
Abstract
Introduction:
The aim of the present study was to determine the extent of mouthguard use, the knowledge about oral health and dental traumatology, the self-reported oral health and oral health behaviors as well as the frequency of oral trauma in a population of contact sports athletes in the North West of Italy.
Methods:
The athletes of different contact sports clubs based in the Province of Novara, Italy were enrolled for this study. Athletes who agreed to participate in the study completed a questionnaire regarding demographic data, personal oral hygiene and care, the use of mouthguards, their past medical history, and their knowledge regarding dental traumatology. All the included athletes completed the OHIP-14 questionnaire too.
Results:
Fifty-five completed questionnaires were returned (15 females, 40 males). The mean age of the surveyed population was 25.54 years. The most represented contact sports in the study population were rugby and kick boxing. On the whole, 53 athletes out of 55 reported to use mouthguards. Most athletes (22 subjects, 40%) used the mouthguard 3 times a week. Most athletes used mouth-formed (boil and bite) mouthguards (40 subjects, 76%).
Conclusions:
The findings highlight the need to improve athlete education on the management of dental trauma. Given that the majority of interviewees are not adequately prepared to deal with these events, it is essential to implement specific educational programs that cover the different types of dental trauma and their immediate treatments.
Introduction
Dental and maxillofacial injuries frequently occur during participation in sports, and particularly in contact sports. Although all sport activities carry a risk of orofacial injury due to falls, collisions and contact with hard surfaces, the increasing popularity of contact sport activities together with the high risks associated with these disciplines have led to a progressive and continuous increase in sport injuries.1-4
In particular, martial arts are associated with a high risk of oral injury, with dental damages that can reveal to be irreversible and may determine functional, esthetic, and psychological impairments.1,5-7
The face and the teeth are among the most exposed body regions to trauma, so that when they are involved, lesions to the teeth or facial bones are frequent to reach more extreme injuries such as cerebral damages or death.1-3,6-12
Dental and facial trauma during sport activities implies subsequent functional, psychological, esthetic and economic impacts, so that the importance of prevention should never be underestimated. The usefulness of wearing a mouthguard in reducing the incidence of dental and orofacial injuries has been showed in several studies in the last decades and among several different sports, thus preventing dental injuries.1,2,4-7
Prevention of dental and orofacial injuries should be one of the prime emphases of sports dentistry. However, many athletes find difficult to tolerate mouthguards and their knowledge regarding orofacial injuries and first aid in dental traumatology is often limited if not insufficient. Furthermore, in the literature, athletes often seem to experience and inappropriate oral health.1-6,9
The education and the consequent positive attitude of contact sport athletes regarding a correct oral health, a correct behavior in dental emergency situations, as well as a correct mouthguards usage, should be crucial in sports and preventive dentistry.
Therefore, the aim of the present study was to determine the extent of mouthguard use, the knowledge regarding oral health and dental traumatology, the self-reported oral health and oral health behaviors as well as the frequency of oral trauma in a population of contact sports athletes in the North West of Italy.
Materials and Methods
The athletes of different contact sports clubs based in the Province of Novara, Italy were enrolled for this study. One hundred surveys were sent out for completion.
Inclusion criteria were: 18 years of age or older, absence of comorbidities, daily contact sport activity (training or competition) at least 5 days a week.
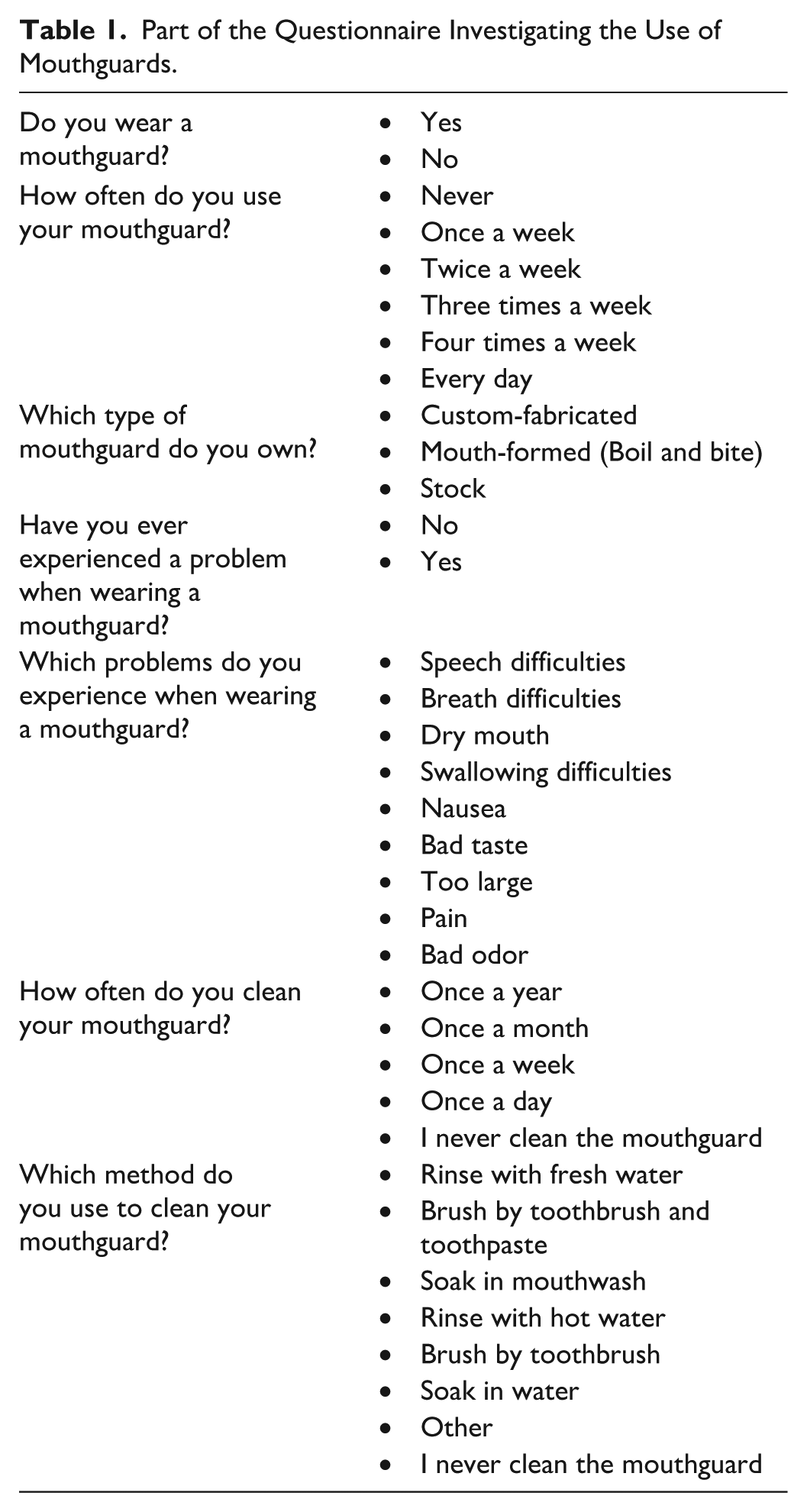
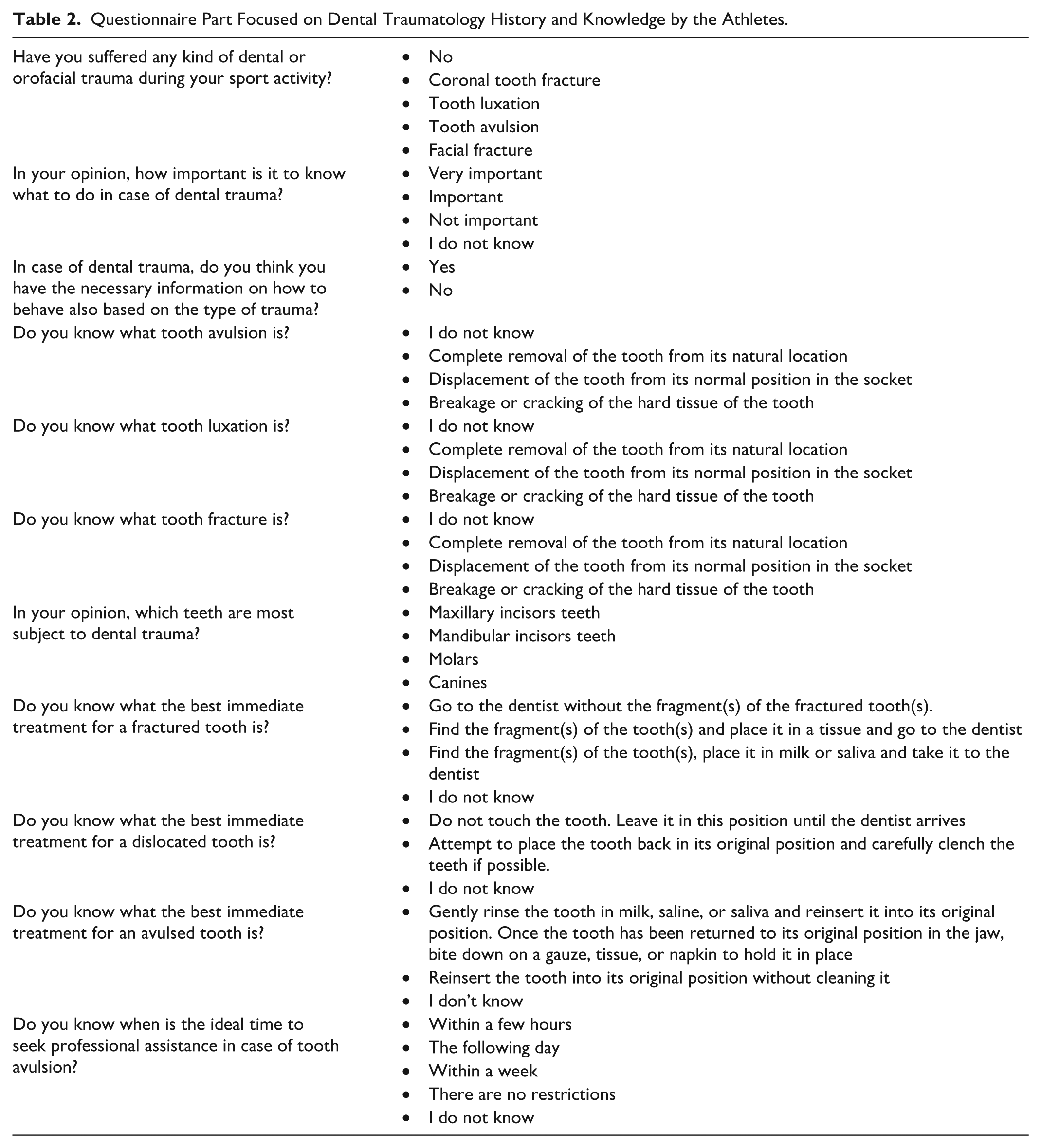
Athletes who agreed to participate in the study completed a questionnaire. The first part of the questionnaire identified the following general information from participants: age, gender, type of sport, smoke and/or alcohol consumption. A second part of the questionnaire focused on personal oral hygiene and care: frequency of teeth brushing, type of toothbrush, use of interdental cleaning devices, frequency of dentist consultation, frequency of professional dental hygiene. A third part of the questionnaire investigated the use of mouthguards (Table 1). The fourth and final part of the questionnaire focused on the history and knowledge of dental traumatology by the athletes (Table 2).
Part of the Questionnaire Investigating the Use of Mouthguards.
Questionnaire Part Focused on Dental Traumatology History and Knowledge by the Athletes.
Then, all the included athletes completed the OHIP-14 questionnaire.
Results
Fifty-five completed questionnaires were returned with a response rate of 55%: 15 athletes were females, 40 were male.
The age distribution of the respondents is given in Figure 1: 39 subjects (the 71% of the study population) were aged 20 to 29 years. The mean age of the surveyed population was 25.54 years (range, 18-58 years; median, 23; SD, 8.58). The most represented contact sports in the study population were rugby and kick boxing with 19 patients each, as depicted in Figure 2, followed by karate, boxing, and Muay Thai. The 54% of athletes (30 subjects) did not smoke, whereas 12 athletes occasionally smoked, 10 athletes reported to smoke less than 10 cigarettes a day, and 3 athletes reported to smoke more than 10 cigarettes a day. An occasional alcohol consumption was reported by 45 subjects, whereas only 7 subjects reported not to drink alcohol, and 3 athletes reported a daily alcohol consumption.
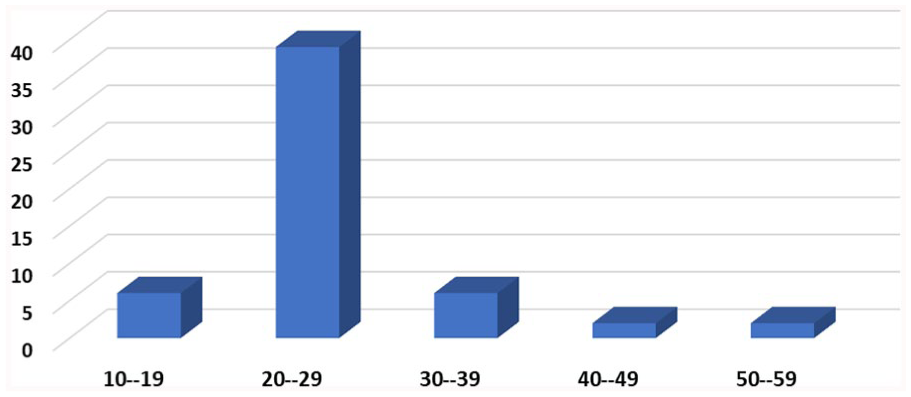
Age distribution of the respondents.
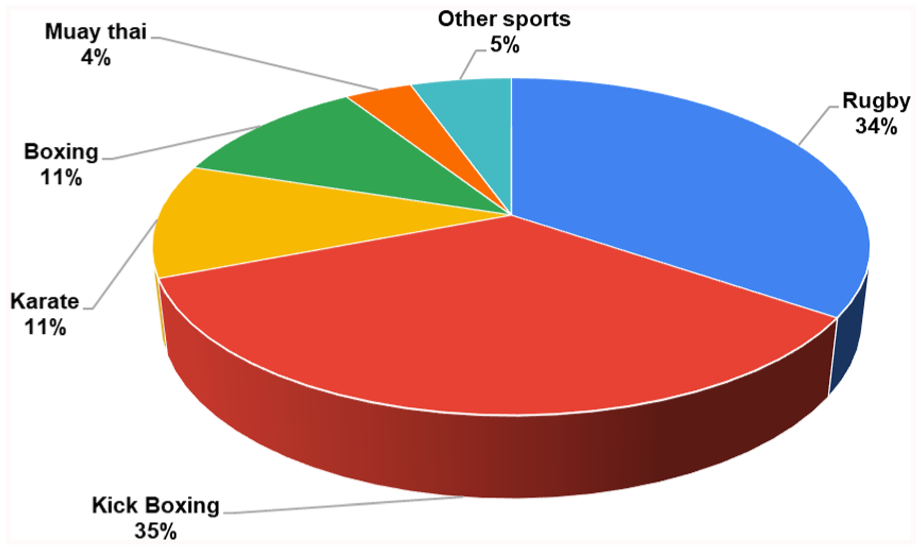
Type of performed contact sports in the study population.
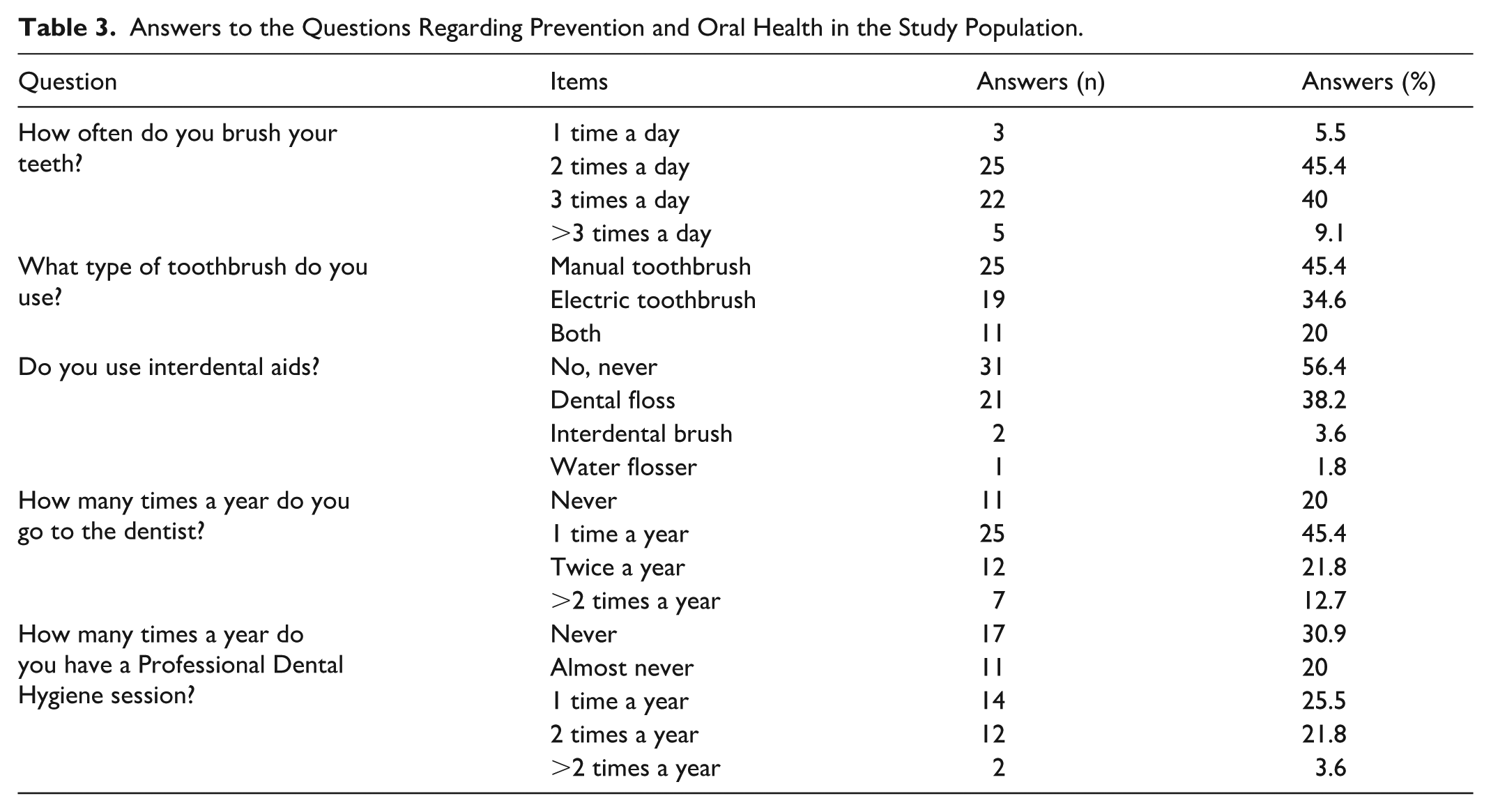
Table 3 resumes the results of the second part of the questionnaire focused on personal oral hygiene and care.
Answers to the Questions Regarding Prevention and Oral Health in the Study Population.
On the whole, 53 athletes out of 55 reported to use mouthguards. Most athletes (22 subjects, 40%) used the mouthguard 3 times a week, followed by those who used it 2 or 4 times a week (10 subjects each, 18%). Most athletes used mouth-formed (boil and bite) mouthguards (40 subjects, 76%), as shown in Figure 3.
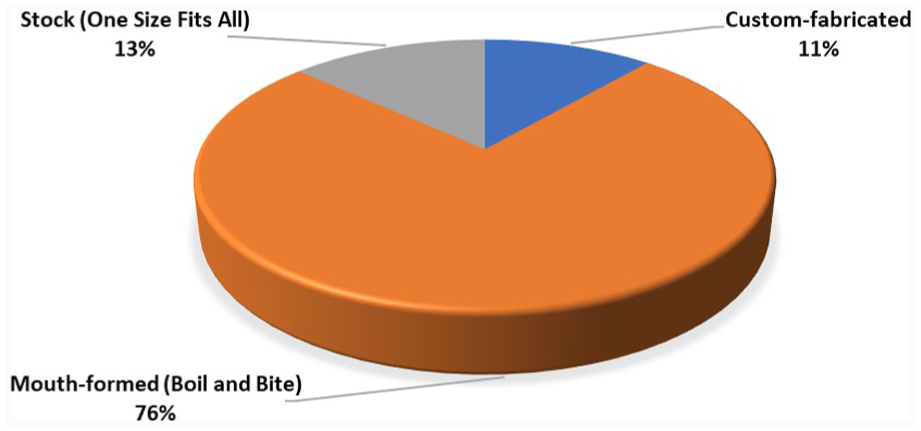
Type of used mouthguards in the study population.
Custom fabricated mouthguards were mostly used by rugby athletes (4 out of 6), whereas stock mouthguards were mainly chosen by karate (3 subjects) or kickboxing (3 subjects) athletes.
Forty-one athletes (77.3%) reported to have experiences some type of problems when wearing their mouthguard: the most frequently reported problems were speech difficulties (31 subjects), breath difficulties (15 subjects), and dry mouth (12 athletes), as depicted in Figure 4. As for the frequency of mouthguard cleaning, most athletes (25 subjects) reported to clean their mouthguard 1 time a week, whereas 19 athletes 1 time a day, 6 athletes 1 time a month, and 3 subjects 1 time a year.
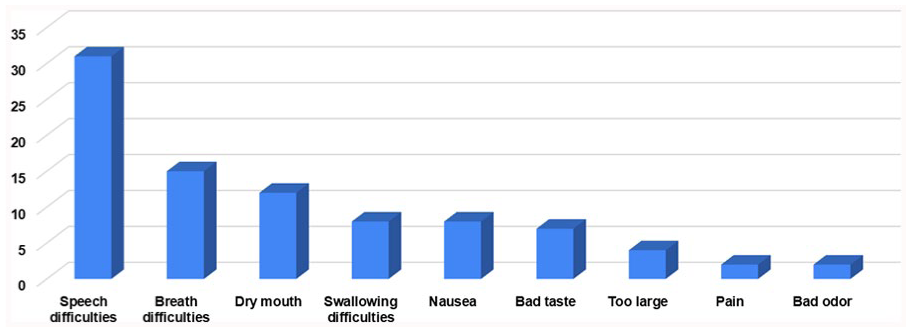
Reported problems while wearing mouthguards in the study population.
The used cleaning methods for the mouthguard are resumed in Figure 5.
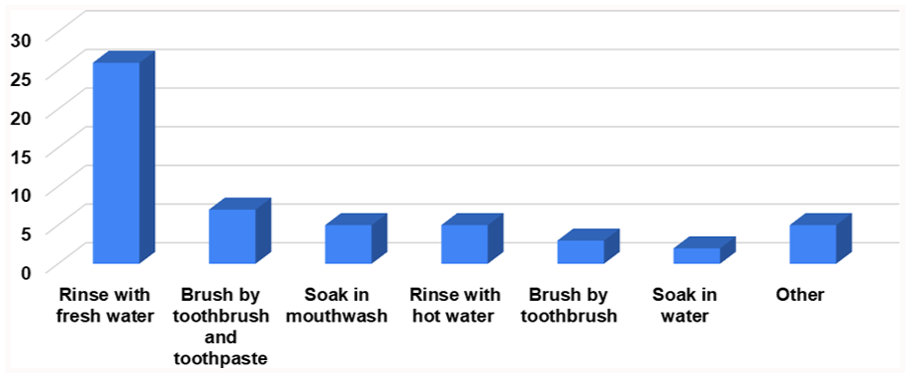
Used cleaning methods for the mouthguards in the study population.
Table 4 resumes the results of the part of the questionnaire focused on the history and knowledge of dental traumatology by the athletes.
Answers to the questions regarding dental traumatology history and knowledge in the study population.
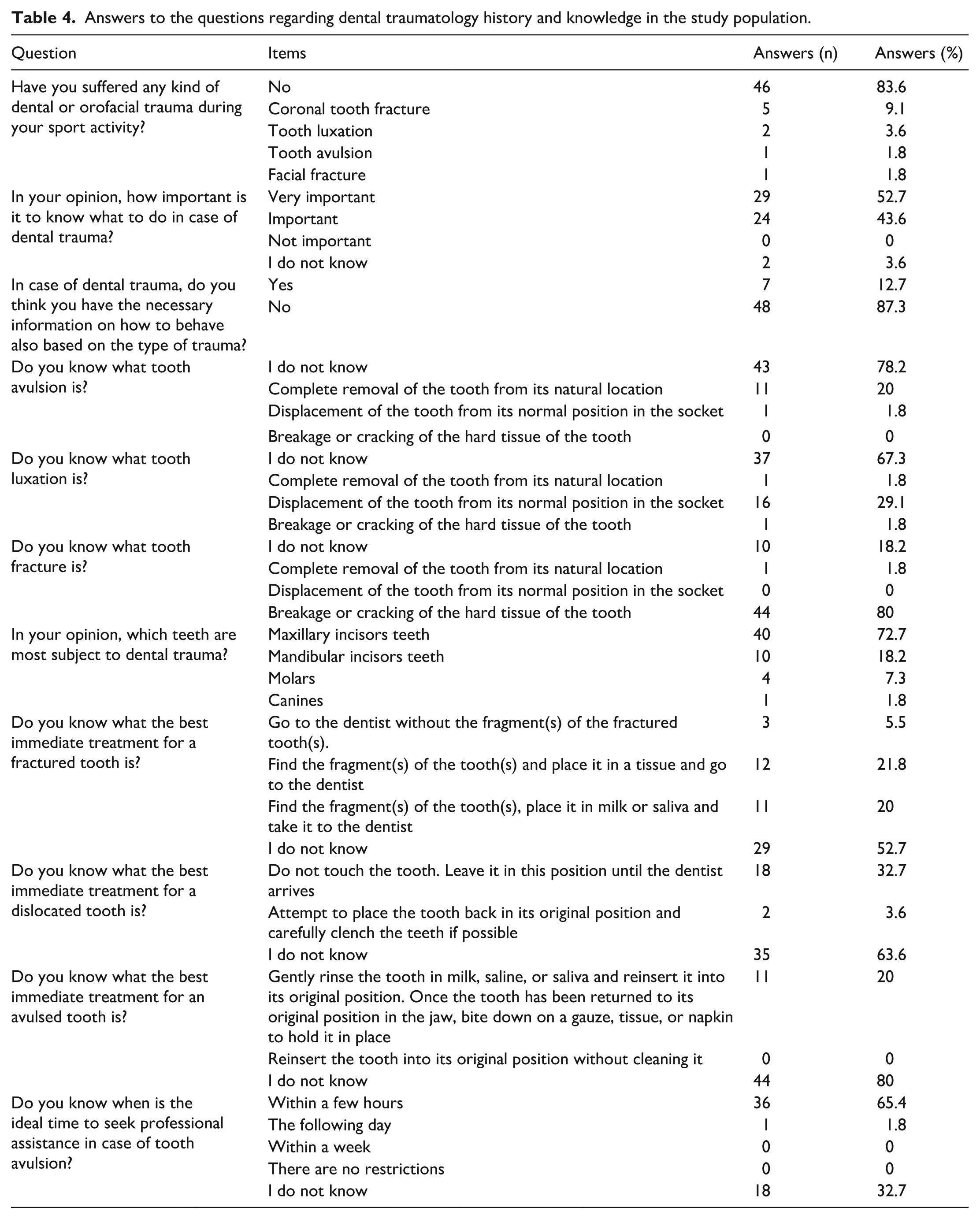
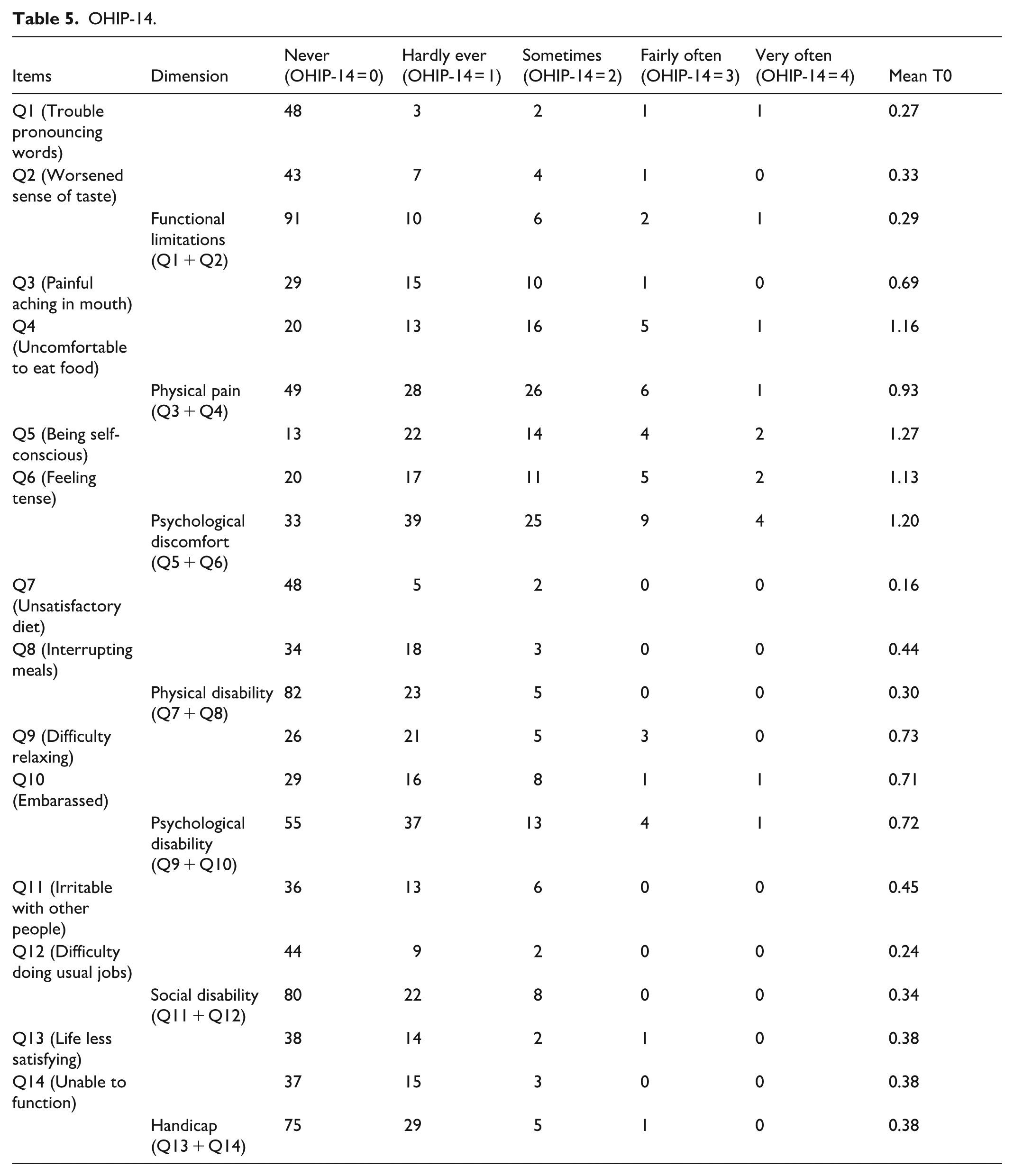
Table 5 presents the results of the OHIP-14 questionnaire in the study population.
OHIP-14.
Discussion
The main purpose of sports dentistry and sports medicine is the prevention of injury and the maintenance of athletes’ health. Dental and orofacial sport injuries often determine lifelong consequences with considerable follow-up costs. Oral hygiene is a critical aspect of overall health, which can have a significant impact on athletic performance. Recent studies have highlighted a high prevalence of oral inflammation, such as gingivitis and periodontitis, among elite athletes.1-6,9 Oral diseases are not only common in athletes, but can also negatively affect their ability to train and compete at the highest levels. Oral health challenges faced by athletes, including dental caries, periodontal disease, orofacial lesions, and dental erosions, are often linked to their lifestyle choices, dietary preferences, health practices, perceptions of health, and oral health knowledge.1-3
The data collected shows that the majority of athletes interviewed said they brush their teeth twice a day or 3 times a day. Fewer participants brushed their teeth only once a day. This distribution shows that the majority of participants have regular brushing habits. However, only a minority use interdental aids such as dental floss or brushes. From the data collected, most participants do not use any type of interdental aid. Among those who use them, dental floss is the most common, while the use of interdental brush is rare.
In the present study, the data collected shows that a good percentage of the athletes interviewed adhere to the recommendations for regular dental visits: 80% of the participants (44 out of 55) declare that they make at least 1 visit to the dentist per year.
From the results of the OHIP-14 questionnaire, it emerges that the dimensions with the highest average values are psychological discomfort (average: 1.20) and physical pain (average: 0.93). In particular, the item relating to the question “Have you ever felt worried about dental problems?” has the highest score (average: 1.27), indicating that worry related to oral health is one of the main sources of discomfort among participants.
Another significant item concerns the question “Have you ever had trouble eating certain foods due to problems related to your teeth, mouth or dentures?,” which obtained the second highest mean value (mean: 1.16), suggesting that functional difficulties related to nutrition are a critical aspect of perceived quality of life.
These results indicate that the control and management of oral diseases can significantly contribute to improving the quality of life of athletes.
The 96% of the athletes interviewed (53 out of 55) regularly use a mouthguard during sporting activity. This is an extremely positive result, reflecting good awareness and adherence to recommendations for the prevention of oral trauma among athletes. In fact, the perception of the usefulness of the mouthguard is predominantly positive: 52 out of 55 participants (95%) believe that its use is useful.
In our questionnaire it was found that the majority of participants (76%) use a “Mouth-formed (Boil and Bite)” type mouthguard, which can be adapted to the shape of the mouth by heating and biting into it. Only 11% use a custom-fabricated mouthguard, despite it being considered the “gold standard” for protection and comfort. This may reflect a lack of access or awareness regarding the benefits of a custom-made mouthguard, or a preference for cheaper, more easily accessible options. When cost becomes a consideration, athletes may prefer the “Mouth-formed (Boil and Bite)” mouthguard rather than the “Custom-fabricated” one, as it is cheaper and easier to obtain. These data highlight that, despite the general preference for the “Custom-fabricated” mouthguard, cost is an important factor in the choice.
Despite the recognition of the importance of the mouthguard and its use by the majority of athletes, in this study many participants (41 of 53 users) reported discomfort during its use. The main problems include difficulty speaking (reported by 58% of users), difficulty breathing (28%), and a feeling of dry mouth (23%). These discomforts can negatively influence the frequency and duration of mouthguard use.
The mouthguard cleaning method varied significantly among participants. The most common method is rinsing with cold water applied by 26 athletes out of 53 total (about 47%), followed by brushing with toothpaste (7 athletes), immersing in mouthwash (5 athletes), rinsing with warm water (5 athletes), brushing mouthguard only (3 athletes), immersing in water (2), Other (5). However, some less effective cleaning methods may increase the risk of bacterial contamination, which requires further attention and awareness among athletes. The FDI says it is crucial to care for your mouthguard properly. Inadequate care causes the mouthguard to deteriorate and lose its protective function. From the evaluation of the results of the literature studies, it is possible to advise athletes who use mouthguards to maintain daily cleaning, adequate storage and regular replacement when necessary. Particularly with regards to daily cleaning, after each use of the mouthguard, it may be recommended to rinse the mouthguard with sterile water and gently brush the mouthguard with a soft bristle toothbrush under sterile running water. Finally, athletes can be advised to conclude their daily cleaning by using a disinfectant spray containing CPC or 0.12% chlorhexidine gluconate, applying the product to the mouthguard, and leaving it to act for at least 60 seconds. Athletes should avoid using alcohol-based solutions, which could deteriorate the mouthguard material. Furthermore, the use of 3% hydrogen peroxide for disinfection or brushing with water and antibacterial soap could be advised too. Finally, it is recommended to dry the mouthguard with a soft cloth. As for an appropriate storage after cleaning, it may be advisable to store the mouthguard in a rigid, ventilated container that is, one with air vents to further reduce bacterial growth. The container should be washed with a non-toxic detergent and warm water, making sure it is completely dry before storing the mouthguard. Finally, regular replacements should be recommended when the mouthguard shows signs of wear or deterioration to maintain effective protection.1-6,9
It is important to communicate to the athletes the information regarding the appropriate combined cleaning, disinfecting and storing tips in a ventilated environment, in order to try to minimize bacterial contamination and ensure safe and hygienic use of sports mouthguards.
From the analysis of the data collected, it emerges that the majority of participants (84%) have never suffered a dental or maxillofacial trauma in a sporting context. Among those who reported trauma, the most common types were fractures (9%), dislocations (3%), and dental avulsions (2%). These findings suggest that, although the prevalence of dental trauma in this sample is relatively low, there is still a variety of injuries that can occur during sporting activities.
The level of awareness of participants on what to do in case of dental trauma appears varied. The 53% of participants consider it “very important” to know how to behave, while 44% consider it “important.” However, 4% of participants did not understand the importance of this knowledge. Furthermore, the majority of athletes (87%) stated that they did not have sufficient information on how to manage dental trauma, revealing a significant gap in practical preparation.
The findings indicate limited knowledge among participants regarding different types of dental trauma. Only 20% of participants were able to correctly define dental avulsion as the complete emergence of the tooth from the socket, while the majority (80%) were not aware of the severity of this lesion and the immediate actions to be taken. Similarly, only 20% answered correctly what a dental fracture is, recognizing it as damage that can range from a simple fracture of the enamel to more complex fractures involving the dentin or pulp. Furthermore, knowledge about dental luxations was found to be adequate in only 29% of cases, with 67% of participants not knowing how to recognize this type of trauma.
The data shows a significant lack of knowledge among participants regarding actions to take immediately in the event of dental trauma. Only 20% of participants know how to correctly intervene in the event of tooth avulsion, indicating that the avulsed tooth should be gently rinsed with milk, saline, or saliva and reinserted into its original position. The majority (80%) have no idea what the correct procedure to follow is.
Regarding a tooth fracture, just 20% of participants know that the fractured tooth fragment should be stored in a moist medium, such as milk or saliva, before going to the dentist, while over half (53%) did not know what to do.
The athletes’ knowledge was insufficient as for tooth luxation too: only the 4% of athletes knew that the dislocated tooth should be gently repositioned in its original location, while the majority (64%) declared they do not know how to intervene. These results highlight a poor general preparation on the emergency treatments necessary to effectively manage dental trauma.
The findings highlight the need to improve athlete education on the management of dental trauma. Given that the majority of interviewees are not adequately prepared to deal with these events, it is essential to implement specific educational programs that cover the different types of dental trauma and their immediate treatments. Adoption of such programs can help reduce the incidence of complications and improve long-term clinical outcomes.
A limitation of the present study is due to its methods: a survey-based study has obvious biases due to the possible not appropriate and honest answers by the investigated subjects. The response rate is an important issue too; in fact, only about half of the surveys were completed. This result, although good if compared with expected response rates in facial trauma surveys, still represents a possible limitation: the possible answers could represent a more “responsive” study population, thus including only the athletes that pay more attention to health issues.
In conclusion, the role of dental practitioners is fundamental in the prevention of dental trauma, especially for athletes who practice contact sports. This study highlighted the need to promote good oral hygiene practices as well as to improve education and awareness regarding the use of mouthguards, their daily cleaning and the management of dental trauma.
Furthermore, athletes should be supported in choosing the most suitable mouthguard, taking into account specific sporting and personal needs. The state of wear of the device should also be periodically monitored, and its replacement should be recommended when necessary to ensure optimal protection over time.
Informing athletes and technical staff on the procedures to follow in case of dental trauma is essential to improve the management of emergencies on the field. Training in emergency protocols can significantly reduce the risk of long-term complications and improve treatment outcomes.
Footnotes
Ethical Considerations
IRB exempt in agreement with local laws as an observational study.
Consent to Participate
All the subjects gave their informed consent to participate to the present study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.