
Abstract
Introduction:
Many states, including ours, mandate coverage of orthodontic treatment as part of cleft care. Despite these mandates, barriers consistently arise for patients leading to lack of coverage, delays in care, and increased financial burden. This study aims to characterize the experience and challenges to obtaining coverage for braces as part cleft care for pediatric patients at our institution.
Methods:
An 18-item REDCap survey was distributed to parents of patients who had been seen in our craniofacial orthodontic clinic for braces from 2019 to 2024. The survey was distributed in English and Spanish based on primary language indicated in the patient’s chart. The survey addressed insurance provider status, the claim process, preauthorization requirement, percentage of coverage by medical and dental insurance, out-of-pocket cost after insurance coverage, and a free response for parents to share any additional experiences in obtaining coverage. Standard statistical analysis was performed.
Results:
Forty-one complete responses were received, with a response rate of 15.6%. 43.9% of respondents filed a claim with their medical insurance carrier. The claim process duration varied from minimal time to 6 months to 2 years maximum. Among those who did not file, 34.8% cited uncertainty as to whether insurance would cover treatment. Preauthorization was required for 50% of respondents, resulting in treatment delays until approval in 35.9% of survey participants. Medical insurance covered an average of 37.9% of costs, dental insurance covered 35.2%, leaving a median out-of-pocket expense of $2580.75 after coverage from either provider.
Conclusions:
Despite mandated coverage, families face significant barriers in securing insurance reimbursement for orthodontia. Additional education, advocacy, and policy enforcement are needed to improve access and compliance with state mandates.
Introduction
The importance of multidisciplinary cleft care is well established and has been shown to improve patient satisfaction and patient outcomes.1-3 The American Cleft Palate Craniofacial Association (ACPA) has established standards for ACPA Team Approval. 4 Within these standards, orthodontists are included as one of the required specialists on the team. 4 Craniofacial orthodontic treatment plays an integral part throughout the various stages of cleft care including preoperative nasoalveolar molding, maxillary expansion, dental alignment, orthopedic modification and orthognathic surgery preparation.5,6 Braces are frequently required to achieve these treatment goals. Despite the important role orthodontia plays in cleft care, many families face difficulties in securing medical insurance coverage for these treatments.
Currently, there is no federal mandate for medical insurance to provide coverage for medically necessary cleft care, including orthodontics for patients with cleft lip and palate. 7 The decision to mandate coverage is deferred to each state. Over the last several decades, there has been an increase in state-mandated coverage for cleft care. 7 However, many states lack mandated coverage, and an even greater number fail to mandate coverage for orthodontics.7,8 Furthermore, even in states with mandated coverage, many families are unable to receive coverage or reimbursement due to difficulties proving “medical necessity” as defined by some legislation and challenges surrounding medical insurance carriers recognizing dental billing codes. 8
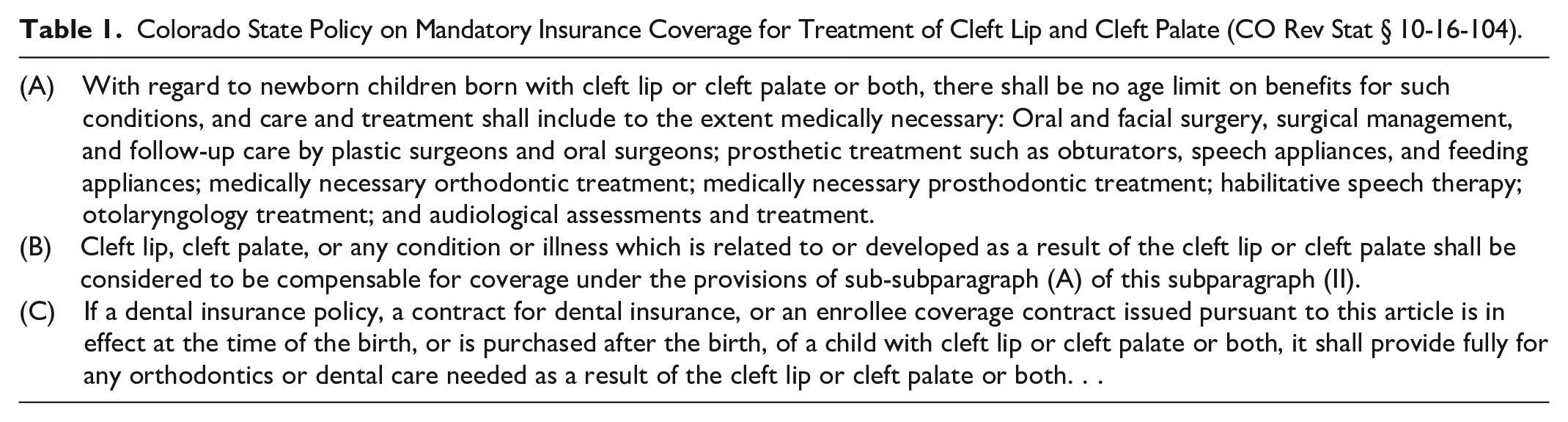
In Colorado, coverage for medically necessary orthodontic treatment as part of cleft care is mandated by law, with no age limitations (Table 1). 9 At our institution, to obtain insurance coverage, patients first undergo consultation and orthodontic records collection. A letter of medical necessity documenting the patient’s cleft diagnosis and treatment rationale is submitted to the insurance payor along with relevant medical records, orthodontic records, and consultation notes from the multidisciplinary cleft team. If coverage is initially denied, appeals or peer-to-peer discussions may be pursued to support reimbursement claims.
Colorado State Policy on Mandatory Insurance Coverage for Treatment of Cleft Lip and Cleft Palate (CO Rev Stat § 10-16-104).
Despite these institutional efforts and the state mandate, many families have reported difficulties in securing coverage for their child’s orthodontic treatment, particularly for braces. To date, no studies have assessed how effectively such mandates and protocols translate into coverage for pediatric patients with clefts. Therefore, this study aims to characterize the experience and barriers families face when obtaining coverage for orthodontic braces as part of cleft care at our institution.
Methods
An 18-item REDCap anonymous survey was distributed to parents or legal guardians of all pediatric patients with cleft-related orthodontic treatment who were seen in our craniofacial orthodontics clinic between 2019 and 2024. The survey was distributed in English and Spanish based on primary language indicated in the patient’s chart (Supplemental Materials). The survey addressed insurance provider status, the claim process, requirement of preauthorization, percentage of coverage by medical and dental insurance, out-of-pocket cost after insurance coverage, and an open-ended response for parents to share any additional experiences in obtaining coverage. Standard statistical analyses were performed. Open ended responses were reviewed for themes.
We also queried LexisNexis legal database as well as individual state legislature to understand the current availability of mandated coverage for cleft care. Search terms included “Congenital,” “Birth Defect,” “Craniofacial,” “Cleft,” and “Anomaly.” States with any explicit mandated coverage for cleft or craniofacial care were identified. Those with mandates that explicitly included orthodontic coverage were also identified.
Results
A total of 263 parents or legal guardians of pediatric patients with cleft-related orthodontic treatment were invited to participate in this study. Of those, 41 completed the survey, yielding a response rate of 15.6%. There were 4 excluded responses as these patients indicated they had not received treatment yet or their residence was outside of Colorado. Of the respondents, 67.5% of respondents had commercial insurance, 24.3% had Medicaid, 3.7% had service member insurance, and 5.4% had a combination of Medicaid and another provider. Additionally, 82.1% also reported having dental insurance.
Only 48.6% chose to file a claim with their medical insurance provider. Those who indicated they did not file a claim were asked why they chose not to file. Many reported uncertainties in the process and whether their insurance would provide coverage. Several sample responses are shown in Table 2.
Sample Open-Ended Responses to “Why Did You Choose Not to File a Claim to Your Medical Insurance Provider for Coverage?”.

Other responses expressed that they were in the process of submitting a claim or that they were not required to file one to obtain coverage. Regarding the duration of the claim process, some reported “minimal time” with other responses ranging from 6 months to 2 years.
Over half of respondents (59.4%) reported having to obtain pre-authorization from their medical insurance, and 40.6% waited until this was obtained before their child received braces.
Coverage from medical insurance ranged from 0% to 100%, with an average coverage of 41.5%. Dental insurance showed similar results with a range of 0% to 100% and an average coverage of 35.1%. The median out-of-pocket cost of braces after all medical and insurance coverage was $2500.00 with a range of $11 000.00 (Figure 1). Of note, patients can only submit to either dental or medical insurance.
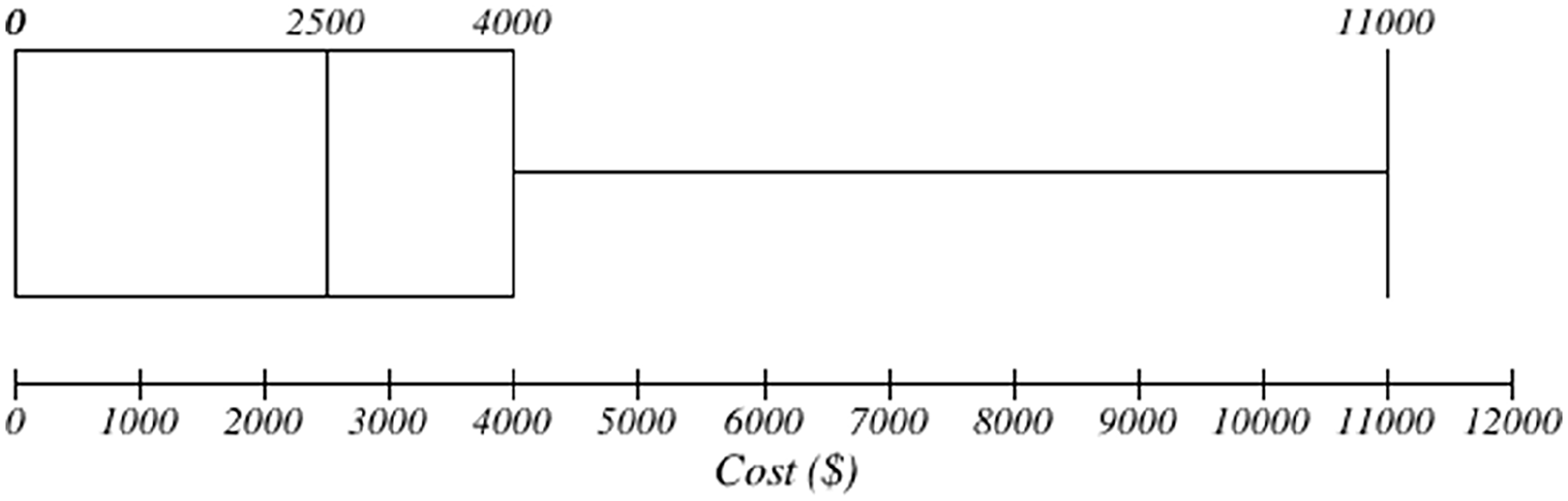
Out-of-pocket costs for braces.
Dental insurance was not observed to lower the average cost after coverage in these patients ($2560.45 vs. $2367.50, P = .726). Furthermore, no significant difference in out-of-pocket cost was noted between those with only private insurance and those with other forms of insurance ($2392.47 vs. $2485.61, P = .376).
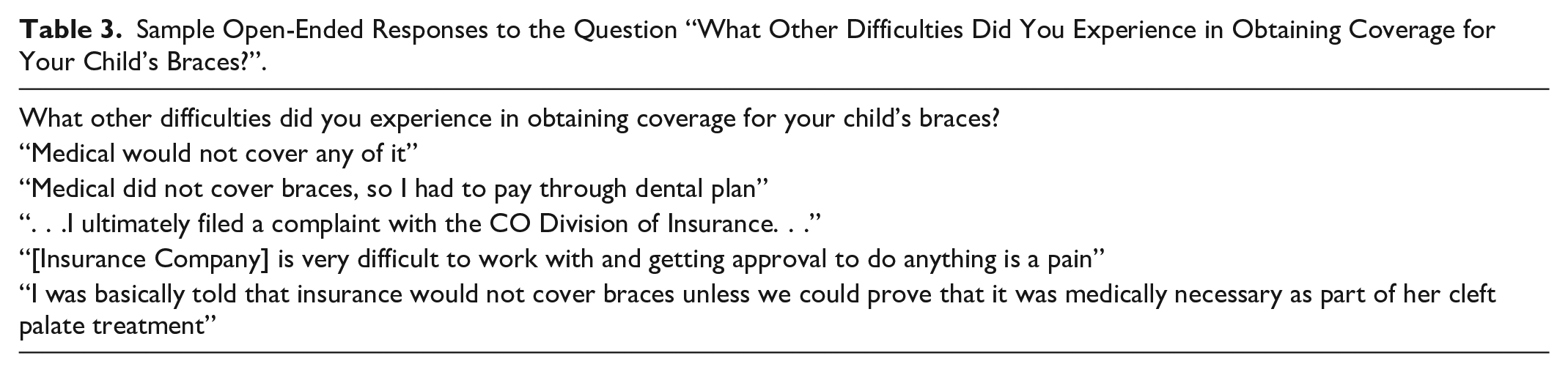
When asked about additional experiences obtaining coverage, parents reported that they did not believe their medical insurance would provide coverage and difficulties proving medical necessity to their medical insurance provider. Several sample responses may be seen in Table 3.
Sample Open-Ended Responses to the Question “What Other Difficulties Did You Experience in Obtaining Coverage for Your Child’s Braces?”.
Regarding available mandated coverage for cleft care, 19 states had some mandated coverage for cleft or craniofacial care (Figure 2; Supplemental Material 2). Of those, 14 explicitly stated coverage should include orthodontics. Of note, some states, such as Washington, include coverage in Medicaid and/or provide coverage for “congenital anomalies” for the newborn period. 10 These states were not considered mandated coverage states due their limitations in coverage. The most relevant state policies, including those with only newborn coverage for congenital anomalies, are included in Supplemental Materials.
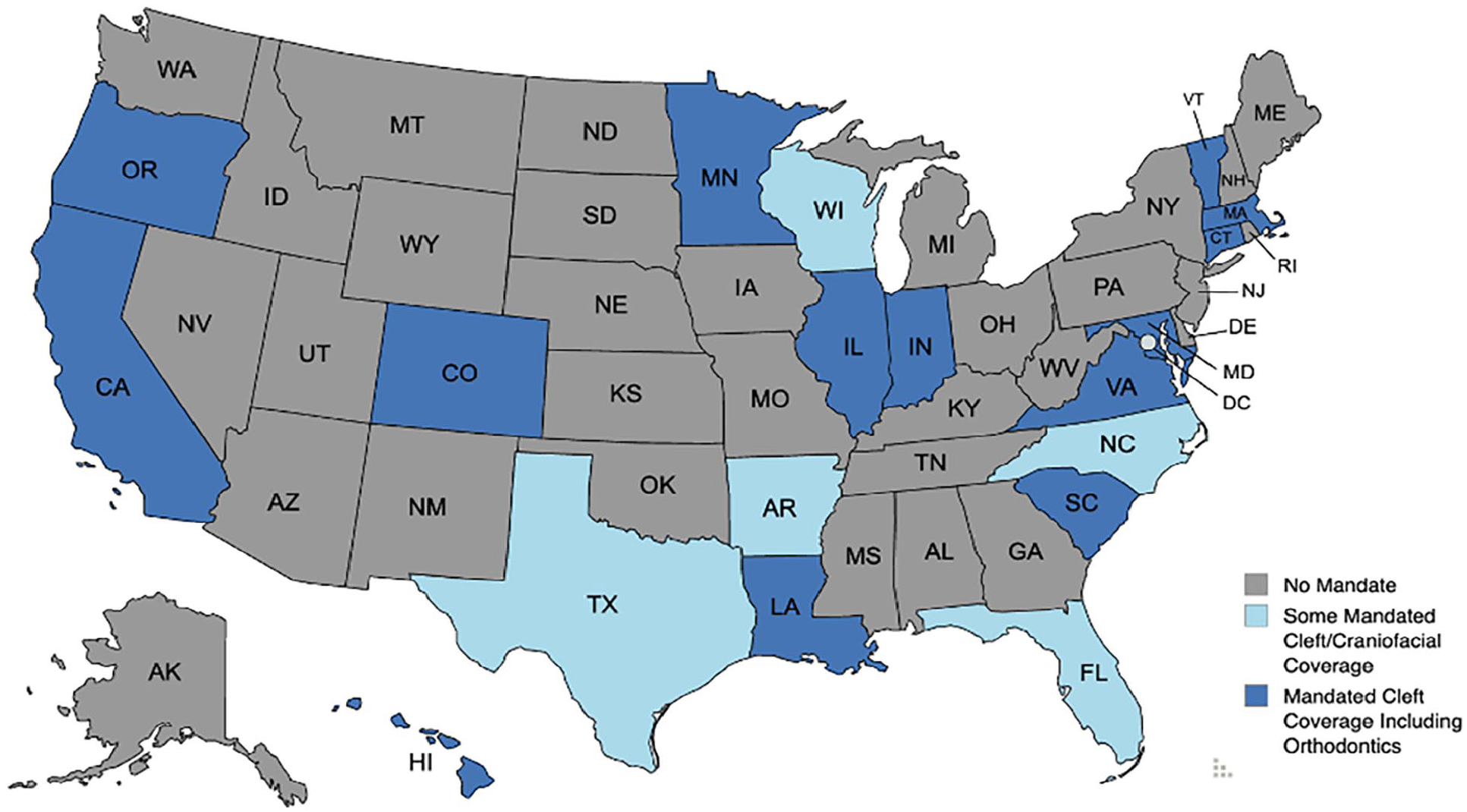
Availability of state mandated coverage.
Discussion
Orthodontics, including braces, is a key component of multidisciplinary cleft care and has been shown to improve both functional and aesthetic outcomes.6,11 Although orthodontics is established as standard of care for patients with clefts, many states do not mandate medical insurance coverage of these treatments.4,7,8 Furthermore, many families experience difficulties obtaining medical insurance coverage for these treatments even in states where it is legally required. To understand these challenges, this study identified several key barriers faced by families when obtaining insurance coverage for braces (Figure 3).
Barriers to coverage for medically necessary orthodontics in cleft care.
The majority of respondents in this study did not file a claim to their medical insurance for coverage of their child’s braces. Furthermore, open-ended responses demonstrated that families either were unaware that their insurance company may provide coverage or believed such coverage was not available. Given the misperception, there is a clear opportunity for education of families regarding the presence and conditions of mandated coverage of braces for cleft care. Additionally, if participants who reported their insurance does not cover braces were informed of this by their insurance providers, this could represent a potential lack of awareness of the mandate, weakness in the enforcement of the mandate, lack of a straightforward mechanism to execute the mandate, or possible noncompliance by insurance companies with state regulations. While our team has always communicated insurance rights to families during clinic visits, the findings from this study have highlighted specific barriers we are now addressing through more targeted and proactive discussions with families navigating insurance coverage.
Although some families received medical and/or dental insurance coverage for care, the amount of coverage and out-of-pocket expenses varied widely. On average medical insurance covered 41.5% of costs, and when present, dental insurance covered 35.1% of costs. Despite this, the median out-of-pocket costs remained high at $2500. Thus, even when insurance companies comply with the state mandate, families continue to face significant financial burdens, highlighting a key limitation of the mandate in providing financial relief for families.
In addition to financial costs, many families spent significant time completing paperwork and working with their insurance companies to ensure braces coverage. Some families reported spending 6 months and up to 2 years navigating the claim process. Furthermore, many families were required to obtain preauthorization for their child’s braces, and some chose to delay care until this was secured from insurance providers. Although we did not evaluate the extent of delayed care in this study, the importance of timely intervention throughout the phases of cleft care is well known. 12 Given the extensive time families spend navigating the insurance process and the potential delays of care, cleft care teams should consider allocating additional resources to assist families throughout this process.
Although the state mandate in Colorado provides explicit provisions regarding orthodontic treatment for children with orofacial clefts when medically necessary, the legislation does not define a legal standard for medical necessity. While this study only includes participants from Colorado, the difficulties our patients experience may highlight a more wide-spread issue as the difficulty in proving “medical necessity” is not unique to this state and has been highlighted as an ongoing barrier in the literature. 8 In states where proof of medical necessity is required for coverage, cleft care teams should make every effort to document this in the medical record and consider allocating resources to help families navigate the process of proving need for care to insurance companies.
While mandated coverage is available to those in Colorado, many states still lack any mandated coverage. Only 19 states were identified to have mandates explicitly including coverage for cleft or craniofacial care, and of these only 14 specifically mentioned orthodontic care within the mandates. These results are similar to those by Wanchek et al., 7 and Pfeifauf et al., 8 conducted in 2017 and 2020, respectively. Thus, there has been limited progress in ensuring patients with cleft are able to receive the care they require. Furthermore, within the states that mandate coverage, there are various restrictions such as age limits. As each state policy has its own nuances, ACPA care teams are encouraged to closely read and evaluate any relevant policy available within their home states.
Beyond state level efforts, there has been an effort to pass a federal mandate for insurance coverage of cleft care. In 2021, the “Ensuring Lasting Smiles Act” was introduced to congress. 13 This bill includes provisions for coverage of a variety of services including orthodontics for patients with a congenital anomaly or birth defects. 13 Despite existing state mandates and continued barriers faced by patient families, additional advocacy at the state and federal level such as this, may be needed to address gaps in coverage and alleviate continued burdens on families.
Limitations to this study include those inherent to survey studies, including potential response bias and low response rates. As such, the barriers identified in this study may not fully capture the experiences of all families seeking coverage for orthodontic treatment. Despite these limitations, we are able to observe the effects of the mandate in our state and characterize several barriers to care families at our institution face. As this study is cross-sectional, it cannot capture future expenses with additional phases of treatment and families may incur additional costs after the time of this study. Additionally, dental insurance providers often have a lifetime maximum on coverage providers and patients with cleft may eventually exceed this maximum requiring additional costs to be paid out of pocket. Furthermore, as respondents are limited to families within our state, the costs, time spent in the claims process, and additional issues obtaining coverage may be greater in other states depending on local mandates and available resources. Given this, ACPA Care Teams are encouraged to discuss these topics with families to better understand and assist in any unique difficulties they may experience. Finally, this study was performed at a children’s hospital, and barriers faced by adults who may have aged out of care at our institution were not captured.
Conclusion
Families often face significant barriers to obtaining coverage for their child’s orthodontic treatment despite state-mandated coverage. Many respondents reported uncertainty of coverage or inability to obtain coverage from their medical insurance provider, suggesting possible misconceptions. Furthermore, even when coverage was provided by insurance companies, many still faced substantial financial burdens. Additional support, education, and advocacy are needed to help families navigate the insurance claim process and ensure compliance with state mandates.
Supplemental Material
sj-docx-1-fac-10.1177_27325016251362419 – Supplemental material for The Burden of Braces in Cleft Care
Supplemental material, sj-docx-1-fac-10.1177_27325016251362419 for The Burden of Braces in Cleft Care by Skyler K. Palmer, Diego A. Gomez, Emily A. Green, Ariel Johnson, Antonio R. Porras, Jason W. Yu, David Y. Khechoyan, Brooke French, Phuong D. Nguyen and Kristen M. Lowe in FACE
Supplemental Material
sj-docx-2-fac-10.1177_27325016251362419 – Supplemental material for The Burden of Braces in Cleft Care
Supplemental material, sj-docx-2-fac-10.1177_27325016251362419 for The Burden of Braces in Cleft Care by Skyler K. Palmer, Diego A. Gomez, Emily A. Green, Ariel Johnson, Antonio R. Porras, Jason W. Yu, David Y. Khechoyan, Brooke French, Phuong D. Nguyen and Kristen M. Lowe in FACE
Supplemental Material
sj-docx-3-fac-10.1177_27325016251362419 – Supplemental material for The Burden of Braces in Cleft Care
Supplemental material, sj-docx-3-fac-10.1177_27325016251362419 for The Burden of Braces in Cleft Care by Skyler K. Palmer, Diego A. Gomez, Emily A. Green, Ariel Johnson, Antonio R. Porras, Jason W. Yu, David Y. Khechoyan, Brooke French, Phuong D. Nguyen and Kristen M. Lowe in FACE
Footnotes
Ethical Considerations
This study (24-1533) was determined to be IRB Exempt by Colorado Multiple Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
We have not received approval to share the data of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.