
Abstract
Studies identifying TMJ synovitis biomarkers are few and far between. During the late 1990s, Chuck Milam’s oxidative stress and re-perfusion models elucidated the molecular mechanisms of TMJ synovitis which centrally involves the cytokines TNF-α, IL-1β, and IL-6. However, a new understanding of TMJ synovitis has been developed given the fields current knowledge on pattern recognition receptors (PRRs), damage-associated molecular patterns (DAMPs), pathogen-associated molecular patterns (PAMPs) and most notably, high mobility group box 1 (HMGB1). Among these molecular markers, the oxidation of HMGB1 plays a key role in promoting pathological inflammation. In this perspective, we explore the role of HMGB1 during TMJ synovitis and how a traumatized TMJ responds to different HMGB1 post translational modifications (PTMs). Specifically, synovial inflammation will be explored in the context of how different PTMs of HMGB1 directs leukocytes to produce chemokines or cytokines. We will also look at the different modifications of HMGB1 molecule via Reduction Oxygenation Reactions. These recently identified mechanisms provide a suitable addition to the currently understood molecular actions of TMJ synovitis noted by Milam and others in the late 1990s and early 2000s. We will then conclude with a discussion on the use of antibodies to the HMGB1 molecule for a variety of conditions: cancers, sepsis, liver disease, traumatic brain injuries and early intervention for joint synovitis along with the use of different delivery modalities.
Introduction
TMJ disorders affect more than 5% to 12% of adults in the USA and 40% globally. 1 Currently, there are some 30 known problems directly related to TMJ disorders and many more individual variations on these major problems. Patients with TMJ disorders can have facial pain and dysfunction during mandibular movement which can occur after acute or chronic TMJ damage. While acute TMJ damage can be easily identified and treated clinically, chronic TMJ damage is only apparent during later stages of disease development when treatment options become limited. 2 To diagnose the progression of chronic TMJ damage, physicians and researchers have placed attention on monitoring biomarker changes in the TMJ synovium. Although identifying early biomarkers in the TMJ is a well-established method to diagnose TMJ disorders, non-surgical treatment modalities and adherence to the mechanical theory of TMJ disorders have overshadowed procedures that involve isolating synovial biomarkers. 3 With acute damage, patients develop post traumatic osteoarthritis and even with surgical repair, signs of progressive joint damage remain evident. 4 Therefore, analyzing early biomarkers can assist in understanding the role of inflammation during the onsets of joint disease to allow for earlier clinical intervention.5,6
All TMJ disorders begin from a cause or etiology. The etiology can stem from trauma, the environment, mechanical issues, hormonal changes, neuropeptides, stress, anxiety, genetics, genetic changes, infections, malignant/benign tumors, and other biological issues. The flow from etiology to a problem, then to a disorder and finally to a specific disease pathology over time is known as the disease course or pathogenesis. 7 In the case of TMJ disorders, the first symptoms are noticed by the patient and can include pain in the TMJ area and jaw dysfunction. While pain experienced by a patient may be TMJ related, the pain could also stem from odontogenic, intracranial, and autoimmune disorders as well. All these potential problems need to be ruled out before diagnosing a patient with a TMJ disorder. Also, an etiology can be repetitive, severe, minor or a combination thereof, and other overlapping problems can further complicate specific TMJ issues which can include muscles and joint trauma, psychosocial issues, facial bone fractures, cysts, and others. Finally, comorbidities such as autoimmune issues, allergies and genetic issues can concomitantly occur with TMJ disorders and complicate a clinician’s ability to reach the correct diagnosis. 8 To better determine whether jaw pain arises from TMJ synovitis, inflammation of the joint complex or intraarticular area is uniquely evident to this disorder. 9 This occurs secondary to early changes in the synovium and if left untreated, synovitis will progress into osteoarthritis. 10 With synovitis, the synovial fluid has high concentrations of TNFα, IL-1β, and IL-6. 11 However, in recent years, another key cytokine called high mobility group box 1 (HMGB1) has been found in patients with septic shock in very large quantities thereby producing a “cytokine storm.” 12 Therefore, examination of this molecule is warranted to find its connection to TMJ synovitis. Along with relating synovitis to intraarticular TMJ disorders, this perspective will look at what causes TMJ synovitis, and the role synovitis plays in initiating joint pathology. In addition, we outline forefront research identifying significant cytokines that are involved with the inflammatory process leading to intraarticular TMJ disorders.
Synovitis
The synovial membrane (synovium) is a specialized connective tissue that lines and surrounds diarthrodial joints. The synovium isolates the synovial cavity from surrounding tissues and is responsible for maintaining synovial fluid volume and composition by producing a lubricating fluid of lubricin and hyaluronic acid. Through this synovial fluid the joint meniscus, chondrocytes and subchondral bone receive nutrition. 13 The synovium is also composed of synovial-type cells called fibroblast-like synoviocytes (FLS), and macrophage-like synoviocytes (MLS). The synovium and synovial cells are present in all synovial joints of the body. With time and other intervening etiologies, inflammation is a problem inside any joint, but early diarthrodial joint inflammation at early stages is known as synovitis. Patients with synovitis have increased pain, heat, redness, edema, and a loss of joint function. 14 At the cellular level, TMJ synovitis causes FLS that are normally greater than MLS to reverse in number. 15 There is additional chemotactic activity with innate immune cells to increase the fluid content of the affected area. If one examines the synovial fluid content of the TMJ during synovitis, one finds various upregulated cytokines including TNFα, IL-1β, and IL-6. 59 If left untreated, continued TMJ synovitis progression can damage the joint at the molecular, cellular and tissue level (Figure 1).
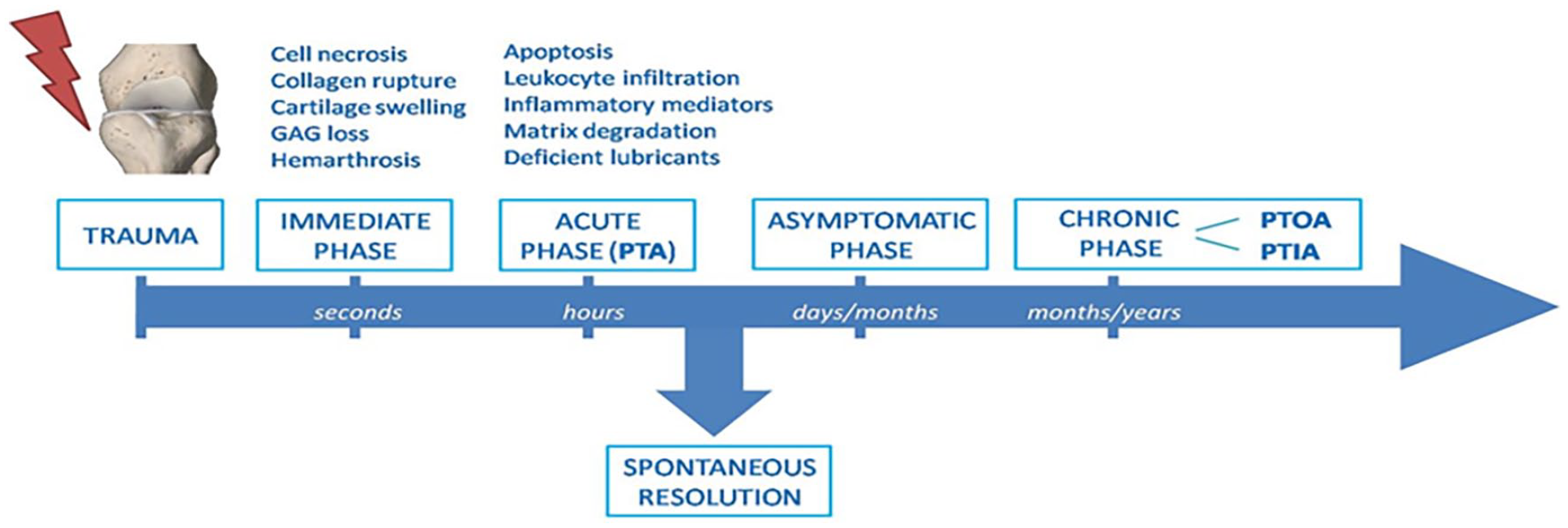
The progression from trauma on the right to the end stage disease of osteoarthritis involving the cartilage and bone proper and the molecular and clinical events that occur. 16
Diagnosing Synovitis
The signs of TMJ synovitis can easily be detected on a clinical level by the patient and the practitioner. 8 A clinical examination with TMJ palpitation and the surrounding area can be performed. Additionally, any restriction of motion can be noted due to the pain. This information can be noted and documented to show the severity of the discomfort: for example, a mild, moderate, and severe pain range (Level 1, 2, and 3). 17 Additional studies including radiographs, MRIs, blood work, etc. can be performed to further document the specifics of synovitis.
Intraarticular TMJ disorders can be imaged under MRI which has now become the gold standard imaging modality for identifying soft tissue injuries, disc abnormalities, inflammation, and synovitis. It has been noted by Schellhas that effusions can be found in the early stages of TMJ disorders using MRIs and that González et al found a 100% correlation of effusion with synovitis in Wilkes Stage IV and V.18-20 Also, gadolinium can be used with MRIs to enhance image contrast to show inflammation in the TMJ and osteomyelitis. 21 Additionally, the diagnosis of synovitis can be obtained via arthroscopic visualization, biopsy techniques and histological examination of the synovial tissue. This microscopic examination can identify the specific type of synovitis as well as its severity grade. 22 As with all potential diagnoses, a complete and comprehensive evaluation and examination of the TMJ, head and neck areas following the ENT Medicare version is mandatory. Also, we need to include routine quality radiographs of the head and neck to include the condyle of the mandible. 8 This comprehensive head and neck evaluation and examination should follow the biopsychosocial medical model by Engel, the Axis II evaluation, and the clusters of Maixner et al.23,24 As with diagnosis, it is imperative to note any areas of other overlapping problems and comorbidities. 8
High Mobility Group Box 1 (HMGB1)
HMGB1, discovered in 1973, is an ancient non-histone nuclear protein and the second most numerous protein next to nuclear histones. 25 The name is derived from the high electrophoretic mobility of this protein in polyacrylamide gels. HMGB1 is found in all eukaryotic cells and platelets. The HMGB1 gene is located on Chromosome 13q12 and includes 5 exons and 4 introns. The molecule contains 215 amino acids and has a molecular weight of about 30 kilodaltons. HMGB1 mainly resides in the cell nucleus where it performs transcription regulation, DNA replication and repair, telomere maintenance and nucleosome assembly. HMGB1 is tightly bound to its nuclear home but can be released into the cytoplasm or extracellular fluid (ECF). 26 Human and rodent HMGB1 have a 99% protein identification with each other, and this bodes well for experimental analysis using small animals. 27 Notably, HMGB1 is plentiful in cells containing 106 HMGB1 molecules per cell. 28 The HMGB1 molecule includes several Cysteine (Cys) members which are active (Cys 23, 45, and 106). The reversible oxidation of these cysteine residues can occur naturally and can also increase during oxidative stress as with inflammation, trauma, and other disease states. These oxidative changes can affect the formation of disulfide bonds, folding of the protein molecule, stability, and function. 29
The HMGB1 molecule also contains many other potential active amino acid residues (Lysine, Methionine and Tyrosine) with the potential for Post Translational Modification (PTM) of these residues by reactive oxygen species (REDOX).
When pathogens are introduced into the body, they are confronted by the innate immune system, and this is started by the recognition of pathogen associated molecular patterns (PAMPs) mainly by macrophages via transmembrane pattern recognition receptors (PRRs). It is by these PRRs that pathogens or parts of lipopolysaccharides (LPS) promote antibody production. However, this process could not explain the strong innate immune response found in sterile conditions which come from ischemic injuries, trauma, tumors, tissue transplantation and autoimmune diseases. 30 In 1994, Matzinger. proposed a “danger theory” that states: some particles have a full-time job when intracellular/nuclear but when released into the extracellular matrix via trauma, etc. they then signed on for an additional job as a damage-associated molecular patterns (DAMPs). DAMPs hook up with PRRs like PAMPs and start the innate immune system. DAMPs are the missing link for initiating sterile inflammation. 31 HMGB1 is a specific DAMP that has been shown to participate in the inflammatory process and is by itself a powerful mediator of inflammation. 32
HMGB1 is divided into 3 basic structures which include an A-Box (9-79 amino acids); a B-Box (89-162 amino acids) and an Acidic C-terminus tail (186-215 amino acids). There are several active amino acid sites located in the A-Box at cysteine-23 and cysteine-45 and in the B-Box at cysteine-106. 33 Oxidization of these cysteines to different sulfur bonds will determine the action or inaction of the HMGB1 molecule in inflammation. But first the HMGB1 molecule needs to be freed from the nucleus of the cell. This occurs via A-Box acetylation of the amino acid lysine (28-44 NLS1) and in the B-Box (179-185 NLS2). As noted, this action occurs in the nucleus and this HMGB1-acetylation molecule now becomes ready for transport out of the nucleus and into the cytoplasm (Figure 2).34,35
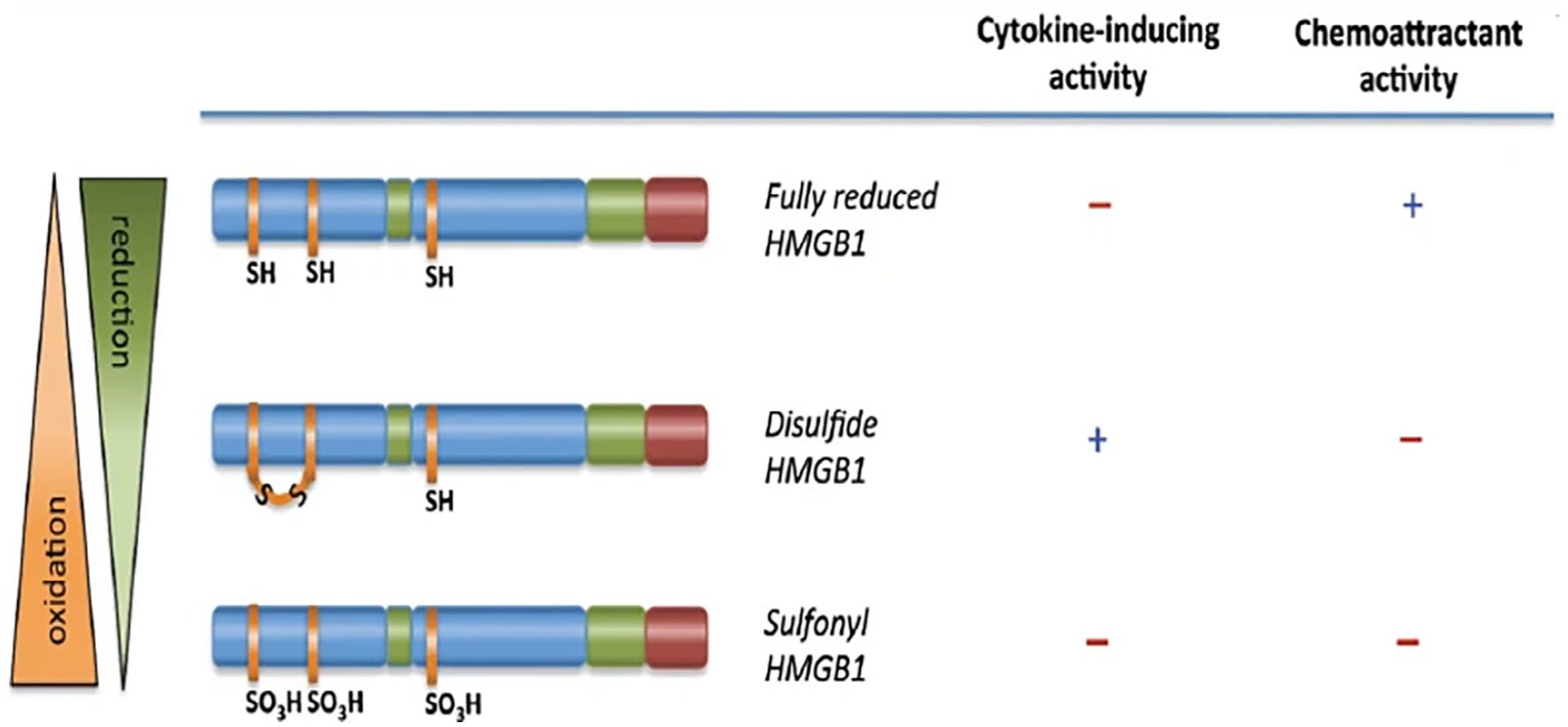
Molecules are reduced by the lack of oxygen into the molecules at cisteine-23, -45, and -106 and continues downward to full oxygenation with all these have SO3H attachments. The final stage where the molecules cannot attach to ta PPR and hence become inactive so healing and resolution of inflammation can occur. 36
The actions of HMGB1 producing inflammation occur in the extracellular fluid. 37 The release of HMGB1 from the cytoplasm and into the extracellular fluid can occur by several mechanisms. These mechanisms include active passage through nuclear membrane pores, acetylation, nuclear localization signals (NLS) 1 (28-44 with 4 lysine sites) and 2 (179-185 with 5 lysine sites), lysosome inclusion and transportation, and indirect release from the cytoplasm by Gasdermin D. Acetylation untangles HMGB-1 from the nuclear chromatin and allows acetylated HMGB1 (HMGB1-acet) to enter the cytoplasm of the cell and join a lysosome. The HMGB1-acet will then act as a signal to be picked up by PRRs on cell membranes of monocytes and macrophages. 38 Along with promoting inflammation, HMGB1 alone can stimulate inflammation by producing cytokines and chemokines. 39 Both nuclear and cytoplasmic HMGB1 are in a fully reduced state in the 3 noted active Cysteines (Cys-23, Cys-45, and Cys-106) and have a terminal -SH configuration. Exposure to the new environment of the extracellular fluid and ROS can modify HMGB1 and allow it to attach to a leukocyte PRR. This action will then continue the inflammatory pathway (Figure 3).
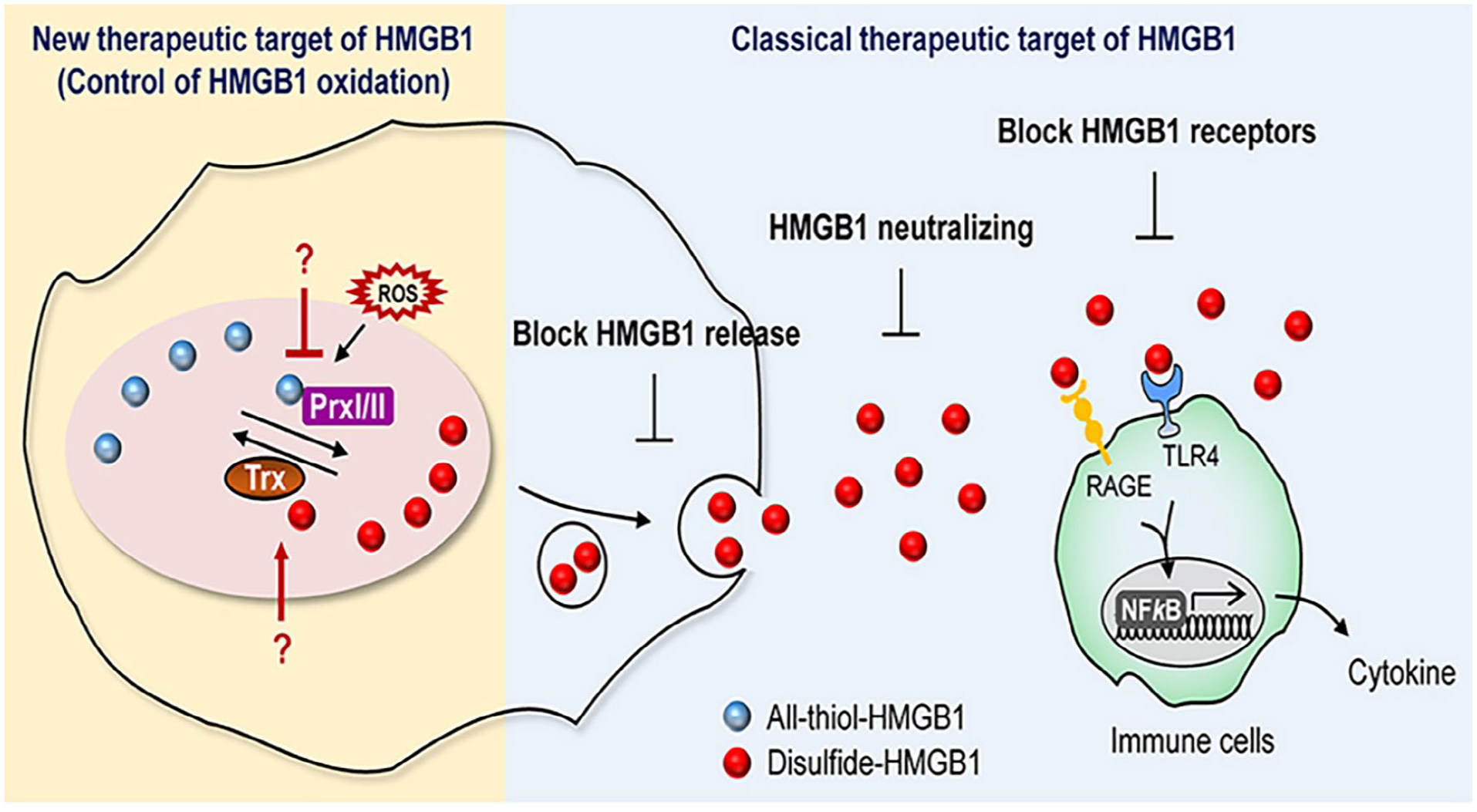
Acetylation of HMGB1 intranuclear, a mechanism of release into the cytoplasm and a mechanism for release into the extracellular fluid (ECF) and then migrating to an immune cell for PPR attachment and for the continued progression inside the immune cell for production of cytokines and chemokines. 40
If TMJ synovitis is left untreated, it will progress to increased DAMP and subsequent cytokine production via PRRs such as RAGE, TLR 2, and TLR 4. 41 Initially, the exit of HMGB1 from the cytoplasm occurs in a fully reduced state into the extracellular fluid. The fully reduced HMGB1 will continue as a pathway for CXCL12 binding to form a heterocomplex. This heterocomplex attaches to a PRR named CXCR4 which then functions by increasing chemokines, chemotaxis, and cell migration.
These PRRs link up with HMGB1 and work intracellularly with a cascade of downstream molecules starting with Myeloid Differentiation First Response 88 (MyD88) which is a cytoplasmic protein that joins with a PRR when a signal from an outside protein is present. MyD88 acts as a relay to join other molecules to join with IL-1 Receptor-Associated Protein Kinase (IRAk) which in turn activates Nuclear Factor kappa Beta (NFкB) to regulate cell fate, advance the immune response, and produce an inflammatory reaction. 42 PRRs like Receptor for Advanced Glycation of End-products (RAGE) as well as Toll Like Receptors 2 and 4 (TLR-2, TLR-4) located on the B box of HMGB1, have specific binding sites on the HMGB1 molecule. The RAGE binding sites are noted on amino acids 150-183 and the TLR-4 binding sites are noted on amino acids 89-108.43-45 Rage binding of the HMGB1 molecule occurs with the fully reduced HMGB1 molecule. As noted above, the fully reduced HMGB1 molecule can form a heterocomplex with the chemokine CXCL12 (which is always present in the ECF), and this complex of HMGB1 and CXCL12 through the PRR CXCL4 and NFkB continues to feed the inflammatory process as well as increases the presence of ROS. 46 These secondary mechanisms involving PRRs and CXCL12/CXCR4 are responsible for increased HMGB1 output by a positive feedback loop. 2 The process of the inflammatory reaction occurs through the process of reduction by oxidation in the extracellular space. 45
As a result, HMGB1 is converted at Cys-23 and Cys-45 to a disulfide bonded HMGB1 which causes an increased inflammatory response. This increase in the inflammatory response occurs when the disulfide bonded HMGB1 molecule binds with macrophage and monocyte PRRs such as TLR4-MD-2 to produce pro-inflammatory cytokines (TNF-α, ILβ-1, and IL-6). Consequently, HMGB1 sustains a long-term state of inflammation with increased stress (Figure 4). 39
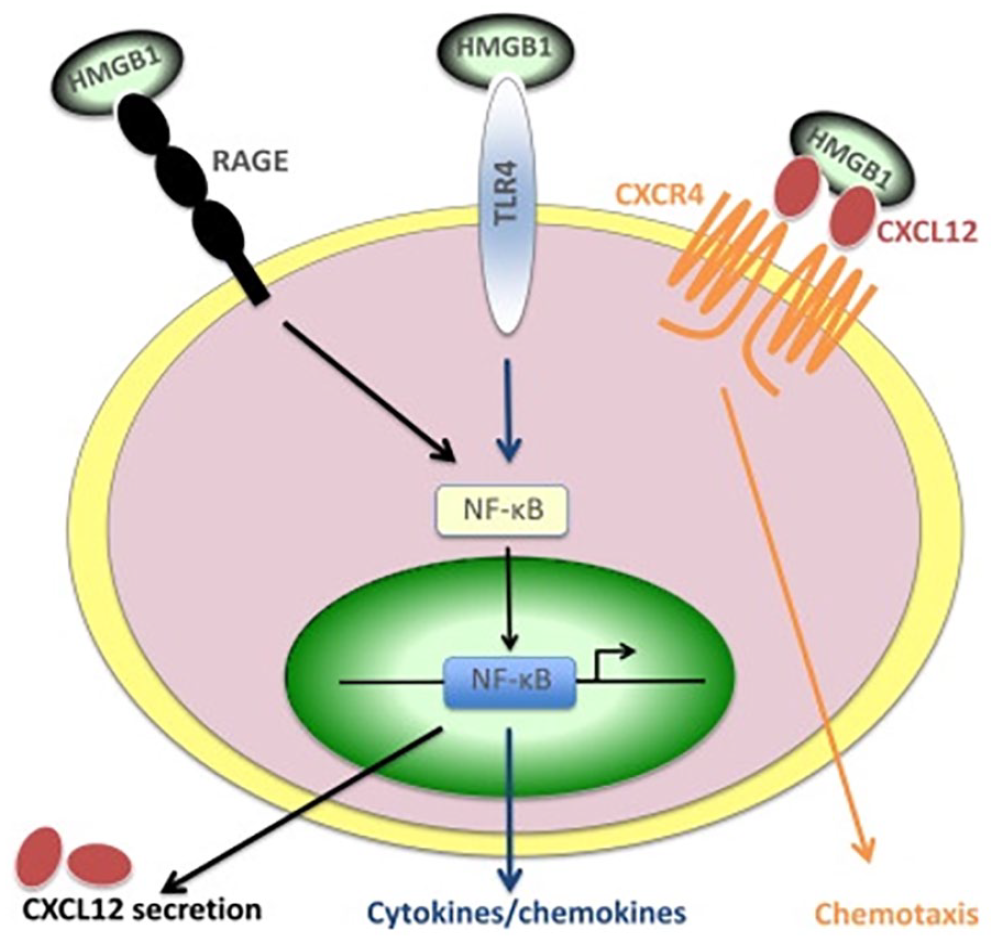
Proteins and receptors involved in HMGB1-induced leukocyte migration and activation. HMGB1 binds to CXCL12 and the heterocomplex activates CXCR4 and induces cell migration. HMGB1 as a disulfur at C-23 and C-45 alone binds TLR4/MD-2 and HMGB1 as fully reduced at C-23, C-45 and C-106 binds to RAGE. Both TLR4 and RAGE ligation lead to the activation of NF-B and the transcription of cytokine and chemokine genes. In particular, CXCL12 secretion depends on RAGE activation. 47
Over time, a reduction-oxygenation reaction favors an oxidize versus reduced forms of HMGB1. The cysteine areas of Cys-23, Cys-45, and Cys-106 form sulfonates (SHO3) which prevents oxidized HMGB1 from attaching to PRRs of RAGE and TLR4, as well as form a hetero complex with CLCX12 to bond with the PRR CLCR4. 48 Thus, HMGB1 oxidation stops the production of cytokines, chemokines and chemotaxis. This effectively ends the inflammatory cycle and sets the tissue area up for healing and repair by promoting angiogenesis and mesenchymal stem cell recruitment. So, we note that while HMGB1 is by itself a pro-inflammatory molecule, the oxidized form of HMGB1 will act as a healing and repair molecule via reduction by oxygenation at the HMGB1 cysteine sites Cys-23, Cys-45, and Cys-106. This pro and anti-inflammatory process will be related to the type of insult and the severity of the insult.49,50 However, other factors such as necrosis, apoptosis, autophagy, and phagocytosis which also promote TMJ inflammation, can significantly change the pathology of TMJ synovitis (Figure 5).
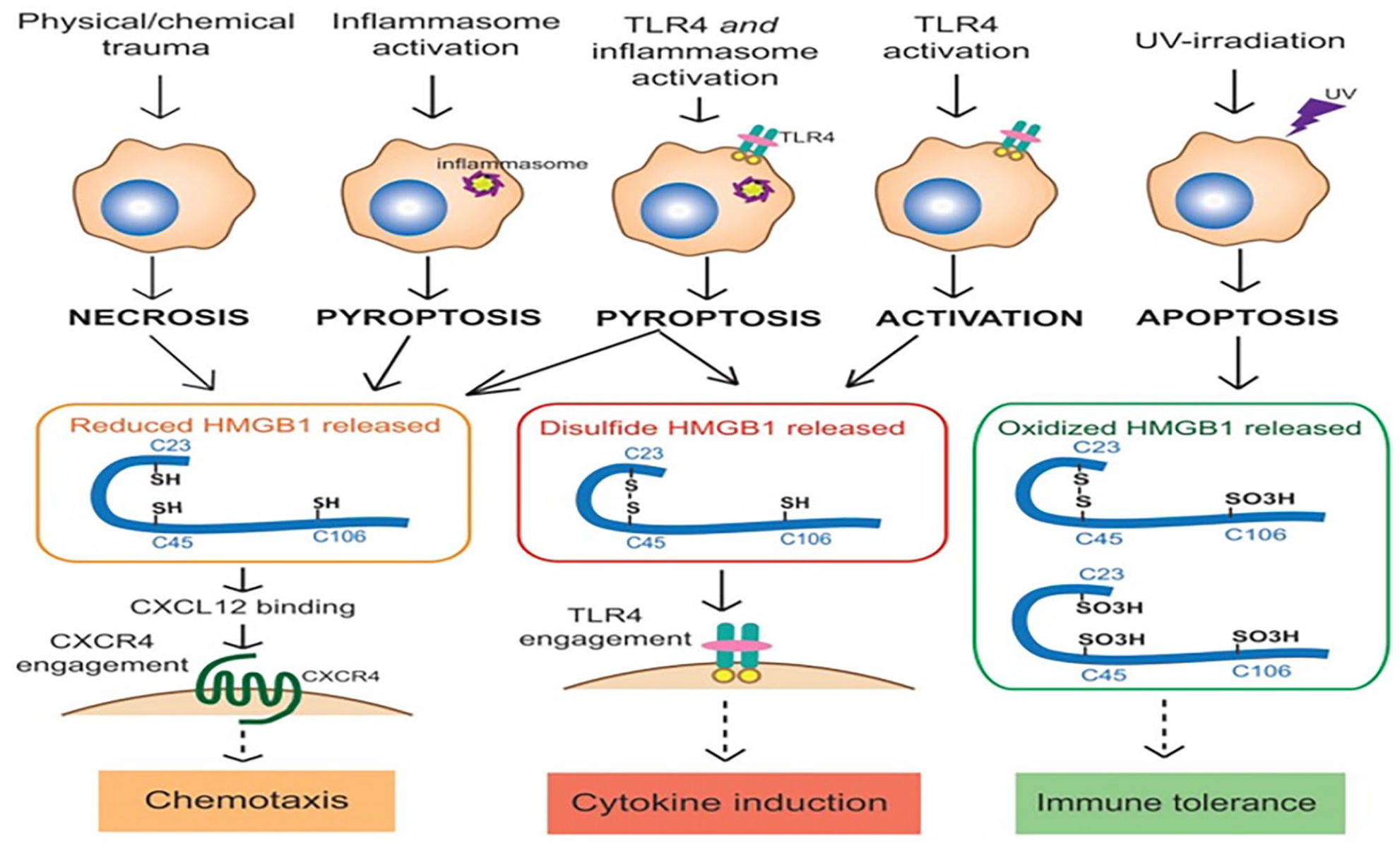
The relationship between HMGB1 release mechanism and HMGB1 isoforms. As this figure illustrates, the various release mechanisms (necrosis, pyroptosis, macrophage activation and apoptosis) can lead to the release of different redox forms of HMGB1.
As noted earlier, most TMJ synovitis is traumatic in nature and the HMGB1 molecule should be an isoform of the PTM. Finding that information out in a short time frame would be a great asset and could require the simple removal of synovial fluid from the TMJ.
There are limited methods for assaying HMGB1 which include western blotting and ELISA. Both methods require a great amount of time and are relatively expensive. The western blotting is not quantitative and hence the preferred test is the ELISA. The ELISA test can average 90 minutes to overnight depending on the sensitivity desired. Therefore, providing alternative methods for rapid HMGB1 detection in any isoform are needed for a rapid diagnostic result with low cost. 51
Summary and Future Perspectives
For practitioners to better aid in ameliorating disease progression, it is important to know when disease progression starts and stops. There may also be combinations of sterile and pathogen-based inflammation which can complicate the treatment regimens administered. Finding anti-HMGB1 antibodies and knowing how, when, and how much to deliver will assist in decreasing the pro-inflammatory process thus increasing patient healing. Thus far, anti-HMGB1 therapies have proven to ameliorate inflammation not only with orthopedic conditions, but also during hemorrhagic shock, massive blunt force trauma and airway inflammation. Anti-HMGB1 antibodies could also be used prophylactically to decrease the inflammatory response to other types of surgical interventions of the TMJ. More recently, glycyrrhizin, a direct HMGB-1 inhibitor used mostly for chronic hepatitis treatment, has been used to regulate TMJOA progression in rats. 5 Specific biomarkers can be noted in the variety of pathologies involving HMGB1 that produce inflammation. It has been shown that PTMs can occur on amino acid residues (termed Proteoforms) and theoretically, there can be thousands of Redox change combinations to the HMGB1 molecule. Finding the correct biomarker for a specific disease can be daunting. However, as TMJ disorders involving traumatic synovitis are usually promoted by sterile inflammation, the biomarkers identified should be similar.52,53
As targeted biologics, such as anti-HMGB1-mc/pc AB, are being developed to antagonize the actions of proinflammatory cytokines, there is a need to improve these compounds’ pharmacokinetics and half-life. To this end, a myriad of drug delivery vehicles are being developed to circumvent the harsh environment that exists in the oral facial area for biotherapeutics. For instance, poly (lactic-co-glycolic) acid, lipid, poloxamer, chitosan-based particles, microneedles, and exosomes have been developed to deliver active molecules that are known to downregulate inflammatory cytokines for a prolonged period.54-59 Although these systems do not specifically deliver anti-HMGB1, more studies exploring anti-HMGB1 loaded drug delivery systems may be coming soon. 60
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Institutional Review Board approval was not required
Informed Consent
Informed Consent was not required for this article