
Abstract
The diagnosis of CRMO of the craniomaxillofacial skeleton is often delayed due to shared clinical features with a range of alternate diagnoses. We present our recent CRMO case series and resulting review of the literature in an effort to re-emphasize CRMO to surgical providers as a diagnostic consideration in inflammatory pathologies of the craniomaxillofacial skeleton. The series elucidates the diagnostic criteria, work-up, and management of this pathology to promote more efficient multidisciplinary communication and coordination highlighting that earlier treatment portends a more favorable prognosis.
Keywords
Introduction
Chronic recurrent multifocal osteomyelitis (CRMO) is an inflammatory disorder associated with skeletal manifestations during childhood. The diagnosis of CRMO is often delayed due to shared clinical features with alternate diagnoses inclusive of malignant and non-malignant bone tumors, infectious osteomyelitis, hematological diseases, metabolic diseases, and other auto-inflammatory causes. 1 Arriving at the correct diagnosis early is crucial since the management for CRMO is different from the differential diagnoses mentioned above. Patients may be subjected to unnecessary antibiotics or even surgery when medical management alone is generally sufficient for CRMO.2,3 Furthermore, the diagnostic delay may lead to progression of the disease before appropriate treatment can be initiated.
In an effort to re-emphasize CRMO to surgical providers as a diagnostic consideration in inflammatory pathologies of the craniomaxillofacial skeleton, we present three cases of pediatric CRMO. We review the current literature highlighting the diagnostic criteria, work-up, and management of this pathology to promote more facile multidisciplinary communication and coordination between craniofacial surgical services, internal medicine, radiology, and rheumatology for appropriate treatment and care.
Case Studies
Case Report 1
A 5-year-old female presented to our department with recurrent swelling and pain in her right jaw after a tooth extraction 2 months prior. No constitutional symptoms were endorsed, and a review of systems was otherwise benign. Physical exam was significant for mild trismus and large firm nonerythematous mass of the right mandible that was tender to touch. There was no evidence of palpable lymphadenopathy in the head or neck.
Computer tomography (CT) scan demonstrated extensive right mandibular subperiosteal new bone, sclerosis, and cortical destruction (Figure 1a). There was cortical destruction at the lateral aspect of the mandibular ramus. There was apparent extraosseous soft tissue thickening in the right masseter muscle. The differential included chronic osteomyelitis or bone-borne craniofacial neoplasm. Magnetic resonance imaging (MRI) was recommended for further evaluation.
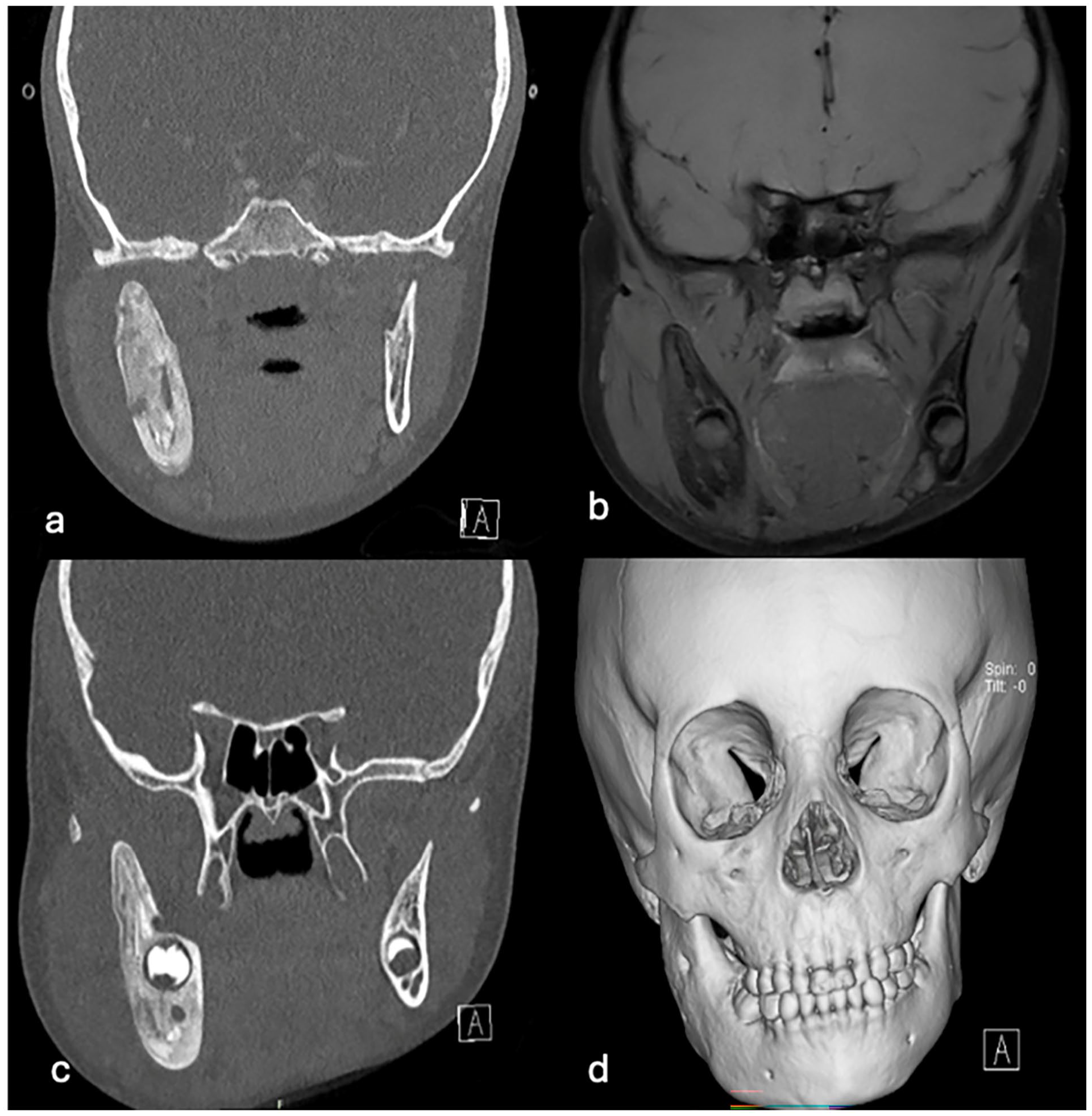
Case 1—Right Mandibular CRMO (a) Initial CT demonstrating right ramal proximal body mandibular lesion. (b) Initial MRI demonstrating right ramal proximal body mandibular lesion. (c) Repeat CT taken 9 weeks later showing persistent mandibular lesion despite antibiotic therapy. (d) Repeat CT taken 17 weeks from initial presentation, persistent lesion at the time of formal CRMO diagnosis prior to initiation of therapy.
MRI demonstrated an abnormally thickened right mandibular ramus with a benign periosteal reaction, supporting chronic osteomyelitis from the CT findings (Figure 1b). Surrounding soft tissues of the ramus were swollen, the parotid gland was displaced, but there was no evidence of diffusion restriction or enhancing fluid collection. Paranasal sinuses had mild mucoperiosteal thickening. No focal abscesses were appreciated. Following the MRI, diagnosis of a neoplasm was thought to be less likely, and osteomyelitis remained the highest in the differential.
Patient subsequently underwent an intraoral biopsy of the right mandible lesion, which exhibited marrow fibrosis and periosteal reaction with woven bone formation. Cytology was consistent with scattered plasma cells with a rare CD138+ immunohistochemistry. Systemic labs suggested acute inflammation, with erythrocyte sedimentation rate (ESR) of 38 mm/hour (normal 0–20 mm/hour) and C-reactive protein (CRP) of 3.1 mg/dl (normal < 1.0 mg/dl). After the biopsy, her culture grew MSSA and Strep anginosis (a rare Strep viridans), leading to the diagnosis of chronic osteomyelitis secondary to multiple dental procedures. Patient was discharged with prescription of 3 months amoxicillin and clavulanic acid 400 mg/5 ml 800 mg BID.
Nine weeks later, the patient returned to the emergency department (ED) with recurrent swelling and pain on her right jaw. Over the interval, the patient noted improvement in pain symptoms without resolution of facial swelling. The patient was compliant with the regimen, except for a period of 5 days in which the caregiver reports a dosing error (dose decreased by 50%) following an error during a refill. Despite dose correction, the patient continued to experience further jaw swelling and complained of mild trismus.
A repeat CT scan again showed right mandibular expansion, subperiosteal new bone and sclerosis as the previous imaging with no sign radiologic improvement. Instead, there was a progression of new periosteal bone on internal areas of lucency (Figure 1c). Cortical destruction of buccal aspect of the ramus was more prominent than the previous imaging. There was a new, small lesion on the lingual aspect of the angle and coronoid process. Concurrently, her ESR had risen to 81 mm/hour and CRP to 5.3 mg/dl.
The patient subsequently underwent repeat intraoral bone biopsy. The pathology reported marrow fibrosis and scant chronic inflammation, with no signs of acute osteomyelitis. Following multidisciplinary discussion with infectious disease, despite the lack of definitive osteomyelitis on histopathologic assessment, the patient was dose-escalated and continued amoxicillin and clavulanic acid. Consequently, the patient had significant decrease in her swelling and improvement in pain on amoxicillin and clavulanic acid at 4-week follow-up. Given the clinical progress, antibiotics were continued with plan for close interval multidisciplinary follow-up every 4 weeks.
After 8 weeks of antibiotics, a CT scan was repeated. Despite improvement in clinical soft tissue edema, the CT illustrated persistent periosteal bone formation, sclerosis, intercortical focal lucencies, and discrete areas of cortical destruction of the mandibular ramus (Figure 1d). Given the clinical progress in swelling, infectious disease services planned to complete a total of 3 months of antibiotics. Three weeks later the patient again developed perimandibular swelling with elevation in inflammatory markers (ESR was 59 mm/hour and CRP was 2.7 mg/dl). Given the persistence of pathology, infectious disease recommended repeat operative biopsy with plan for specialty broad spectrum high-sensitivity PCR analysis through the University of Washington due to continued uncertainty of the causative pathogen.
Intraoperatively, the surgeon again noted evidence of high bone turnover with bicortical sclerosis and intracortical bone of soft, highly-vascularized, inflammatory turgor. As noted, specimen was sent for broad range PCR. Pathology again reported marrow fibrosis with focal mild chronic inflammation and rare plasma cells on the right mandible, without any acute inflammatory infiltrates.
At this stage, the multidisciplinary team was broadened to include rheumatology services, and a diagnosis of CRMO was entertained given the persistence of inflammatory bone pathology without clinical and radiographic resolution despite an appropriate treatment course for presumed chronic osteomyelitis. The PCR microbiology array failed to suggest a causative organism.
Rheumatologic work-up included inflammatory indices (Table 1) and a whole-body MRI to assess for multifocality. When indices did not suggest other specific osseous inflammatory disorder a diagnosis, indomethacin was initiated. MRI revealed pathology at the right mandible and focal edema in right calcaneus. The patient eventually matriculated to methotrexate then adalimumab treatment regimens until the pathology was stabilized.
Rheumatologic Serum Diagnostics: CRMO Work-Up.
Case Report 2
A 10-year-old female presented to the emergency department with a painless swelling of the right midface. The only antecedent event was recent loss of a deciduous tooth. Patient’s caregiver denied constitutional symptoms. Physical exam was significant for right midface and periorbital swelling. There was no evidence of palpable lymphadenopathy in the head or neck.
Cross-sectional imaging was obtained with findings demonstrating mild expansile ground glass attenuation and erosive changes of the right maxilla, anterior zygoma, and right lateral orbital wall. There was an adjacent soft tissue swelling and myositis of the right masseter muscle with periosteal new bone formation along the right lateral mandibular ramus and condyle (Figure 2a). Right dacryoadenitis and parotitis were present. Periodontal/endodontal disease of the first and second maxillary molars with associated erosive changes of the alveolus was also noted.
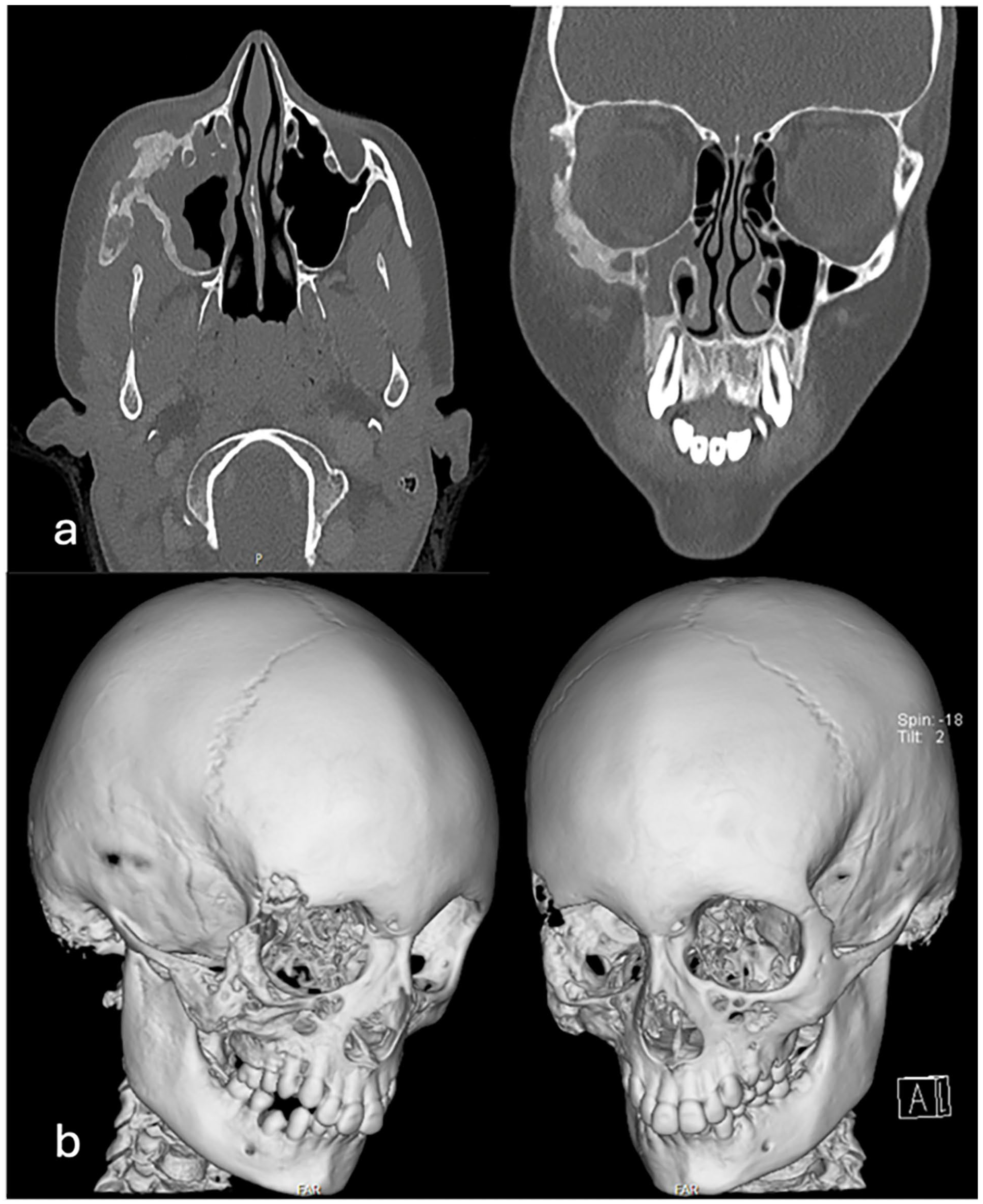
Case 2—Right Midface CRMO (a) Representative CT axial and coronal images of right midface lesion. (b) Representative 3D reconstructed CT right midface lesion.
Clinical and imaging presentations led to a recommendation of intraoral biopsy. Intraoperatively, the surgeon noted expected mixed dentition without gingival pathology. The maxillary bone appeared to be thickened with evidence of cortical sclerosis, however, was without significant contour irregularity. On bone biopsy, the subcortical bone manifested a softer, high turnover type of gross clinical bone pathology. The intraoperative impression heralded a differential including osteomyelitis and fibrous dysplasia. Pathology suggested subacute osteomyelitis of the right maxillary bone, and microbiological assessment yielded gram-negative diplococcus suspicious of Neisseria species, which was more consistent with subacute osteomyelitis. The infectious insult was attributed to a recent dental cleaning in the setting of periodontal/endodontal disease. The patient was started on trimethoprim and sulfamethoxazole with quick transition to amoxicillin and clavulanic acid and plans to follow up with ID. Inflammatory labs were not elevated.
Six weeks onward, the patient’s right maxillary swelling persisted along with complaint of intermittent blurry vision. A CT was repeated with findings characterized by expansile ground glass attenuation but now with progression of erosive/lytic changes of the right maxilla, anterior zygoma, right lateral orbital wall and superior orbital rim (Figure 2b). There was new periosteal bone formation along the right lateral orbit and anterior maxillary sinus wall. There was an increased associated facial soft tissue swelling, with increased extension into the right extraconal orbit. CT also demonstrated progressive myositis of the right masseter muscle with periosteal new bone formation along the right lateral mandibular ramus and condyle and persistent right dacryoadenitis and parotitis.
It was the opinion of infectious disease that the patient has adequately completed her course of antibiotics for a considered diagnosis of bacterial osteomyelitis, sinusitis, and odontogenic infection. The lack of clinical improvement suggested the lesions may not be indicative of an infectious process and repeat biopsy was recommended. Intraoperatively, the surgeon noted progression of bony changes in her right maxilla. Compared to her previous gross findings, the buccal cortex was progressively to osteolytic and soft, with lytic bony changes over the maxillary sinus. Microbiologic specimen was collected from bone and maxillary sinus. Gross bone biopsy was sent to pathology. Immunohistochemistry for IGG/IGG4 was ordered. There was minimal staining with either antibody. Only sparse IGG and IGG4 plasma cells are identified in most fields. In one focus where there was a mild but more prominent lymphoplasmacytic infiltrate, there were around 50 plasma cells with 10 staining for IGG4 (20%). The pathology report finally concluded chronic inflammation and reactive bone formation on maxilla secondary to acute and chronic sinusitis from the microbiology. Inflammatory labs were not elevated.
Given the persistence of a high turnover boney inflammatory process, the lack of clinical improvement with antibiotics and a diagnostically indeterminate pathologic assessment, multidisciplinary discussions with infectious diseases, rheumatology, craniofacial surgery entertained the diagnosis of an atypical presentation of CRMO. Full body MRI and skeletal survey failed to elucidate any multifocality to the pathology. The patient was started on indomethacin and then transitioned to immunomodulation with adalimumab. In rheumatologic follow-up, significant resolution of clinical soft tissue swelling, parotitis, and dacryoadenitis has been noted.
Case Report 3
A 9-year-old male presented with recurrent swelling and pain in his right jaw which began 2 years prior. The caregiver denied constitutional symptoms and associated clinical signs and symptoms. Private dental evaluation was reported to be without evidence of pathology. Over the 2 years the patient was followed by general pediatrics in the outpatient setting, both antibiotics and steroids were prescribed at several intervals. No response was seen with antibiotics and swelling would quickly improve with steroid administration. Without intervention, the swelling generally regressed on its own within a few weeks. Due to the discomfort, the patient became a chronic user of NSAIDs. Family history was significant for first- and second-degree relatives with diagnoses of inflammatory bowel disease. On presentation to the ED, physical exam was significant for trismus, tenderness, and swelling at the angle of the right jaw. There was no gingival or dental pathology. There was no evidence of palpable lymphadenopathy in the head or neck. Inflammatory markers were largely unremarkable (ESR was 17 mm/hour, CRP was 1.1 mg/dl), and HLA-B27 antigen testing was negative.
Cross-sectional imaging was completed. CT showed asymmetric thickening, areas of sclerosis, and lucency on the right mandible with evidence of periosteal reaction (Figure 3a). There was concurrent right masseteric myositis. The diagnosis was suggestive of subacute/chronic osteomyelitis.
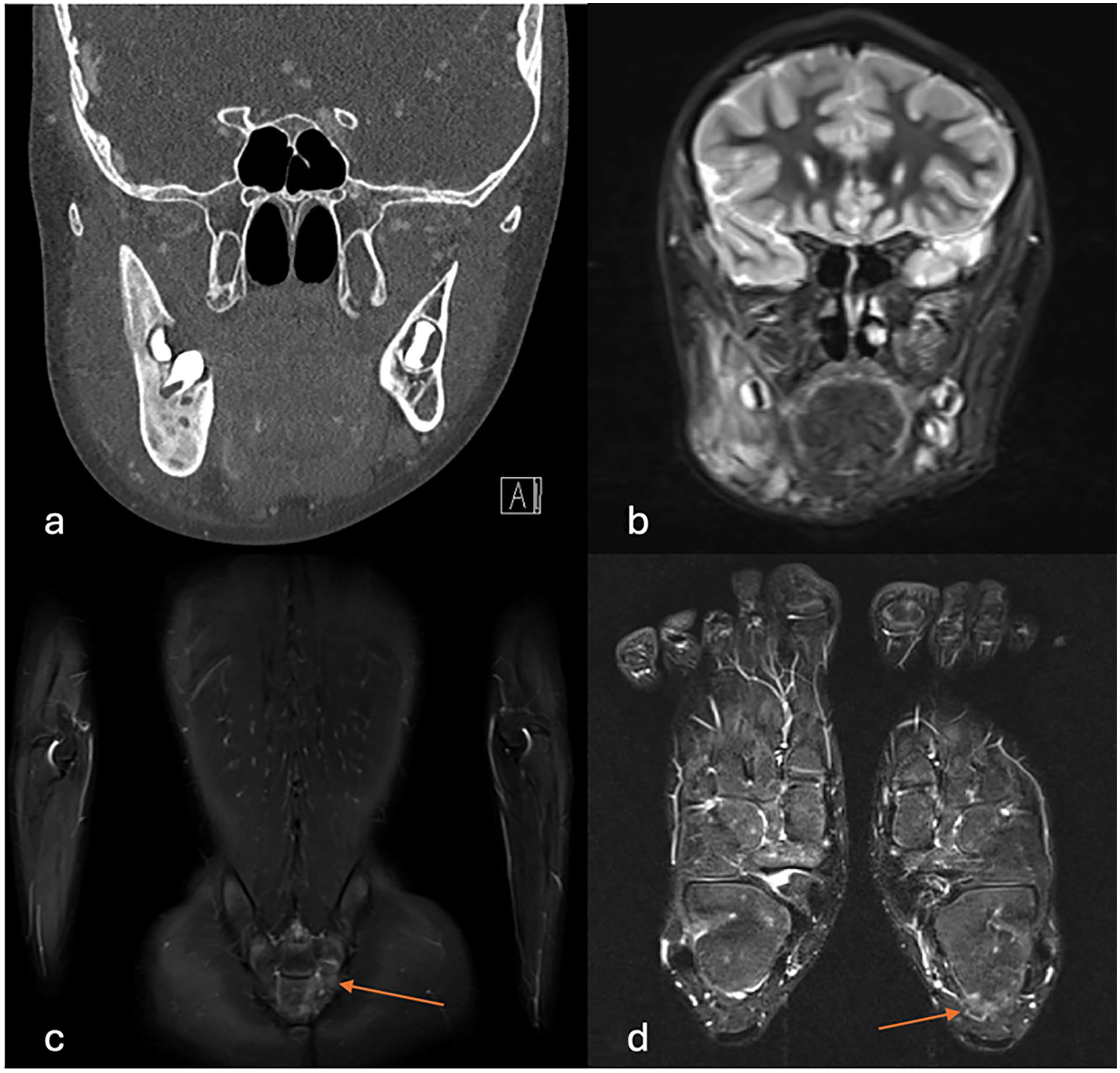
Case 3—Right Mandibular CRMO with Multifocality (a) Representative CT coronal image of right mandibular lesion. (b) Representative T2 MRI of right mandibular lesion. (c) Representative T2 MRI of left sacral lesion illustrating multifocality. (d) Representative T2 MRI of left calcaneal lesion illustrating multifocality.
MRI scan demonstrated abnormal marrow signal involving the right mandible extending from the mandibular condyle to midline (Figure 3b). There was overlying soft tissue and intramuscular edema. The report also showed mild asymmetric T2 signal from left sacrum and focal abnormal signal from the left calcaneus (Figure 3c and d). The radiologic impression was multifocal osteitis and consequently, a diagnosis of CRMO was entertained. Intraoral biopsy was recommended.
Upon biopsy, the surgeon reported mild edema of the masseter with mandibular cortical sclerosis without other notable dental or boney pathology. Both were biopsied and sent for culture and pathology. The mandible showed focal abscess indicative of acute and chronic osteomyelitis, and the masseter biopsy yielded no significant results. The culture was negative for any organisms. A formal diagnosis of CRMO was made, and the patient was referred to rheumatology and started on indomethacin.
Discussion
CRMO is an autoimmune disease rising from an imbalance between pro- and anti-inflammatory signaling molecules. Interleukins 9, 10, 18, and 19 are responsible for anti-inflammatory effects, regulating the pro-inflammatory effects from cytokines IL-1B, 6, 20, and TNF-a.2,4 Monocytes in CRMO compared to general population have been reported to secrete reduced levels of IL-10 and IL-19. 3 Thus, upregulated IL-1B, 6, 20, and TNF-a acutely stimulates neutrophils and chronically stimulates lymphocytes that can be found histologically on biopsy at different timings from the initial onset. 5 In conjunction to upregulated leukocytes, the pro-inflammatory markers also activate nuclear factor kappa-B and RANK signaling, activating the osteoclasts that contribute to the lytic lesions. 1
CRMO primarily presents with bone lesions. The most frequent locations include the metaphysis of long bones and spine, however, the clavicle, craniomaxillofacial skeleton, and sternum have also been reported in literature. 1 Clinical presentation is characterized by the otherwise well-appearing patient presenting with bone pain, typically in a waxing and waning pattern, with swelling, tenderness, skin erythema, and warmth within the subadjacent soft tissue overlying the affected bone. 6 Other variable presentations include fever, malaise, weight loss, and limited range of motion.2,7 Patients with CRMO can have concurrent pathologies that also arise from auto-immune/inflammatory etiologies, such as ankylosing spondylitis, inflammatory bowel disease, psoriasis, palmoplantar pustulosis, pathologic fracture, and acne fulminans. 3
Though a genetic predisposition to CRMO remains controversial, most literature agrees that the pathology occurs sporadically. Monogenic mutations in FBLM1, Pstpip2, LPIN 2, and IL1RN have been tested in murine models and some described in patients. The mutations in these genes are linked to the cytokine instabilities, such as IL1RN mutation with leading deficiency of IL-1 Receptor Antagonist (DIRA), as well as HLA instability, particularly HLA-B27. However, the HLA-B27 positivity, a test indicating autoimmunity, varies in the population, with some literature suggesting there is no association with CRMO.1,2 Other genetic syndromes have been linked to CRMO, such as Majeed syndrome, and adult pathologies including SAPHO, DIRA, and PAPA.2,3
The inflammatory bone pain and lesions in CRMO are often mistaken for other pathologies. Common differential diagnoses include primary malignant bone diseases (Ewing sarcoma, osteosarcoma), benign bone tumors (osteoid osteoma, osteoblastoma, cystic bone tumor), hematological diseases (leukemia, lymphoma, Langerhans cell histiocytosis), metabolic diseases (hypophosphatasia, Vitamin C deficiency), auto-inflammatory diseases (chronic arthritis, PSTPIP1 associated disease), and others (avascular necrosis, growing pain, cherubism, fibrous dysplasia, infectious osteomyelitis).1,2,8 Labs that indicate the autoinflammatory nature of CRMO are variable according to literature as well. As mentioned previously, some report HLA-B27 positivity in a small subset of the CRMO population while others conclude there is no association at all.1,2 The incidence of elevated ESR and CRP is varied, ranging from 19% to 90% of CRMO cases, while leukocytosis was present in 14% to 20% of cases. 1 Other biomarkers with possible linkage to the pathogenesis of CRMO (MCP-1, IL-6, IL-12, RANTES) are still being tested, however, it is conclusive that there are no standardized lab findings that confirm the diagnosis of CRMO. 3
There are two diagnostic criteria, both utilizing biopsy and radiographic findings to frame a CRMO diagnosis. Bristol diagnostic criteria indicates that the patient must have (1) presence of typical clinical findings AND (2) typical radiological findings AND either (A) more than 1 bone involvement (except clavicle, then single bone) with CRP <30 g/l, or (B) if 1 bone (except clavicle) or if CRP >30 g/l, then the additional presence of inflammatory cells without bacterial growth while not on antibiotics. 9 The Bristol criteria further elaborates on typical clinical findings as bone pain with or without swelling without significant features of local and systemic inflammation or infection. Typical radiological findings show that with x-ray, combination of lytic areas, sclerosis, and new bone formation, or with STIR MRI, bone marrow edema with or without bone expansion, lytic areas, and periosteal reaction.9,10 CRMO is diagnosed if the patients meets both (1) and (2) with (A) or (B).
Jansson et al criteria is divided into major and minor diagnostic criteria. Major diagnostic criteria include: (1) radiologically proven osteolytic/osteosclerotic bone lesion, (2) multifocal bone lesion, (3) PPP or psoriasis, and (4) sterile bone biopsy with inflammation, fibrosis, and sclerosis. Minor diagnostic criteria include: (A) normal blood count/general state of good health, (B) CRP and ESR are mild to moderately elevated, (C) observation time was longer than 6 months, (D) hyperostosis, (E) association of other autoimmune disease, and (F) grade I or II family relative with autoimmune/autoinflammatory/non-bacterial osteitis. 11 CRMO is diagnosed using Jansson et al criteria if they meet two major or one major and three minor criteria. 11 Both Jansson et al and Bristol criteria describe the auto-inflammatory nature, clinical presentations, and elusive lab and biomarkers described above while reinforcing that CRMO remains diagnosis of exclusion. Both criteria utilize radiographic images to arrive at CRMO diagnoses.9-11
Radiologically
The stimulation of RANK and RANKL interaction from proinflammatory cytokines result in osteoclast activation, which result in cyclic osteolysis and fibrous replacement. This can be appreciated with x-ray, as suggested by Bristol criteria. 10 However, for a more accurate assessment, CT is preferred, and whole-body (WB) MRI (gadolinium T1 or T2-weighted) is the gold standard for diagnosis.1,4,9,10,12 There are various locations where CRMO can manifest, from acetabulum, femur, tibia, hand, foot, knee, ilium, fibula, clavicle, mandible, sternum, and spine.5,12,13 Aside from the clavicle and mandible, which mainly manifest as unifocal involvement, all other locations typically present multifocally, with one study reporting that 40% of affected population present the lesions symmetrically. 14
CRMO is described as a pathology of stages, with some utilizing the terms chronic nonbacterial osteomyelitis (CNO) or nonbacterial osteitis (NBO) to characterize earlier stages of CRMO.1,15,16 The staging of CRMO from acute to chronic sclerotic progression can be appreciated by analyzing the lesions in WB MRI – the lesions begin as osteolysis, then osteonecrosis, fibrosis, and finally sclerosis. 4 Some also speculate that the number of lesions found in the body indicate chronicity of CRMO manifestations, with discussion from one case study of 8 patients indicating that those with acute, early diagnosis and chronic, late diagnosis all began with one lesion found in MRI. Those with late diagnosis progressed with multifocal lesions while arriving at their correct diagnosis and proper treatment. 5
Although diagnosing CRMO based on radiology is challenging given that lytic lesions are present in a variety of other boney pathologies, Menashe et al discusses how to distinguish CRMO from its mimics. Neoplasms, such as Ewing sarcoma and osteosarcoma, have “moth-eaten” or “sunburst” appearance. Langerhans cell histiocytosis has characteristics which overlap neoplasm and CRMO, appearing to have floating teeth, perilesional sclerosis, lamellar periostitis, and intralesional fluid. Infectious osteomyelitis can be distinguished by pus, bony sequestrum, and fistula formation. 14 Any history of trauma, surgery, or dental procedures can aid in diagnosis against CRMO. Although two of our three cases had a recent and ultimately unrelated history of dental cleaning or periodontal involvement, along with nonsterile microbiological cultures consistent with common oral flora, dental treatment history in the setting of inflammatory osseous pathology initially served as a clinical confounder, pointing our patients toward infectious osteomyelitis, and consequently delaying the correct diagnosis of CRMO.
Histologically
Once a lesion in the bone has been identified, bone biopsy is preferred to further categorize CRMO into different stages. Various stages of immune cell infiltrates in a sterile setting may point to the autoinflammatory characteristics of the pathology. Acutely, there is neutrophil predominance, chronically, lymphoplasmocytic predominance with or without sclerotic bone, and once the bone is fibrosed, there is scant cellular inflammatory infiltrate.5,15 Between bone fibrosis and late-stage sclerosis, multinucleated giant cell recruitment was described in one report. 4
Treatment
Child Arthritis and Rheumatology Research Alliance (CARRA) provides a consensus treatment plan for CRMO patients. The three-treatment arm includes (1) Conventional disease-modifying antirheumatic drug (DMARDs), methotrexate or sulfasalazine, (2) biologic DMARDs, TNF-a inhibitor (usually infliximab) with or without concomitant methotrexate, and (3) bisphosphonate (pamidronate for pediatric population).8,17-19 A short course of glucocorticoid may be used for acute flares, which are common with up to 83% of patients experiencing at least one flare up.1,4 The treatment regime shows favorable outcomes in those who are diagnosed earlier, with a general, 40% remission rate in pediatric patients within 5 years follow up. 1 There are variable reports on treatment responses for those who received late diagnoses as complications are more likely in chronic stages, such as limb length discrepancy, deformity in extremities, and vertebral fractures. 4
Conclusion
CRMO is an autoimmune disease that presents in pediatric populations. It remains a difficult pathology to diagnose as it shares common features with more prevalent bone pathologies both radiologically and histologically. CRMO of the craniomaxillofacial skeleton presents further diagnostic challenges when compared to disease of the axial skeleton due to its often monostotic presentation and mimicry of other facial bone pathologies. We present of our recent CRMO case series and resulting review of the literature in an effort re-emphasize CRMO to surgical providers as a diagnostic consideration in inflammatory pathologies of the craniomaxillofacial skeleton. The review highlights the diagnostic criteria, work-up, and management of this pathology to promote more efficient multidisciplinary communication and coordination remembering that earlier treatment portends a more favorable prognosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Institutional Review Board approval was not required.
Informed Consent
Informed consent for the utilisation of any relevant patient specific information or medical imaging was obtained and filed.