
Abstract
We report a rare case of an extramedullary plasmacytoma (EMP) in the frontal sinus with an indolent clinical presentation. Although a history of trauma was absent, the initial diagnosis was a mucocele, based on the radiological findings. Upon surgical excision, the patient was found to have an EMP. EMP, a form of solitary plasmacytoma, has a significantly high rate of conversion to multiple myeloma. This mandates long-term follow-up, even after successful radiotherapy and/or resection. While radiation therapy is generally considered a first line treatment for EMP, surgical intervention may provide optimal treatment in complicated cases. This case presentation highlights the prognosis of patients diagnosed with EMP.
Introduction
Plasmacytomas are CD-138 positive non-epithelial neoplasms originating from plasma cells and classified as a sub-type of non-Hodgkin lymphoma. 1 These tumors are differentiated from multiple myeloma by lack of bone marrow involvement, systemic spread, hypercalcemia, and anemia. 1 Initial work-up for a suspected plasmacytoma should exclude multiple myeloma by ruling out systemic involvement. 1 Plasmacytomas are further classified into solitary and extramedullary plasmacytoma. Although extramedullary plasmacytoma (EMP) and solitary plasmacytoma (SPB) both originate from plasma cells and are regionally isolated, the differentiation is important to quantify risk of progression to multiple myeloma (MM). EMPs less frequently progress to MM, changing their treatment.2,3
EMPs are uncommon tumors comprising only 3% to 4% of all plasma cell neoplasia and represent 1% of head and neck tumors. EMP most commonly present within the fifth decade of life and have been found to affect men 3 times more often than women.4,5 Approximately 80% of EMPs occur in the upper respiratory tract with a 11% to 33% conversion rate to multiple myeloma in 10 years. 6 The optimal treatment for extramedullary plasmacytomas is not standardized and depends on tumor location, size, and recurrence. EMPs are highly responsive to radiation. Various studies have shown that radiation doses of 40 to 50 grays (Gy) have resolved plasmacytomas and increased survival.4,7-10 However, a few cases of radiation-resistant EMP have been reported.11,12 Surgical excision offers the benefits of local control and may avoid need for postoperative adjuvant radiation therapy. However, large tumors and tumors involving vital structures are often unable to be fully excised with clear margins, requiring post-operative adjuvant radiation therapy. Advancements in radiation therapy strategies and head and neck surgery have allowed for more accurate and safer treatment modalities for extramedullary plasmacytoma.
EMP are very rarely found within the frontal sinus. The authors located only 2 other case reports of frontal sinus EMP in the literature. 7 We report a case of an extramedullary plasmacytoma localized to the frontal sinus treated with resection and obliteration of the frontal sinus. Patient underwent focal adjuvant postoperative radiation therapy. The patient has had no clinical or radiological evidence of local or regional recurrence to date. However, the patient was found to have a Kappa light chain transformation to myeloma.
Case Presentation
We present a case of a 60-year-old asymptomatic female who presented to her primary care physician after noticing a pulsatile erosion in the frontal bone of her skull. At the time of presentation, the patient denied any other neurological or obstructive symptoms. The patient underwent magnetic resonance imaging (MRI) and computed tomography (CT) of the Head, which revealed a 7 cm × 7 cm × 3 cm mass in her frontal sinus compressing the frontal lobe of her brain (Figure 1). Despite the absent history of trauma, the location of the mass and radiological findings led to a presumptive diagnosis of frontal sinus mucocele. The preoperative neurosurgical plan was surgical excision of the “frontal sinus mucocele” and obliteration of the frontal sinus.
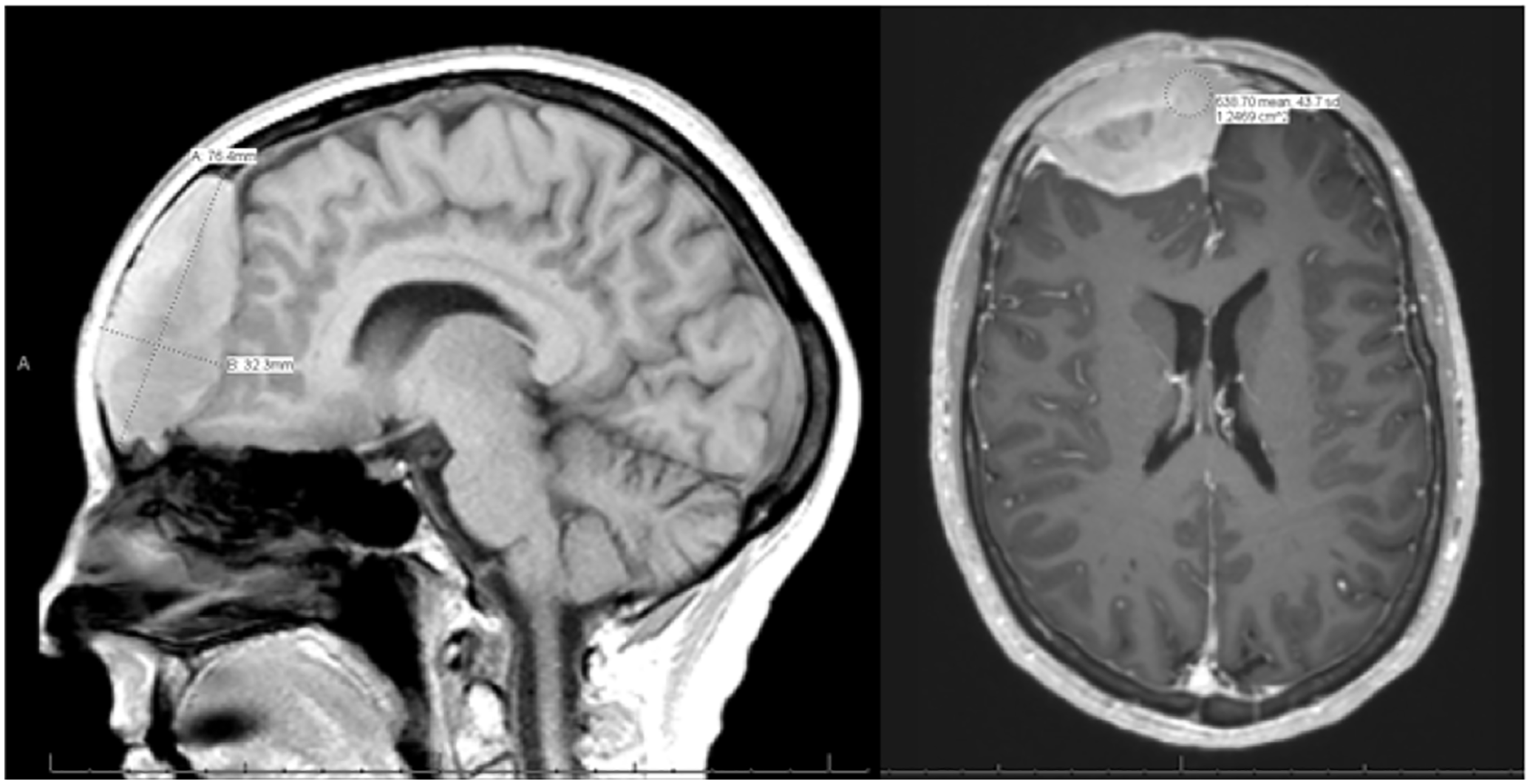
Pre-operative T1-weighted MRI.
Management/Outcome
The patient underwent wide local resection of the frontal sinus lesion with obliteration of her frontal sinus (Figure 2). Intraoperative findings included a 3 cm × 3 cm erosion of the anterior table of the frontal sinus. During the resection, the lesion did not violate the dura, which allowed for complete resection. The lesion was easily differentiated from the dura and surrounding structures with well-defined borders.
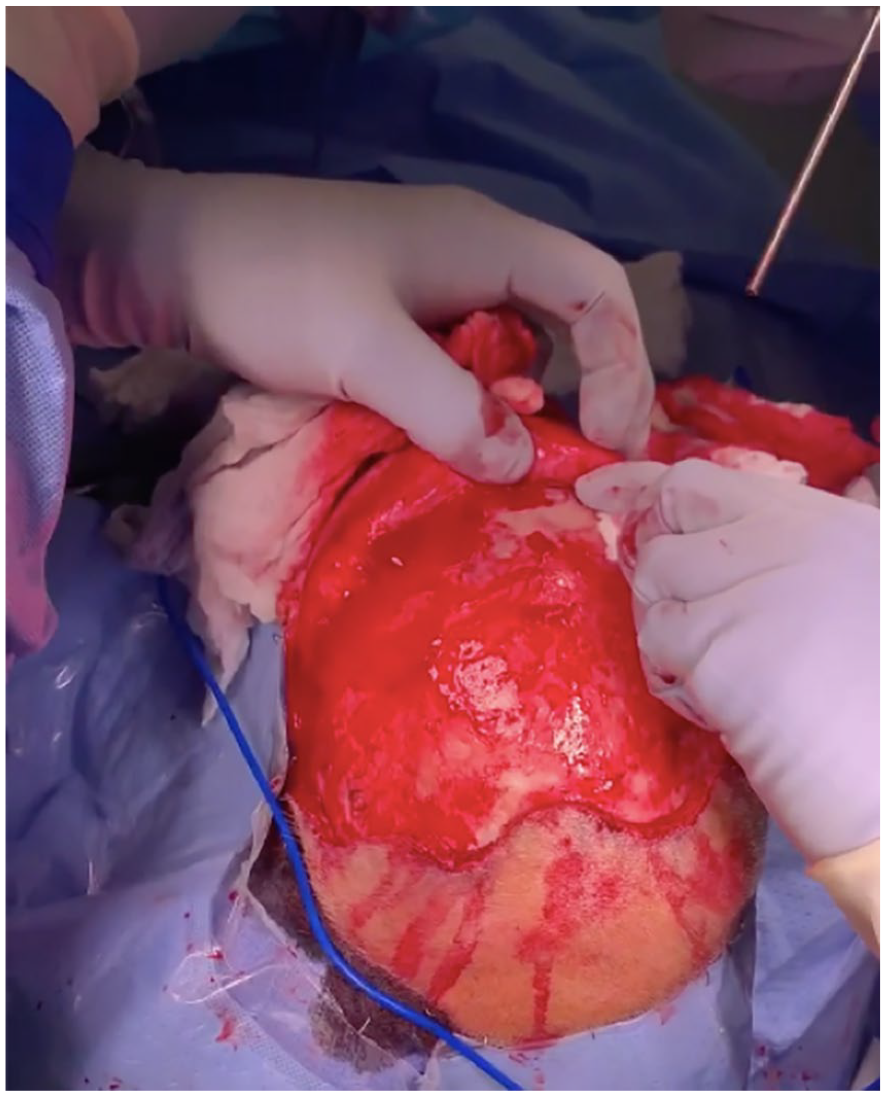
Intra-operative view of frontal sinus mass resection with bony erosion of the frontal bone.
Histopathology was positive for CD 138 and had kappa light chain restriction consistent with extra osseous plasmacytosis. The specimen removed had negative margins. This unexpected result led the patient to undergo further hematologic workup with bone marrow biopsy and positron emission tomography (PET) CT did not have findings concerning for multiple myeloma. Follow-up MRI indicated complete resection of the plasmacytoma (Figure 3). PET/CT confirmed that there was no residual disease or additional foci of disease. The patient was discussed at tumor board, and postoperative radiation was recommended. She received 37.8 Gy/14 fractions to the frontal skull out of the recommended 40.05 Gy with intensity-modulated radiation therapy (IMRT) approach. 7 months post-resection the patient developed severe mid-back pain due to a lesion in the T8 vertebral body causing compression fracture. The patient received palliative radiation therapy 3 Gy/10 fractions to T7 through T9 vertebrae. The patient is currently on oral chemotherapy at present due to the distant metastasis. The patient is currently 18 months post-resection. She will continue to undergo hematological monitoring with the hematology-oncology service every 4 months. A follow-up MRI Brain will be obtained every 6 months to monitor the progression of the disease.
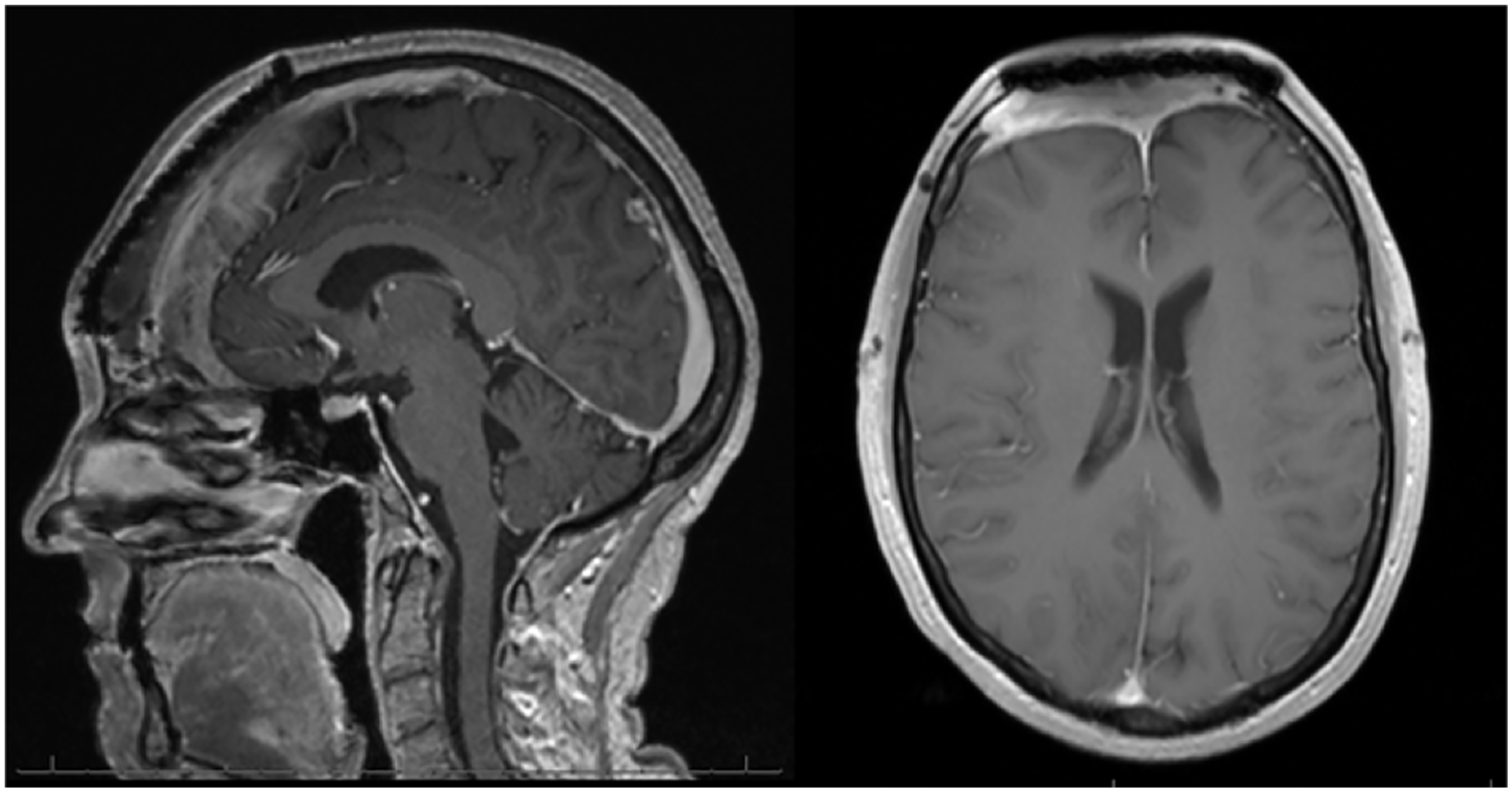
Post-operative T1-weighted MRI.
Discussion
The clinical presentation of paranasal sinus EMPs depends on the volume of the mass and site of involvement. This type of tumor is slow growing, and patients generally become symptomatic once the mass completely fills the sinus cavity. EMPs are usually diagnosed after the patients experience symptoms of nasal obstruction, soft tissue swelling, epistaxis, nasal discharge, pain, and proptosis, observed in decreasing order of frequency. 13 Our patient was asymptomatic at the time of presentation. Fortunately, the EMP did not infiltrate into the dura and the mass could be completely resected from the frontal sinus.
Initially, the surgical plan included utilizing a split calvarial bone graft for reconstruction of the frontal calvarium. However, given the extent of bone resection, a large MEDPOR TITAN (Stryker, USA) implant measuring 10 cm × 7.6 cm × 1.5 cm was chosen intraoperatively. MEDPOR TITAN was selected for the cranioplasty for its cosmetic outcomes (Figure 4) as well as low complication rates per literature.14,15 The National Cancer Center Network recommends that patients with EMP undergo 6-month follow-up intervals for testing for progression to multiple myeloma. This involves serum albumin, corrected calcium, creatinine, and platelet count. 1
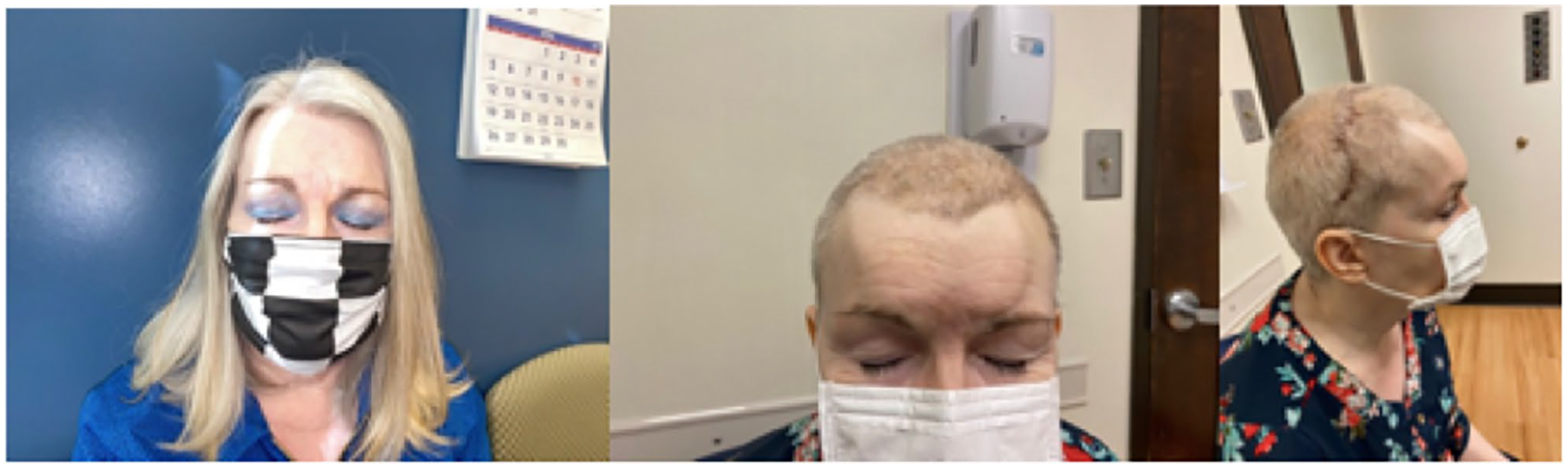
(a) Pre-operative clinical photographs and (b–d) post-operative clinical photographs.
While this is a rare condition, EMP should always be considered when forming a differential diagnosis in older patients presenting with head and neck tumors or symptoms of nasal obstruction/abnormal nasal discharge. EMP have a reported conversion rate to multiple myeloma of 11% to 33% making long-term follow up mandatory even if adjuvant radiotherapy is pursued.
Conclusion
EMP of the frontal sinus is an extremely rare clinical presentation. A thorough systemic work up is required. Adjuvant radiation therapy was recommended in our patient, to mitigate risk of local recurrence given the size of the lesion. This case emphasizes the need for close monitoring and long term follow up for patients diagnosed with an EMP, because of the significantly high conversion rate to myeloma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.