
Abstract
Introduction
Even small scars or alterations to the face after facial burns can have a detrimental effect on a patient’s quality of life, making the minimization of visible sequelae a primary goal of facial burn care and reconstruction.1,2 Compared with other anatomical regions of the body, facial burns have unique characteristics due to the visibility and potential for significant functional impairment. Anatomical features and natural defense mechanisms, such as reflexive protection of the face with hands, the typical absence of protective clothing on the face (allowing for rapid removal of burning substances), and robust blood supply, dissipate heat and reduce exposure time resulting in decreased thickness burns than other anatomical locations. 1 Nevertheless, facial burns are generally more severe due to frequent association with inhalation injuries, need for specialized surgical interventions, and increased risk of psychosocial impairment.1,3 Adolescent survivors of head and neck burns, in particular, place emphasis on cosmetic outcomes, experience distress from physical appearance changes, and have significantly worse satisfaction with appearance scores than their peers without burns. 4 Similarly, adults experiencing alterations in body image perception post-burn report decreased psychosocial functioning, especially in cases with high total body surface area burns. 5
As overall burn-related mortality continues to decrease, long term sequelae of burns, such as reduced quality of life, dissatisfaction with appearance, scar numbness, joint pain, heat intolerance, hearing loss, change in voice, vision problems, post-traumatic stress, and swollen extremities, are becoming increasingly prevalent.4,6 Both pediatric and adult minority burn survivors are at higher risk for long-term complications which frequently results in higher rates of depression, fatigue, sadness, increased pain, and lower levels of community integration.5,7-10
Prevention of these chronic sequelae begins at initial presentation and admission to the emergency department (ED). Initial management of facial burns includes acute airway management, wound management, and operative planning. 11 With the recent improvements in wound care mortality, the focus has shifted to decreasing the impact of short- and long-term complications. Effective prevention of facial burns is arguably the most direct way to decrease long-term sequelae. Preventive efforts require identification of at-risk groups and thorough understanding of current epidemiological trends to develop and evaluate targeted prevention campaigns.
This study aims to quantify the incidence of facial burn presentations to United States emergency departments from 2014 to 2023 and to identify common causes of facial burns across different demographic groups, thereby providing foundational data for the development of focused facial burn prevention initiatives.
Materials and Methods
Materials and Methods
The National Electronic Injury Surveillance System (NEISS) database is a statistically validated surveillance system operated by the United States Consumer Product Safety Commission (CPSC). The NEISS database collects data on consumer product related injuries from 100 hospitals considered representative sample of all emergency departments in the United States. At NEISS hospitals the NEISS coordinator reviews emergency department records coding the injury based on the emergency medicine physician’s diagnosis at time of presentation. Each injury is entered into the NEISS database including the patient age, gender, ethnicity, injury diagnosis, affected body parts, incident locale, brief narrative description of the incident, and consumer product involved.
Search Criteria and Analysis
The NEISS database was queried for all burn types (scald, thermal, chemical, electrical, and radiation) resulting in facial injury from 2014 to 2023. Thermal burns in this case are defined as burns from flammable liquids that ignited, burns caused by touching a hot surface, or chemical ignited causing injury from resulting flame. The query included injuries to the face only, defined by NEISS to include eyelid, eye area, nose, and forehead (NEISS Code: Face). Scalp, ear, eyeball, mouth, and neck were not included in this query. Each event is treated as a unique datapoint, and the most severe injury cause is what is documented. This severity measure applies to the affected body part as well, with the most severe or 2 most severe body parts documented. The NEISS database is publicly available, so this study is IRB-exempt. Data queried and extracted was initially evaluated using Microsoft Excel. Raw reported data was analyzed, and results are reported as incidence in the sample 100 NEISS hospitals unless otherwise stated.
The age demographic cohorts were defined using the Munich Age Classification System (MACS) for emergency patients. 12 These were defined as neonate (up 27th day of life), infant (30 days-12 months), toddler (13 months-2 years), early childhood (3-5 years), late childhood (6-11 years), adolescent (12-17 years), and adult (older than 17 years). Aggregate comparison of pediatric (0-17 years old) and adult (>18 years old) patient cohorts was also completed.
Based on the CDC COVID-19 pandemic timeline, the pre-COVID-19 pandemic cohort was defined as treatment dates from 2014 to March 14th, 2020, the COVID-19 pandemic cohort was defined as March 15th, 2020 to April 2021, and post-COVID-19 was defined as April 2021 to 2023. This classification was used to assess if injury patterns varied with behaviors during lockdown during the COVID-19 pandemic.
Statistical Analysis
Descriptive statistics were used to summarize demographic variables and are presented as means with standard deviations (SD). Electrical burns were excluded from analysis due to the very small sample size across 100 EDs. Chi-squared tests were performed to compare burn types between gender and age cohorts. Standardized residual analysis was evaluated where appropriate. SPSS (IBM Corporation, Armonk, NY, USA) was used for all statistical analysis. Statistical significance was defined as P < .05 for chi-squared and >
Results
A total of 6883 patients were included in this study and the mean age of patients was 72.5 years (SD, 25.0), with a national estimate of 249 657 facial burn injuries presenting to emergency departments (Figure 1). 2740 (39.8%) facial burns occurred in the pediatric population whereas 4143 (60.2%) facial burns occurred in the adult population. 2754 (40.0%) female patients and 4090 (60.0%) male patients presented to the emergency department with facial burns over the study period. The racial make-up of this patient cohort was 42.1% White, 18.6% Black, 2.67% Asian, <1% American Indian or Alaska Native, <1% Hawaiian or Pacific Islander, and 36% unspecified or other. The common types of products involved in facial burns in this study were liquid propane, microwave or range ovens, pressure cookers, paraffin, cookware, tableware, gasoline, fireworks, cigarette lighters, home fires, hot water, and gas grills or stoves.
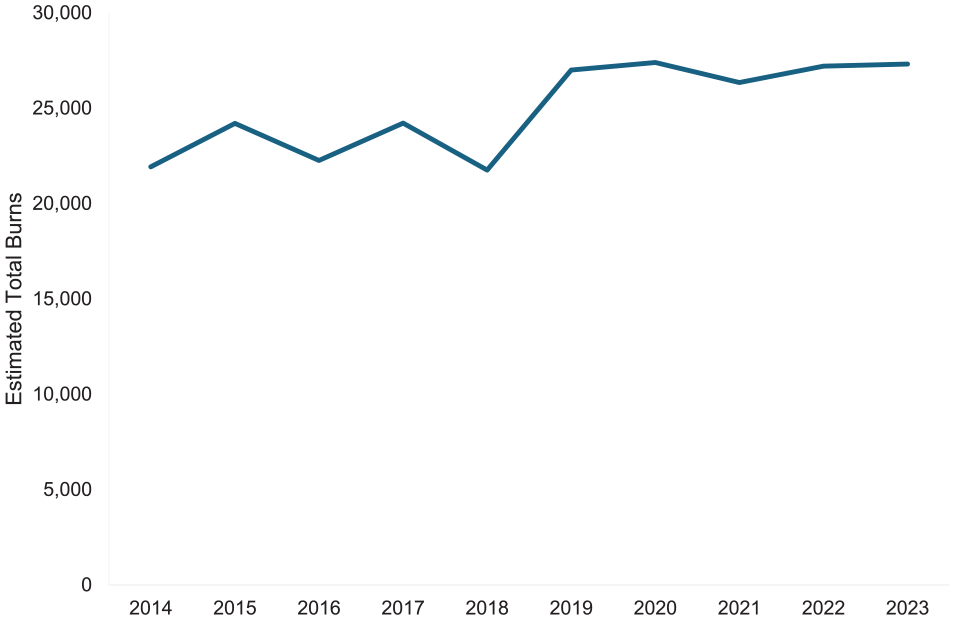
Estimated National Facial Burns YOY from 2014 to 2023.
Burn Type
Thermal burns and scald burns were the most common type of facial burn from 2014 to 2023 with a total of 3900 (57%) and 2313 (34%) injuries, respectively (Figure 2). The total number of facial burns stayed consistent year over year (YOY), as did the distributions between different burn types (Figure 2). Thermal burns in the most recent year of the study, 2023, has the highest incidence in July with relatively steady incidence throughout the rest of the year.
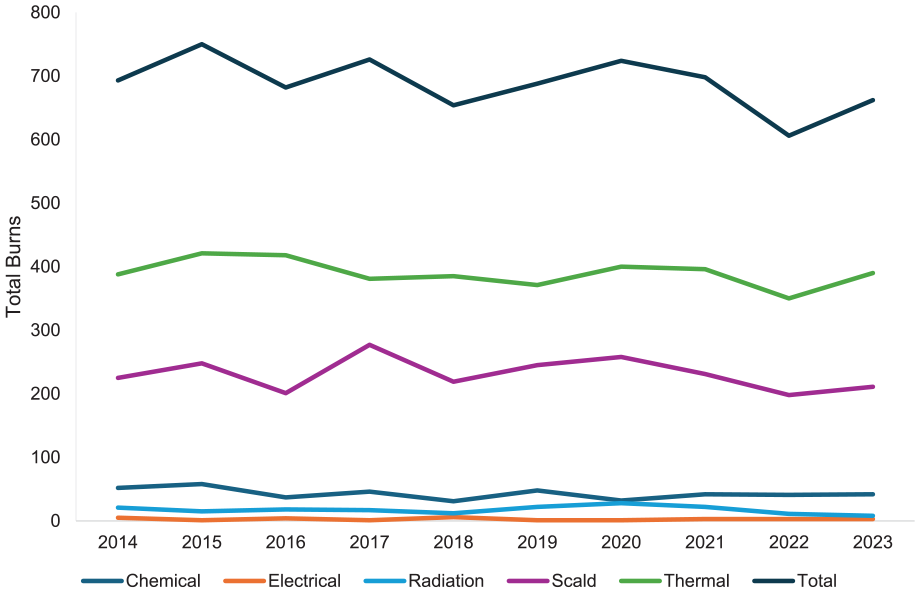
Burn type trends YOY from 2014 to 2023.
Age Distribution
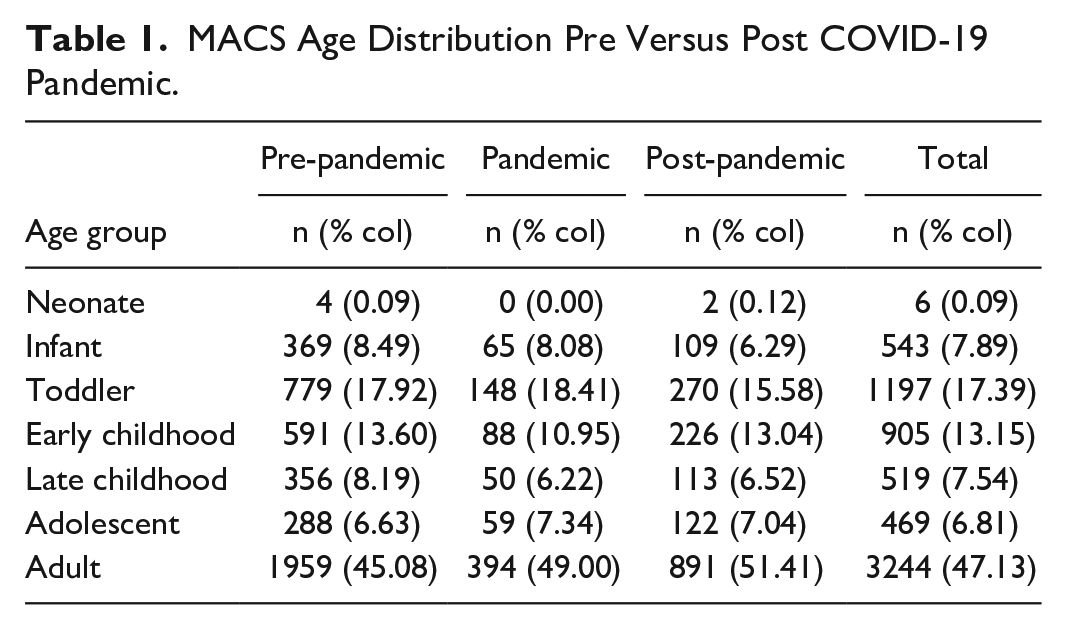
Prevalence of each age group of facial burns stayed consistent between pre- and post-COVID-19 pandemic (Table 1). The 60 to 69 and the 70 to 79 demographics increased from 6.94% to 8.88% and 2.96% to 4.39% of total facial burns, respectively. Interestingly, the 20 to 29-year-old demographic is the group with the highest likelihood of experiencing a facial burn.
MACS Age Distribution Pre Versus Post COVID-19 Pandemic.
Pediatric Versus Adult
Pediatric facial burns increased in 2020 to 307 facial burns followed by a steady decrease yearly to 218 in 2023. Whereas adult facial burns prevalence remained consistent YOY from 2014 to 2023 (Figure 3). Pediatric burns were most likely to be caused by hot water and cookware/tableware whereas adults were more likely to be caused by gasoline, cooking appliances, and grills.
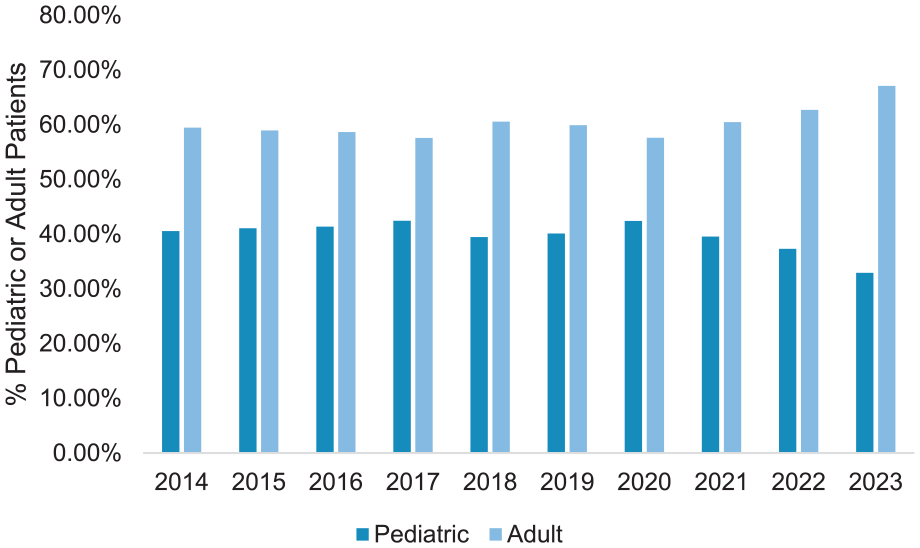
Adult versus pediatric facial burn incidence YOY from 2014 to 2023.
There was a statistically significant difference of some MACS age cohorts between burn types (P < .001; Figure 4). Chemical facial burn variation between age cohorts was not statistically significant. The adult cohort had significantly lower rates of radiation (−4.4) and scald (−12.5) burns, and significantly higher rates of thermal (10.7) burns. The adolescent cohort had significantly lower rates of scald (−3.6) burns but significantly higher rates of radiation (10.8) burns. In the infant cohort there were statistically higher rates of scald (8.5) burns and significantly lower rates of thermal (−7.2) burns. The late childhood cohort had a higher incidence of radiation (6.6) burns and scald (3.9) burns. In the toddler cohort there were significantly lower rates of radiation (−3.0) and thermal (−10.5) burns however in this cohort there were higher rates of scald (14.7) burns. The early childhood and neonate cohorts did not have statistically different incidence of burn types compared to other age cohorts.
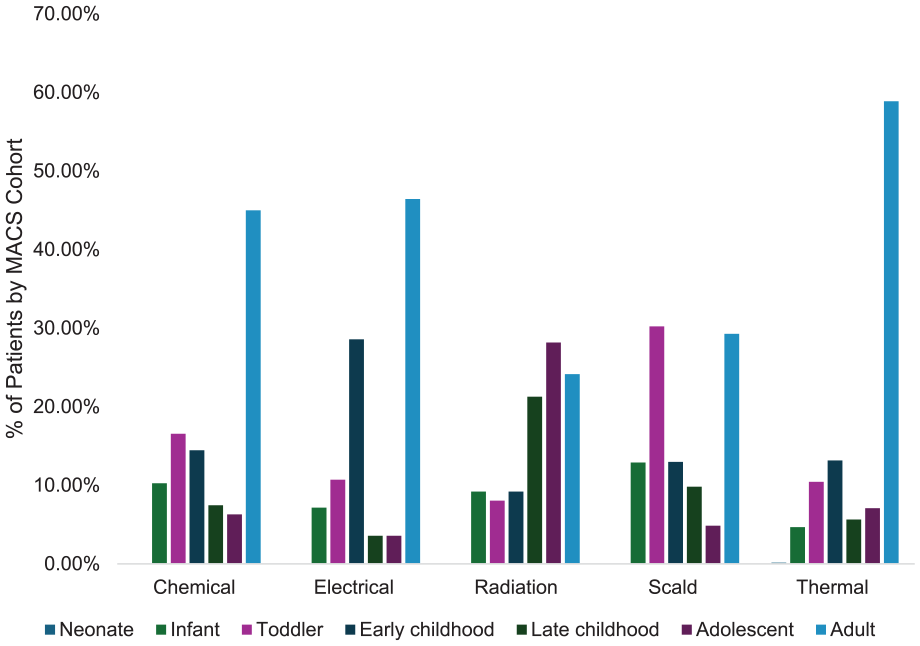
Relative distribution of MACS age brackets by burn type.
Gender
Overall, there were 1.5× more males than females to obtain a facial burn. Comparing incidence of facial burns of male versus female between different burn types, the incidence of burns was relatively equal between males and females excluding thermal burns. Though thermal burns were the highest incidence of facial burns for both males and females, males obtained 2598 (67%) thermal facial burns compared to females at 1302 (33%) facial burns, so 2× more males obtained a thermal facial burn (Table 2).
Facial Burn Type by Gender from 2014 to 2023.
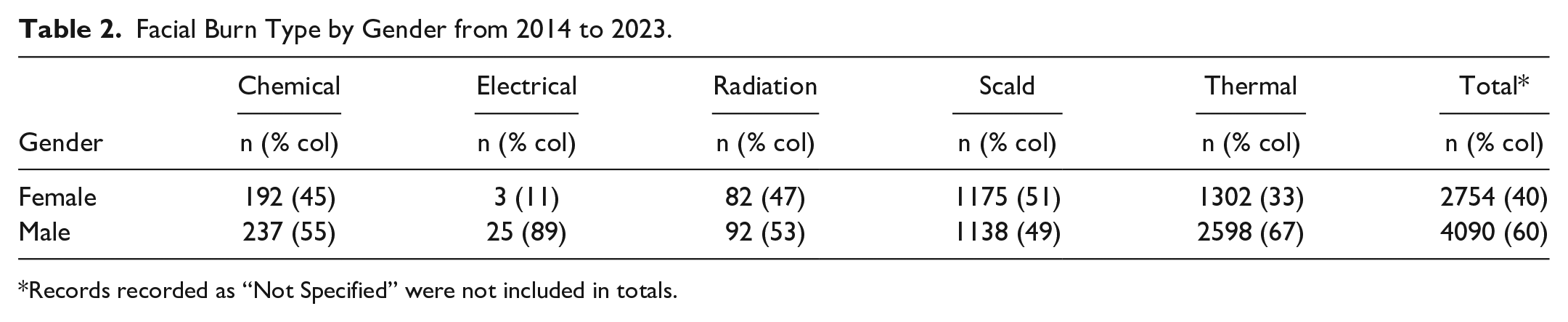
Records recorded as “Not Specified” were not included in totals.
There was a statistically significant difference of between gender (P < .001). Females were more likely to be injured by chemical (1.4), radiation (1.4), and scald (7.9) burns whereas males were more likely to be injured by thermal (5.6) burns.
Race
Since 2016 the percentage of overall facial burns recorded as “Not Stated in ED Record” has shown a negative correlation (R = − 0.93) year over year from a high of 45% to 19% in 2023. While the specific racial groups have shown an increase since 2016 tracking with the decrease in the not recorded category. Black and White patients made up 60% of facial burns presenting to the emergency department during the study period with 42% and 18% for White and Black, respectively.
Discussion
Existing Literature on Burn Incidence
In the United States, facial burns are commonly caused by thermal burns and scald burns, aligning with the results in our study.13,14 Interestingly, a prior study using the NEISS database investigating head and neck burns from the preceding 5 years of this study (2009-2013) found a similar distribution of head and neck burns with 40% from thermal burns, 23% from chemical burns, and 22% from scald burns. 13 Comparatively, the data in our study found a higher percentage of thermal and scald burns with a large decrease in chemical burns. We only reviewed facial burns while Heilbronn et al evaluated all head and neck burns which may account for this drastic distribution difference but also could be due to improved education on burn prevention or safety mechanisms in consumer products. A similar study in pediatric populations from 2000 to 2018 found facial burns had a similar distribution between burn types as our study and other previous studies. 14 Auh et al 14 also demonstrated a similar decline in pediatric burns. Existing literature on gender-based differences on burn injuries supports the male preponderance found in our study and have found males are more likely to suffer electrical or flame burns while females are more likely to suffer scald injury.15,16 However, complication rate and overall mortality are found to be similar. 15
In recent decades, burn injury incidence has been decreasing in developed countries, with an overall downward trend in burn severity in high income regions. 17 Improved prevention in the United States such as smoke alarms, safer home appliances, and residential building code updates have resulted in declining burn rates in the past 2 decades, especially in pediatric populations. 14 There is limited literature on the trends of adult facial burn incidence in the most recent decades, though a recent Canadian study of burn patients presenting to Vancouver General Hospital found a decreased incidence and mortality in all adult burns over a 40-year period (1976-2015). 18 Advancements in education and safety measures over the decades prior to our study likely led to the significant decreases in burn incidence seen in the previously mentioned studies whereas our study of the most recent decade shows a steady rate of facial burn incidence in both adult and pediatric populations. This underscores the need to develop focused burn campaigns targeting specific mechanisms of injury as well as increased safety measures of commonly implicated consumer products, such as grills. Similarly, the impact of the efficacy of burn campaigns on burn incidence is understudied. The results in our study provide an epidemiological starting point for burn prevention education and future studies using the NEISS database could be used as long-term quality measure of prevention campaigns.
Burn Campaign Impact
The wide variety in burn etiologies leads to great difficulty in prevention methodologies. Additionally, with an extremely diverse patient demographic, interventions must apply across multiple patient subsets. Research has shown that online burn first aid information can be inconsistent and inaccurate, underscoring the importance of quality and effective burn campaigns. 19 However, even with these limitations, burn prevention campaigns have proven to be effective.20-23 It is important to contextualize the effectiveness of these campaigns among the myriad of confounding factors and applications, and a brief discussion is offered in the context of the presented data for US emergency room burns due to the global approach many of these studies take.
There have been numerous burn campaigns over the last several decades. These campaigns extend over many countries and many different regions within individual countries. There are generalized campaigns such as Global World Burn Week by the International Society for Burn Injuries. The American Burn Association created the annual National Burn Awareness Week the first full week of February each year. This is one of the more prominent campaigns in the US, and the campaign is targeted at general burn prevention awareness among all burn types. Fact sheets, social media pushes, and a variety of other strategies are utilized in this campaign. Each year has a different target on top of spreading general awareness, and 2025’s campaign focuses on preventing burns in the home.
Burn prevention strategies are also utilized among targeted, one-time campaigns. 24 For example, in 2019, a UK multimedia campaign called SafeTea was launched on National Burns Awareness Day, running for 3 months. 25 Cowley et al 25 demonstrated effective reach and engagement for SafeTea, which centered around preventing hot drink scalds in children. Another study in Ontario utilized standardized pre and post campaign surveys to monitor increases in burn prevention knowledge, and they demonstrated a significant increase in burn prevention knowledge post intervention among an adult population. 21 A US campaign was implemented in 1977 to 1978 in Boston, delivering a multimedia educational approach. 26 The heterogeneity of these studies in both their interventional strategies and measured outcomes begs the question of their true effectiveness.
Although these campaigns have been demonstrated to be effective individually, the current steady rates of facial burns demonstrated in our study pose the question if other strategies should be evaluated. A limitation within these burn prevention campaigns is the immense variability within the selected population, and van Balen 2024 emphasizes that current research and evidence on this subject is limited, particularly in the pediatric population. 22 Community level disparities have been shown to affect the severity of burn injuries. 27 Tupetz et al 28 similarly found that solutions for childhood unintentional injury, in which burns is a major category, are often deployed at much lower rates in low-income countries. Even within singular US metropolitan areas, great socioeconomic disparities exist among communities. Combining the differences in burn injury outcomes and the potential differences in prevention rates with the steady rates of burns in our data could indicate that burn campaigns should have more targeted objectives. However, it is important to acknowledge that due to the specificity of facial burn data here, widespread claims about the state of prevention are challenging to make. The variability in existing literature on overall trends and trends among specific demographics complicates any claims further. Further research should more stringently analyze the effectiveness of burn campaigns and whether they are changing behavior, not just increasing awareness.
Racial Differences in Injury
Racial disparities in burn incidence and outcomes in the United States are well documented with recent studies finding the burn patient racial makeup was 65% White, 19% Black, and 22% other minority groups. 7 Our study found a similar incidence between racial groups. Interestingly, the largest change in percentage over the 10-year period of our study was the decreased “Not Otherwise Specified” category. A possible explanation is improved recording of patient demographics over this period. Improved recording could provide further insight into racial differences in burn incidence assuming this trend continues in the NEISS database. Burn studies have historically been less likely to enroll minority populations, but a recent 2025 study has found increasing incidence of omission of race in the NSQIP-P, a national surgical database.29,30 This contrasts with the results in our study which found increased reporting of race over the 10-year period.
The higher proportion of burn incidence in minority populations compared to the general population distribution is likely due in part to socioeconomic factors including unsafe heating practices due to unresolved heating complaints in low-income communities, challenges with childcare (eg, poor supervision or neglect may result in increased incidence/severity of burn injuries), and systemic healthcare barriers.31,32 Apart from incidence, previous studies have shown Black burn patients have higher inpatient complication rates and higher mortality compared to white patients. 7 Similarly, Native American burn patients have been shown to have higher rates of respiratory complications, wound complications, and infectious complications of all racial groups. 33 Though socioeconomic status plays a critical role in morbidity and mortality, racial minority groups do not see the same improvements as white individuals. 34 Another important factor to consider in treating racial minority burn patients is the higher incidence of post-burn scarring through hypopigmentation, keloids, and hypertrophic scars. 35 The well studied and documented racial disparities underscore the importance of continued improvement of demographic data recording to provide accurate representation of racial disparities. This continues to be important in focused interventions to decrease complications in minority burn patients and improve burn prevention in minority groups.
COVID-19 Demographics
During the early COVID-19 pandemic, there was a shift in burn injury patterns. A multicenter study found when comparing pediatric head and neck burn incidence in April 2020 to April 2019 there was a 200% increase, thought to be secondary to the lockdown precautions at this time. 36 This aligns with our study results showing a spike in pediatric facial burns in 2020. During the pandemic there was an increase in adult average age burn incidence, with younger adult (18-25-year-olds) burn incidence decreased, specifically in reduction of scald, flame, and explosion burns whereas adults 76 to 85 years old had an increase in contact burns. 37 Despite these demographic changes, current literature supports no major change in overall burn incidence which is supported by our study results. 38 The change in distribution is thought to be due to different settings and behaviors during the lockdown period of the COVID-19 pandemic. These trends observed in the literature support the findings in our study and provide context for the epidemiological differences observed during the pandemic period. Research indicates the COVID-19 pandemic did not appear to have a large impact on the prevalence of burns between demographics.
NEISS Limitations
Though the NEISS database is a valuable tool, it is not without limitations. Data in the NEISS database consists only of injuries presenting to the emergency department, hence it does not capture cases that presented to care outside the emergency department and may underreport purely occupational burns. Additionally, each visit to the ED is recorded as a separate entry hence not accounting for repeat visits for the same injury in the same patient creating the potential for double counting. The NEISS also does not comprehensively report all consumer product types individually, leading to possible underestimation of the real incidence.
Similarly, the NEISS database only includes data from 100 emergency departments in the United States, not capturing the total incidence across emergency departments nationwide. NEISS considers the sample of emergency departments statistically representative of the total population, but the predictive model of national estimates is subject to sampling bias due to the weighted probability of sample model. 39 Our analysis also utilized raw data, which could lead to sampling bias. There is the possibly of incorrectly coded injuries due to the limited information provided in the narrative description for each entry. 40 Finally, comparisons between pre-COVID-19 pandemic, COVID-19 pandemic, and post-COVID-19 pandemic assume overall populations characteristic did not change between these periods while there are a multitude of variables that may have changed between these time periods. This limitation introduces potential confounders, however by the nature of this dataset this was not possible to be controlled.
With the limitations from this dataset, generalized conclusions from these data may be limited, however this study provides an epidemiological estimate of facial burn incidence presenting to United States emergency departments. Importantly, these findings provide insight into demographic specific mechanism of facial burn injury providing the basis for development of targeted prevention measures.
Conclusion
Facial burn incidence in adult and pediatric populations has remained steady over the recent decade, with thermal burns and scald burns being the most common mechanism of injury. Adult populations were more likely to be burned by gasoline and cooking appliances whereas pediatric populations were more likely to be burned by hot water and tableware. Minority populations continue to be disproportionately affected by facial burns in this period.
The steady incidence of facial burns over the past decade supports the importance of further patient education and awareness for facial burn prevention. The results from this study can be used as a basis to refine burn campaigns and emphasize the importance of evaluating the efficacy of campaigns. Overall, these data provide a foundation for future research and evaluation of facial burn prevention, importantly to mitigate disparities in patient outcomes.
Supplemental Material
sj-docx-1-fac-10.1177_27325016251355517 – Supplemental material for Face the Heat: Facial Burn Emergency Department Visits Over 10 Years
Supplemental material, sj-docx-1-fac-10.1177_27325016251355517 for Face the Heat: Facial Burn Emergency Department Visits Over 10 Years by Gemma Toogood, Harrison Smith, Meghan Underwood and Devra Becker in FACE
Footnotes
Data Accessibility Statement
Data used in this study is publicly available through the NEISS database. Further information may be obtained from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Devra Becker is a member of the Editorial Board of FACE and did not take part in the peer review or decision-making process for this submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study was IRB exempt because the data used is deidentified and publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.