
Abstract
Introduction
The zygoma is a quadrangular-shaped bone that forms the lateral cheek prominence. It consists of 3 processes: a maxillary process that articulates anteromedially with the maxilla, a frontal process articulating superiorly with the frontal bone, and a temporal process attaching posteriorly, completing the zygomatic arch. From a functional standpoint, the zygoma is crucial for mastication, serving as the origin of the masseter muscle. Lateral orbital rim/floor integrity and volume are formed by the zygoma. As the articulations of the zygoma form the scaffolding of the surrounding bone and soft tissue, deviations in its position or structure can cause noticeable functional and esthetic deficits.1,2,3 For example, malposition of the zygoma can lead to facial widening, enophthalmos, and other defects that distort the natural facial structure. 3 These defects may alter esthetics by changing the classic face shape triangle, from the lateral canthi to tip of the nose, which aids in facial recognition, and tracking. 4 In cases of zygoma malposition and/or malformation, Zygomatic Osteotomy and Repositioning (ZyOaR) may be necessary to achieve both functional and cosmetic goals.
Zygoma malposition or malformation may be the result of multiple etiologies, which can be categorized as either exogenous or endogenous (Figure 1). Acute traumatic displacement with improper healing is the predominant exogenous cause of zygoma malposition.1,5 Orbitozygomatic complex fractures are common and proper anatomic reduction and fixation can be challenging. They often occur in conjunction with injury to surrounding bones and soft tissue, which may increase the risk of acquired zygoma malposition from incorrect healing.1,3 Congenital conditions causing skeletal or soft tissue overgrowth, such as Treacher-Collins Syndrome and Sturge-Weber Syndrome, are important endogenous causes of zygoma malposition. Other endogenous causes may result from gross underlying deformities, such as distorting neurofibromas of the orbit and surrounding area. Such pathologies may alter the volume of other important structures, such as the orbit, due to the articulation points of the zygoma.6,7
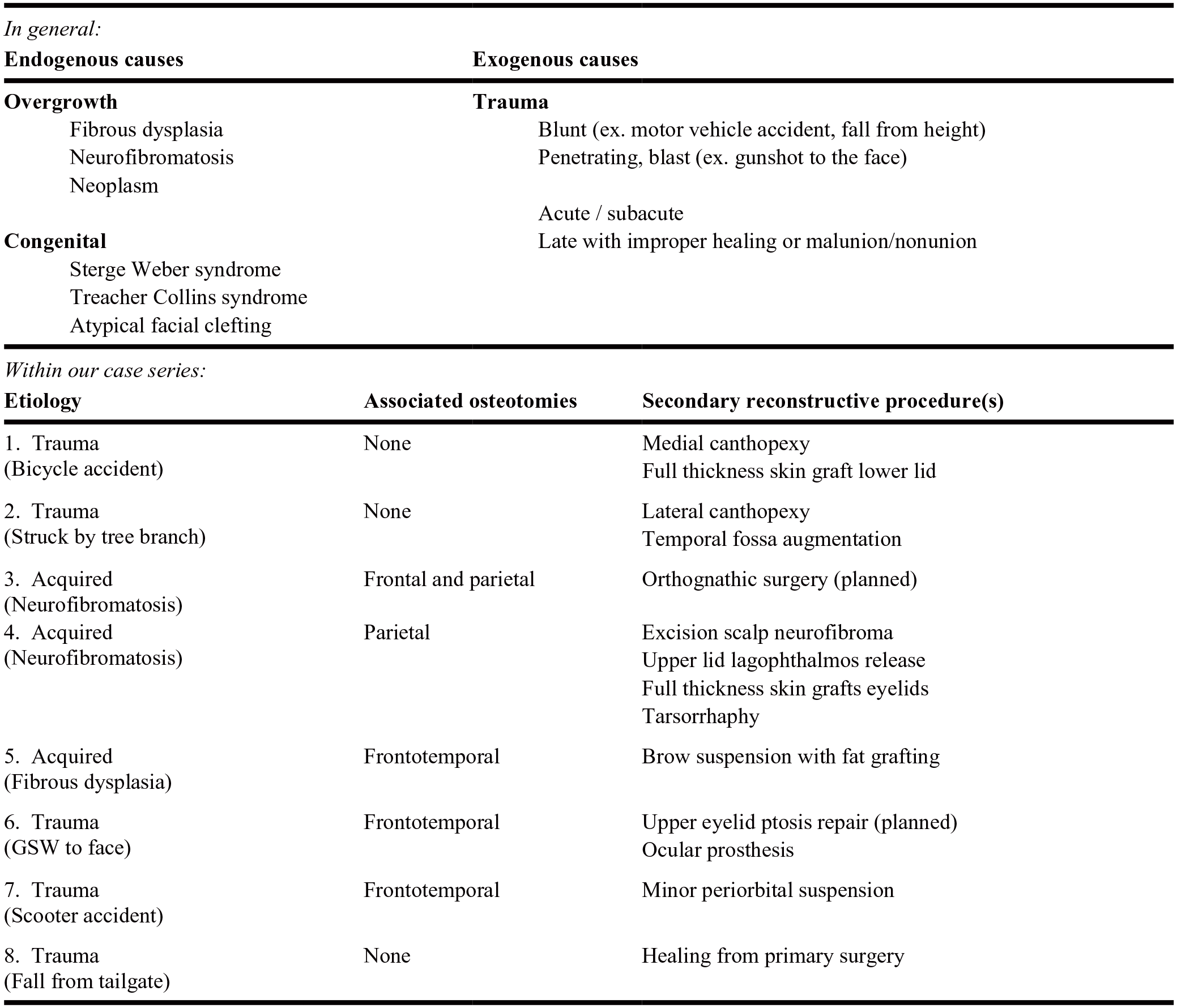
Etiologies of zygoma malposition and/or malformation and reconstructive procedures (in addition to zygomatic osteotomy and repositioning) involved in addressing the deformity.
Zygoma malposition or malformation is not uncommon, owing to its many potential etiologies, with post-traumatic malpositioning being most appreciated clinically. However, an algorithmic approach to ZyOaR has not been well described, and there is not a singularly established technique to address all inherent challenges. The anatomic context, critical functions, and often complex alterations involved in zygomatic anomalies requiring correction make ZyOaR a particularly challenging procedure that demands careful planning and patient-specific technical considerations. Advancements in available technology have recently provided a potential answer to some of these challenges, especially in the form of virtual surgical planning (VSP) as well as customizable guides and implants.
Use and advantages of virtual planning, 3D modeling, and customizable implants have been described in craniofacial surgery broadly, with applications from orthognathic surgery to cranioplasty.8-11 These technological aids may improve operative efficiency, optimize implant design, increase reproducibility, and aid in surgical fidelity. There are few reports of VSP use specifically applied to zygoma malposition or malformation requiring ZyOaR. Mentions of its use in this setting are limited to theoretical addition of computer-assisted techniques to concurrently plan zygomatic reconstruction with iliac bone crest and introduce titanium mesh, providing long-term functional and esthetic benefits for patients.12,13,14 However, to date, there have been no clinical studies describing the use of VSP in both preoperative mapping, creation of custom surgical guides, and patient-specific implants for this application. The following study, therefore, aims to describe our algorithmic approach to ZyOaR using VSP for cases of zygoma malposition/malformation, and represents to our knowledge, the first clinical case series on this topic.
Methods
This study was conducted in accordance with the University of Texas at Austin Institutional Review Board, and a waiver of informed consent documentation was granted. We performed a clinical case series reviewing all adult patients who underwent ZyOaR at our institution by the senior author from January 2010 to September 2024. We included all patients who underwent ZyOaR for malpositioned and/or malformed zygoma and investigated the etiology in each case. All patients were skeletally mature at the time of ZyOaR. Patients with zygomatic malposition in the acute initial trauma setting were excluded. Data were collected on patient demographics, physical exam findings, preoperative diagnoses, surgical documentation, and postoperative follow-up time. Esthetic outcomes, future planned surgical interventions, and functional deficits were also documented. Surgical planning included a complete facial and soft tissue analysis as well as a review of computed tomography (CT) scans and an assessment of bony anatomy. VSP and the creation of custom surgical guides and titanium implants were used in all described cases. Patients provided consent for photography and publication.
Case 1: Trauma
A 59-year-old male who suffered a bicycle accident resulting in a fracture of the left zygoma, left orbit, and left frontal sinus underwent open reduction and internal fixation (ORIF) at an outside hospital. He presented to our clinic 3 years status post ORIF complaining of facial asymmetry, palpable hardware, diplopia (Figure 2, left). On exam, the patient had left brow ptosis, left hypoglobus and enophthalmos, lack of cheek support, a widened face, and protruding hardware from previous operations. CT scan revealed a malreduced, comminuted zygoma fracture with an enlarged orbit and frontal sinus fracture (Figure 3). The patient underwent successful ZyOaR using operative deliverables (custom guides/implants) derived from VSP. Concurrent frontal sinus and lateral orbital wall reconstruction was also performed (Figure 4). At the primary reconstruction a left subperiosteal facelift was performed to correct lid ptosis. Secondary reconstruction consisting of lateral and medial canthopexy with lower lid release and skin grafting was performed several months later (Figure 2, right). Comparison of final postoperative CT against preoperative virtual planning demonstrates a high degree of surgical fidelity (Figure 5).

Case 1: Preoperative (left) and 2-month postoperative from secondary soft tissue surgery after ZyOaR surgery.
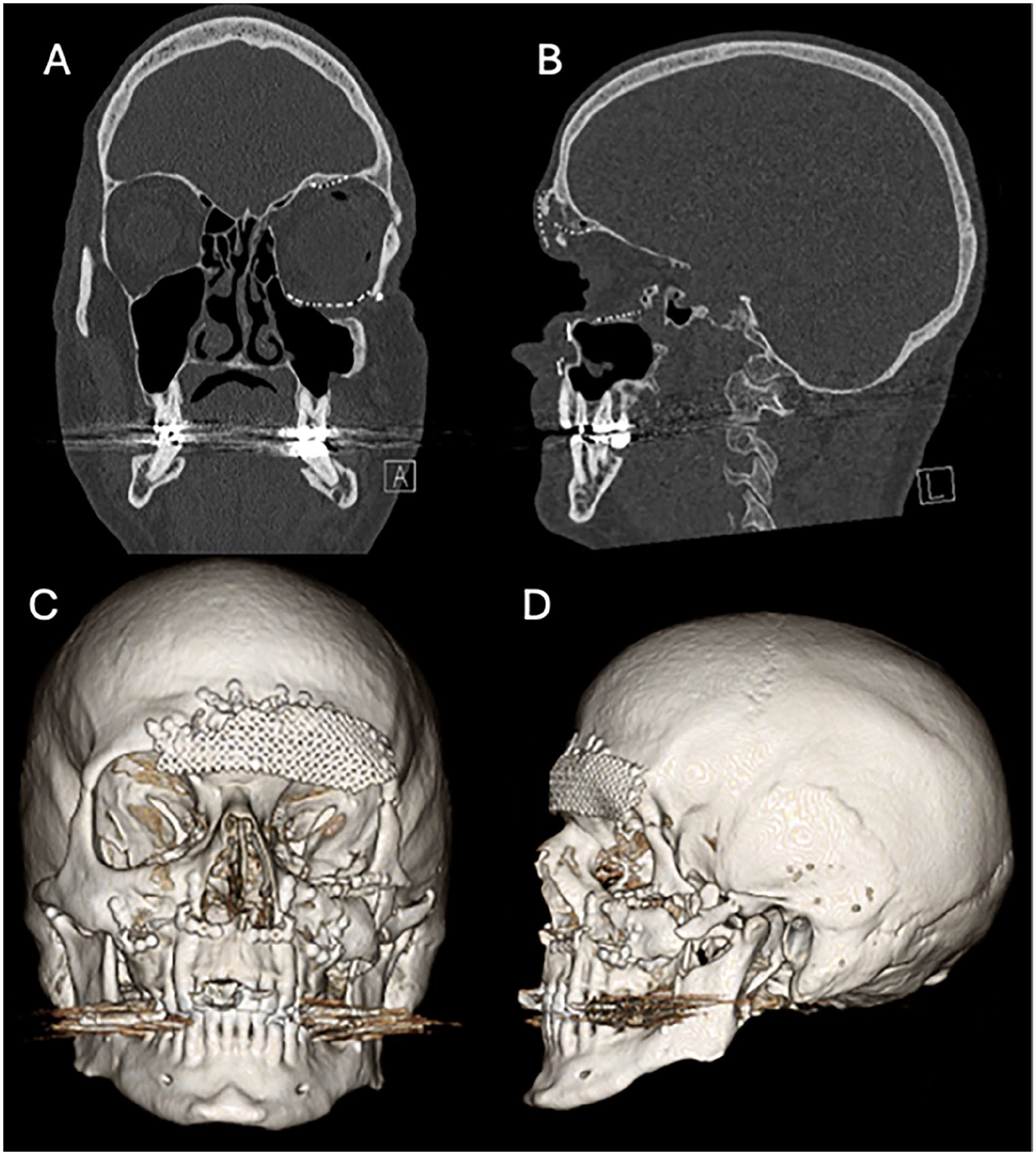
Preoperative coronal (A) and sagittal (B) CT scan cuts as well as CT 3D reconstruction (C and D) images of patient in case 1.
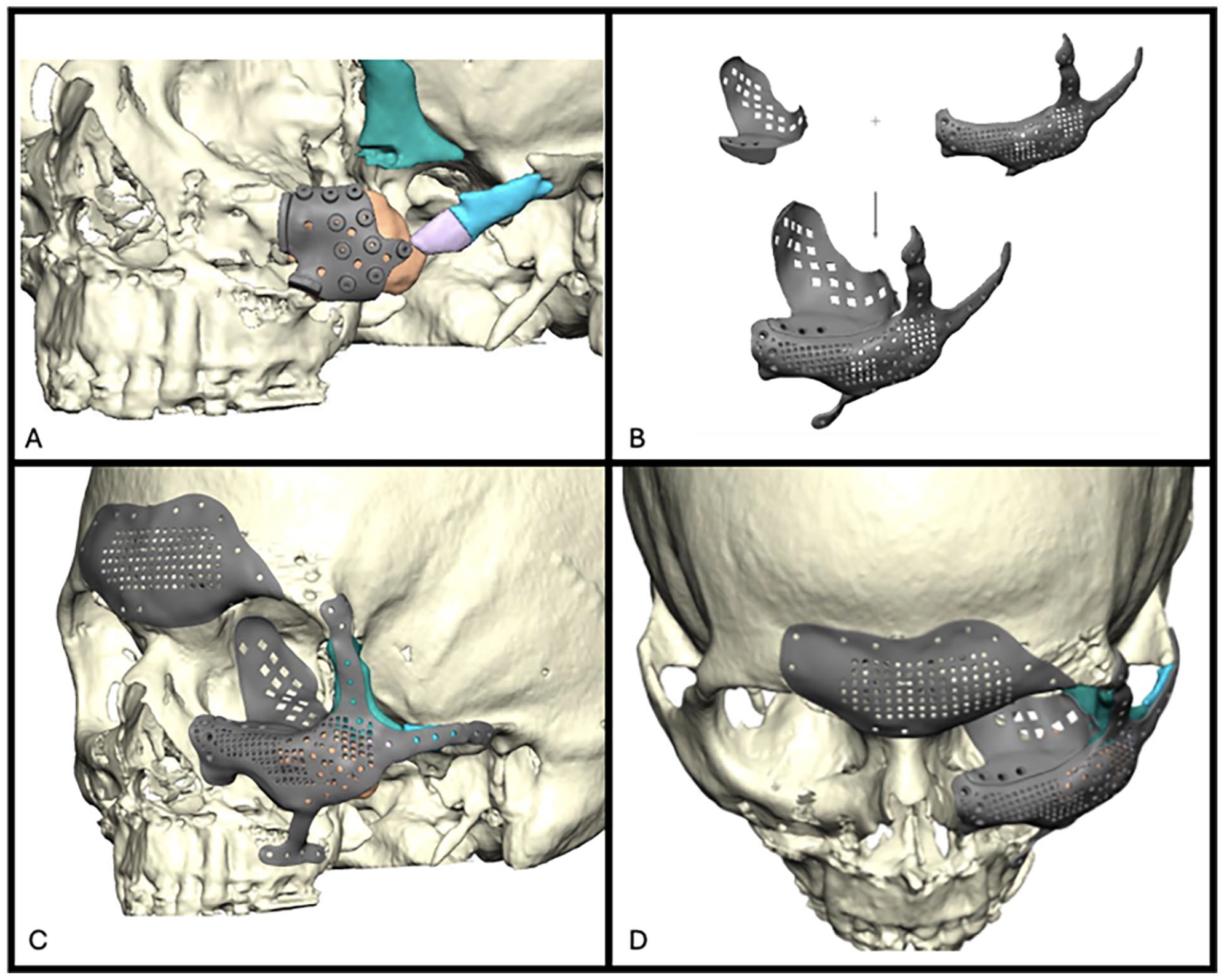
Custom titanium surgical cutting guide (A). Interlocking custom titanium zygomatic and intra-orbital implants (B). Preoperative planning with the custom implants (C and D).
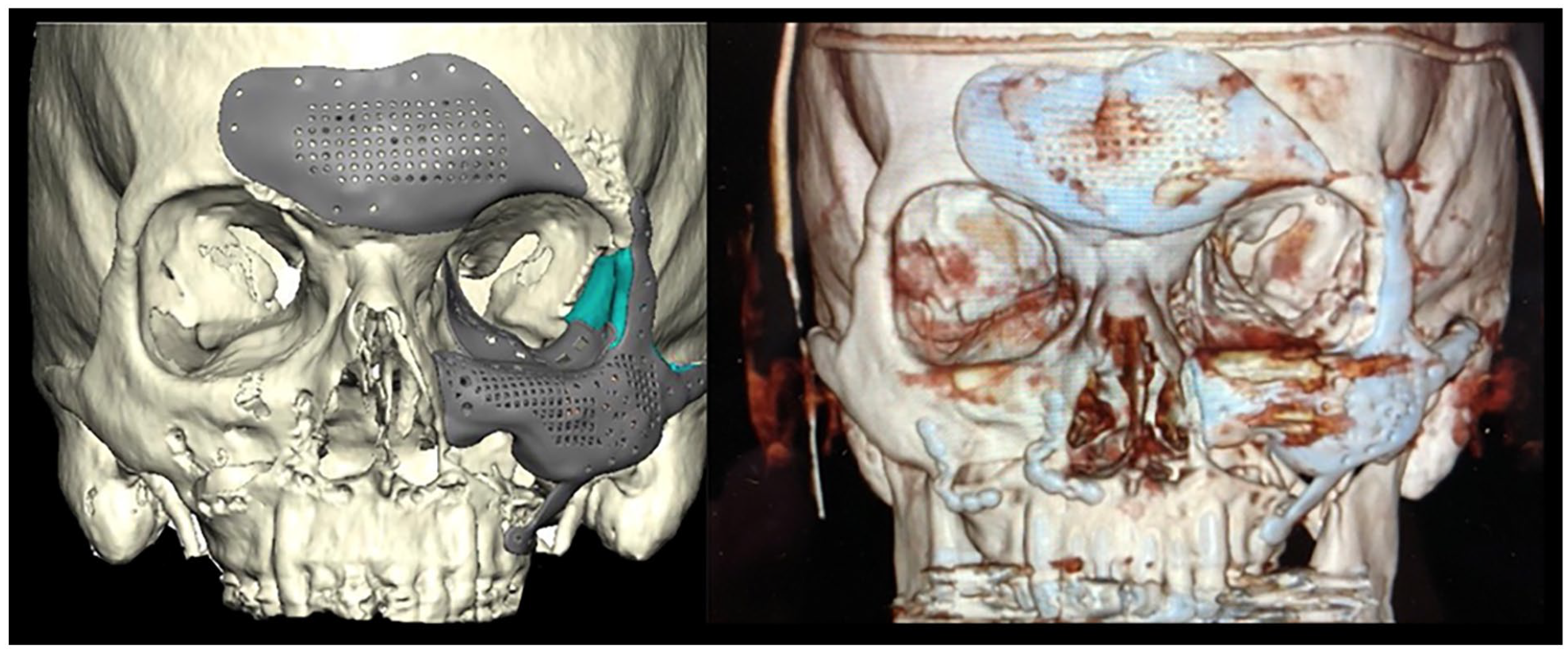
Case 1: (left) preoperative VSP plan and (right) postoperative CT scan.
Case 2: Trauma
A 30-year-old male was struck by a tree branch and sustained extensive craniofacial trauma, including right frontal, parietal, occipital, temporal, zygomatic arch, and orbital floor fractures. Patient underwent ORIF of the zygomatic complex with accompanying reconstruction of the medial orbital wall with a titanium implant. Follow-up exam 5 years after initial operation revealed persistent enophthalmos. With malpositioned zygoma demonstrated on CT. Surgical exposure included reopening the coronal incision, along with stealth facial incisions. ZyOaR was completed. The orbital floor was reconstructed with a custom titanium implant. A year later, the patient underwent right lateral canthopexy to correct residual laxity.
Case 3: Acquired
A 17-year-old male with craniofacial neurofibromatosis type II presented to our clinic with difficulty masticating and left-sided facial droop. Exam revealed left soft tissue excess, occlusal cant, left periorbital fullness, and increased facial width. CT scan revealed malpositioned/malformed cranium/supraorbital margin, orbit, and zygoma. The patient underwent both ZyOaR and neurofibroma excision to reshape and decrease orbital volume. using a coronal and facial stealth incisions. Trans-nasal wire medial canthopexy was also performed. There were no postoperative complications. Orthognathic surgery is planned at a second stage to correct occlusal cant.
Case 4: Acquired
A 55-year-old female with a history of neurofibromatosis status post multiple neurofibroma excisions of the scalp, forehead, and periorbital region, presented to our clinic with visual obstruction due to recurrence of forehead neurofibroma. Physical exam showed a mass in the lower left forehead with left lateral canthal dehiscence and brow ptosis. CT scan showed absence of the left orbital superio-lateral wall, and zygomatic malposition. Patient underwent neurofibroma excision of the face and scalp, as well as ZyOaR. A reconstructive PEEK implant was placed into the orbital region and the zygoma was then moved to its anatomically correct location. Secondarily, the patient underwent successful left lateral canthopexy and left upper lid full-thickness skin grafting.
Case 5: Acquired
A 21-year-old female with a history of fibrous dysplasia status post previous resection in Africa, presented with lower forehead purulence secondary to open frontal sinus injury. Initially she underwent frontal sinus cranialization, with anterolateral thigh free flap. Following initial infection treatment, she was evaluated for secondary reconstruction. CT scan showed mild remaining dysplasia in the left sphenoid and ethmoid bones, with zygomatic malposition/malformation and hypoglobus. Patient underwent ZyOaR, reconstruction of left orbital bandeau and frontal cranium with PEEK implant, and left enophthalmos correction with a custom titanium implant. Post-operatively the patient had a left brow descent with impairment of upward gaze vision but improved left orbital contour and symmetry. Patient later underwent secondary brow suspension with dermal fat grafting to the left temporal region.
Case 6: Trauma
A 19-year-old male suffered a gun-shot wound to the face/head with emergency hemi- craniectomy, ORIF of right periorbital fractures, and right eye enucleation. Five months later, the patient presented for cranioplasty evaluation. CT revealed hemispheric cranial defect along with a malpositioned zygoma/orbit. Patient underwent simultaneous right temporoparietal alloplastic cranioplasty, osteotomies of the right lower frontal orbital bone with ZyOar, along with reconstruction of the orbital roof, lateral wall, medial wall, and floor with custom implants. Patient is awaiting upper eyelid ptosis repair.
Case 7: Trauma
A 42-year old male with a history of motorized scooter accident leading to ORIF of facial fractures and decompressive hemicraniectomy. Upon presentation to the clinic to evaluate for cranioplasty, the patient was noted to have significant hypoglobus and enophthalmos. CT revealed cranial defect and malpositioned zygoma. Patient underwent left frontal-temporoparietal alloplastic cranioplasty with an associated ZyOaR, left orbital floor and medial wall reconstruction with custom implants, and left supraorbital rim/frontal bone osteotomy and repositioning.
Case 8: Trauma
A 60-year-old female presented over 1 month after left zygomaticomaxillary complex fracture sustained from fall. . On exam, she exhibited facial nerve weakness likely from muscle tethering and scarring over the fracture site. CT revealed zygoma fracture/malposition and early bone bridging. ZyOaR was planned utilizing VSP. A coronal incision, with facial stealth incisions were used for exposure. A custom cutting guide and 3D plates were used to achieve osteotomies and final zygoma positioning and fixation. Patient is currently healing from primary surgery, may require minor secondary reconstructive procedures but none yet planned at this time.
Results
Five male and 3 female patients ages 18 to 60 years old (mean = 38) with malposition and/or malformed zygoma met our inclusion criteria. Both exogenous and endogenous causes were included (5 trauma, 3 acquired). Follow-up time ranged from 1 to 50 months (mean = 17 months). No intraoperative complications or postoperative infections occurred. At the time of last follow-up, no postoperative complications, including the removal of implants, were noted. All of our patients underwent secondary reconstructive surgery following ZyOaR, including brow suspension, fat grafting, skin grafting, augmentation of the temporal fossa, medial canthopexy, upper lid lagophthalmos release with lid retraction repair, and lateral canthopexy (Figure 1). No functional defects in mastication or vision change secondary to globe malposition were recorded following ZyOaR. In all patients, preoperative VSP images were compared with postoperative results, showing a high degree of fidelity.
Discussion
Osteotomy and repositioning of the zygoma is challenging due to complex 3D anatomy, multiple bony articulations, intricate soft tissue overlay, and potentially limited surgical exposure. Malposition or malformation of the zygoma can result in functional and esthetic consequences.3 -5 Zygomatic Osteotomy and Repositioning (ZyOaR) is a procedure that aims to restore ideal form and function. In this study, we presented 8 cases of ZyOaR, all achieving successful bony repositioning and proper soft tissue management. Consistent results in ZyOaR based on our series were related to several factors: detailed preoperative analysis, use of virtual planning and creation of custom operative deliverables, accurate intraoperative execution of plan using clinical transfer tools including guides/custom fixation, and staged soft tissue reconstruction. Figure 6 demonstrates our algorithmic approach.
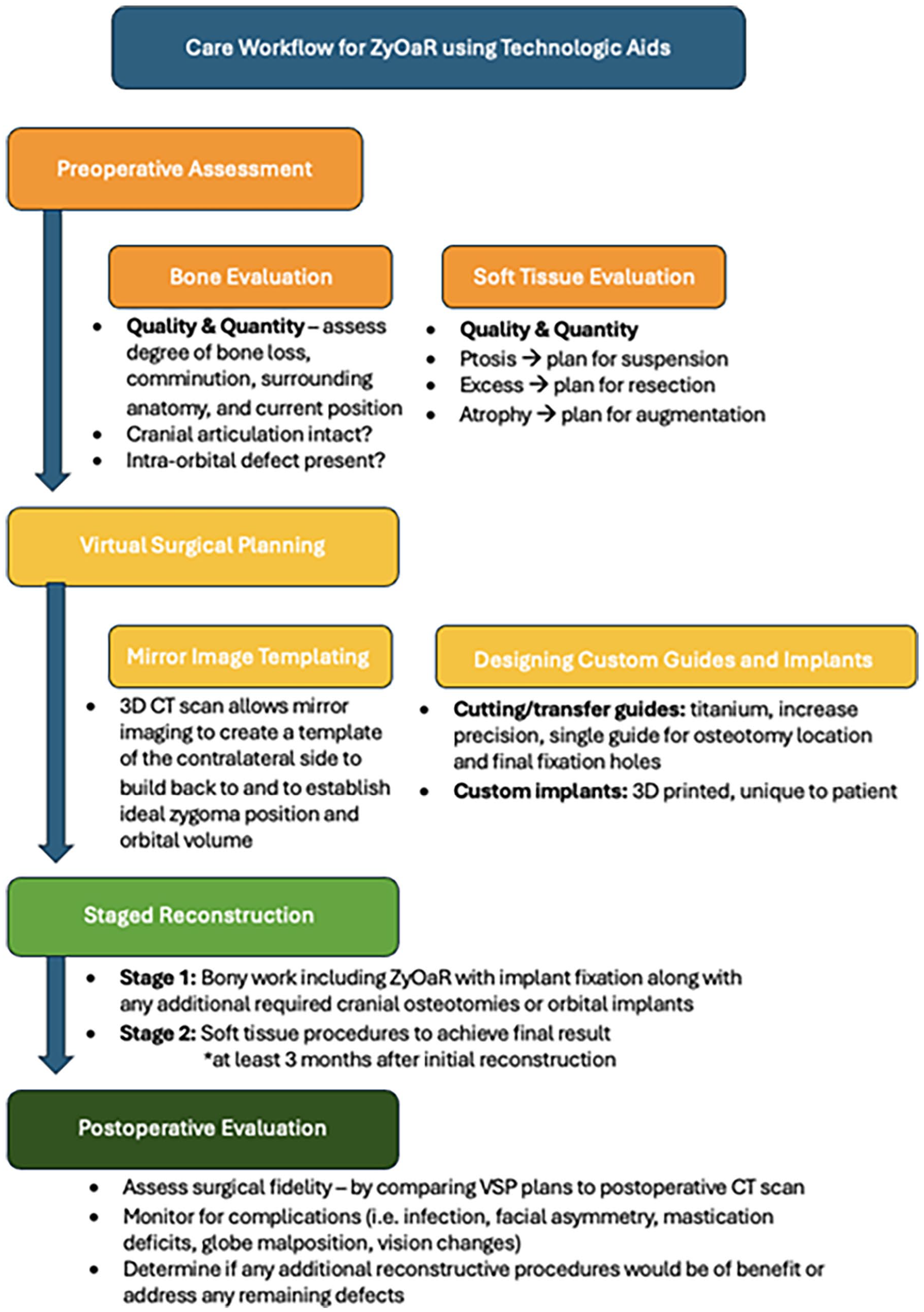
Care workflow for planning and performing ZyOaR utilizing technologic aids including VSP and custom surgical guides and fixation.
Preoperative Analysis
An imperative first step in surgical planning is understanding the specific defect of each patient, starting with a history and timeline, physical examination, and imaging. Preoperative planning is especially important in a patient with zygomatic malposition/malformation, as specific identification of the bony and soft tissue deformity is paramount. Pertinent historical considerations include the etiology of the defect, potential changes in the defect over time (ie, neurofibromatosis, fibrous dysplasia), and the patient’s functional and esthetic goals. On examination, soft tissue analysis is thoroughly completed, with specific emphasis on quantity and quality. Globe position and orbit size should be assessed, noting the presence of entities like hypoglobus or enophthalmos. Detailed bone analysis is achieved using VSP. Visualization of the ideal form using mirror imaging, aids in determining the operative approach and improves understanding of the surrounding morphology. This technology has been shown to improve outcomes and increase patient safety and satisfaction.9,11,15 During preoperative analysis, we followed a “peripheral to central” approach, starting with the zygoma’s articulation with the cranium and other bones. To achieve the proper anatomic location of the zygoma, an assessment of the adjacent bony structures has to be performed. If the frontotemporal articulation of the zygoma is malpositioned, then craniotomy and frontal repositioning are considered. This concept is applied to the other articulating bones in the zygoma.
Once proper adjacent bony anatomy is confirmed or planned using VSP. Mirror imaging is utilized to achieve optimal zygomatic position. Given the zygoma’s importance in orbital morphology and intra-orbital volume, attention should be given to perfecting the walled boundaries of the intraconal contents. Again, mirror imaging is used to achieve an ideal orbital form. Often these patients have increased orbital volume before surgery. After external orbital anatomy is planned, custom implants for the walls/floor of the orbit are designed.
Clinical Transfer Tools and Custom Fixation
Technological aids have evolved significantly over the last 20 years, allowing for increasing precision in procedures involving complex craniofacial osteotomies, including ZyOaR.12,13,16–18 VSP has revolutionized the ability to conceive, and plan complex craniofacial procedures. With the simultaneous advancement of manufacturing capabilities of surgical guides and implants, taking a virtual plan to the operating room and maintaining accuracy, has been enhanced. In earlier days of VSP, 3D printed plastic marking and separate positioning guides were often used to reference an osteotomized segment of bone. However, with the development of 3D printing of custom fixation and the evolution of titanium guides, a single guide has replaced the need for 2 separate guides. Modern guides, typically manufactured in titanium, will register both osteotomies, and predictive holes for final implant fixation. The custom 3D hardware essentially replaces the positioning guide of the past.
Deformity visualization in 3D and virtual osteotomy performance enables the creation of 3D-printed titanium implants that are customized to each patient’s specific pathology. For example, one of our cases utilized an orbit and midface implant, which interlocked to form a stable orbit base and normalize facial width. Prior studies show that custom implants not only improve functional and cosmetic outcomes but also reduce operative time due to the ease of placement.19,20 Historically, clinical transfer tools, such as cutting and drilling guides, were made of plastic materials (ie, thermoplastic resin). 21 However, in many of the presented cases, we used titanium surgical guides. Plastic is inherently more flexible and therefore requiring a thicker, bulkier design to maintain its strength, making use of stealth facial incisions more difficult. The increased strength-to-weight ratio (calculated by dividing a material’s strength by its mass) and sleek design of titanium allow for lower profile registration, making it better suited for limited access surgical approaches. 20 Additionally, titanium cutting guides withstand the saw blade, which decreases the risk of an inaccurate osteotomy (sometimes seen with plastic guides).
Specific surgical approaches using low profile custom titanium guides are largely patient-dependent. In patients undergoing revision surgery, it may be logical to reopen prior incisions. However, when possible, we prefer stealth incisions for ZyOaR procedures. These discrete incisions may offer better cosmetic outcomes and decrease recovery time. Still, appropriate access is paramount; the surgeon should remain open to approach options to ensure optimal visibility.
Intra-Orbital Reconstruction
Following proper external orbital reconstruction, all patients underwent primary intra-orbital reconstruction. Custom orbital implants, which have been virtually planned, can be inserted and fixated to the infraorbital rim, correcting hypoglobus and enophthalmos. Custom implants are recommended in ZyOaR due to the complexity of orbital bony anatomy change, allowing for accurate final volumetric sizing. Intra-orbital implants which interlock with external fixation are preferred, further increasing accuracy.
Additional Considerations
Anatomic alignment of the zygoma may require repositioning of associated articulated bones to achieve proper morphology. Most patients with zygomatic fractures have extensive damage to the surrounding tissue and bony components of the face. In our case, most of our patients had global skull defects including the frontotemporal or parietal bone. A clear understanding of surrounding bony damage is vital to ensuring optimal long-term outcomes in patients.
After achieving anatomic skeletal positioning, soft tissue overlay was addressed. Malar soft tissue suspension to the repositioned orbital rim was paramount as a first step to achieving ideal external appearance. Drill hole lateral canthopexy was also performed. Soft tissue resection was sometimes necessary before re-draping in cases of soft tissue excess, that is, neurofibromatosis.
Following at least 3 months of healing, patients underwent secondary procedures. Soft tissue correction requires an understanding of muscle/connective tissue integrity as well as desired skin fullness, and this could not be fully ascertained until adequate healing time after the bony repositioning. In all the presented cases, secondary soft tissue and/or bone procedures were performed to improve functional and esthetic outcomes. Most commonly, these corrections consisted of periorbital reconstruction in the form of canthopexies, lid release, and skin grafting.
Study Limitations
The case study design relies heavily on historical documentation, which may be incomplete and inaccurate. In addition, our study contains a small sample size and may therefore lack generalizability. Last, no objective measurement data, including comparison measurements between VSP images and postoperative outcomes, were utilized.
Conclusion
Zygomatic osteotomy and repositioning (ZyOaR) is an inherently challenging procedure with complex 3-dimensional anatomic factors dictating issues of facial form and function. Based on our review, comprehensive patient analysis followed by the use of virtual surgical planning, custom operative guides/plates, and follow-up secondary procedures yields an approach that achieves accurate results in ZyOaR. This is the first clinical case series reporting ZYOaR using technological aids to improve surgical performance and postoperative results.
Footnotes
Acknowledgements
Not applicable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Raymond Harshbarger is a member of the Editorial Board of FACE and did not take part in the peer review or decision-making process for this submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study involving human participants were reviewed and approved by the Health Sciences Institutional Review Board at The University of Texas at Austin.
Consent to Participate
A waiver for obtaining written informed consent was obtained by the Health Sciences Institutional Review Board at The University of Texas at Austin prior to study initiation.
Informed Consent
A waiver for obtaining written informed consent was obtained by the Health Sciences Institutional Review Board at The University of Texas at Austin prior to study initiation.
Data Accessibility Statement
All data collected and reviewed for purposes of this study was included directly in the manuscript. We are pleased to provide any additional clarification and/or address any questions through written or email correspondence.