
Abstract
Background:
Osteogenesis imperfecta (OI) is a genetic disorder of impaired collagen synthesis leading to bone fragility and a spectrum of craniofacial anomalies. In this case report, we describe the management of a mandibular fracture in a 19-year-old woman with Type III OI who had several complicating factors, including dentinogenesis imperfecta (DI), and basilar invagination.
Methods:
The patient, presented with mandibular pain and occlusal changes following third molar extractions. Imaging revealed a comminuted fracture of the mandibular angle and ramus. Intraoperatively, the patient’s head was immobilized to avoid exacerbating basilar invagination. Hybrid arch bars were used for maxillomandibular fixation (MMF) to accommodate DI, and occlusion was achieved using pre-injury photographs due to difficulty identifying wear facets. A reconstruction plate placed through a Risdon incision secured the fracture, and the patient was placed in dynamic MMF postoperatively.
Results:
The patient tolerated the procedure well, and subsequent surgeries, including Lefort I distraction, were successfully performed using similar protocols for safety.
Conclusion:
This report underlines the importance of individualized management in OI patients, considering their unique skeletal and dental challenges. It also demonstrates that with careful planning and intraoperative adaptations, such as the use of hybrid arch bars and immobilization techniques, complex mandibular fractures in patients with additional anomalies like basilar invagination can be managed effectively.
Keywords
Introduction
Osteogenesis imperfecta (OI) is a collection of genetic disorders characterized by defective bone formation resulting in skeletal abnormalities and bone fragility. 1 It is the most common form of heritable bone fragility. 2 OI occurs at an incidence rate between 1/10 000 and 1/20 000, with a population prevalence ranging from 2.35 to 4.7 in 10 000 worldwide.3,4 Most cases are due to defects in genes responsible for the production and processing of type I collagen, with a predominantly autosomal dominant inheritance pattern. 5
Phenotypical severity of OI varies from fetal demise to asymptomatic presentations and may include short stature, increased susceptibility to recurrent fractures, and bone deformities. A patient with OI can also present with scleral deformities, facial dysmorphism, hearing loss, and skin laxity. Because of this phenotypic variability, OI is classified into subtypes. Type I exhibits mild or absent bone abnormalities, type II is associated with severe abnormalities resulting in perinatal death, and types III and IV are associated with moderate to severe bone deformities, in addition to growth retardation and frequent craniofacial involvement. 2
Craniofacial features in patients with OI include a triangular face, frontal bossing, broad forehead, deep-set eyes, beaked nose, and malocclusion, with Angle class III being the most frequently observed (Figure 1).6,7 Additionally, teeth can present with dentinogenesis imperfecta (DI), a dentin anomaly that results in teeth discoloration, brittleness, and abnormal crown and root development. 8 Type I dentinogenesis imperfecta is a subgroup of the disorder that occurs only in association with OI. 9 Because OI presents with brittle bones, patients are also susceptible to fractures of the craniofacial skeleton. 10 In mandibular fractures, in particular, the brittle nature of the bones, temporomandibular disorders, and malocclusion increase the repair challenge. In patients with concomitant DI, management is further complicated by an inability to use tooth-borne methods of obtaining occlusion intraoperatively, such as Erich arch bars or interdental wiring.
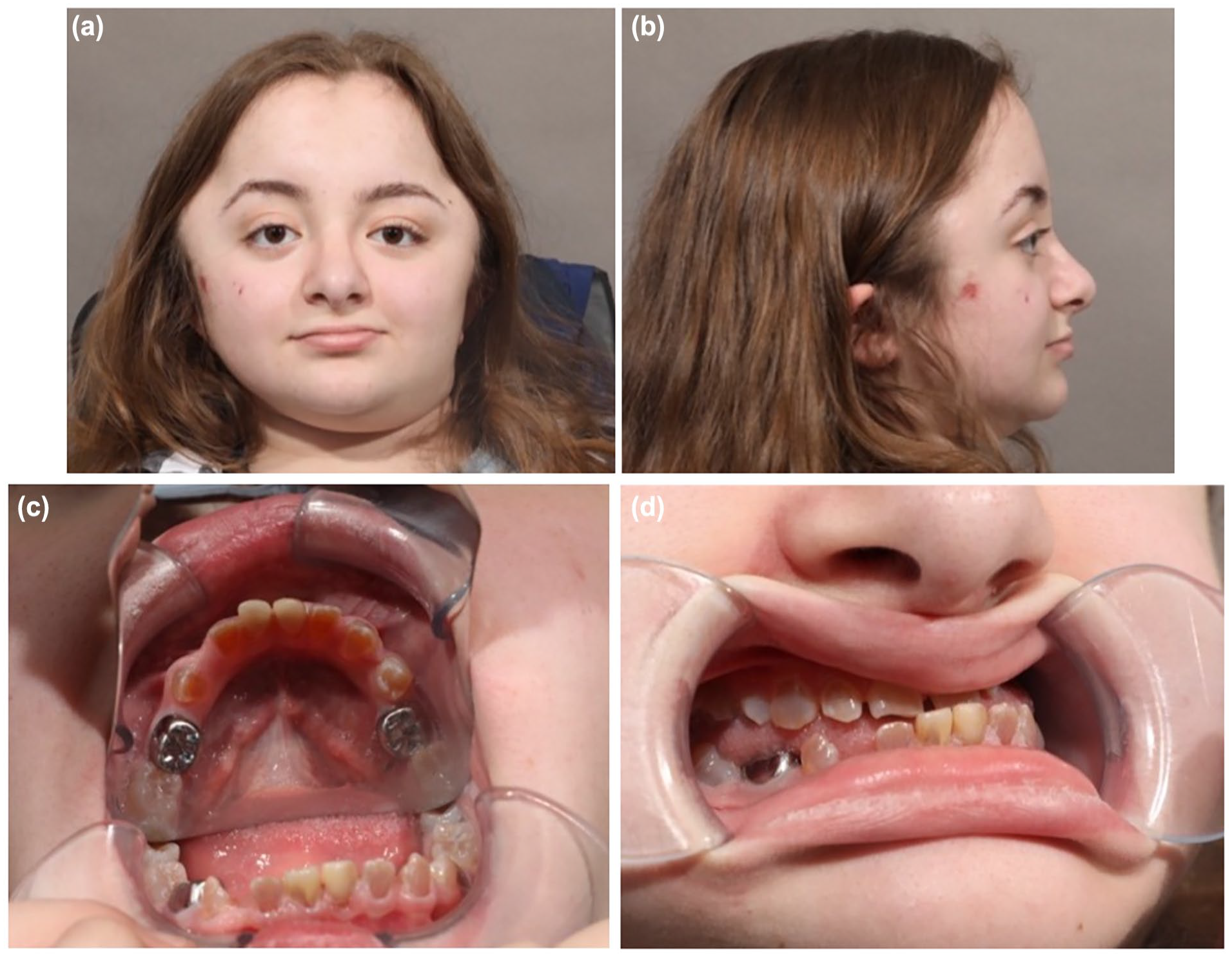
Preoperative patient photographs: (a and b) show a broad forehead and deep-set eyes and (c and d) show the dental anomalies and Angle Class III malocclusion.
Patients with OI may also present with craniovertebral anomalies that can further complicate medical and surgical management. Basilar invagination is one of these, characterized by protrusion of the cervical spine structures, such as the odontoid process into the foramen magnum. 11 Although uncommon, it can result in devastating complications such as brainstem compression, hydrocephalus, and impingement of cranial nerves. 11 Because the movement of the cervical spine can further exacerbate symptoms, basilar invagination becomes a significant challenge during surgery when the cervical spine needs to be manipulated, such as during intubation for anesthesia, where the movement of the neck can result in compression of the vertebral artery.12,13
Reports of management of mandibular fractures in patients with OI have been previously described in the literature.10,14 However, mandibular fracture management in patients with OI can be further complicated if basilar invagination is present, warranting an individualized approach. In this case report, we describe the management of a mandibular fracture in an adult patient with Type III OI with concomitant dentinogenesis imperfecta and basilar invagination, in hopes of guiding surgeons who may encounter this challenging situation.
Clinical History
A 19-year-old woman with a history of osteogenesis imperfecta (OI) type III, class III malocclusion, and over 100 previous long bone fractures presented with a new onset of right mandibular pain and drastic alteration in occlusion during chewing of soft foods. She reported no previous history of facial fractures. One month prior, she had undergone extractions of fully bony impacted third molars by another surgeon. Physical examination revealed tenderness to palpation and edema at the right mandibular angle. A cone beam CT scan of the face showed a comminuted, atypical fracture of the right mandibular angle and ramus/subcondyle (Figure 2).
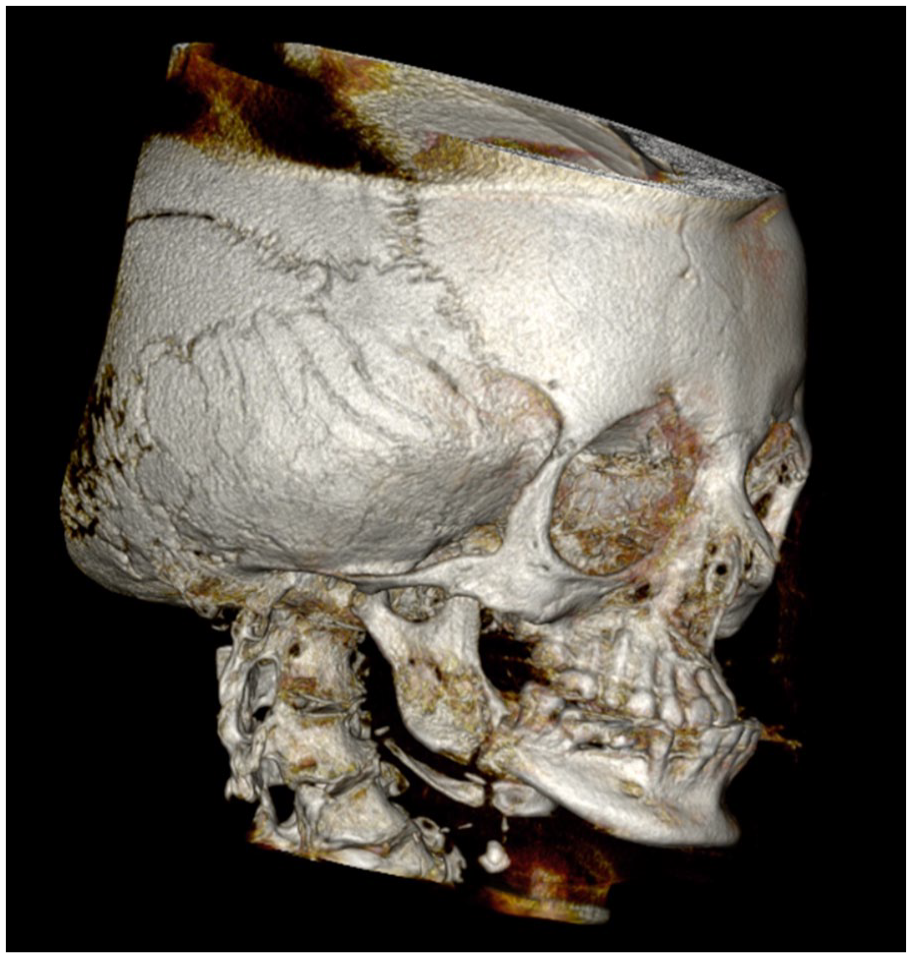
3D reconstruction of CBCT scan with a comminuted, atypical fracture of the right mandibular angle and ramus.
Her medical history included dentinogenesis imperfecta, scoliosis with posterior spinal fusion of levels T2 to L4, chronic gastroparesis, and basilar invagination of the cervical spine. Basilar invagination was significant, with 0.5 cm upward displacement of the tip of the odontoid process above McGregor’s line and 0.4 cm displacement above Chamberlain’s line. The patient also had a Chiari I malformation, making this, by definition, a type II basilar invagination. She had no neck pain and a good neck range of motion on examination.
We recommended open reduction with internal fixation of the fracture, given her malocclusion, and she agreed to proceed with surgery. The patient’s neurologist was concerned about the safety of surgery in the setting of basilar invagination, so her neurosurgeon was consulted and recommended minimizing motion of the neck during surgery.
Intraoperative Course
Due to the significant basilar invagination, the patient’s head was immobilized in a neutral position using sandbags and taped to the operating table, just as one would do for a patient with an unstable cervical spine in trauma. Naso-tracheal fiberoptic intubation was used after the head was immobilized.
To maximize access in the setting of a neutral neck position, an extraoral Risdon incision was utilized. A disorganized callus was found over the fracture site. This was debrided, revealing an angle fracture through the third molar socket. An additional nondisplaced fracture extended up the ramus toward the subcondylar region. Maxillary and mandibular hybrid arch bars (KLS Martin Corporation, Jacksonville, FL) were placed due to the patient’s dentinogenesis imperfecta, which precluded the use of standard arch bars or interdental wires. Fracture reduction was achieved, and the patient was placed into her premorbid class III occlusion based on pre-injury photographs. Given her DI, wear facets were extremely challenging to identify and use for occlusal guidance. A 1 mm miniplate was placed on the inferior border of the mandible to hold preliminary reduction (Figure 3). An intraoperative CT scan was used to verify fracture reduction and identify potential further displacement of the subcondylar fracture and iatrogenic fractures from mandibular manipulation. Definitive fixation was then performed using a 2.0 mm reconstruction plate with bicortical locking screws and transbuccal trocar placement along the ramus (KLS Martin, Jacksonville, FL). MMF was released, and the patient’s occlusion was maintained. The subcondylar extension of the fracture was nondisplaced and too high up the ramus to be easily treated; therefore, the patient was placed in dynamic MMF with heavy elastics. The patient tolerated the procedure without any surgical or anesthetic issues and was discharged on outpatient basis (Figure 4).
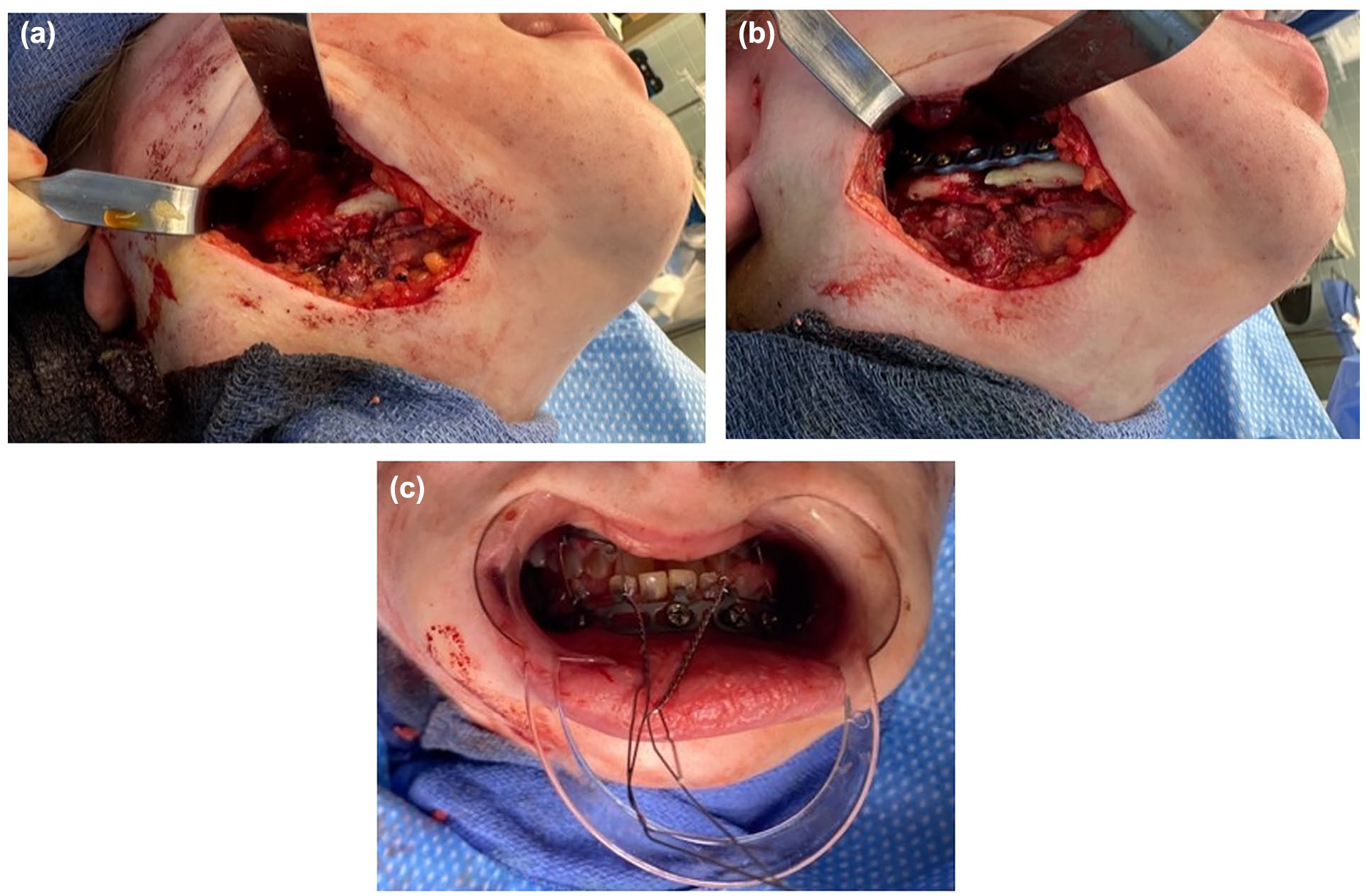
Operative approach to ORIF through an extraoral Risdon incision. (a) lateral view pre-fixation. (b) lateral view post-fixation. (c) hybrid MMF system utilized.

Postoperative photographs following mandibular fracture repair and LeFort I distraction surgery. (a) frontal view. (b) lateral view. (c) maxillary occlusal view. (d) occlusion.
Post-Operative Course
The patient was maintained in tight MMF for 2 weeks, then transitioned to guiding elastics. While in guiding elastics, she had some increased pain, so she was placed in tighter elastics at night. She also had some neuropraxia of her right marginal mandibular nerve, which improved during subsequent clinic visits. Guiding elastics were slowly weaned until 8 weeks postoperatively. A postoperative CT scan was obtained to ensure the fracture wasn’t displaced. However, it did show the superior-most screw in the reconstruction plate was in the sigmoid notch and did not have bone purchase (Figure 5). Because she was asymptomatic from this and had a normal maximal incisal opening, and because a locking screw was utilized, it was decided to leave this in place without intervention. Figure 5 also shows the 3D reconstruction of the CT scan, confirming that the fracture was not displaced.
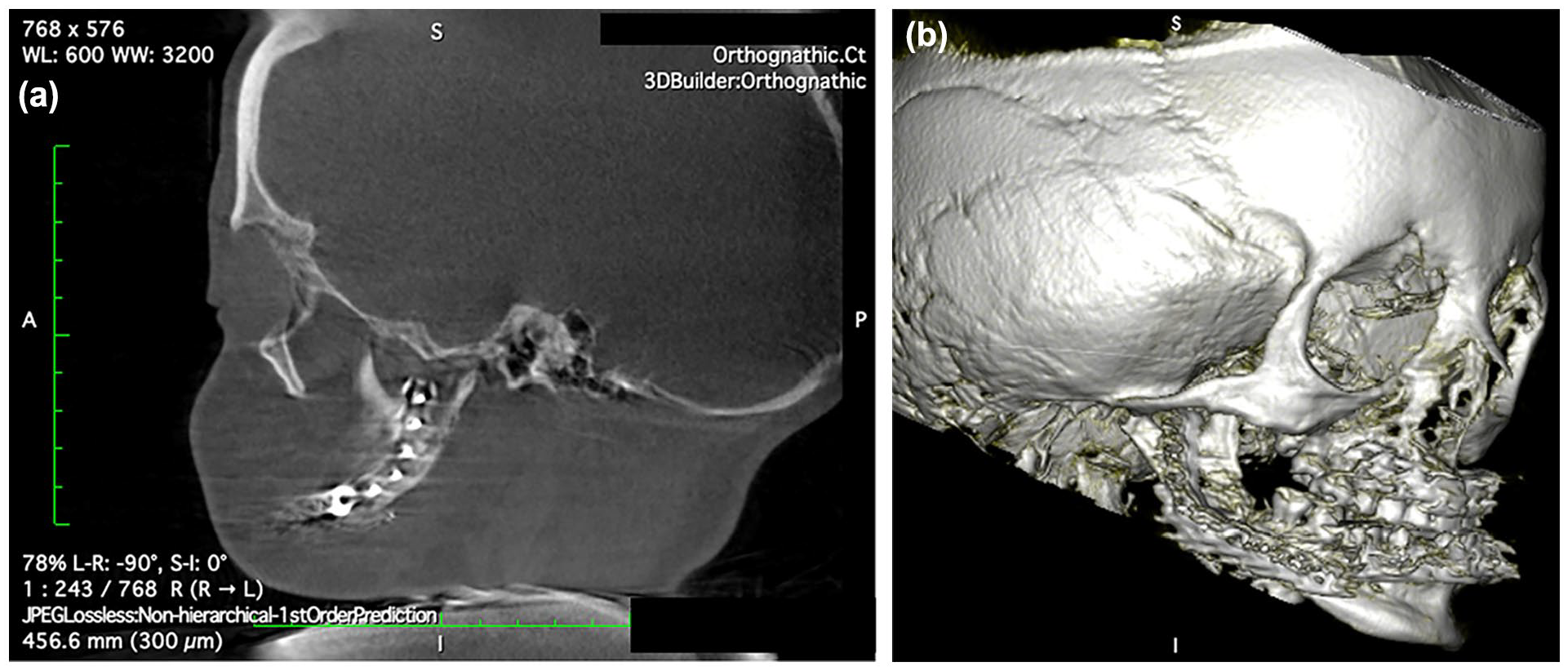
(a) Postoperative CT at 40 days following mandibular fracture repair shows the superior-most screw of the reconstruction plate in the sigmoid notch without any bone purchase. (b) A 3D reconstruction of the postoperative CT is shown here.
Due to the safe execution of this mandibular open reduction and fixation, our multidisciplinary team felt that more elective surgeries could safely be performed using a similar protocol. Approximately 5 months after treatment of her mandibular fracture, the patient underwent LeFort I distraction with an external maxillary distraction frame to primarily repair the significant vertical shortening of her maxilla, as evidenced by the absence of incisal show even when she smiles. DO was used because vertical disimpaction is a relatively unstable move that is prone to relapse. There was particular concern about the limited ability to fixate bone grafts in a patient with OI, so DO was used to provide more stability without the need for fixation. A rigid external distraction (RED) system (KLS Martin, Jacksonville, FL) was used because a significant vertical and transverse distraction was performed. A standard latency of 5 days and extended consolidation of 12 weeks was utilized. Distraction was performed at 1 mm/day, split into 0.5 mm twice daily. Goal of distraction was a slight Class II skeletal relationship and appropriate incisal show in repose, given that we expected some skeletal relapse. Total movement of the A point from pre-op to distractor removal was 10 mm transverse advancement and 11.6 mm vertical disimpaction. At 6 months of follow-up, the patient’s imaging did not show any evidence of skeletal relapse. Routine imaging has not been obtained since that time, but the patient’s occlusion has been stable at 1 year of follow-up since distractor removal. The hybrid MMF system from the mandible fracture was utilized to fixate the splint attached to the external distraction device. This served to both avoid a strictly tooth-borne system which was not suitable to be used due to her DI and to distribute the forces of distraction across many more screws and a much larger thread surface area than would be used with more typical plates for distractor anchorage (Supplemental Figure 6). The halo device was anchored with 5 screws per side which is more screws than what is typically used, and only 1 finger torque was applied for tightening the screws. This was to reduce the risk of potential skull fractures.
Discussion
Mandibular fracture management in a patient with OI requires consideration of the risk factors and additional craniofacial deformities caused by the disorder. Classically, there are 4 subtypes of OI, with type III exhibiting the most craniofacial involvement, including mandibular overjet and class III malocclusion. 2 Prior malocclusion can complicate mandibular fixation during surgery. The fragility of the bone in OI also places patients at a risk of iatrogenic fractures. In this report, we describe the considerations when planning surgical treatment for mandibular fractures in a patient with OI further complicated by basilar invagination and DI.
Patients with OI generally suffer from fractures of the long bones with even minor trauma. On the other hand, fractures of the facial skeleton are rare, estimated from prior studies to be 1% to 2%. 15 This could be due to the immature state of the bone requiring relatively stronger trauma to fracture or the asymptomatic nature of the fractures leading them to being overlooked. 15 Mandibular fractures have been reported in prior case reports to be discovered following a molar extraction.16,17 It has been suggested that the sectioning of the tooth rather than bone removal is recommended to prevent mandibular fractures during molar extraction. 17 Although management of mandibular fractures in patients with OI have been reported before, our management differed based on the experience of prior authors as well as our patient’s specific comorbidities. Several authors have noted previous failures of miniplate fixation, and thus we selected an immediate repair with a locking load-bearing reconstruction plate.18,19Reports that utilized more rigid fixation have achieved better outcomes.18,20Additionally, iatrogenic fractures have been reported during the process of fracture repair, so both a combination of intraoperative imaging and very careful reduction maneuvers were performed to confirm no iatrogenic fracture was created. 19
Basilar invagination is a potentially life-threatening complication in patients with OI. Its reported prevalence within patients with OI varies among different studies, with values ranging between 6.5% and 25%.21 -23 Prior investigations showed that type III OI is the subtype with the highest prevalence of basilar invagination.22,24,25 The wide variation in the prevalence of basilar invagination could be attributed to differences in how it can be defined based on different criteria. Basilar invagination could be defined as a protrusion of the odontoid process more than 5 mm above the Chamberlain line (the line connecting the posterior nasal spine to the posterior lip of the foramen magnum in a lateral cephalogram) or more than 7 mm above the McGregor line (the line connecting the posterior nasal spine to the most caudal portion of the posterior cranial base in a lateral cephalogram). 11 Basilar invagination classification is based on the absence (type I) or presence (type II) of a Chiari I malformation, with type II carrying a worse prognosis. 26 Compression of the brainstem in basilar invagination places patients at risk of neurologic deficits, respiratory depression, and death. 23
Flexion and extension of the neck exacerbate basilar invagination symptoms, so manipulation of the cervical spine during surgery places patients at risk of catastrophic complications. A previous report has described a stroke originating from the compression of the vertebral artery due to neck rotation of a patient with basilar invagination. 13 This creates the need to avoid neck manipulation during surgery, such as when intubation for anesthesia is performed or during surgery involving head and neck structures. In such situations, fiberoptic intubation is described as a preferred technique to ensure the patient’s neck is immobilized. 12 Neck manipulation is often performed during mandibular fracture reduction as well, highlighting the need for evaluation for cervical spine injuries in acute trauma patients with mandible fractures. However, this patient’s case demonstrates that even in the setting of a cervical spine anomaly, a mandibular fracture can be safely addressed if care is taken to ensure the neck is completely immobilized during intubation and surgery.
This patient’s management was further complicated by dentinogenesis imperfecta (DI). The abnormal dentin structure in DI leads to the formation of opalescent, discolored teeth that are often brittle and prone to wear or breakage. 8 Globally, DI incidence ranges from 1 in 6000 to 1 in 8000 individuals. 8 There are multiple subtypes of DI, with type I being always associated with OI. DI is relatively common in patients with OI, with prior reports demonstrating between 10% to 86% of patients with OI also having DI, particularly in individuals with type III OI.24,25 DI teeth can wear down quickly due to the poor quality of dentin, which further complicates the approach to a variety of craniofacial procedures. If left untreated, further tooth deterioration in DI can affect the structure of the facial bones and the functioning of the temporomandibular joint. 27 The patient did not undergo pre-operative orthodontia because we anticipated that orthodontic management might be challenging, and her main complaint was a lack of tooth contact resulting in difficulty chewing. Therefore, a surgery-first approach was taken. Postoperatively, she had a functional occlusion and elected not to undergo further orthodontic care. Orthodontic management is challenging in DI given an inability for traditional fixed appliances to bond to the teeth. Other options have been described, including orthodontic bands, but removeable clear aligners seem to provide the most reliable method of orthodontic movements in these patients.28 -30
The combination of an unstable cervical-occipital joint due to basilar invagination and brittle teeth with malocclusion due to DI required a unique approach to the management of the mandibular angle fracture in our patient. The patient’s complex pathology required modifications when planning the open reduction internal fixation of the mandible. Immobilizing the neck in a neutral position to avoid basilar invagination-related complications was achieved using sandbags and taping the head to the operating table. An immobilized neck can limit access to the fracture, especially if an intraoral incision is used, so an external incision using a Risdon’s approach was utilized. Access to the fracture through a Risdon approach allowed the opportunity to limit both spine extension and rotation while making it possible to increase exposure further if needed, as a large plate was used for fracture repair. Despite offering more exposure with the neck extended, a Risdon approach with the patient’s neck in a neutral position provided sufficient exposure to safely repair the fracture. An intraoral approach would have been challenging due to the small size of the mouth opening and the need for rotating the neck.
Additionally, care was taken not to introduce iatrogenic fractures while repairing the original fracture due to the vulnerable craniofacial skeletal structure. An intraoperative CT scan was performed to inspect if additional fractures were introduced. The risk of iatrogenic mandibular fractures in patients with OI undergoing craniofacial surgery is unknown, probably due to the rarity of cases. However, a prior report did describe the case of a patient who originally sustained fractures of the right mandibular angle and the left parasymphysis, then an additional iatrogenic fracture of the right mandibular ramus while being treated for the others. 19
A traditional tooth-borne approach to MMF would not have been suitable for this patient due to her brittle teeth caused by DI. Decision making regarding MMF in OI has been quite variable in the literature. Traditional Erich Arch bars were used in several reported cases, presumably in patients without DI.18,20 In other cases, wire ligatures in a patient with DI or a custom bonded splint have been used.31,32 IMF screw usage has also been reported. 19 There were several factors considered that led to the use of hybrid arch bars in this patient’s case. Because of the unfixated subcondylar component of the fracture, postoperative elastic management was planned, which precluded the use of wire ligatures. Pediatric wiring techniques, such as pyriform drop wires and circummandibular wires, would have reduced the risk of a screw-related fracture, but would also not allow elastic management. While IMF screws have been successfully used in patients with OI, it was felt that a hybrid system would allow more elastic flexibility as well as distribute the force of elastics over a greater surface area of screws, potentially decreasing fracture risk.18,20
Patients with type III OI exhibit significant craniofacial involvement of the disease, which is consistent with our patient. Rigid load-bearing fixation was utilized, as the structural abnormalities in OI not only lead to brittle bones but can also affect the healing of the repaired fractures. 33 The patient was placed in dynamic MMF with dental elastics for 12 days. A longer duration of MMF could be considered for patients with OI for concern of delayed fracture healing, and careful monitoring of the postoperative period is warranted to ensure no additional fractures were introduced due to the fixation process.
Following the repair of the mandibular fracture, the patient underwent a LeFort I distraction osteogenesis procedure. The patient demonstrated a stable distracted segment. Distraction was used over the traditional advancement with bone grafting to reduce the risk of relapse. The process of bone formation in distraction has distinct characteristics from typical fracture healing. In typical fracture healing of the craniofacial skeleton, a substantial subperiosteal callus forms within 2 weeks, consisting of both chondroid, and immature osteoid tissue. Over the following 2 weeks, this callus is gradually replaced by trabecular bone, which becomes entirely integrated with new blood vessels and Haversian systems. 34 In distraction osteogenesis, a structure called the fibrous interosseous zone forms within the distraction gap. On each side of the fibrous interosseous zone is the primary mineralization front, which contains a high density of proliferating osteoblasts that undergo primary mineralization and form bone columns. The primary mineralization front advances as the distraction progresses from the side toward the center of the distraction gap until the fibrous interosseous zone is also ossified. 34 While patients with OI have abnormal bone physiology and defective collagen structure, the mechanisms of bone healing in OI remain mostly normal, except for a delay in the early stages of healing. 35 This could explain how several case reports have described successful distraction osteogenesis in patients with OI.36 -39 It is also supported by the successful LeFort I distraction osteogenesis results in our patient.
Conclusion
Managing mandibular fractures in patients with Osteogenesis imperfecta (OI), especially with accompanying craniofacial anomalies like basilar invagination and dentinogenesis imperfecta (DI), presents intricate challenges. This case underscores the imperative to tailor surgical strategies to an individual patient’s unique pathology. Recognizing and accommodating these complexities in OI patients is pivotal for achieving favorable outcomes and minimizing postoperative complications. Ensuring safety during the surgery, especially when basilar invagination is present, is paramount. Additionally, adopting specialized techniques, such as intraoperative imaging and hybrid arch bar systems, may be critical for effectively addressing fractures in these patients.
Supplemental Material
sj-jpg-1-fac-10.1177_27325016251342718 – Supplemental material for Management of a Mandible Fracture in a Patient with Osteogenesis Imperfecta Type III with Basilar Invagination and Dentinogenesis Imperfecta: A Case Report
Supplemental material, sj-jpg-1-fac-10.1177_27325016251342718 for Management of a Mandible Fracture in a Patient with Osteogenesis Imperfecta Type III with Basilar Invagination and Dentinogenesis Imperfecta: A Case Report by Sobhi Kazmouz, Kevin Yang, Akriti Choudhary, Hanna Codreanu, Mark E Runge and Chad A. Purnell in FACE
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Chad Purnell is a member of the Editorial Board of FACE and did not take part in the peer review or decision-making process for this submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Informed Consent
Informed Consent was obtained from the involved patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.