
Abstract
Keywords
Introduction
Giant congenital melanocytic nevi are large pigmented lesions which can result in disfigurement of the head, neck, torso, and extremities, as well as significant associated psychological morbidity. It is estimated that 1 in 20 000 infants are born with giant congenital melanocytic nevi. 1 Giant congenital melanocytic nevi develop in utero between the 5th and 25th weeks of gestation and are typically present at birth, 2 but may not be appreciated until 2 years of age due to increasing pigmentation over time. 3 Lesions are classified according to their projected adult surface diameter. Small, medium, and giant nevi have projected diameters less than 1.5 cm, 1.5 to 20 cm, and greater than 20 cm, respectively. 4 It is anticipated that most nevi grow proportionately with age although rapid growth in the earlier stages of life is not uncommon. 5
Melanoblasts originate in the neural crest and migrate to many anatomical sites during weeks 8 and 10 of gestation, including the skin, eyes, and mucous membranes (Mort et al., Plastic Surgery Indications, Operations, and Outcomes). Throughout migration, any dysregulated growth in neuroectodermal development can result in congenital melanocytic nevi.6 -9 Although not well understood, giant congenital melanocytic nevi are predominantly caused by sporadic gain-of-function somatic mutations in either BRAF at V600 or NRAS at Q6. 10 It is also hypothesized that the genetic basis of congenital melanocytic nevi involves hepatic growth factor/scatter factor. Hepatic growth factor/scatter factor is associated with the development and migration of neuroectodermal cells and may be overexpressed in congenital melanocytic nevi. 3
Histological characteristics specific to congenital melanocytic nevi include nevus cells that extend into the lower two-thirds of the dermis and subcutaneous tissue, as well as infiltrate the extracellular space between collagen bundles, sebaceous glands, hair follicles, eccrine sweat glands, and arrector pili muscles. In some cases, a perifollicular and perivascular invasion may develop that resembles an inflammatory reaction.3,11 Histological patterns of giant congenital melanocytic nevi include compound or dermal nevus, blue nevus, neural nevus, and epithelioid cell nevus. 3
The purpose of the following review is to discuss the clinical presentation and complications of giant congenital melanocytic nevi pertaining to the head and neck, the breadth of treatment options, and the quality-of-life and outcomes after treatment.
Giant Congenital Melanocytic Nevus in General
Clinical Presentation and Characteristics
Giant congenital melanocytic nevi represent lesions that vary in size, shape, color, and location. A nevus is generally round to oval shaped but can assume alternative shapes with more ill-defined or well-defined borders. Representative colors are usually shades of black or brown, and some nevi may not be pigmented. 12 The nevi may darken overtime or become more hypopigmented and diminish in size. As the child grows, the lesions may become increasingly darker with a uniform brown or black color. Nevi have occasionally been described to exhibit a verrucous, hairy, or pebbly surface. 11 The location of these nevi can be anywhere on the skin, including the face, extremities, and trunk, although it is most frequently identified on the posterior trunk.11,13
Approximately 80% of patients with giant congenital melanocytic nevi have satellite nevi that spread throughout the head and neck, trunk, and extremities. 14 Associated proliferative nodules can also form, which may indicate a potential malignancy, but may also be benign. 15 A particular type of associated nevus is the “divided nevus” or “kissing nevus.” These paired nevi occur on the fingers, penis, and eyelids. When the eyelids separate around the 24th week of gestation, the nevus divides into 2. Associated complications with kissing nevi include eyelid malposition, epiphora, and amblyopia. 16
Natural History and Complications
The natural history of giant congenital melanocytic nevi is one in which the nevi grow proportionally to the growth of the body. Dark, coarse hairs may develop within the first 2 years of life, and around 10 years of age, these nevi can have elevated ridges and grooves with hyperkeratosis, coarser hair, and the formation of dermal nodules. 17 These changes may moderate near the end of adolescence.
Giant congenital melanocytic nevi can lead to alteration of form and function to the affected body site, extracutaneous features, and systemic complications. Extracutaneous features involve distinct facial characteristics and complications of the central nervous system. When present, these findings are indicative of “congenital melanocytic nevus syndrome” and patients with the giant subtype are at the highest risk. 18 Additional systemic complications can include scoliosis, limb dysfunction, and spinal dysraphism. 19
Although generally asymptomatic, giant congenital melanocytic nevi may have clinical features of ulceration, xerosis, pruritus, and skin erosion. 20 These indications, alongside focal growths, tenderness, pain, and bleeding, may be indicative of malignant transformation. 21 Recent data suggests that the true risk of melanoma transformation lies between 0.7% and 2.8%.22,23 Additional complications include psychosocial dysfunction due to an esthetic outcome, as well as the severe physical and psychological distress that may develop in response to a prolonged treatment course, which inherently places the patient at risk of medical and surgical complications.3,24
Malignant Melanoma
While the main focus of plastic surgeons is on cutaneous melanoma, it is important to recognize that malignant transformation can often take the form of noncutaneous melanoma. 19 Specifically, these areas can involve the mucosa of the gastrointestinal tract, retroperitoneum, and deposits of neurocutaneous melanosis. The risk of malignant transformation in patients with giant congenital melanocytic nevi varies widely with reports ranging from 1.7% to 45% 25 ; however, most studies report a risk of 3% to 8%.1,22 A lifetime risk of patients with giant congenital melanocytic nevi developing melanoma is estimated to be 6.3%, which is nearly a 17-fold increased risk compared to the general population. 26
Significant risk factors for the development of melanoma include 3 or more lesions, size (20 cm diameter or greater), and younger age (3-5 years).2,25 Given that young age increases the risk for malignant transformation, complete surgical excision for high-risk cutaneous nevi is recommended in early childhood rather than in adulthood. To date, treatment strategies for melanoma in the pediatric population remain less studied than in the adult population. As in the adult population, the use of sentinel node biopsy for staging pediatric melanoma has been adopted and become widespread. The thickness of the primary tumor, as well as any ulceration, have been linked to a higher incidence of nodal involvement. 27 Mode of treatment and prognosis are subsequently linked to the disease stage.
Neurocutaneous Melanoma
Neurocutaneous melanoma is described as benign or malignant melanocytic proliferation in the central nervous system (leptomeningeal melanosis) with patients having a giant congenital melanocytic nevi or 3 smaller nevi. 28 It is a very rare disease with prevalence estimated at 1:50,000 to 1:200,000.18,29 Factors that have been reported to increase the risk for neurocutaneous melanoma include the presence of many satellite nevi (>20) and congenital melanocytic nevi in the midline of the trunk or calvaria. 24 Though satellite lesions may represent early stigmata of melanoma, melanoma itself has never been reported in a satellite lesion. 30
Neurocutaneous melanoma is the result of an inborn embryologic error of neuroectodermal development with dysregulation and proliferation of melanoblasts.24,28 These depositions may occur naturally in the brain and spinal cord with most being asymptomatic. Regardless of malignant transformation, however, neurocutaneous melanosis may become symptomatic with patients presenting with signs of hydrocephalus, seizures, cranial nerve palsies, and developmental delay. 24
Neurocutaneous melanoma peaks at 2 critical age groups. Patients between 2 and 3 years of age with neurocutaneous melanoma may present with hydrocephalus, increased intracranial pressure, papilledema, constant headaches, and developmental delay. 24 The later peak occurs among those patients 20 to 30 years old whereby these patients may present clinically with large lesions, increased intracranial pressure, or spinal cord compression. 5 Patients with any aforementioned risk factors should undergo a magnetic resonance imaging (MRI) scan of the brain and spinal cord between 4 and 6 months of age before myelination of the brain obstructs the view of the melanocytic deposits (Figure 1).2,24
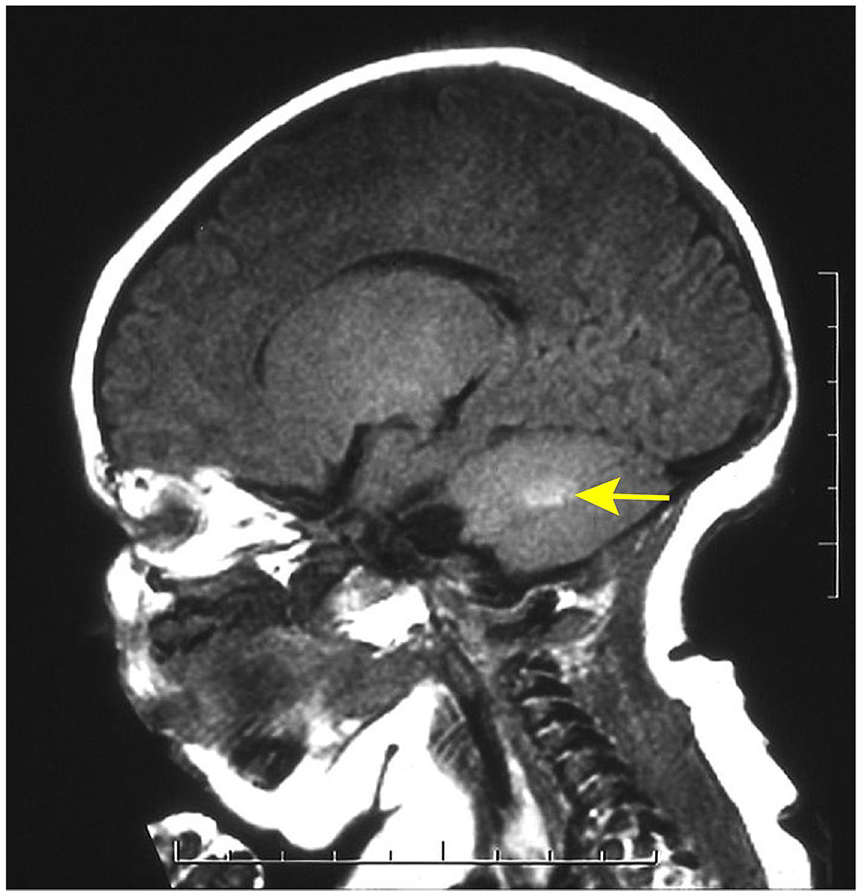
Surveillance magnetic resonance imaging of a 3-month-old girl with giant congenital melanocytic nevi in a “bathing trunk” distribution revealed a focus of leptomeningeal melanosis (yellow arrow).
Given the severity and rarity of neurocutaneous melanoma, any diagnosed cases should be referred for additional medical and surgery treatment often including surgical excision, ventriculoperitoneal shunt placement, radiation therapy, or immune modulation. 24 Lifelong monitoring for progression of malignant nevi is essential given the poor prognosis with death frequently occurring within 3 years after initial diagnosis. 2 Management of asymptomatic neurocutaneous melanoma remains controversial; however, serial MRI scans should be conducted with the time intervals determined on a per patient basis. Importantly, the treatment of cutaneous CMN should not be changed despite the presence of asymptomatic neurocutaneous melanosis.
Treatment
Indications for Treatment
Indications for treatment depend on the size of the nevus, pigmentation (to decrease the melanocytic load), established melanoma, persistent symptoms, maintenance of function, and psychological burden.17,30,31 Prompt surgical removal has historically been recommended in early childhood to lower the risk of malignant transformation22,32; however, recent evidence suggests the risk is lower than previously described and early excision may not reduce the risk of developing melanoma.6,31,33 -35 Nonetheless, many continue to advocate for early intervention given the profound psychological benefit 35 and observed patient tolerance of treatment at younger ages.24,31 Specifically, the literature supports initiating treatment at 6 months of age with completion prior to starting school.31,34
A multidisciplinary approach should be applied in the treatment of patients with giant congenital melanocytic nevi. This may include consultation from dermatologists, plastic surgeons, neurosurgeons, radiologists, and pediatricians. 2 Work-up should include a thorough, frequent examination by a dermatologist and discussion with a plastic surgeon early in the clinical course. Regular monitoring is essential, as the presence of satellite nevi or ill-defined margins may indicate malignant transformation, although this has been controversial in the literature. 11 Furthermore, given the significant psychosocial impact on children and parents alike, a clinical psychologist should become involved in the care of the patient early on. 29
Those that do not undergo treatment should still monitor for changes of the nevus suggestive of malignant transformation. In contrast to malignancy of small and medium congenital nevi that begin at the dermal-epidermal junction that quickly alter its appearance, a cancer diagnosis of giant congenital melanocytic nevus typically requires the development of a large nodule or ulceration. 36 The nodular and rough surface of giant nevi often prevents early tumor observation. 26
Non-Surgical Treatment
Treatment approaches for giant congenital melanocytic nevi are either non-surgical, which focus on esthetic outcomes, and surgical, which focus on both esthetic and oncologic outcomes. In general, non-surgical treatment approaches focused on the esthetic appearance of the nevus with the goal of avoiding undesirable scarring. These approaches are controversial due to the inability to obtain a tissue diagnosis or surveil for recurrent disease, and undocumented impact on the oncologic sequelae of the nevus. 35 As such, esthetic treatment methods focus on desquamation of the more superficial layer of cells and do not necessarily address the increased density of nevi (pigment-producing cells derived from melanocytes) in the deeper dermis.24,37 In 1 porcine study that ranked the depth of injury of different esthetic resurfacing modalities, it was found that 1 phenol chemical peel yielded the deepest injury, followed by 3 carbon dioxide laser treatments, 1 dermabrasion, and 1 carbon dioxide laser treatment giving rise to the most superficial changes. 38
Chemical peels and laser ablation are the most commonly used nonexcisional methods. First described by Brown in 1959, 39 deep chemical peels that contain phenol were found to produce a smoother and less pigmented outer surface with mid-reticular dermal injury, marked collagen formation, and organization of elastic fibers below the surface. 40 In the adult literature, histological effects of phenol chemical peels have been found to persist for 15 to 20 years after treatment. 41 In the pediatric literature, a study of 20 patients determined that approximately 2.6 peels were required to achieve optimal lightening of a congenital melanocytic lesion within 6 to 84 months. 42
In regard to Light Amplification by Stimulated Emission of Radiation or “laser’ ablation, high-intensity monochromatic light is transmitted to a chromophore of interest with a specific wavelength of energy that destroys the target while sparing surrounding tissue.43,44 Approximately 20 different lasers or combination modalities have been described in the literature for the management of giant congenital melanocytic nevi24,45 -48; however, the most preferred is the 10 600 nm carbon dioxide laser that targets water and removes melanin via selective photothermolysis. 49
Of note, the longer wavelength of 10,600 nm utilized in carbon dioxide lasers (wavelength selective for melanin is between 630 and 1100 nm 50 ) allows for deeper penetration of the skin, but has been criticized for undesirable thermal effects and hypertrophic scarring.51,52 In a review of 12 patients with congenital melanocytic nevi treated with carbon dioxide laser ablation, half developed hypertrophic scarring within 5 years of treatment (P = .01). 51 The authors concluded its use should be avoided in areas where the skin is poor quality or the dermis is thinned, which is not ideal in previously operated fields. 51 Several reports in the dermatology literature have also criticized lasers for the development of malignant melanoma after treatment,53 -55 a finding which has been supported by in vitro studies of melanocytes that demonstrated increased risk of malignant transformation after exposure to laser energy.56 -58 Owing to the heterogeneity of studies, however, there is no high quality evidence for the long-term safety of lasers. 47
Surgical Treatment
When considering surgical treatment for lesions with malignant potential (pigmented or nonpigmented), a multimodal approach is generally employed, including serial excision, excision with skin grafting and/or skin substitutes, and tissue expansion. Serial excision is recommended if the lesion is amenable to complete removal in 3 stages or fewer. 13 Benefits of serial excision include a shorter resulting scar than if the original lesion were to undergo a single-stage elliptical excision, 59 as well as shorter procedure time, minimal pain, and, in most cases, outpatient surgery when compared to other reconstructive options. 60 Elasticity of the surrounding tissue dictates the extent of skin excised during each procedure, and approximately 3 to 6 months of recovery is recommended between each excision to allow for adequate relaxation of the tissue and scar maturation. 60
In areas where excision may compromise functionality due to extensive tissue displacement and traction (ie, eyelids, perioral folds, large scalp lesions, etc.), reconstruction with skin grafts is advised. 60 On account of a more optimal esthetic outcome with less skin contracture, split thickness skin grafts have largely been supplanted by expanded full thickness skin grafts (Figure 2). 24 Nevertheless, the use of allogeneic split thickness skin grafts may still have a role in garment-like giant congenital nevi, where there is deficient available donor skin for grafting and dermal substitutes serve as a scaffold for coverage with a split thickness skin graft.61,62
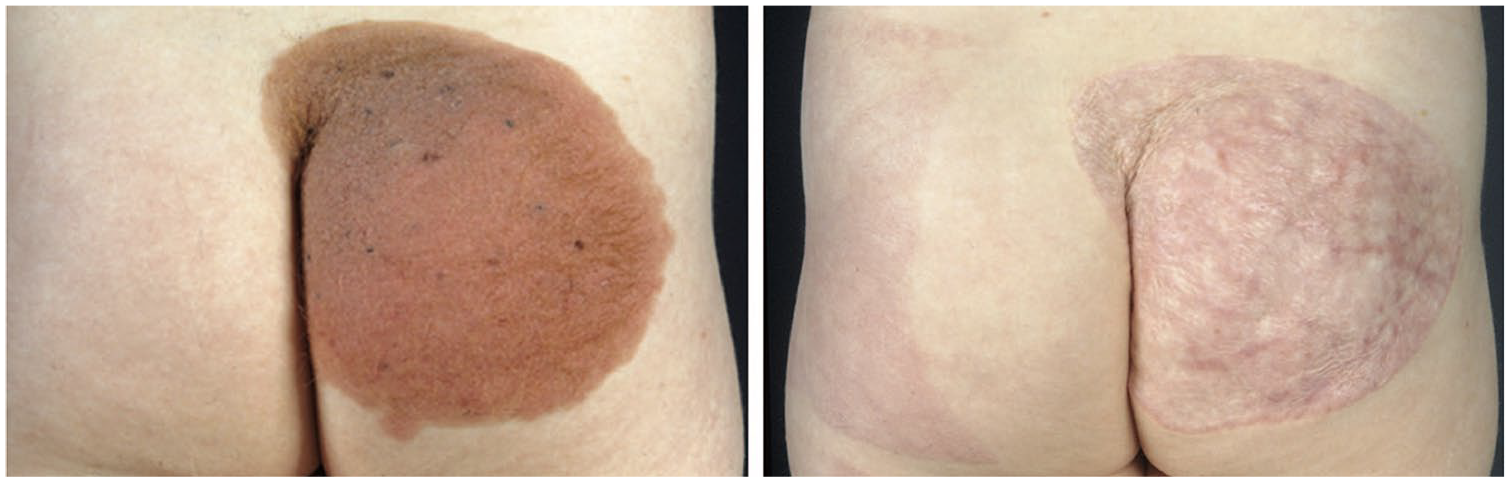
An 8-year-old girl presented with a giant congenital melanocytic nevus of the buttock (Left). The family preferred reconstruction in 1 stage, and the buttock was resurfaced with a split-thickness skin graft (Right). At 1 year postoperatively, note the difference in esthetic coverage between native buttock skin and the skin graft.
Tissue expanders create a highly versatile piece of tissue that can be utilized not only as an expanded full thickness skin graft, but also as an expanded advancement, rotation, transposition, or free flap. 13 Tissue expansion is typically performed over a 3- to 6-month interval prior to excision of the lesion, with weekly inflations that may be performed at home if proper teaching, anticipatory guidance, and psychological support are provided.13,63 At the time of excision of the melanocytic nevus, the tissue expander is also removed and the expanded skin is rearranged to cover the soft tissue defect. Investigation of tissue expansion protocols that elicit optimal results is currently underway in a porcine model that utilizes computational modeling to determine differential growth and stretch of skin based on fill volume, fill frequency, and location of the expander. 64
Despite its widespread use, tissue expansion is fraught with complications in approximately 13% to 40% of cases.63,65 -67 Complications are highest for serial expansion beyond the second round of expansion and lower extremity expansions due to the relatively inflexible skin and potential for migration in these areas.13,63 As such, the role of tissue expanders is most prevalent in head and neck cases, where multiple tissue expanders have been shown to decrease the risk of complications (Figure 3). 21
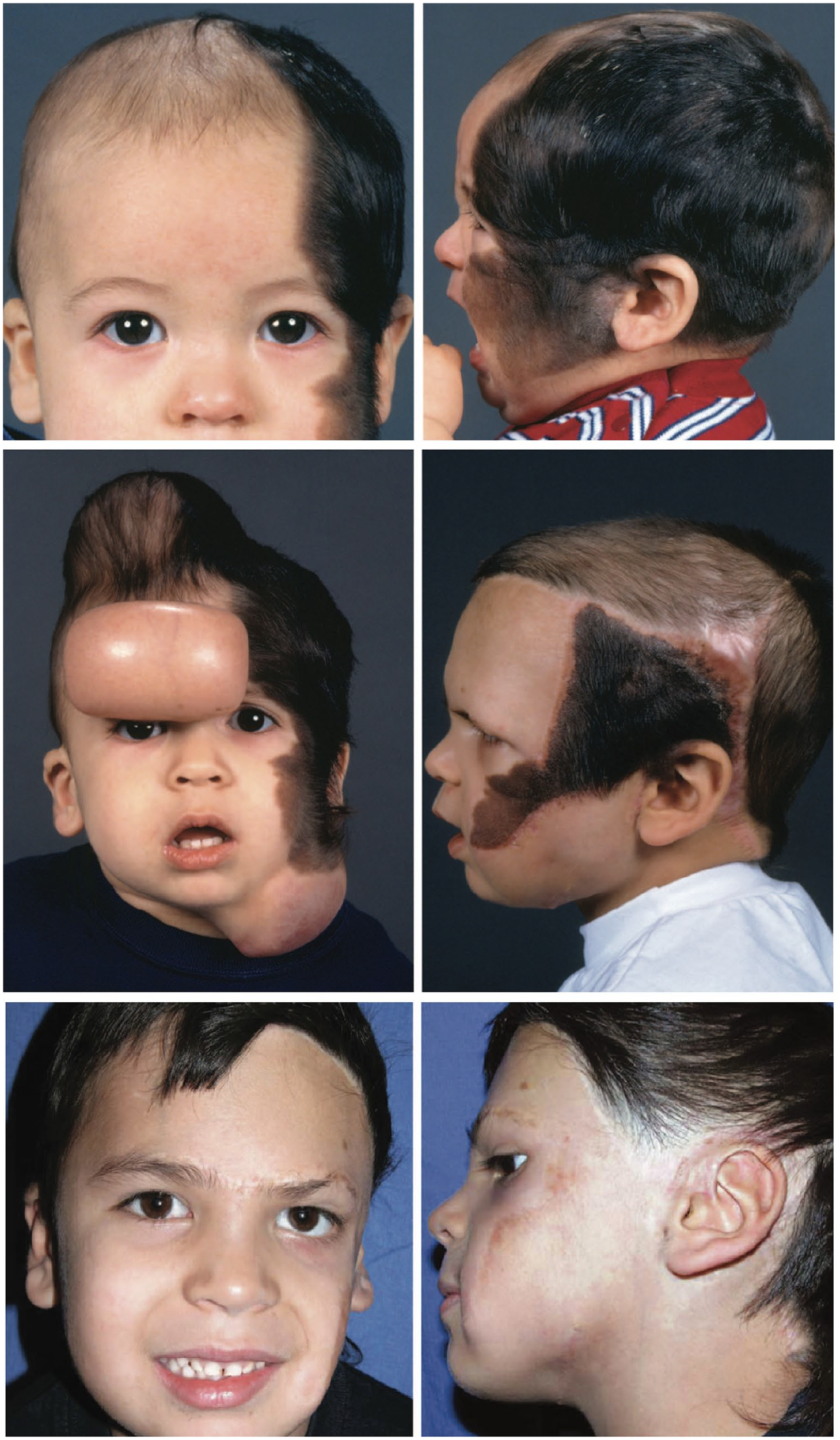
(Top) A 2-year-old boy presented with a giant congenital melanocytic nevus involving the scalp and face. (Middle) Three expanders were placed to reconstruct adjacent tissues in the scalp, forehead, and neck. (Bottom) The final outcome of the patient following completion of tissue expansion.
Major complications that require immediate removal of the expander include exposure, rupture of the expander, and infection. 63 Placement of expanders in the scalp has been cited as a risk factor for rupture due to sports and patient activities such as tumbling that has been observed in younger patients. 63 Infections can be viewed as minor and major. Minor infections consist of localized cellulitis, and this can be managed conservatively with antibiotic therapy at the onset. If infection persists and leads to recurrent fevers or spreading cellulitis, or localized abscess formation, this constitutes a major infection. In the latter case, prompt expander removal is indicated, and the expanded flaps should be advanced concurrently so as not to lose the progress made during expansion. Serial expansion has been implicated in the development of infections, highlighting the importance of utilizing an aseptic technique for port access. 63 The most frequent minor complications include migration, port malfunction or access difficulty, and skin compromise without expander exposure. Minor complications may necessitate modification of the original reconstructive plan; however, they do not require immediate expander removal, nor should they preclude attainment of reconstructive goals.
For cosmetically challenging melanocytic nevi with malignant concern (ie, nevi that involve the eyebrows, eyelid margins, and nasal alae where complete excision is not possible without disfigurement of the structure), Fahradyan et al 68 demonstrated that leaving behind residual lesions on the face in lieu of a more optimal cosmetic outcome carries an acceptable loncologic risk. After an average follow-up of 5.6 years (average patient age of 9.6 years at final follow-up), melanoma was not discovered within the residual lesion on any patient (n = 32). 68 These findings support the overall consensus that malignant potential is often the least important principle guiding reconstruction, but rather esthetic outcome, quality of skin involved, and quality of life.
Facial resurfacing done in conjunction with removal of a giant melanocytic nevus varies with the anatomic subunits of the face that are involved, and how amenable this region is to expansion of adjacent tissues without distorting critical facial structures. For giant nevi involving the forehead, our current practice is to perform serial excision if the lesion involves <25% of the forehead, simultaneous expansion of the forehead as well as other affected areas if the lesion involves 25% to 70% of the forehead, or an expanded full thickness skin graft if >70% of the forehead is involved (Figure 4). Due to the risk of eyebrow ptosis following expanded forehead flap reconstruction (estimated incidence of 24% 59 ), our preference is to minimize excision of redundant skin when insetting the flap, allow for contraction of the remaining skin over time, and excise excess skin and correct ptosis after tissue contracture and scar maturation have progressed (at least 1 year post-operatively). 31

(Left) A 6-year-old boy presented with a giant congenital melanocytic nevus involving the forehead, the left side of the face, and half of the scalp. (Right) The scalp and face were resurfaced by expansion and advancement of adjacent tissues, and the forehead was resurfaced with an expanded full-thickness skin graft from the lower abdomen.
Outcomes
Quality of Life
Several studies have explored the subsequent improvement in quality of life following surgical treatment of giant congenital melanocytic nevi. Surgical excision has been shown to increase the quality of life as early as 6 months following the procedure, with male gender and age over 65 years being associated with the highest improvements. By 1 year, general positive emotions also increased among those that underwent surgery and the effect of gender was no longer present. 69
In children and adolescents, surgical treatment has especially been shown to increase quality of life because the population reports significantly lower baseline quality of life and higher emotional and behavioral problems when compared to those born without a giant congenital melanocytic nevus. 70 A worldwide analysis of 135 adolescent patients revealed the majority of adolescents self-reported their congenital nevus having a moderate to very large impact on their quality of life. Notably, the effect was more severe at older ages and if the nevus was in a visible location. 70 The highest drivers of these mental and behavioral health impairments were perceived stigmatization and low socioeconomic status. Partial surgical excision was not shown to be associated with higher quality of life, suggesting full removal with an esthetic focus is important in treating this population. 70
Post-Operative Surveillance
Following initial treatment, follow-up surveillance of the area may still be necessary due to potential malignant transformation. The literature reports a 0.6% risk of malignant melanoma development following full surgical excision of the nevus, suggesting a decreased need for surveillance compared to non-excisional treatment. 24 Further work is needed to identify appropriate surveillance following non-excisional treatment modalities.
Future Directions
Tissue expansion is an evolving treatment modality with many applications that warrants further research into the cellular mechanisms that govern this process. In a porcine model of tissue expansion that utilizes finite element analysis to predict stretch and growth of the skin, we demonstrated cellular proliferation peaks 3 days after expansion, and begins to translate into skin growth by day 7. 71 Using this model, we subsequently identified novel candidate genes that may play a pivotal role in stretch-induced skin growth, and may serve as future therapeutic targets to optimize this process. 72 Knowledge of the time required to reach optimal skin growth, as well as the biological processes involved, will assist surgeons to design a scientific-based schedule that reliably predicts growth rate and minimizes the often tedious and prolonged process of tissue expansion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.