
Abstract
Introduction:
Patients with cleft lip and/or palate (CL/P) face unique challenges that extend beyond physical health, affecting their psychosocial well-being. This paper reviews the existing literature on psychosocial outcomes of individuals with CL/P and the various methods employed to evaluate these outcomes.
Methods:
A comprehensive review of current studies was conducted, categorizing findings into 5 primary psychosocial domains: Self-Image, Social Relationships, Psychological Well-Being, Behavioral Adjustment, and Societal Stigma. The review also analyzed methodological variability, including self-report instruments, parent-proxy assessments, and whether measures were cleft-specific.
Discussion:
The findings revealed that children with CL/P, compared to their unaffected peers, may experience lower self-esteem, greater difficulties in social interactions, and increased anxiety or depression. However, studies showed mixed results regarding behavioral adjustment, with some comparable levels of behavioral issues between affected and unaffected children. Adults with CL/P demonstrated resilience in achieving similar levels of education, income, and occupational success as their peers.
Conclusion:
Discrepancies in evaluation of psychosocial wellbeing highlight the need for more standardized methodologies and a holistic approach to assessment. Furthermore, the influence of social stigma remains significant, underscoring the importance of addressing public perceptions of cleft conditions. Care recommendations include: multidisciplinary teams, minimizing unnecessary surgical interventions, self-report outcome instruments, holistic assessment of both deficit-based and asset-based qualities, and increased visibility within mass media.
Keywords
Introduction
Cleft lip and/or palate (CL/P) are among the most common congenital birth defects, affecting an approximate 1 in 700 live births per year globally, with higher prevalence in various regions of Northern Europe, Latin America, and Asia. 1 Although prominent functional impairments such as speech, hearing, feeding, or breathing difficulties may benefit from surgical intervention, patients with CL/P may still experience persistent psychosocial challenges. Children with CL/P may face the dual challenges of standing out socially and physically among their peers while also coping with speech impairments, such as hypernasality or compensatory misarticulation patterns, which can further isolate them socially. Additionally, the emotional toll of repeated medical procedures may lead to the development of pediatric medical traumatic stress. Caregivers may also feel an increased sense of stigma because of their child’s distinctiveness, which is exacerbated by the emotional and financial difficulties stemming from prolonged and repetitive medical interventions. Previous research has thus highlighted potential differences for those born with CL/P in relation to quality of life, psychological health, functional well-being, social emotional well-being, and school environment. 2
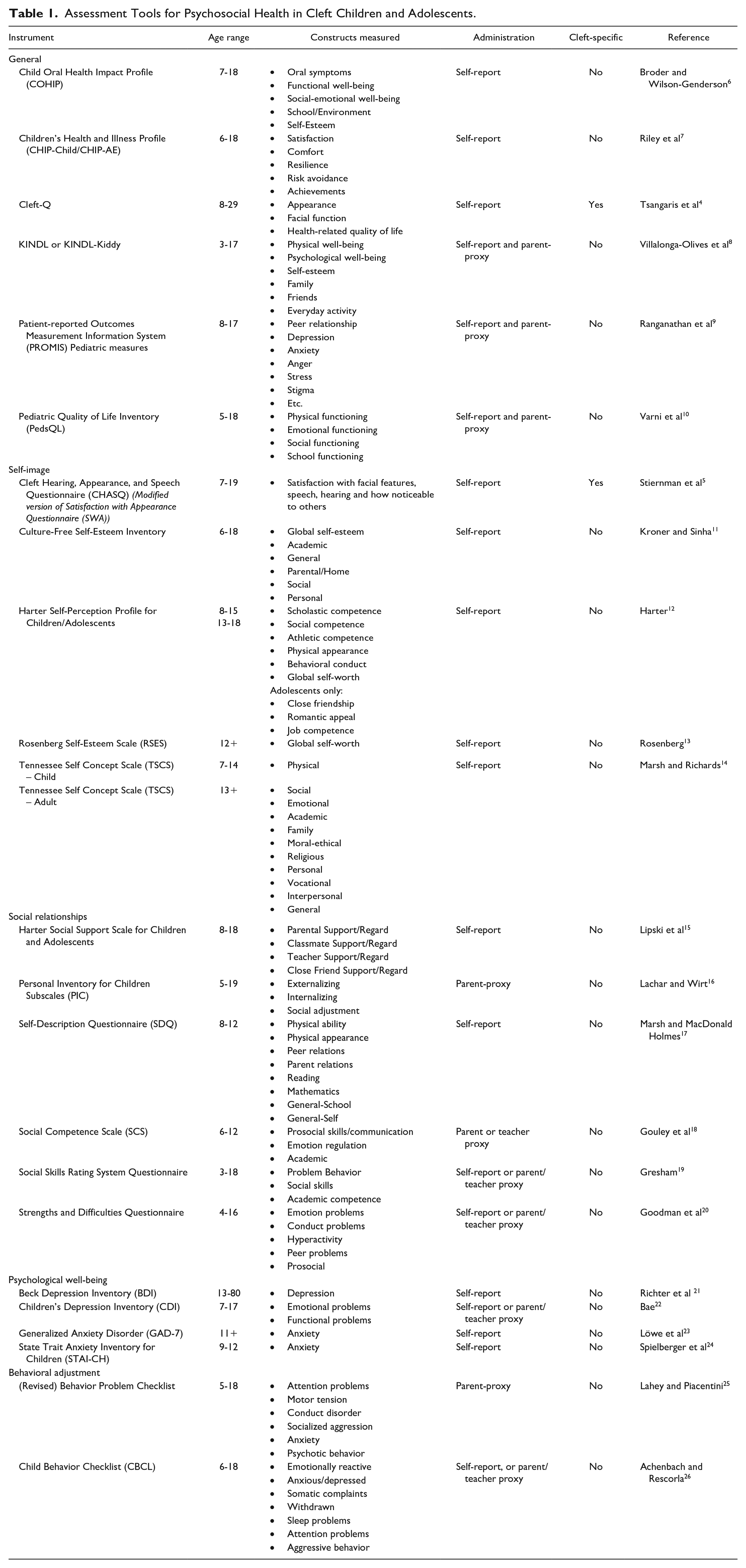
A recent scoping review by Yusof and Mohd Ibrahim 2 reports on the findings of 20 recent studies on patients ages 7 to 18 years, with 16 out of 20 studies showing negative impacts of CL/P conditions on overall quality of life. However, one of the largest limitations in the current literature is due to the large variation in reporting of psychosocial functioning, which often leads to broad generalizations. Guillén et al 3 showed this lack of uniformity in assessment strategies across 26 studies between 2007 and 2017 which utilize 36 different generic instruments for psychosocial health in CL/P patients and only 1 instrument specific to CL/P patients (QoLAdoCleft questionnaire). They conclude that the most commonly reported psychological variables in studies of CL/P children and adolescents are quality of life (QoL), social function, and coping. However, studies which report on “quality of life” may be referring to different dimensions of psychosocial wellbeing, such as physical wellbeing, psychosocial wellbeing, self-esteem, family, friends, and school functioning. Table 1 thus provides an extensive list of commonly used assessment tools for the psychosocial health in children and adolescents with CL/P, along with the specific constructs measured, appropriate age groups, and methods of administration. Since 2017, two new instruments have been developed which are specific to the CL/P population, including the CLEFT-Q developed in 2017 and the CHASQ developed in 2019.4,5
Assessment Tools for Psychosocial Health in Cleft Children and Adolescents.
In light of the existing variability in the current psychosocial literature, the aims of this review are twofold. First, we report updated findings from the current literature through 5 distinct domains:
Self-Image
Social Relationships
Psychological Well-Being
Behavioral Adjustment
Societal Stigma
As expected, many of these domains may overlap and influence each other, which highlights the need for improved consistency and clarity of specific outcomes. Secondly, while the majority of review articles tend to limit findings to patients younger than 18 years of age, this review will report on the psychosocial functioning and long-term outcomes in adulthood.
Self-Image
Self-image is defined as the mental picture or perception that one has of oneself. It encompasses how individuals see their own physical appearance, personality traits, abilities, and overall worth. Popularly utilized instruments for measuring feelings of self-image in children and adolescents include the Rosenberg Self-Esteem Scale (RSES) and the Harter Self-Perception Profile for Children and Adolescents.12,13 Additionally, the CLEFT-Q and CHASQ are newly developed instruments since 2017 which each have scales assessing appearance and satisfaction with facial features.4,5 Each questionnaire is validated for the ages 8 to 29 and 7 to 19, respectively. In general, most self-report psychosocial questionnaires are most effective when delivered to individuals older than 8 years of age.
In general, individuals with CL/P report to be significantly less happy with their facial appearance compared to unaffected individuals, across all genders.27-31 Multiple studies find that children and adults with CL/P report lower self-esteem compared to control groups.32-34 The most common sources of dissatisfaction are the appearance of nose, lips, teeth, and visible scars. Of note, scar visibility has been identified as a significant predictor of dissatisfaction with facial appearance and worse psychological wellbeing.28,35,36 Additionally, facial dissatisfaction may be exacerbated by female gender and peer harassment in school aged children.27,37,38 It has been suggested that dissatisfaction with facial appearance predicts lower health-related quality of life (HRQL), while acceptance of one’s cleft may improve self-esteem and social experiences.27,39,40 On the other hand, 1 study with 94 Scottish children age 10 found significantly higher self-esteem in children with CL/P compared to unaffected peers, 35 while 1 study with 91 Dutch participants ages 10 to 17 years found similar levels of self-esteem. 41 Thus, while individuals with CL/P generally report lower self-esteem and higher facial dissatisfaction compared to unaffected peers, there is variability in self-esteem outcomes, suggesting that factors such as gender, peer interactions, and acceptance of one’s appearance play significant roles in psychosocial well-being.
Social Relationships
In the CL/P population, evaluations of social relationships primarily evaluate interactions between peers or family relationships. Compared to unaffected peers, children with CL/P may experience greater social difficulties.42,43 Although many measure instruments for social functioning exist, many studies often rely on parent and teacher proxy reports. However, studies show that significant discrepancies may exist between self-report and caregivers evaluations, suggesting that caregiver reports should be considered complementary to the reports of patients themselves.44,45 Evaluation of social functioning typically involves examining proficiency in communication strategies and emotion regulation skills. Many questionnaires for patients with CL/P may also focus on everyday conversational comprehensibility (eg, “Other people clearly understand what I’m saying”) to gage the potential impact of one’s cleft condition on their communication abilities. On the other hand, peer relationships are often assessed by the degree of avoidance (eg, “I would rather be alone than with people of my age”) or experiences with bullying (eg, “Other children or young people pick on me or bully me”). Thus, it is advantageous for clinicians to clearly distinguish if any issues with social interactions are due to difficulties with pragmatic language, speech impediments, shy personality, or bullying problems, as each issue requires a distinct intervention.
It has been suggested that children and adolescents with CL/P exhibit less assertiveness in their conversation styles, preferring to socially withdraw rather than participate actively in conversations.46-52 This could be partially attributed to the negative social judgment of hypernasality in a select number of patients. 53 Berger and Dalton 50 demonstrated that speech difficulty was a significant predictor of poor adjustment and accounted for 19.6% of the variance in patients’ total scores for the Strengths and Difficulties Questionnaire. In general, children with CL/P and their parents may view them as having lower social competence in comparison to their peers.38,47,51,54-57 However, other studies show no significant differences in social competence, social acceptance, or social support when compared to control groups.29,49,52,58-60 On the other hand, Slifer et al 51 found that children with clefts who reported feeling more socially accepted on the Harter Self-Perception Profile had a positive correlation with greater time looking an unfamiliar peer in the face during social interactions. Interestingly, this relationship was not observed in the control group of children without clefts. Contrarily, Feragen et al 36 found that the visibility of a cleft negatively affected girls’ perceptions of peer problems but positively affected boys’ perceptions of their close friendships. Boys with visible clefts perceived their close friendships more positively, compared to both the nonvisible cleft group and the reference group. This finding suggests that the social impact of cleft visibility can vary significantly based on gender, with potentially positive or negative social effects.
Behavioral Adjustment
While there is considerable overlap between evaluations of social interaction and behavioral adjustment, lacking social skills does not always indicate more significant behavioral issues. Behavioral adjustment refers to the process through which individuals are able to cope with new situations or achieve personal goals. Behavior problems may be categorized into two types: internalizing issues (anxious-depressed, withdrawn, and somatic problems) and externalizing issues (aggressive behavior and delinquency). A few studies suggest that children with CL/P may have higher levels of internalizing behavioral problems compared to their peers.43,61 Ha et al 56 found in a study with 93 patients with CL/P ages 6 to 11 years that males were more likely to score in the clinical range for aggressive behavior, while females were more likely to score in the clinical range for anxious-depressed behavior on the Child Behavior Checklist (CBCL). Although previous studies report higher rates of social and behavioral problems in patients with CL/P,62-64 many newer studies suggest that children with cleft conditions have equivalent or even lower levels of behavioral problems compared to their peers.31,36,60,65,66 Soedjana et al 66 found in a cross sectional study of parent reports among 104 participants with a median age of 8 years old that the majority are within normal range for social, school, and problem subscales on the Child Behavior Checklist (CBCL). On the other hand, the majority of patients report experiences of taunting and bullying directly related to their cleft condition, often beginning in primary school and reaching peak aggressiveness in middle school.30,67,68 Thus, it is essential for care providers and guardians to distinguish between internalizing/externalizing behavioral problems and external contributors to negative school experiences in order to provide the most effective support.
Children born with oral clefts tend to demonstrate lower educational attainment compared to their unaffected peers, irrespective of socioeconomic status (SES), subject area, or grade level.31,69-71 On the other hand, higher socioeconomic status is found to be associated with reduced behavioral problems and somatic symptoms in children ages 2 to 12 years. 31 Additional risk factors contributing to poor academic performance include isolated cleft palate (CP), adolescent motherhood, low maternal educational attainment, and infrequent utilization of prenatal care. 72 It is possible that learning difficulties may be more common in CP due to a higher association with syndromic conditions, such as 22q11.2 deletion or Stickler syndrome, compared to CL/P.73,74 Children with clefts also tend to have higher need for special education services compared to their classmates.71,75 These findings indicate the importance of implementing interventions targeting both verbal and nonverbal learning skills, ideally before the children begin school. This approach would enable optimal collaboration among caregivers, school administrators, and craniofacial medical teams.
Psychological Well-Being
In contrast with behavioral adaptations to one’s environment, psychological well-being refers to the overall state of an individual’s mental health, encompassing emotional, psychological, and social aspects of well-being. Studies suggest that patients with CL/P across all ages are significantly more likely to experience emotional and behavioral difficulties.28,38,41,42,61,76-78 Children ages 6 to 12 years may be especially at risk of high incidences of anxiety, depression, and impaired wellbeing. 79 Other risk factors for worse emotional well-being include female gender, non-private insurance status, visible scars, and ethnic minority status.36,80,81 Additionally, the number of surgeries that individuals undergo during their lifetime appears to play a large role in long-term well-being. Broder et al 80 found that a cohort of 402 youth who received a surgical recommendation at baseline showed lower average functional well-being, emotional well-being, and self-esteem scores when compared to 798 youth who did not receive a surgical recommendation. In a study by Wehby et al 31 with 104 children aged 2 to 12 years with isolated oral clefts, the number of cleft-related surgeries was associated with increased anxiety, depression, and somatic symptom risks. Similarly, although Potemra et al 82 found no association between cleft conditions and emotional problems, they observed that the quantity of surgeries had an adverse impact on anxiety and depression levels, particularly during the ages of 8 to 10 years. Thus, care providers should take into consideration vulnerable age groups and the exacerbative effect of repeated exposures to medical interventions when assessing psychosocial wellbeing of patients. If possible, the number of unnecessary medical interventions should be minimized in order to preserve the mental health of patients.
Societal Stigma
Societal stigma refers to the negative attitudes, beliefs, and discrimination that society generally holds toward a particular group based on characteristics perceived as different. The majority of patients with CL/P and their caretakers report perceptions of stigma and unwanted staring or questioning during childhood and adulthood.59,83-86 Hunt et al 28 reports that 55% of experiences with bullying and teasing are related to the individual’s facial appearance, while 34% are related to speech difficulties. In contrast to other unseen disabilities, facial differences and speech disorders notably affect every social interactions, exposing patients to potential harassment and discrimination. Compared to patients with isolated CP only, it appears that patients with cleft lip (CL) or cleft lip and palate (CLP) report higher experiences of stigma. 87 One explanation for this is the higher likelihood of a visible scar that accompanies surgical lip repair, which has been shown to predict worse overall psychosocial outcomes. 28 Feelings of stigma may additionally extend beyond the school environment and persist in the workplace during adulthood.67,85,88 In one study by Pausch et al 89 a cohort of 273 adult laypersons were presented with pictures of 50 patients with repaired clefts and were asked to rate their level of social acceptance. Although their study found improved levels of social acceptance between results from 1973 and 2013, there was still lower levels of acceptance for individuals with CL/P as a “marriage partner,” “son or daughter-in-law,” and “buddy” compared to as a “fellow citizen” or “neighbor.”
Societal factors and media portrayal of facial differences also play an important role in shaping general public perceptions of visible scars and disability. Historically, media portrayals have often depicted facial difference, disabilities, and scars with strong connotations of evil and malevolence. 90 A few popular examples include “Scar” from The Lion King, the Joker, and Freddie Kruger. This pattern of negative representation has thus contributed to a pervasive stigmatizing effect for individuals with facial differences. However, the opposite effect may be true with positive portrayals. Increased representation and direct interaction with individuals with cleft conditions could foster a more positive attitude development by challenging initial assumptions and dispelling negative stereotypes. 88 One study shows that listening to an audio or watching a video of someone with a facial disfigurement sharing their personal story may result in more favorable impressions regarding social skills, emotional stability, leadership qualities, and capacity to build relationships compared to merely viewing a still photo. 91 Although a few studies report that patients with CL/P may attain equivalent education, income, occupation, and home ownership levels compared to the general population, 92 it is apparent that considerable levels of stigma and social barriers remain regarding public perception of visible difference and disability.
Conclusion and Future Directions
Due to the abundance of literature on the CL/P population and large variation in psychometric instruments, the current literature on psychosocial functioning in this particular population holds many conflicting findings or broad generalizations. This review aims to summarize the key dimensions of psychosocial functioning, including self-image, social relationships, psychological well-being, behavioral adjustment, and societal stigma. While individuals with CL/P generally report lower self-esteem and higher facial dissatisfaction compared to unaffected peers, there remains some variability in reported outcomes, suggesting that factors such as male gender, positive peer interactions, and self-acceptance of facial appearance can help mitigate low self-esteem. Evaluations of social competence by parent proxies also tend to be harsher than patients’ self-evaluations, thus highlighting the need for self-reported data. Furthermore, measures of social communication should distinguish between speech impediments and assertiveness in communication style. When it comes to behavioral assessment, it is essential for care providers and guardians to distinguish between internalizing versus externalizing behavioral problems, as well as external contributors to negative school experiences in order to provide the most effective support. In order to mitigate anxiety or depression in children with CL/P, it is ideal to minimize the number of surgeries occurring between the ages of 7 to 12 years. Last but not least, increased positive media portrayal has been shown to result in more favorable impressions of patients with facial differences.
As expected, many of these domains may overlap and influence each other, which highlights the need for improved consistency and clarity of specific outcomes. Additionally, while a large portion of the literature focuses on negative outcomes of CL/P conditions, many children and adults with CL/P may not actually experience major psychosocial problems, as evident by studies which report equivalent mental health, social functioning, and socioeconomic attainment compared to the general population. Thus, healthcare providers and researchers should aim to not only report on the deficits of patients, but also shed light on protective measures of psychosocial well-being, such as coping strategies, resilience, community building, and positive attitudes. Certainly, high levels of depression and anxiety does not negate the possibility for high levels of positive outlook and resilience as well. A few possibilities for measuring general resilience include the Brief Resilient Coping Scale (BRCS), the Baruth Protective Factors Inventory (BPFI), and the Resilience Appraisals Scale, although no current studies have utilized these instruments in the CL/P population.93-95 Example statements include, “I look for creative ways to alter difficult situations,” “I have at least one caring person in my life,” and “If I were to have problems, I have people I could turn to.” Despite substantial societal progress regarding disability and facial difference, there remains opportunity for improvement, including increased representation in mass media, recognition of protective traits in the CL/P population, further research on long-term outcomes in adulthood, and incorporation of patients as integral members of the care.
Footnotes
Acknowledgements
This manuscript has not been presented at any professional meetings.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCL is a medical education consultant for Stryker. All sources of funds supporting the completion of this manuscript are under the auspices of the University of California, Los Angeles.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bernard G. Sarnat Endowment for Craniofacial Biology (JCL), the Jean Perkins Foundation (JCL), and the National Center for Advancing Translational Science (NCATS) of the National Institutes of Health under the UCLA Clinical and Translational Science Institute grant number UL1TR001881. The authors declare that there are no conflicts of interest.
Ethical Approval
Institutional Review Board approval was not required.
Informed Consent
Informed consent was not required.