
Abstract
Traumatic injuries resulting in complex pan-orbital fractures, often accompanied by fractures of the skull base, calvarium, and midface, present a unique surgical challenge. These injuries are often difficult to address in a single operation due to the need for staged neurosurgical and orbital reconstruction. Neurosurgical repair of the dura and orbital roof fractures may need to be performed before addressing fractures of the medial orbital wall and orbital floor. Pushing orbital contents back into the orbit from below is especially difficult with swelling from a CSF leak, and the risk of damaging a newly repaired orbital roof and dura. Waiting for the orbital roof and dural repair to heal is an option, but delayed repair of the other orbital walls is difficult once there is scarring and fibrosis of the orbital contents to sinus mucosa. In ballistic injuries with near-total destruction of the orbit, reconstruction is further complicated by the loss of natural anatomical landmarks. We present a novel staged operative repair of complex pan-orbital trauma due to a gunshot wound. This patient suffered multiple fractures of the orbit, including right orbital roof and medial orbital wall fractures, and left orbital roof, floor, and medial orbital wall fractures. The patient also had bifrontal herniation, CSF leak, and suffered a left globe obliteration rendering that eye unsalvageable.
Introduction
Approximately 3% of all emergency department visits in the United States involve ocular trauma, requiring rapid assessment to determine the urgency of eye injuries and possible concomitant damage to the brain, spinal cord, or facial bones.1,2 Complex orbital fractures can involve a single or multiple anatomical subunits of the bony orbit, with fractures possible at the orbital floor, medial orbital wall, orbital roof, and involving the lateral orbital wall within the zygomaticomaxillary complex (ZMC). The most common location is the lamina papyracea of the ethmoid bone (54.9%), the thinnest bone of the orbit. 3
The orbital roof is the least frequently fractured component of the bony orbit, usually breaking only due to high-energy impacts such as motor vehicle accidents (MVAs), falls, or assaults, which can result in serious craniofacial traumas. Neurologic injuries (57%-90%), ocular damage (14%-38%), and additional facial fractures (33%) are commonly associated with orbital roof fractures. Therefore, orbital roof fractures pose a unique challenge as they also involve skull base reconstruction. Due to the orbital roof’s proximity to the intracranial space, emergent surgical intervention can often be required to mitigate the risks of CSF leakage, hematoma formation, mucocele development, and encephalocele. 4 Ophthalmic indications for intervention in orbital roof fractures are less common, but may include ocular open globe injury, retrobulbar hematoma, or bony fragments displaced into the orbit causing extra ocular movement restriction. 5
The bicoronal craniotomy approach is the most common surgical technique for addressing orbital roof fractures. It facilitates reconstruction of the superior orbital rim and roof using titanium miniplates, bone grafts, or porous polyethylene implants (MedPor; Stryker Corporation, Kalamazoo, MI) that provide enhanced structural stability and promote early vascularization. 6 For non-emergent injuries, surgical timing remains controversial. A semi-urgent approach (7-14 days post-injury) is often recommended to allow for the resolution of edema while minimizing the risk of extensive soft tissue fibrosis, which traditionally begins after 2 weeks.7-9 However, evidence supporting this recommendation is largely anecdotal for orbital roof fractures, with minimal literature commenting on the increased scarring and resulting difficulty of orbital reconstruction.
Surgical access to the medial orbital wall and the orbital floor may involve a transcutaneous, transconjunctival, or transnasal approach. 10 Unlike orbital roof fractures, medial orbital wall fractures generally do not carry the same urgency to being repaired if there is no concurrent intracranial injury, and only need to be addressed urgently in cases of muscle entrapment. In a growing number of cases, preoperative planning with a mirror-image overlay (MIO) of the patient’s normal orbit or real-time intraoperative computed tomography (CT) imaging have recently gained traction for improving the accuracy of implant placement and bone repositioning.11,12
Traumatic complex pan-orbital fractures present a unique challenge. Orbital roof repair is usually combined with urgently required neurosurgical procedures, but reconstruction of the other orbital walls and orbital floor from below is often difficult in the same surgical setting. However, delayed repair carries the risk of fibrosis and suboptimal outcomes. Additionally, ballistic injuries also cause the loss of anatomical landmarks and can significantly complicate bone re-approximation, prolong operative time, and increase the risk of enophthalmos.9,13 We present a case of a patient with a complex ballistic pan-orbital trauma, in whom a staged repair was performed. An additional implant was placed during the primary surgery of orbital roof repair, which facilitated the secondary repair due to the medial orbital wall implant serving as a structural guide. This novel approach allowed for ease of re-approximating the medial orbital wall, provided structural support of the orbital floor implant, and potentially improved the esthetic outcome in the setting of extensive orbital trauma.
Case Presentation
A 27-year-old male presented to our emergency department with multiple gunshot wound injuries to the face and head. He sustained multiple fractures of the bony orbits, along with bifrontal cerebral herniation, total obliteration of the left eye, subarachnoid hemorrhage, subdural hematoma, and a cerebrospinal fluid leak. Upon imaging, the patient was found to have an acute gunshot injury traversing from the left maxilla through the right temporal bone, leaving a 13 mm comminuted ballistic hole-like fracture that extended linearly into the right parietal bone. The left eye was deemed unsalvageable with no identifiable ocular contents upon exam or CT scan (Figure 1).
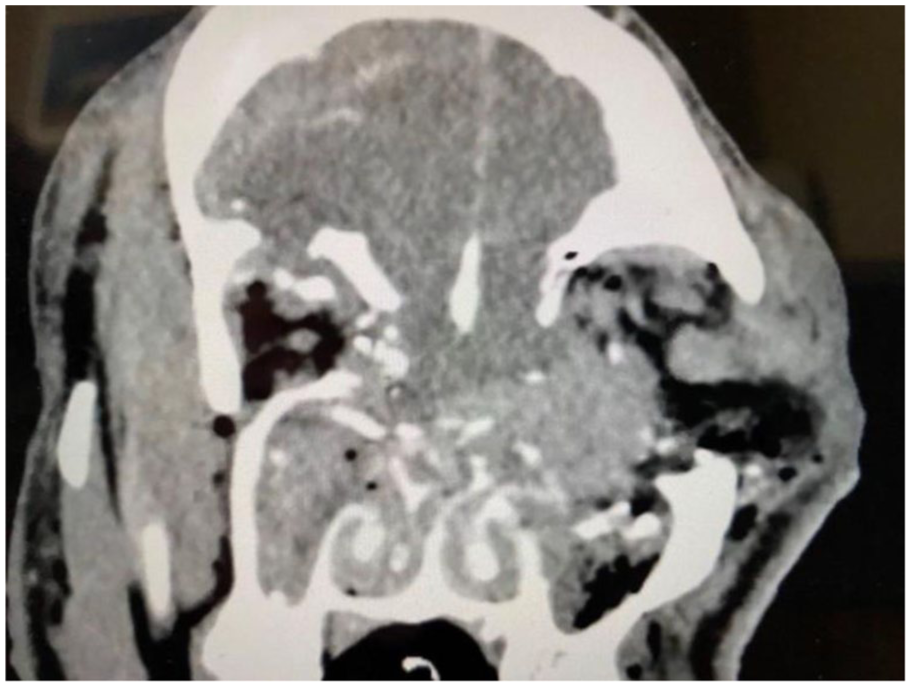
Coronal CT imaging of the patient with comminuted fractures of multiple facial bones, including right orbital roof, right medial orbital wall, left orbital floor, and left medial orbital wall.
The initial surgery was performed by the Ophthalmology, Plastic Surgery, and Neurosurgery teams. First, a left eye evisceration was performed, followed by the placement of a 19 mm silicone sphere ocular implant. Then, a bifrontal craniotomy was performed, and the dura was repaired. Through this approach, both orbital roofs were also repaired using a Stryker Medpor Barrier 0.35 mm implant. The periosteum of the left medial orbital wall was carefully elevated, and an additional Medpor Barrier implant was then placed via direct visualization in the left orbit from above against any intact bone to cover the superior portion of the medial orbital wall fracture. The patient also underwent frontal sinus cranialization by removal of the posterior wall and resection of the crista galli. The pericranial flap and the craniotomy were then closed (Figures 2-4).
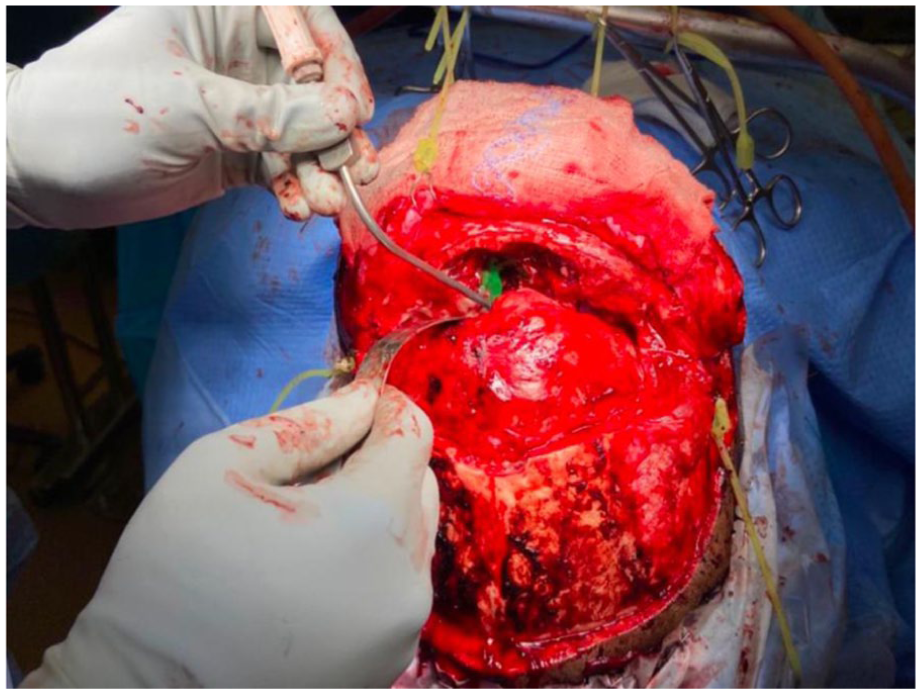
Intraoperative photograph demonstrating the initial placement of the Barrier implant (covered in green adhesive) in the left orbital medial wall from above.
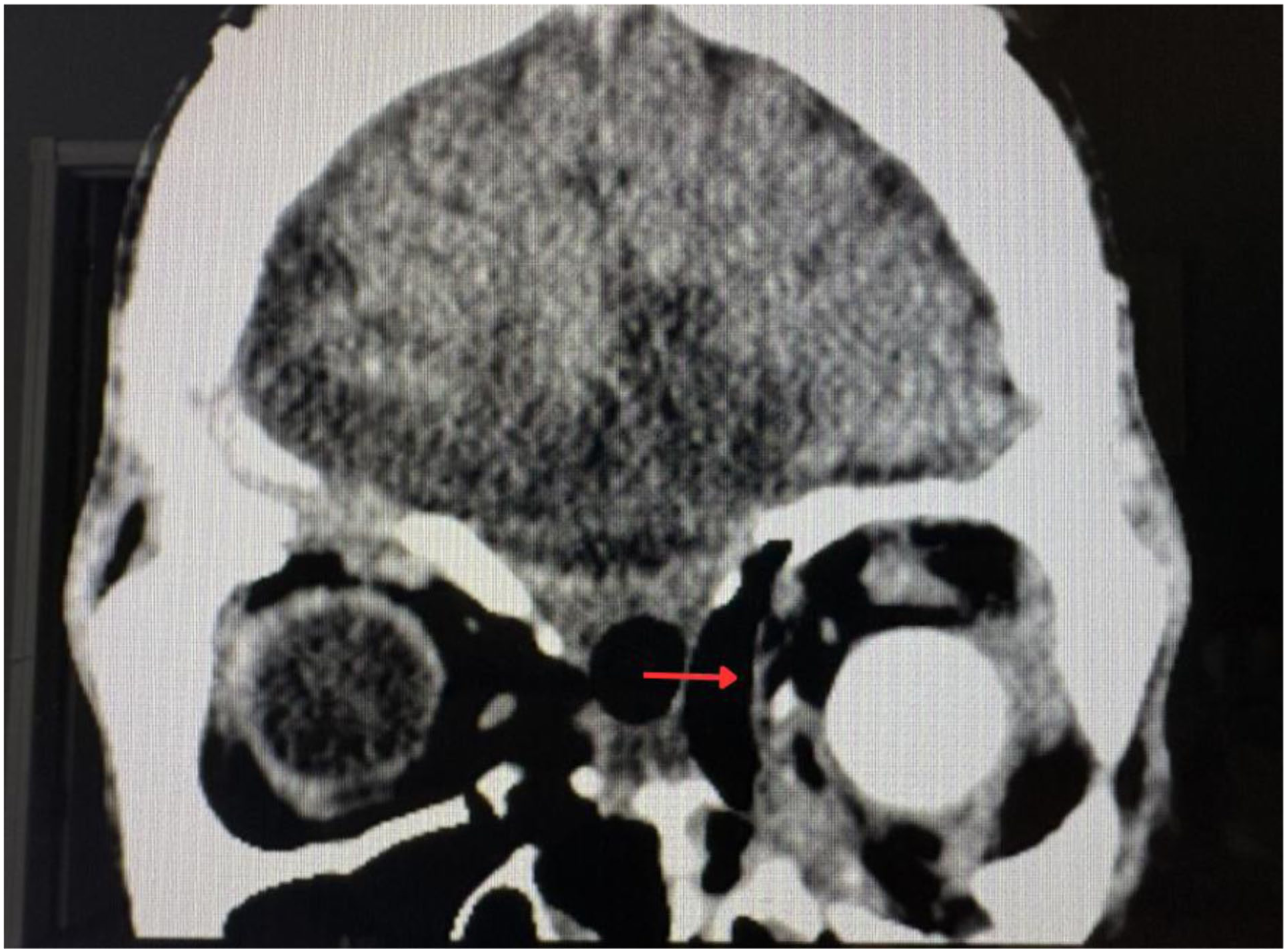
Postoperative CT scan 1 month after the first surgery demonstrating the supramid implant in position along the left medial wall, shown as the red arrow.
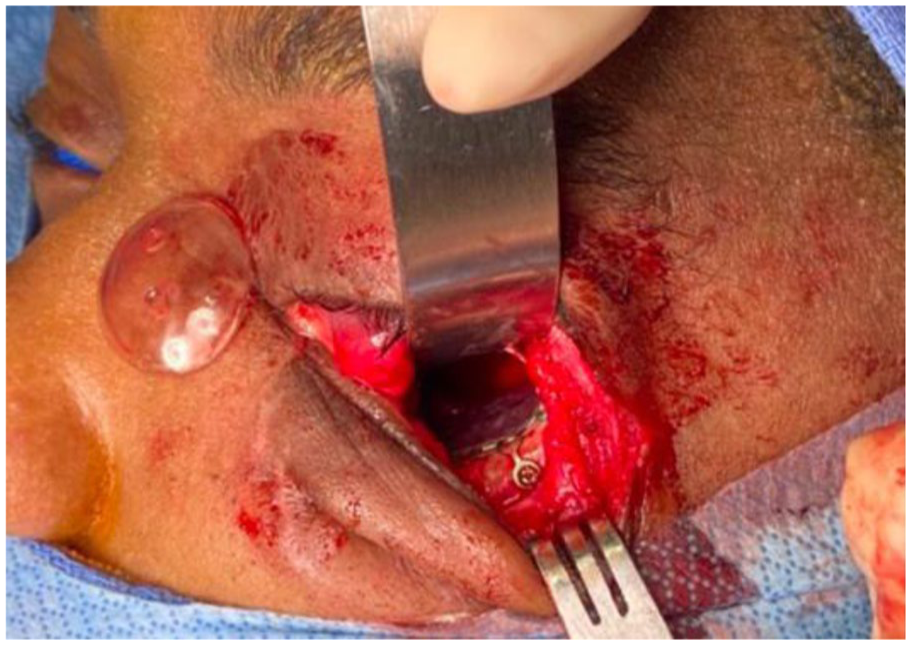
Follow up surgery took place 6 weeks later to reconstruct the left orbital floor and inferior part of the left medial orbital wall fracture.
After a 6-week healing period to allow the medial wall implant to stabilize, the left orbital floor and inferior part of the medial orbital wall were reconstructed during a second operation through an inferior conjunctival approach. After reduction of tissue that had prolapsed into the orbital floor fracture, the tissue plane was dissected superiorly up the medial orbital wall fracture to locate the previously placed Barrier implant used to reconstruct the upper part of the medial orbital wall. The implant served as a guide to place a Stryker Medpor Titan Floor (polyethylene-titanium) implant that curved up to meet the Barrier implant. The Titan Floor implant was then fixated to the inferior orbital rim with a screw. Although the patient sustained bilateral orbital fractures, the contralateral (right) orbit showed relatively little displacement. Also, the right eye had sustained retinal injury, and we did not want to risk further damage to the only functional eye.
Outcome
The postoperative course for both procedures was uneventful and there were no major complications.
Discussion
The high-velocity nature of ballistic trauma poses unique reconstructive challenges due to obliterative damage along with the displacement of orbital components. Tissues can be lacerated and crushed along the path of the projectile, capable of deforming a widespread area of soft tissue and bony foundations. 14 Nonavulsive injuries can typically be managed as blunt facial fractures with overlying lacerations, whereas avulsive injuries due to high-energy transfers (close-range shotguns, rifles, and handguns) can lead to both immediate tissue loss and a larger secondary area of evolving necrosis. 15 Unlike more common fracture patterns from blunt trauma, gunshot wound injuries lack intact reference points, making implant positioning and anatomic approximation particularly difficult. 16 Immediate primary repair can be complicated by initial dead space, ischemia, hematoma, and infection. For managing bone defects, the goal is typically to prevent contracture of the soft tissues while restoring the width and height of facial proportions. 14 Literature guiding surgical management in this field is limited, with many studies lacking any reports on esthetic outcomes and optimal timing of debridement or fixation. In a systematic review including 17 articles, early definitive reconstruction and aggressive interventions appeared to improve outcomes, resulting in decreased incidence of soft-tissue contracture and hospitalization time. 15 Conversely, another study indicated that initial debridement and stabilization should take place within 48 hours, followed by delayed reconstruction after 30 days to reduce risks of infection and fistula formation. 17 Although surgical techniques for orbital reconstruction have advanced significantly, there remains a notable lack of standardized guidelines and high-quality evidence regarding the optimal sequence of bony repair and implant placement in complex ballistic trauma patients.
Pan-orbital ballistic fractures can often require surgery within an urgent time window, especially if there is intracranial injury. Even after surgical repair, however, there is often a need for re-operation, with a major reason for the high revision rates (2%-18%) being poor positioning of the implant.18,19 While intra-operative computer-assisted surgical planning has offered advantages for nonavulsive fractures involving the bony orbit, the loss of structural anatomical integrity in ballistic injuries complicates the use of these techniques.15,20 Therefore, this case offers a novel strategy for staging fracture repair by placing an implant as a guide for the second surgery in complex pan-orbital trauma.
Extensive fractures require prioritization of intracranial injuries and surgical restoration of original orbital volume, often requiring more than 1 surgery. A similar case report by Pawar et al also employed a 2-stage surgical repair of a cranio-orbital gunshot wound that required close collaboration with Otolaryngology, Neurosurgery, and Oculoplastic Surgery services. 21 The first surgery involved using an autogenous bone graft to reconstruct the superior orbital roof, followed by a second surgery with enucleation and use of a cantilevered titanium mesh to repair the orbital floor and ZMC via a standard transconjunctival approach. In our approach, the left globe was enucleated in the first-stage reconstruction and a Stryker Medpor implant was placed in the medial orbital wall prior to the second surgery. Both cases used a titanium mesh implant for reconstruction of the orbital floor, which demonstrates good biocompatibility, resistance to infection, and adequate strength. Polyethylene-titanium implants (ie, Stryker MedPor Titan Floor) specifically can be pre-sized and pre-contoured to model anatomically averaged orbits, providing improvements in diplopia, enophthalmos, and lowered incidences of postoperative revisional surgeries. 22 Since 2010, patient-specific implants (PSI) from CT scan-derived MIOs have also become more common and show improved enophthalmos compared to standard orbital mesh. 23 Since the existing medial wall implant effectively guided floor reconstruction in this case, a custom implant was not expected to offer additional benefit. Overall, a coordinated interdisciplinary staged-repair approach involving multiple specialties is crucial to addressing complex cranio-orbital ballistic injuries.
A limitation was that the patient was lost to follow up after the second surgery, precluding additional postoperative imaging. Additional studies are needed to assess the optimal timing between surgeries and the most appropriate type of implant material used. Although staging orbital repair over time may help improve the outcome, it could potentially increase the risk of infection and prolong recovery time.
Conclusion
Ballistic injuries present one of the most complex challenges in facial reconstructive surgery. For patients with complex pan-orbital trauma, staging operative repair and using a previously placed medial orbital wall implant to guide the placement of an orbital floor implant may be a useful way to reconstruct the orbit and to improve surgical outcomes. In the setting of significant anatomical landmark disruption and soft tissue swelling, a fixed reference point for secondary reconstruction facilitates accurate implant positioning of the orbital floor and medial orbital wall.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.