
Abstract
Background:
Ameloblastoma is a rare benign odontogenic tumor that occurs mainly in the mandible. It is characterized by a high tendency to recurrence. The aim of this study was to determine the frequency of recurrence and to investigate the risk factors (RF) for recurrence in mandibular ameloblastoma (MA).
Methods:
We conducted a retrospective descriptive study including patients with MA in the maxillofacial surgery department of Charles Nicolle Hospital over a 26-year period (1997-2022).
Results:
The recurrence rate after the first treatment was 30%. Recurrence- free survival was significantly associated with anterior location (P = .033). The recurrence rate was higher for unilocular tumors. The presence of intra-tumoral bone septa was significantly associated with a lower recurrence-free survival rate (P = .042). In cases where the tooth was included in the tumor, patients did not significantly experience recurrence (P = .043). Cortical rupture (CR) was significantly associated with a higher rate of recurrence (P = .045). From a tumor size of 5 cm, the recurrence rate was estimated at 58%. Radical treatment was associated with a non-significantly high rate of recurrence-free survival. Extraction of 2 teeth upstream and downstream of the tumor was significantly associated with a low recurrence rate (P < .001). Multicystic histological type had a statistically significant higher recurrence rate than unicystic ameloblastoma (P = .049).
Conclusion:
This updated RF study would enable us to classify AM patients according to their level of risk of recurrence, and thus adjust their surgical management.
Introduction
Ameloblastoma is a benign odontogenic tumor of epithelial origin with mature fibrous stroma but no odontogenic ectomesenchyme. 1 Ameloblastomas account for approximately 1% of all maxillary tumors and 13% to 58% of odontogenic tumors. 2 Around 80% of ameloblastomas are located in the mandible. 1 Ameloblastoma is a unique tumor in that it is very slow-growing, has a high potential for local spread, and is highly prone to recurrence. A strategic approach is essential in the management of ameloblastoma, to minimize the number of surgical interventions while ensuring maximum efficacy. The aim of this work was to determine the frequency of recurrence and to study the risk factors (RF) for recurrence of mandibular ameloblastoma (MA) in patients with this tumor in the maxillofacial surgery department of Charles Nicolle Hospital between 1997 and 2022.
Methods
This is a descriptive, retrospective, monocentric study of patients MA in the maxillofacial surgery department of Charles Nicolle Hospital between 1997 and 2022. Inclusion criteria: all patients with MA documented by anatomopathological study were included in the study. Non-inclusion criteria: We did not include patients with maxillary, extraosseous or metastatic ameloblastoma. Exclusion criteria: We excluded patients for whom no data on evolution were available, as well as those lost to follow-up. Data were collected using a data collection form that included socio-demographic, clinical, radiological, therapeutic, anatomopathological, and follow-up parameters. We calculate absolute frequencies and relative frequencies (percentages) for qualitative variables. We calculate means, medians and standard deviations, and determine extreme values for quantitative variables. Comparisons of 2 means on independent series are made using Student’s T-test for independent series and the non-parametric Mann-Whitney test. Comparisons of percentages on independent series are made using Pearson’s chi-square test, and in the case of non-validity, Fisher’s 2-tailed exact test. Recurrence-free survival data will be studied by establishing survival curves using the Kaplan Meier method. To identify independent factors following each uni-variate analysis, Cox regression will be used, considering factors with a significance level (p) of less than 0.2. The measure of association will be the Hazard Ratio (HR) and its 95% confidence interval (95% CI). In all statistical tests, the significance threshold was set at 0.05.
Results
The recurrence rate after the first treatment was 30%. The median time to first recurrence was 47.6 months. Six patients had a second recurrence. Recurrence was not influenced by gender. Recurrence-free survival was significantly associated with anterior mandibular location (P = .033).
The recurrence rate was non-significantly higher for unilocular tumor images. From a tumor size of 5 cm, the recurrence rate was estimated at 58%. The presence of intra-tumoral bone septa (Figure 1) was significantly associated with a lower recurrence-free survival rate (P = .042). The presence of an impacted tooth was significantly associated with a lower recurrence rate (P = .043). Cortical rupture (CR) was significantly associated with a higher rate of recurrence (P = .045).
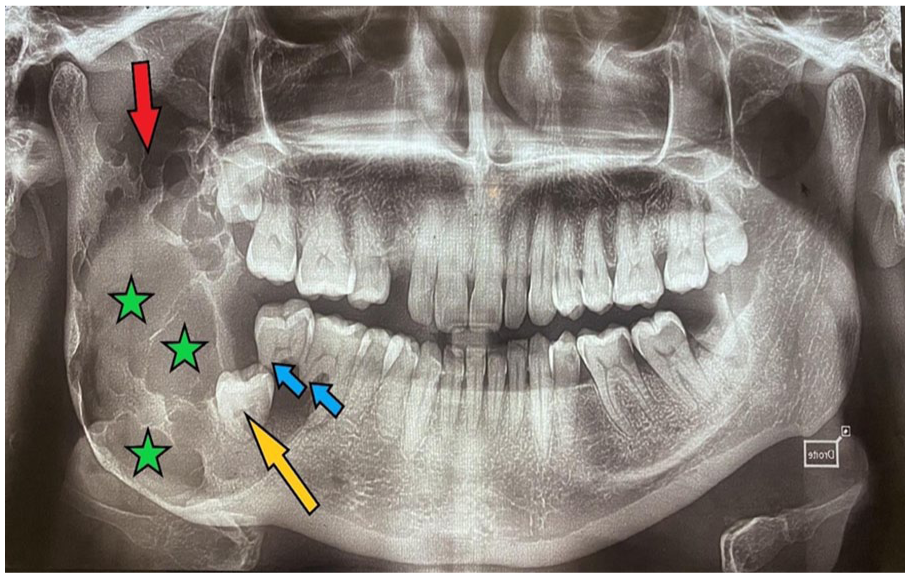
Panoramic X-ray of a posterior multi-cystic ameloblastoma presenting as multilocular clarity (stars) reaching the coronoid process and sigmoid notch (red arrow) and sparing the condyle with the 48 included in the tumor. Note the rhizalysis of 46 and 48 (blue arrows).
Thirteen percent of our patients underwent radical treatment versus 87% (n = 47) who underwent conservative treatment that is, tumor enucleation (Figure 2). Radical treatment, which was mandibulectomy (Figure 3), was associated with a non-significantly high recurrence-free survival rate (P = .343). Extraction of the 4 neighboring teeth (2 upstream and 2 downstream) was performed in 54% of AM cases in our study. The association with a low recurrence rate was significant (P < .001).

Residual cavity after enucleation and supported bone curettage for the management of anterior mandibular ameloblastoma.
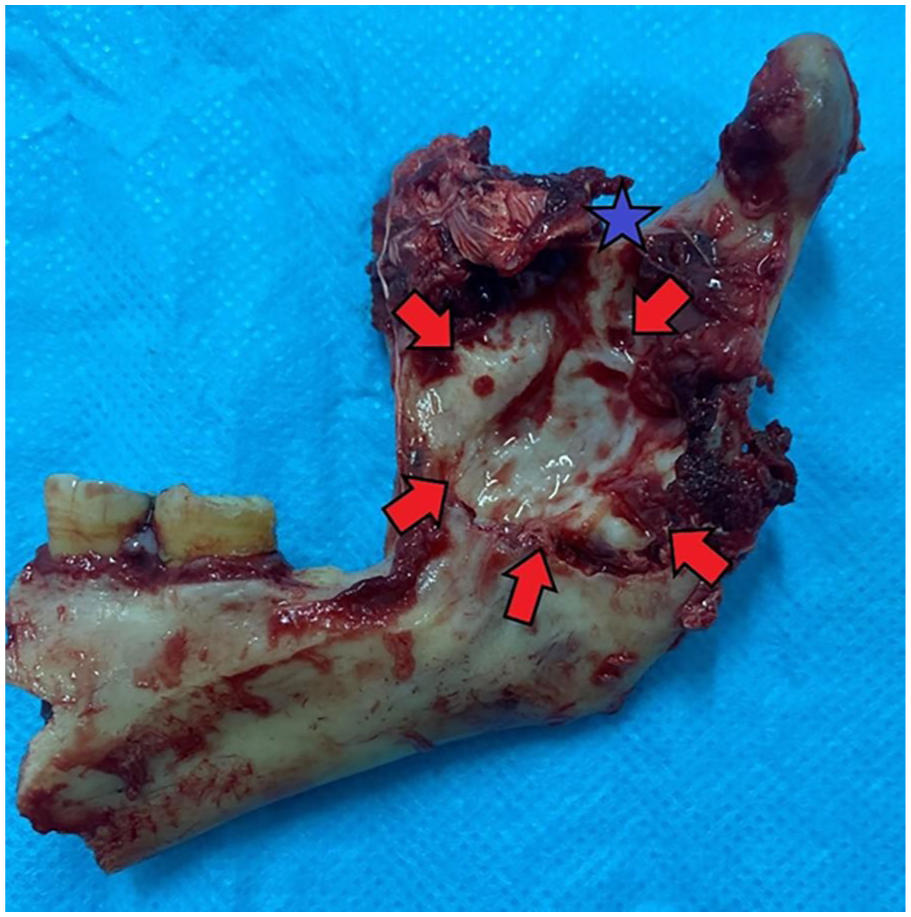
Interrupting mandibulectomy with disarticulation for recurrent posterior unikystic ameloblastoma. The tumor ruptured the cortex (red arrows) and reached the sigmoid notch (blue arrow).
The histological type was multicystic (conventional) in 56% of cases and unicystic in 46%.
For multi-cystic ameloblastoma, the follicular subtype was the most frequent (n = 14 or 47% of multi-cystic ameloblastomas). No histological subtype of multicystic ameloblastoma (MCA) was specified. The mean age of onset of MCA was 38 years in our series, and that of unicystic ameloblastoma (UCA) was 29 years. Our study demonstrated that UCA can present on imaging as multilocular clarity and vice versa. Indeed, 12% of UCA were multilocular on panoramic x-ray, and 14% of MCA were unilocular in radiological presentation. The recurrence rate of MCA was higher than that of UCA in our series (45% and 12% respectively). The multicystic histological type had a statistically significant higher recurrence rate than AMU (P = .049). Among the histological subtypes of conventional ameloblastoma (MCA), the acanthomatous and desmoplastic subtypes did not recur. The plexiform histological subtype was associated with a significant number of recurrences (5 recurrences among 6), but the difference was not significant compared with recurrence of the follicular subtype (P = .09).
Discussion
Imaging Data
Location
In our study, we found that most MA occurred in the posterior part of the mandible (78%). This result is in line with the literature.1,3-6 Indeed, Ling Bi et al found that posterior localization accounted for 93% of MA cases. 1 This location was not significantly associated with recurrence. On the other hand, our study found a significant association between anterior mandibular location and less recurrence (P = .033). This may be explained by the predominance in our study of the unilocular radiological image in the anterior location, which is surgically more controllable. There are no studies in the literature that have concluded that a mandibular region is involved in ameloblastoma recurrence.
Image Nature
We found that the rate of MA recurrence in our study was non-significantly greater when a unilocular image was involved. Our result is consistent with a Chinese retrospective study involving 158 cases of ameloblastoma. 1 However, it has always been known that MA presenting as a multilocular image on imaging is more likely to recur. 4 This is because the majority of MA presenting as multilocular on imaging belong to the multicystic histological subtype known for its infiltrative and therefore recurrent potential.3,7,8 Our result could be explained by the presence of small unilocular tumors on imaging that had the histological characteristics of a MCA, 8 but these lesions were treated conservatively, resulting in a higher recurrence rate. These results illustrate the importance of thorough curettage of tumor cavities whenever conservative treatment is used.
Impacted Tooth
Sixteen percent of our patients had a tooth embedded in the tumor. These patients showed no significant recurrence (P = .043). This result is consistent with a study by Ling Bi et al who found a significant association between recurrence and the presence of an impacted tooth, notably the third molar. 1 This association may be explained by the fact that the posterior zone of the mandible is the preferred location for both ameloblastoma and impacted third molars.9,10 An impacted tooth contains several epithelial components with the potential to develop various neoplasias and lesions such as ameloblastoma. Therefore, as an etiological factor, when the tumor is correctly removed, together with the impacted tooth and its various histological components, recurrence is unlikely to occur. 1
Intratumoral Bone Trabeculations
Fifty percent of patients in our series showed intra-tumoral bone septa on imaging. CT was more sensitive than orthopantomogram in detecting them. We found a significant association between these septa and recurrence (P = .042). Indeed, in the case of a multilocular image, the presence of these bony trabeculations points to an infiltrating ameloblastoma, that is, a multicystic ameloblastoma. 8 It is therefore important to collapse these septa to minimize the risk of recurrence.
Cortical Bone Break
CR was present in 80% of patients in our study. It was detected by CT scan and was significantly associated with a high rate of recurrence (P = .045). Several studies have found a strong association between CR and recurrence of AM.3,11-13 Zheng et al found that the only predictive factor for recurrence was CR, and that it provided information on the tumor’s pejorative biological characteristics. 13 Yang et al consider bone cortical invasion to be an independent factor in AM recurrence. 11 A Chinese study considered cortical bone perforation to be the only reliable predictor of recurrence, independently of other factors. 13
Tumor Size
In our study, the recurrence rate was estimated at 58% from a tumor size of 5 cm. Several studies in the literature consider tumor size as an RF for recurrence.1,4,12,14,15 Au et al concluded in their retrospective study including 128 MA that there was a significant association between tumor size and recurrence.
Pathological Data
MCA was present in 56% of patients in our series. The follicular histological subtype was the most frequent (10/30). UCA was found in 44% of patients. These results are consistent with the literature, as demonstrated by a retrospective Chinese study of 158 cases of ameloblastoma, which found that MCA was present in 60% of patients. 1 Our study demonstrated that UCA can present on imaging as multilocular clarity and vice versa. Indeed, 12% of UCA were multilocular on panoramic x-ray, and 14% of MCA were unilocular in radiological presentation. According to several publications on the subject, unilocular or multilocular images can be observed with both types of ameloblastoma.8,16,17 The recurrence rate for MCA was higher than for UCA in our series (45% and 12% respectively). This result is consistent with the literature.18-21 Hendra et al concluded in a systematic review of the literature and metanalysis that the recurrence rate of MCA was higher than that of UCA irrespective of treatment, due to the more aggressive and infiltrative nature of MCA.14,18,22 In our pathology reports, we did not find any histological subtypes specified for UCA. Several studies in the literature have found that patients with the mural subtype in UCA have a higher probability of recurrence than those with the luminal or intraluminal subtypes.13,21 Indeed, a retrospective Chinese study of 128 MAs concluded that the mural subtype of UCA can penetrate bone through the cystic cavity and proposed treating this subtype as an MCA. 4 The mural subtype can only be identified by meticulous histological examination of the surgical specimen. A biopsy does not represent the entire lesion. Consequently, the diagnosis of mural subtype ameloblastoma may go undetected even after a preoperative diagnostic biopsy. 4
Therapeutic Data
Conservative Versus Radical Treatment
Thirteen percent of our patients had radical treatment versus 87% (n = 47) who had conservative treatment. Radical treatment was associated with a non-significantly higher recurrence-free survival rate (P = .343). This result is in line with several studies, including several systematic reviews of the literature and meta-analyses, which have all concluded that radical treatment, irrespective of histological type, is effective in controlling recurrence.1,18,20,23 The goals of surgery must be curative removal of the tumor while minimizing the functional and esthetic consequences of ablative surgery. A radical approach (marginal or segmental resection with adequate margins) guarantees complete removal of an MCA, thus reducing the risk of recurrence.
The management of UCA is the subject of much debate, and is grouped into 3 categories: enucleation, marsupialization (or decompression) and radical resection. Several studies advocate a more conservative approach to the management of UCA.14,20,24,25 Conservative treatment is associated with an unfavorable prognosis, while the various complications associated with radical treatment pose a significant disadvantage. A recent attempt to define the optimal treatment for MA in children indicated that the luminal and intraluminal subtypes are less aggressive and respond well to conservative treatment, in contrast to the mural type. 21
Extraction of 2 Teeth Upstream and Downstream
Extraction of the 4 neighboring teeth was performed in 54% of MA cases in our study. The association with a low recurrence rate was significant (P < .001). Indeed, the retention of teeth in the alveolar bone surrounding the lesion presents a risk of subsequent recurrence. 8 Extraction of the 4 neighboring teeth was performed in 54% of MA cases in our study. The association with a low recurrence rate was significant (P < .001). Indeed, the retention of teeth in the alveolar bone surrounding the lesion presents a risk of subsequent recurrence of the lesion during treatment.3,8 It is important to extract neighboring teeth, as the tumor tends to spread between the tooth roots in question. The extraction of teeth close to or adjacent to the lesion concerns teeth located within the safety margins. 8 These same margins are conditioned by the potential of tumor cells to microscopically exceed macroscopic tumor limits by 10 to 20 mm.1,5,26,27
Outlook and Recommendations
■ Careful questioning can reveal any history of previous dental treatment, as well as the patient’s habits.
■ Given the association between smoking and BRAF V600 mutation, patients should be strongly advised to stop smoking.
■ Imaging must be meticulously interpreted to watch for the slightest sign predictive of recurrence: posterior localization, presence of intra-tumoral bone trabeculations, CR and soft tissue invasion, tumor size greater than 5 cm. Signs of a good prognosis include anterior localization, tumor size less than 5 cm, unilocular image, and intra-tumoral inclusion of a tooth.
■ Biopsy remains a controversial procedure, since it increases the risk of tumor dissemination and false-negative Ackermann mural. Biopsy is indicated for diagnostic purposes in the case of non-specific unilocular images.
■ An anterior unilocular image can be treated conservatively.
■ In the case of a posterior unilocular image without intra-tumoral tooth inclusion, or in the case of a multilocular image, signs predictive of recurrence should be sought. Their presence is an indication for segmental or marginal mandibulectomy.
■ If the pathological report concludes that the ameloblastoma is multicystic or unicystic, further bone resection is indicated if the initial treatment was conservative.
Conclusion
The following factors were significantly and independently associated with the occurrence of recurrence: cortical rupture, presence of intra-tumoral bone septa and multicystic histological type.
The following factors were significantly and independently associated with less recurrence: anterior mandibular location, presence of an impacted tooth in the tumor, extraction of 2 teeth upstream and downstream of the tumor during surgical treatment.
This updated recurrence factors study would enable us to classify patients with MA according to their level of risk of recurrence, and thus adjust their surgical management (Figure 4).
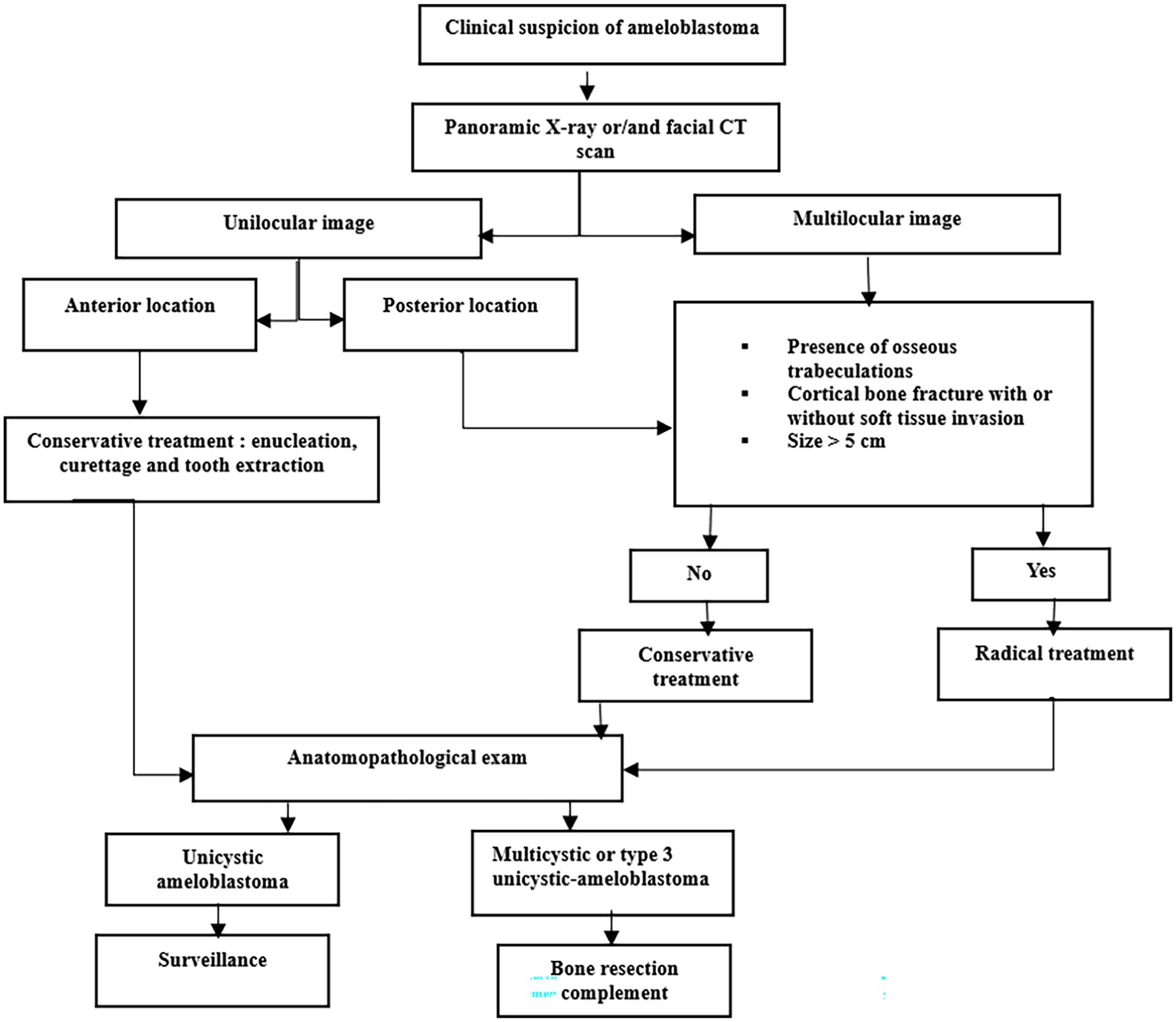
Management chart for suspected mandibular ameloblastoma.
Footnotes
Ethical Considerations
Institutional Review Board approval was not required.
Consent to Participate
Not applicable. This study was conducted retrospectively from anonymized medical records and did not involve direct participation of human subjects.
Consent for Publication
We have obtained a written informed consent from the patient’s parents to publish this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.