-osteotomy intentionally to facilitate clockwise rotation. In Kawase-Koga et al.’s study, the classification of osteotomies were determined on postoperative panoramic radiographs suggesting that curvilinear osteotomy was not planned preoperatively. There have been reports and case series of linear angled variations of ramus osteotomies such as Y or J shapes to allow for minor rotational movements.21,23,24,25 However, we believe that the curvilinear design of this modified C-osteotomy facilitates greater arc of rotation while optimizing bone contacts between proximal and distal segments.
Bimaxillary surgery with a large clockwise rotation was strongly indicated for our patient. During the preoperative planning phase, multiple mandibular osteotomies were explored including a BSSO, IVRO, and Inverted-L. The planning was completed using Guided Surgical Solutions (Denver, CO). None were able to provide an adequate bony interface free from interference due to the degree of maxillary hypoplasia and reverse occlusal plane angle. As shown in Figure 9, there was roughly 4 mm of interference in all directions with the BSSO approach which puts the inferior alveolar nerve at increased risk of injury. It was also apparent that more rotational movement was required to improve some of her functional symptoms: abnormal speech patterns related to incisor-tooth relationship and difficulty in mastication. Adding to the fact that she also exhibited temporomandibular symptoms, the C-osteotomy pattern, similar to IVRO, was selected.
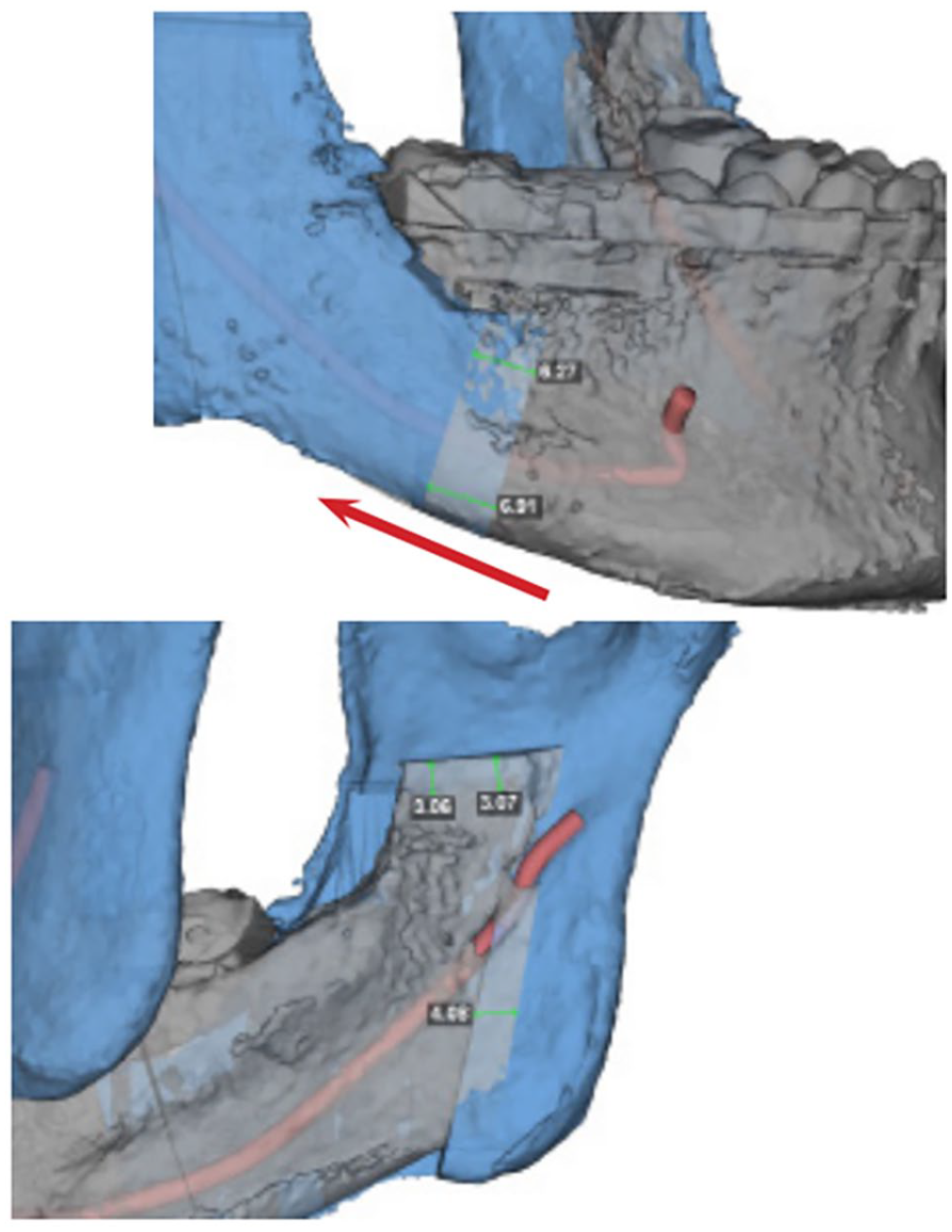
Bilateral Sagittal Split Osteotomy plan showing interference.
Important technical considerations in this case are also worth noting. Conventional oscillating saw, rather than piezosurgery, was used to osteotomize the ramus. As such, a cogwheel rather than a smooth curvilinear design was made (Figure 3). Concerns of relapse due to temporalis attachment to the coronoid process and trismus due to the coronoid process itself are valid. As such, release of temporalis muscle from the coronoid or bilateral coronoidectomies should be considered.
Despite the loss in popularity as indicated by the paucity in literature in recent decades, we believe C-osteotomy should be revisited. Concerns regarding precision and accuracy of osteotomies performed under limited and poor visibility should be mitigated with the advent of customized patient specific stereolithographic templates. Such cutting guides have shown to increase intraoperative accuracy and efficiency in performing these osteotomies. 26
Although it may have fallen out of favor in a majority of orthognathic cases, its considerations should be made for such patients requiring bimaxillary rotational movement with minimal anteroposterior mandibular movement. This particularly would imply to patients with the common class III abnormality: maxillary hypoplasia with relative mandibular excess exhibiting convergent, concave facial profile.
Conclusion
In summary, we present a case report in which a modified C-osteotomy of the ramus was able to accommodate the large clockwise rotation in a patient with severe maxillary hypoplasia exhibiting pseudo-prognathism.
Supplemental Material
sj-docx-1-fac-10.1177_27325016211048203 – Supplemental material for Improving Esthetic and Functional Outcomes of Severe Habsburg Jaw Using Modified Mandibular C-Osteotomies: A Case Report and Review of Literature
Supplemental material, sj-docx-1-fac-10.1177_27325016211048203 for Improving Esthetic and Functional Outcomes of Severe Habsburg Jaw Using Modified Mandibular C-Osteotomies: A Case Report and Review of Literature by Andrew M. Henry, Jason W. Yu and Brian B. Farrell in American Society of Maxillofacial Surgeons
Footnotes
Author Contributions
Andrew M. Henry, DMD, MD made substantial contributions to the conception and design of the manuscript, assisted in the drafting and revising of the manuscript, approved the final version to be published, and ensured the accuracy and integrity of the work. Jason W. Yu, DMD, MD made substantial contributions to the conception and design of the manuscript, assisted in drafting and revising of the manuscript, and ensured accuracy and integrity of the work. Brian B. Farrell, DDS, MD, FACS made substantial contributions to the conception and design of the manuscript, assisted in the drafting and revising of the manuscript, approved the final version to be published, and ensured the accuracy and integrity of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.