
Abstract
For patients born with cleft lip and/or cleft palate, surgical reconstruction(s) during early childhood serve as the foundation for attaining more normal anatomy and function of the involved areas. As a longstanding cleft and craniofacial institution, we have experienced significant changes in perioperative care regimens. Most notably, the evolution of enhanced recovery protocols has transformed how we care for our patients in the perioperative period. Part I of this publication provides an overview of our institution’s peri-operative protocols, for various cleft-related surgeries, including cleft lip repair, cleft palate repair, speech pharyngoplasty, and alveolar bone grafting. Part II will focus on orthognathic surgery and cleft lip/nasal revisions. This comprehensive review may serve as a prototypical guide for other institutions.
Introduction
Successful medical management of patients with orofacial clefts is complex, as it requires recurrent evaluations of each patient, coordination of care among numerous specialists, and appropriately sequenced surgical reconstructions. Regarding surgical intervention, both technique and peri-operative management play crucial roles related to the surgical care of patients with a cleft lip and/or palate. Novel surgical approaches paired with patient-centered recovery protocols are continually being tested and implemented to achieve the most effective patient care and surgical outcomes. Frequent internal evaluations by a cleft care surgical team (and subsequent changes in its protocols, when indicated) help ensure that invasive operations provide successful restoration of normal form and function for these patients. The development of standardized perioperative protocols serves to ensure that comprehensive and time-sensitive care is provided to this patient population in the safest and most effective manner.
Our institution has previously described the utilization of enhanced recovery protocols for various cleft-related surgeries to successfully manage perioperative pain.1 -3 Part I of this manuscript provides an overview of our institution’s peri-operative protocols, with a focus in pain management, that have been implemented at our institution for various cleft-related surgeries, including cleft lip repair, cleft palate repair, speech pharyngoplasty, and alveolar bone grafting.
ERAS: Safer Pain Management
Traditionally, perioperative pain management in this surgical patient population has centered around the use of opioid medications. Though the use of narcotic medications during the perioperative period often provides adequate pain control, their effects can also be unpredictable and may result in serious complications such as central nervous system depression and ultimately, respiratory failure. 4 Novel approaches to pain management are especially important in the setting of the burgeoning opioid abuse epidemic in the United States.5 -7 Pediatric surgical specialties play a substantial role in this epidemic, as 90% of prescriptions for controlled substances in children were written by surgical services. 8 In addition to this staggering statistic, it is prudent to consider that patients born with a cleft defect often struggle with poor self-esteem and other forms of psychological distress, which may ultimately increase the risk of inappropriate and/or prolonged opioid use following surgical intervention.9,10
To combat the deleterious effects associated with opioid medications, while also providing patients with adequate peri-operative pain management, our institution primarily utilizes non-narcotic alternatives such as non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, gabapentin, and regional anesthetics. To effectively utilize these safer alternatives, we have formed and implemented numerous surgery-specific Enhanced Recovery After Surgery (ERAS) protocols. ERAS protocols (or enhanced recovery protocols [ERPs]), first described by Kehlet in Denmark in the mid-1990s, serve to minimize post-operative morbidity through the utilization of evidence-based perioperative practices. 11 As multidisciplinary perioperative care programs, ERAS protocols are designed to achieve more efficient post-operative recovery through the optimization and maintenance of pre-operative organ function, the reduction in physiologic stress response following surgery, and the implementation of multimodal techniques to provide effective pain relief. 12 Until recent years, ERAS protocols were almost exclusively utilized for adult surgical encounters; however, beginning in 2017, our pediatric plastic surgery team successfully created and implemented an ERAS protocol for patients undergoing cleft palate repair. 1 Its success served as a framework for other pediatric cleft programs, and ultimately prompted the formation of subsequent ERAS protocols for other cleft-related surgeries at our institution.
Perioperative NSAID Use
The use of perioperative NSAIDs as an effective analgesic in both adult and pediatric patients has been comprehensively studied. Due to the drug class’s opioid-sparing effect, NSAIDs have been shown to significantly reduce the need for opioid analgesics as well as postoperative nausea and vomiting (PONV). 13
NSAID safety in infancy
One integral component of successful customizable ERAS protocols involves the minimization of opioid medications paired with the utilization of intra- and post-operative non-steroidal anti-inflammatory drugs (NSAIDs). However, significant provider reluctance regarding the use of this drug class in pediatric pain management still exists. As NSAIDs, ketorolac and ibuprofen are often thought to be linked with gastrointestinal effects, renal dysfunction, and increased bleeding. 14 These concerns are often heightened in patients younger than 6 months of age, despite regular NSAID use in neonatal intensive care units.14,15 As with all medications, possible contraindications or dose reductions must be considered in relevant patient populations. These precautions are applicable when utilizing NSAIDs in patients with bleeding diatheses, cerebrovascular hemorrhage, advanced renal impairment, or those taking nephrotoxic medications.16,17 However, unless deemed a high-risk patient, studies have shown that NSAIDs are safe and effective modes of pain management among infants younger than 6 months.14,18-20
Ketorolac and bleeding risk
One NSAID, ketorolac, has recently gained substantial notoriety as a successful treatment of acute pediatric pain. Although only formally approved for “the short-term (up to 5 days in adults) management of moderately severe acute pain that requires analgesia at the opioid level,” peer-reviewed evidence supports the efficacy and safety profile of the NSAID derivative down to infancy, including patients less than 6 months of age in select populations.17,18,21,22 In addition, earlier notions that NSAIDs, like ketorolac, are associated with an increased risk of major bleeding have been repeatedly disproven. Large-scale prospective randomized controlled trials have failed to establish an association between ketorolac use and perioperative blood loss.23-26 Furthermore, several studies have also shown that ketorolac has a low incidence of major bleeds following surgery in patients younger than 6 months of age (with normal renal and coagulation function).18,27,28
Our institution has found that short-term use of NSAIDs as part of our peri-operative care protocols, inclusive of patients less than 6 months of age, has served as an effective pain control modality without any notable NSAID-related adverse events. This experience aligns with the findings of numerous peer-reviewed studies that validate the short-term use of NSAIDs in patients less than 6 months of age as both a safe and effective option for postoperative pain control.13,14,18,23,27,28
Gabapentin
As in traditional ERAS protocols, our institution utilizes gabapentin as an adjunct therapy to increase the perioperative pain threshold. As a voltage-dependent calcium channel blocker, gabapentin functions to reduce the hyperexcitability of dorsal horn neurons induced by tissue injury, encountered in both trauma and surgery. 29 This reduction in pain realization can subsequently facilitate the minimization of opioid consumption and opioid-related adverse effects.
Multiple studies have shown that the utilization of gabapentin in the acute perioperative setting can provide safe and effective pain management for adult patients.30-32 However, in a 2020 meta-analysis of perioperative gabapentinoid use in 24 682 adult patients, Verret et al concluded that the use of perioperative gabapentinoids in adult patients failed to provide a clinically significant reduction in self-reported pain scores when compared to a control. This finding, paired with an increase in adverse effects (dizziness and visual disturbances), led the authors to dissuade providers from using gabapentinoids for pain management in adult patients. 33
Despite the conflicting results surrounding perioperative gabapentin use in adults, studies examining its safety and effectiveness in the pediatric population have shown significant benefits. The use of gabapentin in the pediatric surgical population has not been extensively studied; however, numerous studies have shown the use of gabapentin during the perioperative period can provide substantial benefits, most notably, lower pain scores and decreased opioid consumption, decreased agitation, and fewer incidences of PONV.34-38 Burjek et al’s review of current perioperative gabapentin studies in both pediatric and adult populations concluded that the drug is generally well tolerated by children and that the undesirable effects of the medication sometimes shown in the adult population (described above) may not be as significant in the pediatric population. 35 Our institution’s use of gabapentin as a part of a multi-modal approach to acute perioperative pain management supports these findings.1-3
Cleft Lip Repair
At our institution, patients born with a cleft lip undergo repair at approximately 3 to 5 months of age, with the precise timing of surgical intervention often dictated by the presurgical molding device. Surgical eligibility also necessitates positive trending weight gain—historically, a minimum of 10 pounds at the time of surgery has been used.
Pre-operative
Prior to surgery, these patients do not receive an anxiolytic; however, some patients are given oral acetaminophen, at the anesthesiologist’s discretion.
Intra-operative
After identifying anatomical landmarks with methylene blue tattoo, the surgical team performs local infiltration of the surgical site with either 0.5% lidocaine with epinephrine (1:200 000) or 0.25% bupivacaine with epinephrine (1:200 000) to provide adequate vasoconstriction and analgesia prior to incision. Although we have not instituted an official ERAS protocol for this surgery, administration of opioid medications is minimized both intra- and post-operatively.
Post-operative
Following surgical completion and appropriate recovery in the post-anesthesia (PACU) unit, these patients are admitted to the hospital for further postoperative monitoring and care. Generally, our cleft lip repair population progresses very well following surgery. This pattern, combined with a period of COVID-related bed/staff shortages, and in hopes of preventing further delay in surgical management, prompted our team to initiate a trial of managing this surgical population on an ambulatory basis. Although this change in status did not result in any reported health-threatening events, both the caregivers and the day surgery nurses communicated multiple concerns including an increase in caregiver anxiety and a lack of post-surgical nursing staff to care for the patient for a prolonged amount of time. Following internal deliberation, we ultimately resumed our prior admission protocol, which usually consists of an admission of less than 24 hours. Further, approximately 9% of patients who underwent cleft lip repair patients (primarily those with form fruste and/or whose repair does not require any significant nasal dissection) are safely discharged home after less than 8 hours of observation once discharge criteria (pain control, feeding, and guardian comfort level) are met.
Surgical site care
For approximately 2 weeks following surgery, patients who underwent cleft lip repair are required to wear bilateral elbow restraints (sometimes called “welcome sleeves” or “no-no’s”) to help mitigate the risk of direct trauma to the surgical site. Patients can resume normal bathing practices (including temporary removal of the arm restrictors) approximately 48 hours after surgery. All 3 surgeons at our institution use absorbable sutures followed by placement of a layer of surgical skin glue over the philtral repair. Aside from light cleaning of the surgical site, no other topical care is required until the first post-operative evaluation (approximately 2-3 weeks after surgery), when the surgical site is evaluated, and personalized scar (or wound) management is prescribed.
Diet
Our team allows patients to resume nutritional intake via bottles immediately after surgery. Syringes with soft rubber tips are sometimes utilized to encourage postoperative feeding. In addition, pacifiers are permitted after surgery.
Pain management
In the postoperative period, pain is generally well-managed with the utilization of oral ibuprofen (or intravenous ketorolac) and oral (or rectal) acetaminophen. If the patient refuses to eat and is having trouble sleeping due to assumed surgical pain, a one-time dose of oral hydrocodone/acetaminophen (7.5 mg/325 mg/15 ml) may be ordered. Upon discharge, the patient’s caregivers are encouraged to continue giving the patient over-the-counter (OTC) acetaminophen and/or ibuprofen as needed for pain.
Cleft Palate Repair
To maximize speech function, our institution prefers to perform primary palatoplasty on patients that are between 9 and 12 months of age. The acute postoperative period following cleft palate repair is often burdensome due to severe pain and associated feeding difficulties paired with the administration of oral and/or intravenous opioids. Since its institution in the Spring of 2017, our Cleft Palate ERAS Protocol has served to standardize our approach to perioperative pain management serving to significantly mitigate opioid administration and improve the rate of feeding tolerance.
ERAS Protocol
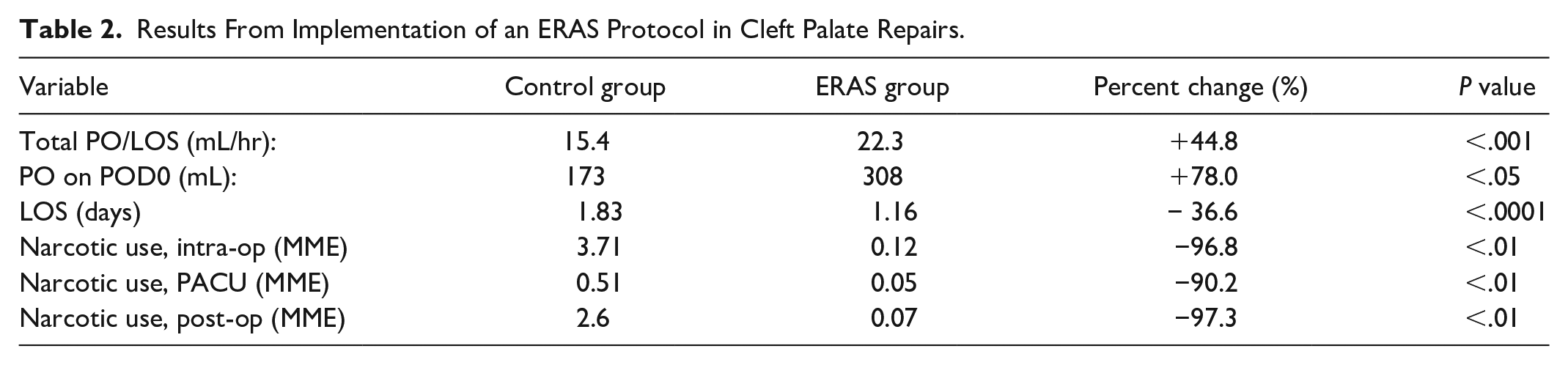
The primary components of our flagship protocol include: (1) pre- and post-operative gabapentin administration, (2) minimal perioperative narcotic use, and (3) postoperative pain control using scheduled acetaminophen and ketorolac (Table 1). 1 Ultimately, our ERAS protocol pilot study demonstrated a 90% to 97% decrease in narcotic utilization in all 3 peri-operative phases of care (Table 2)—intra-operative, post anesthesia care unit (PACU), and postoperative (P ≤ .01). 1 Postoperative feeding rates also drastically improved, shown by an increase of 44.8% (15.4 ± 6.9 ml/hour to 23.0 ± 10 ml/hour, P ≤ .001) among ERAS patients. 1 Inclusive of all patients who underwent primary palatoplasty, the implementation of our ERAS protocol resulted in a 31.7% decrease in length of stay when compared to historical controls (1.83 ± 1.18 vs 1.25 ± 0.76, P ≤ .001). 2 In late 2019, in hopes of further augmenting the protocol’s beneficial effects, our institution implemented the use of an ultrasound-guided bilateral suprazygomatic maxillary nerve block (SMB), performed by the anesthesia pain team following anesthesia induction.
ERAS protocol for cleft palate repair.
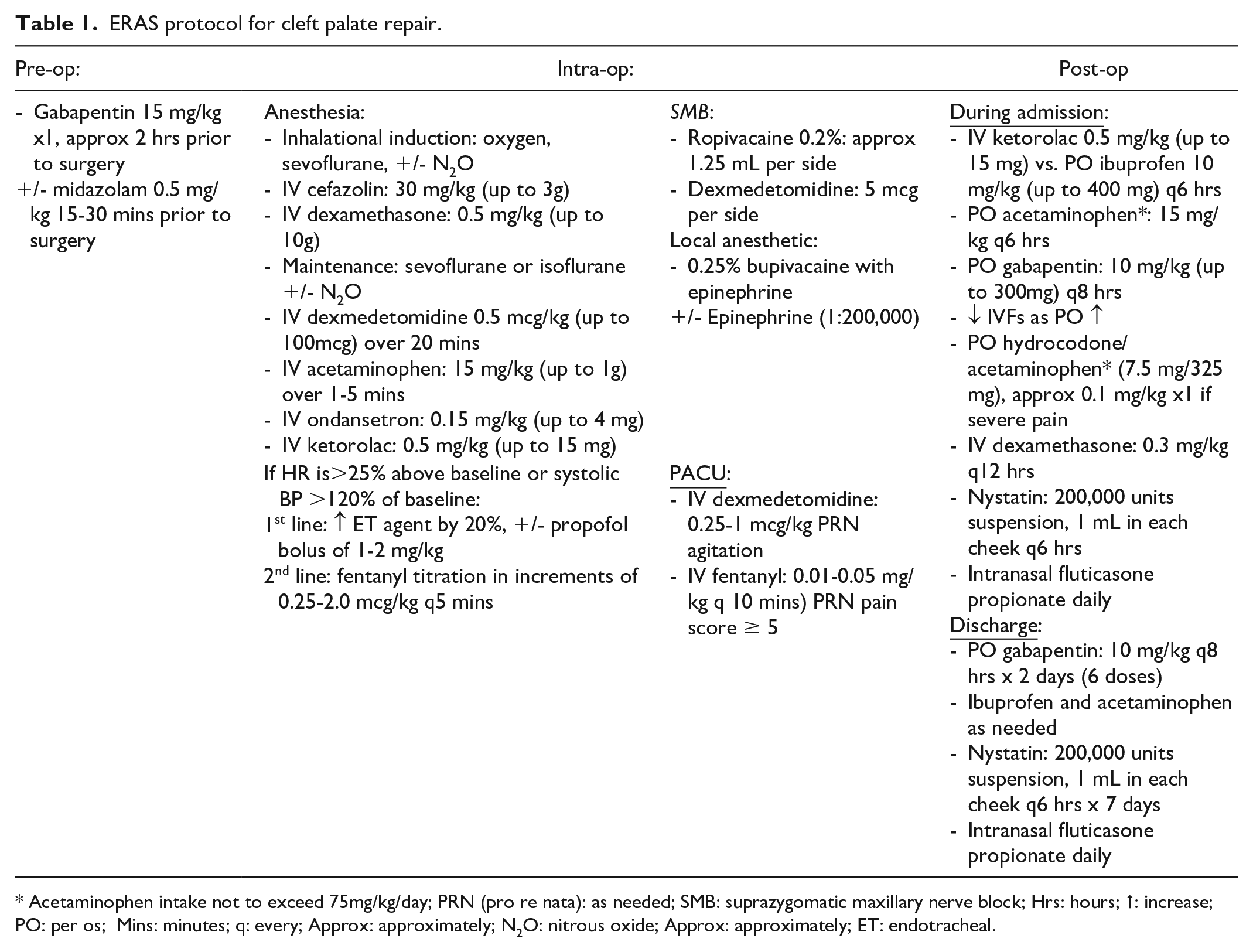
Acetaminophen intake not to exceed 75mg/kg/day; PRN (pro re nata): as needed; SMB: suprazygomatic maxillary nerve block; Hrs: hours; ↑: increase; PO: per os; Mins: minutes; q: every; Approx: approximately; N2O: nitrous oxide; Approx: approximately; ET: endotracheal.
Results From Implementation of an ERAS Protocol in Cleft Palate Repairs.
Pre-operative
As mentioned above, a loading dose (15 mg/kg) of gabapentin is given to patients undergoing primary palatoplasty approximately 2 hours prior to surgery. Patients are also encouraged to consume clear, carbohydrate-rich beverages up to 2 hours prior to surgery to prevent a catabolic state and to minimize post-surgical insulin resistance and hyperglycemia.
Intra-operative
Patients who receive bilateral SMBs following anesthesia induction rarely require pain management with opioids during the operation. Proper anesthesia is maintained using dexmedetomidine at a rate of 0.5 to 1.0 mg/kg. On occasion, intravenous fentanyl is administered by the anesthesia team on an as-needed basis, especially upon emergence. Even with the assumed coverage from the SMB, the surgical field, including the greater palatine nerve, is locally infiltrated with 0.25% bupivacaine with epinephrine (1:200 000). However, some areas involved in cleft palate repair do not benefit from the nerve block. If a buccal fat flap is utilized during the repair, a small amount (1-2 ml) of 0.25% bupivacaine with epinephrine (1:200 000) is injected into the donor site to ensure adequate pain control. At the conclusion of the procedure, a similar amount of the same local anesthetic is injected into the anterior tongue, and a stitch is placed for potential airway management in the PACU. During the PACU phase of care, the stitch is removed by the nurse once a patient is deemed stable.
Post-operative
Despite the utilization of various surgical techniques among the staff surgeons, the same postoperative regimen is universally implemented. As with patients undergoing cleft lip repair, patients who are status post cleft palatoplasty are also admitted to the hospital. Since implementing our ERAS protocol, the average LOS has decreased from 1.83 ± 1.18 days to 1.16 ± 0.76 days, resulting in a 36.6% decrease (P ≤ .001) (Table 2). 2
Surgical site care
Infants who underwent cleft palatoplasty are required to don bilateral elbow restraints to prevent trauma to the surgical site. Unlike the cleft lip repair patients, however, these patients are not permitted to use a pacifier postoperatively for at least 3 weeks. No surgical site cleaning regimen is required, but caregivers are encouraged to observe for signs of thrush, as its presence tends to lead to premature dissolution of the vicryl sutures used during surgery. Based on experience, our institution prescribes oral nystatin (200 000 units suspension) to help prevent the development of oral thrush. We recognize that we may be unique in this; however, over the course of a year, we experience several (10-12) patients who have significant thrush that impacts the healing of the palate. This may be related to the amount of oral feeds; no postoperative antibiotics are used. We are particularly mindful of this in patients who are G tube or NG tube dependent with little oral intake.
In order to help manage surgery-related nasopharyngeal swelling, caregivers are instructed to administer one spray in each nostril of intranasal corticosteroid spray, like fluticasone propionate or mometasone furoate, for a total of 3 weeks after surgery.
Diet
This surgical population is also encouraged to drink from bottles that have Dr. Brown or pigeon nipples. They may also consume stage 1 to 2 baby food and drink out of a spoutless or low- and soft-spout sippy cup. Syringes with a soft tip extension are also available during admission for feeding assistance if needed.
Pain management
In the postoperative period, a scheduled regimen of oral gabapentin, oral acetaminophen, and intravenous ketorolac (or oral ibuprofen if IV is lost) is utilized to comprehensively manage surgical pain (Table 1). The use of oral opioids (ie, hydrocodone/acetaminophen 7.5 mg/325 mg/15 ml) is rarely indicated, but a one-time dose is available in the order set upon admission. Upon discharge, these patients are sent home with 6 doses (to cover 48 hours) of gabapentin, to be taken every 8 hours. In addition, caregivers are encouraged to continue the use of OTC oral ibuprofen and oral acetaminophen at their discretion.
Under the assumption that oral intake correlates with adequate pain control, our ERAS protocol for patients undergoing cleft palatoplasty was tremendously successful at its goal of establishing an effective and safe alternative to traditional pain control methods. With the joint execution of a customized ERAS program by both the anesthesia and surgical teams, our patients received effective pain control while minimizing narcotics, evidencing a faster return to feeding, and a shorter LOS without an increase in complication rates. Since its inception, our ERAS protocol has been utilized for over 600 patients undergoing cleft palate repair at our institution. This protocol, supported by our statistically significant findings, serves as a framework from which other pediatric surgical subspecialties can adapt and create their own comprehensive ERAS specialty-specific protocols.
Speech Surgery
Despite closure of the palatal cleft prior to major speech development, approximately 20% to 30% of children who undergo cleft palatoplasty will require speech-correcting surgery due to velopharyngeal dysfunction.39-42
ERAS Protocol
Similar to patients undergoing cleft palate repair, the historic pain management modality for patients undergoing surgery for velopharyngeal insufficiency has traditionally been with opioid medications. Following the success of the cleft palate ERAS protocol, an ERAS protocol was created and tailored to patients undergoing pharyngoplasty. The major guiding elements in the speech surgery ERAS protocol are congruent with those in the cleft palate repair ERAS protocol; however, a few alterations were made to more appropriately serve this specific patient population. Patients undergoing speech pharyngoplasty vary from patients undergoing cleft palatoplasty in several ways—these patients are of advanced age (no younger than 2 years old) and have more developed speech (and an increased ability to communicate pain level). Additionally, these patients will likely not benefit from the administration of a suprazygomatic maxillary nerve block, as the sensory innervations of the maxillary nerve (hard and soft palate, upper jaw, upper dental arch, and upper lip) fail to include the primary structures involved in pharyngoplasty. 43 After several years of anecdotal success, patient outcomes (narcotic use, feeding rate, length of stay, and complication rate) with the use of this ERAS protocol were compared to those included in the traditional (heavily reliant on opioid medications) pain management regimen. An analysis of order to assess the success of an ERAS protocol for this surgical population, our institution reviewed patient demographics, narcotic use, length of stay (LOS), and complication rates. Results revealed that implementation of our speech surgery ERAS protocol provided effective perioperative pain control (allowing for narcotic minimization) and was associated with a reduced LOS, without an increased complication rate (Table 3). 3
Results From Implementation of an ERAS Protocol in the Surgical Management of Pediatric Velopharyngeal Insufficiency.

Pre-operative
As with the recovery protocol implemented for cleft palate repair, our ERAS protocol for VPI surgery includes a pre-operative dose of gabapentin (15 mg/kg, maximum dose: 600 mg), given 2 hours before surgery. If deemed appropriate by anesthesiology, the patient may also receive an anxiolytic (such as oral midazolam) approximately 30 minutes before surgery.
Intra-operative
The anesthesiology team utilizes the same intraoperative ERAS protocol applied to cleft palate repair. Since a regional block is not administered for this patient population, short-acting opioids like fentanyl are judiciously given based on pain parameters established in the protocol. Prior to surgical incision, relevant anatomical structures are infiltrated with 0.25% bupivacaine with epinephrine (1:200 000). If undergoing a sphincter pharyngoplasty or pharyngeal flap a member of the surgical team will insert an appropriately sized nasopharyngeal airway (also called a “nasal trumpet”) before closing the oral mucosa. This is done to ensure adequate airway patency in the setting of soft tissue swelling during the recovery period. The soft tube is taped in place by the anesthesia team at the conclusion of the surgery, and welcome sleeves are placed on the patient if deemed age-appropriate to prevent the patient from pulling the tube out upon waking.
Post-operative
Following speech pharyngoplasty, patients are admitted overnight for respiratory monitoring and pain management.
Surgical site care
Care and cleaning of the surgical sites primarily rely on adequate oral intake, especially fluids. Upon surgical rounds (if the patient is adequately alert), the nasal trumpet is removed at the bedside (and welcome sleeves are removed, if applicable), approximately 4 to 8 hours after surgery. To abate swelling of the soft tissues, patients who are status post pharyngoplasty are prescribed daily use of an intranasal corticosteroid for approximately 3 weeks.
Diet
Patients are required to follow a strict soft mechanical (moist and minced) diet to avoid damage to the surgical incisions, and patients are encouraged to begin consuming liquid or soft foods early in the postoperative course. This diet is maintained at least until the first postoperative evaluation, approximately 3 weeks following surgery.
Pain management
Postoperative pain management during admission consists of oral gabapentin, oral acetaminophen, and an NSAID (IV ketorolac or oral ibuprofen), all of which are given on a scheduled basis. Rarely, patients require one or more doses of a narcotic pain medication. When discharge criteria have been met, patients who underwent a pharyngoplasty are prescribed a 2-day course of scheduled gabapentin. Like the inpatient regimen, this medication is most effective when used in combination with over-the-counter acetaminophen and ibuprofen, and upon completion of the gabapentin prescription, patients can continue to utilize the OTC medications as needed. Postoperative opioids are not routinely given.
Alveolar Bone Grafting
Repair of the alveolar cleft with bone grafting is completed during the period of mixed dentition (7-9 years of age). Phase one orthodontics for expansion/correction of crossbite is completed prior to surgery, and lateral segments are secured with either a dental-based palatal expander or brackets and wires. Both are maintained post-reconstruction for approximately 6 months.
Traditionally our institution used autologous bone (iliac crest) for the alveolar reconstruction, requiring hospitalization and opioids for pain management, despite surgical site infiltration with local anesthetic. Although newer, less-invasive techniques have been implemented for harvesting the cancellous bone, the elements of postoperative care remained.44-48 Since 2016, our institution has regularly used recombinant human bone morphogenetic protein (rhBMP-2) for alveolar cleft reconstruction. Demineralized bone matrix (DBM)—alone or infused with mesenchymal stem cells and growth factors—was subsequently added to the treatment regimen, creating a “sandwich” or “roll” structure that is placed in the cleft. This helps maintain a 3-dimensional space and therefore provides adequate room for new bone to grow with adequate volume. Preparation of each product was accomplished by following the manufacturers’ instructions. With the implementation of BMP-2 and DBM, we have been able to successfully transition the postoperative course from an overnight stay to an ambulatory status. Our experience has been supported by multiple institutions.49-53
Pre-operative
Patients are asked to perform their normal oral hygiene regimen on the morning of surgery. At the discretion of the anesthesia attending, oral midazolam (0.5 mg/kg) may be given to the patient approximately 15 to 30 minutes before surgery.
Intra-operative
To minimize contamination of the grafts (described above), oral chlorhexidine is utilized throughout the procedure as irrigation. Involved tissues are infiltrated with 0.25% bupivacaine with epinephrine (1:200 000) or 0.5% lidocaine with epinephrine (1:200 000) prior to incision.
Post-operative
Surgical site care
Patients are asked to use caution when resuming oral hygiene practices and are generally asked to refrain from brushing their upper teeth for at least 5 days. A prescription for oral chlorhexidine rinse is also given to help maintain oral hygiene. Due to the concentration of BMP present on the collagen carrier, significant localized soft tissue edema is anticipated in all patients; therefore, a methylprednisolone dose pack is prescribed to help combat this. Patients are also encouraged to gently apply cold packs to the mouth and cheeks for comfort and swelling reduction.
Diet
Patients are asked to maintain a soft mechanical diet for at least 3 weeks.
Pain management
Postoperative pain is managed with OTC oral NSAIDs and acetaminophen. Patients do not require perioperative narcotics for this outpatient procedure.
Conclusion
Recent literature shows that patients with cleft lip and palate undergo an average of 4.8 to 10.5 cleft-related surgeries by the age of 18.54-56 In order to consistently provide the best surgical outcomes and address the needs of our patients throughout their surgical journey, we have heavily relied upon the utilization and maintenance of perioperative regimens. Part I of this review describes our experience with their application to the early part of the cleft paradigm (cleft lip repair, cleft palate repair, speech surgery, and alveolar bone grafting). These perioperative regimens have successfully reduced perioperative narcotic utilization, time to postoperative oral intake, and admission length, without increasing complication rates.
The motivation for this paper was to provide an overview of patient care through the lens of pain management. Our institution has described specific aspects of pain management for cleft palate, speech surgery, orthognathic surgery in previous manuscripts. Our goal was to provide this in the context of the entirety of all cleft surgeries that a patient may experience. The authors would like to reiterate that the creation of our ERAS and pain management structure does not prohibit the use of opioids or outline specific boundaries for management by healthcare providers (surgical team, anesthesia, nursing staff). We understand that each individual patient is unique, and management should be tailored appropriately. Our second installment will present multimodal analgesia regimens as they apply to orthognathic surgery and cleft lip/nasal revisions.
Footnotes
Acknowledgements
None
Correction (December 2024):
Article has been updated to address minor stylistic adjustments.
Data Accessibility Statement
Data sharing is does not apply to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Informed Consent
No informed consent is required, as this review only analyzes previously published information and does not involve anynew interventions or data collection on human subjects.