
Abstract
There has been much debate about the utility of the Glasgow Coma Scale (GCS) in terms of predicting outcomes of pediatric trauma. While some studies state GCS can reliably predict mortality outcomes, others have stated that its dependence on verbal responses and interobserver discrepancy limit its application. In pediatric facial trauma, there is a relative lack of variables that predict functional outcomes. Applying GCS to this patient cohort may elucidate its role in this patient population and possible inclusion in a patient’s treatment decisions. This retrospective examination uses a multi-center database to evaluate pediatric (<18 years old) facial trauma patients (N = 1094) visiting 2 level-one trauma centers from 2020 to 2022. The number of complications, consultations, moderate and significant physical impairments, number of surgical interventions, and deaths were compared to the GCS score, number of soft tissue injuries and fractures, and length of hospital stay. For both AHCMC and AHWFB, a lower GCS score was the factor that most strongly correlated to post-trauma complications, significant physical impairment, and deaths (P < .001). Acknowledging the correlation the GCS score has with outcomes can help guide healthcare decisions and expectations by informing patients and their families of potential complications based on their initial post-trauma status.
Introduction
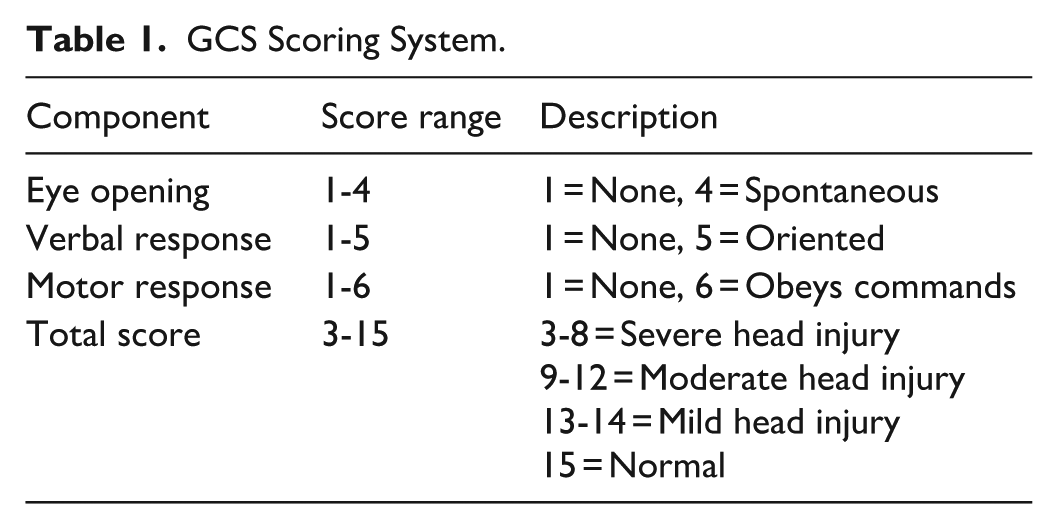
The Glasgow Coma Scale (GCS) is a scale of 3 to 15 that objectively measures the level of consciousness in a patient. The table below (Table 1) summarizes the GCS components and scoring system. 1 Although the GCS score is commonly documented in healthcare systems and widely used in NIH and national databases, there is debate about its utility in application and ability to predict outcomes, especially in pediatric patients. 2
GCS Scoring System.
Previously, the GCS score has been used to aid in the decision-making process of the management and treatment of head and brain injuries and has been established as a reliable factor in evaluating patients’ health status. GCS score has been used to track patients’ recovery over time because there is a relationship between progressively decreasing GCS scores from 15 to 3 after a head injury and increasing mortality.2,3 This relationship allows the GCS to track recovery or lack thereof, but also be used to predict future progress based on the trajectory of GCS scores. Other studies have found similar results that GCS score on admission is an independent predictor of outcomes of traumatic brain injuries and is prognostic of brain injury severity and mortality. 4 In addition to brain injuries, there is a significant correlation between decreased consciousness and skull fractures. 5 To adjust for patients with severe verbal impairments, the motor score has been used more than the eye and verbal scores which allows the GCS to be applied to a greater population of patients. 2 Specifically concerning pediatric patients, studies have established the ability of the GCS to serve as an accurate measure of children’s neurological status and reliably predict outcomes of pediatric head injuries, even though the skulls and brains of children and adults differ. 6
On the other hand, shortcomings of the GCS have been noted. First, patient charts often only include the total GCS score and not the scores of the individual components, which may hinder the reliability of the scale as healthcare providers do not know the details of responsiveness. 2 Second, although various modifications have been suggested, there is no universally accepted version of the GCS for patients younger than 5 years old who may not be able to speak or follow instructions. 2 This complication also applies to older patients who are mentally or physically impaired or who encounter language barriers. 2 Third, there may be poor interobserver agreement which argues against solely using the GCS score to make clinical decisions. 7
Other studies have noted the limitations of the GCS in predicting outcomes of traumatic brain injuries (TBI). A low GCS score does not always accurately predict the outcome of patients with a severe TBI because pediatric patients with a GCS score of 3 to 5 (in the absence of ischemic injury) can recover independent function. 8 Another study found that the overall GCS score does not have a linear relationship with the mortality of children with severe head injuries whereas the motor component of the GCS does, which raises the question if the eye response and verbal response components should even be recorded. 9
This study aims to identify the ability of the GCS to predict outcomes of pediatric facial trauma related to special consultations and surgeries, complications, physical impairments, and death. Knowing the utility of the GCS could argue for or against the importance of obtaining and recording it across larger healthcare systems. Additionally, identifying an objective method to predict outcomes of pediatric facial trauma could help guide treatment decisions by serving as justification, and could provide patients and their families with information to create preliminary care plans and manage their expectations of outcomes.
Methods
Data was obtained from a database that includes incidents of facial trauma of pediatric patients (less than 18 years of age) between January 1, 2020, and December 31, 2022 who were cared for at either level-one trauma centers in North Carolina. Data was compiled in a REDCap survey.10,11
Recorded data included information on patient demographics, past medical history, trauma history, trauma care/management, and outcomes. All patients had either a fracture or soft tissue injury (contusion, abrasion, laceration, burn, or puncture wounds) involving the face or skull. Common specialty consultations included plastic surgery, neurosurgery, ENT, ophthalmology, dentistry, radiology, and trauma care. Common post-trauma complications were concussion, traumatic brain injury, facial deformity, scarring, seizures, airway/nasal airway obstruction, headaches, nasal/septal deviation, and cranial nerve injuries leading to paralysis, weakness, and sensory deficits. Moderate physical impairment was classified as some deformity and scarring or issues with cranial nerves (sensory and/or motor) that did not cause extensive deficits. Significant physical impairment was classified as extensive deformity and scarring or debilitating issues with cranial nerves (sensory and/or motor).
An institutional review board-approved retrospective analysis was conducted in which objective information pertaining to the patient’s facial injuries (GCS score, number of soft tissue injuries and fractures, and length of hospital stay) was compared to information on patients’ health outcomes (number of complications, consultations, moderate and significant physical impairment, number of surgical interventions, and deaths). The data was analyzed using IBM’s SPSS software for statistical analysis. 12
Results
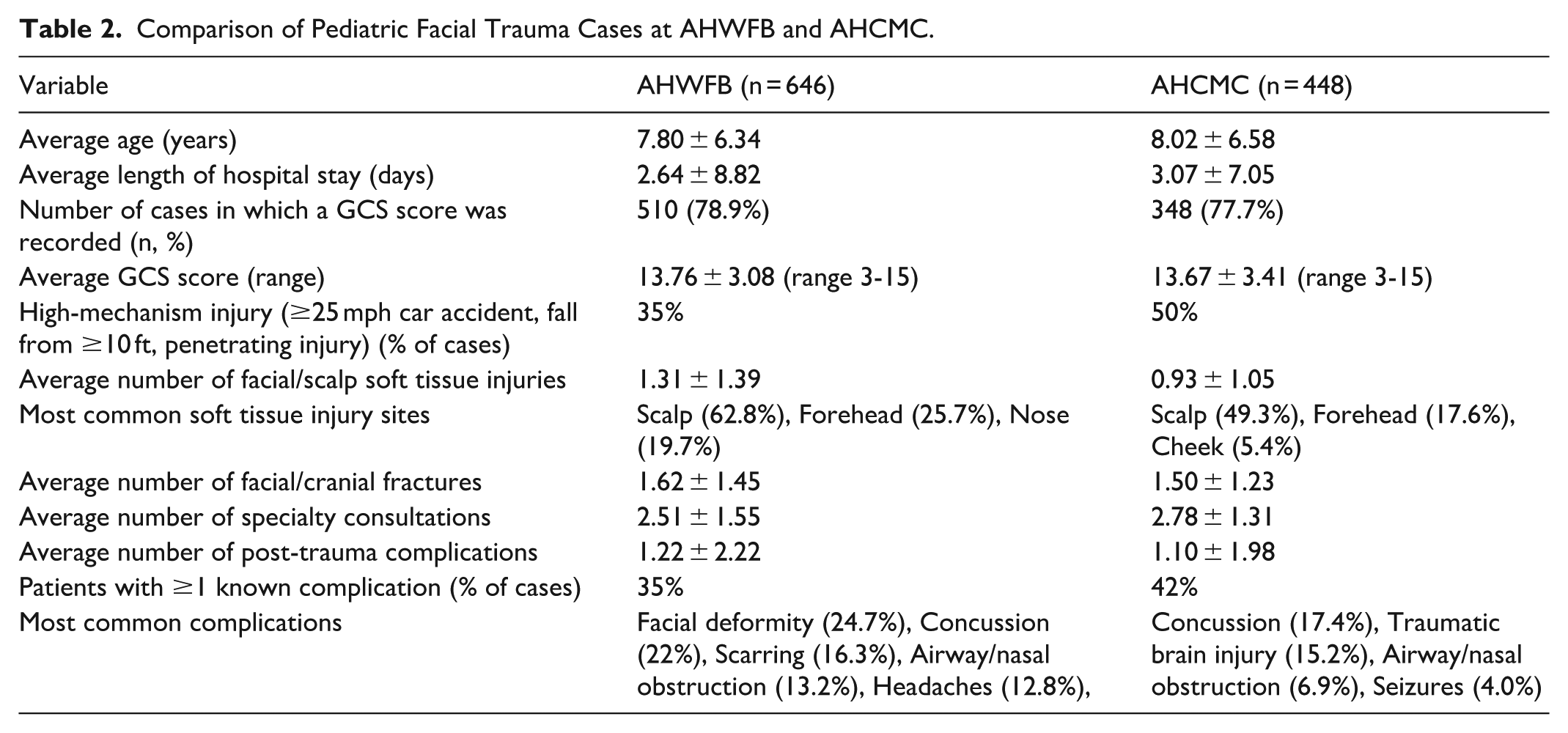
A total of 646 pediatric facial trauma cases were identified at AHWFB from 2020 to 2022, and 448 cases at AHCMC. Table 2 summarizes demographic and clinical characteristics for both cohorts.
Comparison of Pediatric Facial Trauma Cases at AHWFB and AHCMC.
Univariate correlations for AHWFB and AHCMC were analyzed separately to better examine the predictors of complications for each institution. Correlations for AHWFB and AHCMC are compiled in Tables 3 and 4, respectively. The sample size of GCS scores is less than that of the other variables because some patients did not have a recorded GCS score.
Specific Correlations for AHWFB.
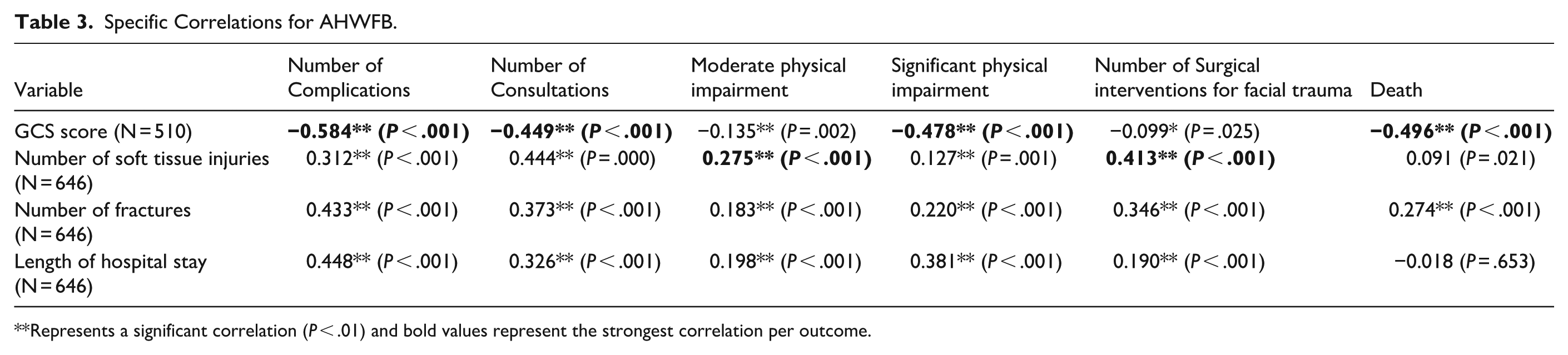
Represents a significant correlation (P < .01) and bold values represent the strongest correlation per outcome.
Specific Correlations for AHCMC.
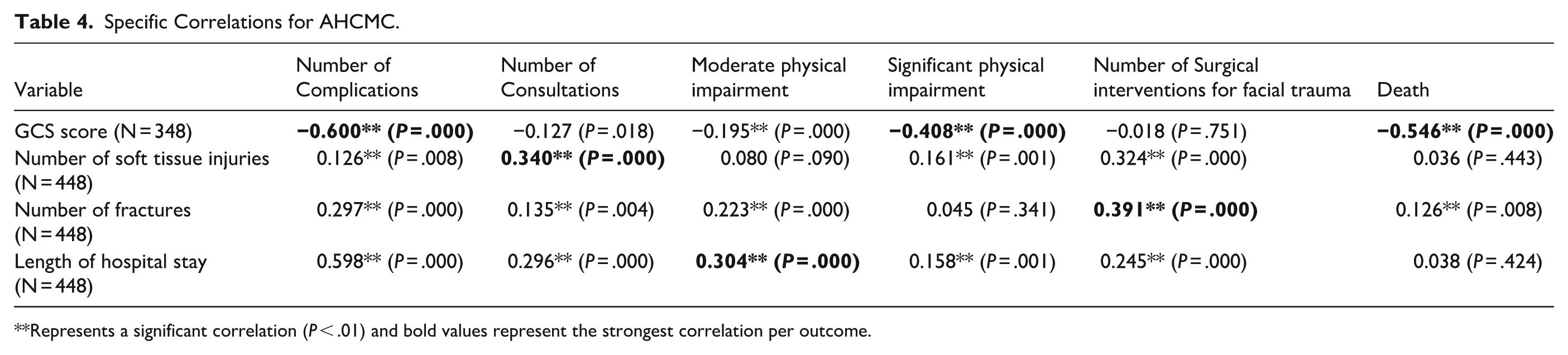
Represents a significant correlation (P < .01) and bold values represent the strongest correlation per outcome.
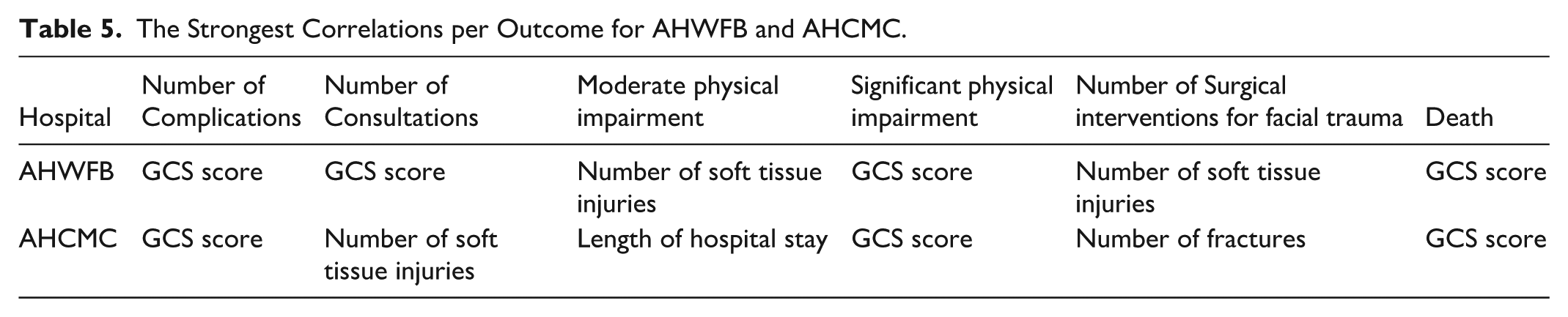
The variables with the strongest correlation for complications, consultations, moderate and severe physical impairments, surgical interventions, and death are summarized in Table 5. GCS had the largest correlation with the number of complications, significant physical impairment, and death at both AHWFB and AHMC, as well as with the number of consultations at AHWFB.
The Strongest Correlations per Outcome for AHWFB and AHCMC.
The following figures demonstrate the distribution of each GCS score for the patients with post-trauma complications of moderate physical impairment, severe physical impairment, and death for AHWFB (Figure 1) and AHCMC (Figure 2).
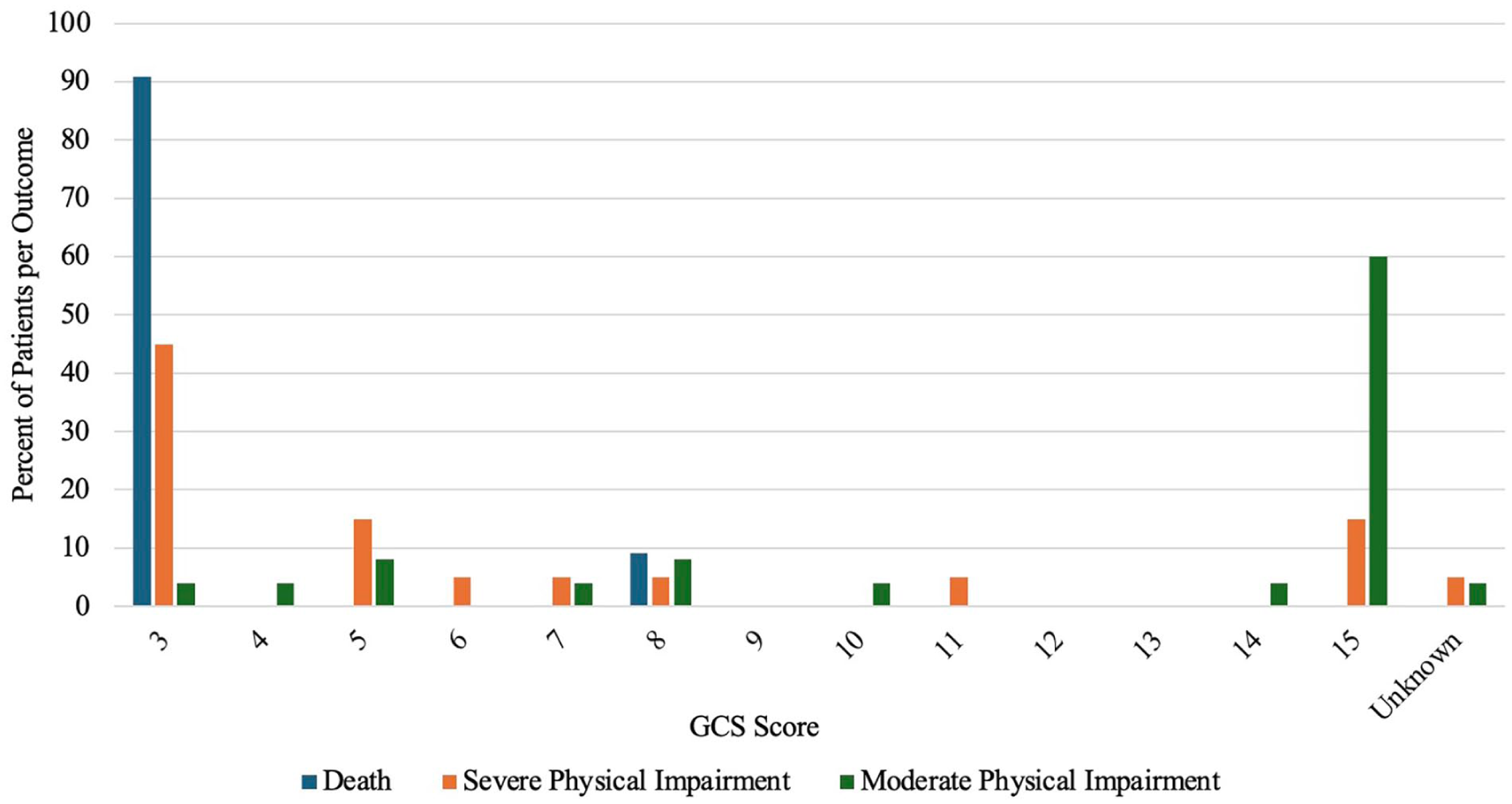
Distribution of GCS scores for 3 outcomes for AHWFB.

Distribution of GCS scores for 3 outcomes for AHCMC.
Discussion
At AHWFB and AHCMC, 2 large North Carolina hospitals, GCS score, compared to the length of hospital stay and the number of injuries, was found to have the highest correlation and therefore the greatest predictive potential for the number of post-trauma complications, significant physical impairments, and deaths due to pediatric facial trauma. In both hospitals, the majority of patients who experienced severe physical impairment or death had a GCS score of 3, whereas the majority of patients with moderate physical impairment had a GCS score of 15. Additionally, GCS scores had the greatest predictive potential for the number of required consultations at AHWFB.
Acknowledging the correlation the GCS has with outcomes can help guide healthcare decisions and expectations by informing patients and their families of potential complications based on their initial post-trauma status. Using an objective score to quantify mental status following facial trauma can assist physicians to track and measure progress, or lack of progress, of patients. Some healthcare centers have already used predictive outcomes to improve the outcomes of pediatric head injuries by employing targeted preventative measures and treatments in vulnerable populations. 6 This score also helps various healthcare professionals be congruent with the understanding of the mental status of the patient. This information, paired with an explanation of what the GCS is and what scores indicate, could provide empirical data to patients and families who are often facing the unknowns concerning current and future health status.
This study supports previous research that found that the GCS score does correlate with mortality. 4 Additionally, this study adds the extra component that GCS scores correlate with the number of post-trauma complications and significant physical impairments. The significant correlations between GCS scores and various outcomes demonstrate that the GCS can be applied to pediatric populations, which has previously been a point of contention and noted limitation due to communication challenges and developmental variability. The significant correlations also refute the assertion that the GCS score is not a reliable measure in pediatric patients. 2
Limitations include small sample size and lack of control of variables such as past medical history and pre-trauma health status. Future studies could evaluate the correlations of outcomes and complications with the subscores of GCS to further determine the reliability of the total GCS score compared to its subsections. This could further answer the question if the motor response alone should be used in children. 9 A similar study model could also be applied to adult patients and patients with injuries other than facial trauma.
Conclusions
This study demonstrates that the Glasgow Coma Scale (GCS) score has the strongest correlation with adverse outcomes, specifically post-trauma complications, significant physical impairments, and death, among pediatric facial trauma patients at 2 major North Carolina hospitals. This study contributes to ongoing discourse by affirming the applicability of GCS score in pediatric populations and its ability to contribute to healthcare decisions.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Wake Forest University School of Medicine and Wake Forest Baptist Medical Center (protocol code 00093445 approved on 2/23/2023).
Consent to Participate
Patient consent was waived due to the retrospective nature of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Christopher Runyan is a member of the Editorial Board of FACE and did not take part in the peer review or decisionmaking process for this submission.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.